
Abstract
Optimizing immunosuppressive therapy remains central to improving long-term outcomes after kidney transplantation. Both induction and maintenance therapies are widely used, yet their comparative effectiveness across heterogeneous populations requires further evaluation. To this end, this national retrospective cohort study analyzed 228,855 deceased-donor kidney transplant recipients using the over two-decade data (2000-2024). We employed multivariable Cox proportional hazards (PH) models for clinical inference and four machine learning (ML) survival models: random survival forest (RSF), support vector machine (SVM), penalized Cox regression (CoxNet), and extreme gradient boosting optimized with the Cox partial likelihood (XGBoost-Cox) to assess predictive performance of death-censored graft failure and all-cause patient mortality. Model performance was evaluated using the concordance index (C-index) and time-dependent area under the curve (tdAUC).
Maintenance regimens with calcineurin inhibitors (CNI) and mycophenolate mofetil (MMF) demonstrated protective effects for both graft failure (CNI+MMF: hazard ratio [HR] 0.72, 95% confidence interval [CI] 0.70-0.74; CNI+MMF+steroids: HR 0.84, 95% CI 0.82-0.87) and patient mortality (CNI+MMF: HR 0.78, 95% CI 0.76-0.81; CNI+MMF+steroids: HR 0.90, 95% CI 0.88-0.93). Among induction therapies, antithymocyte globulin (ATG) showed protective associations (HR 0.93 for both outcomes), while interleukin-2 receptor (IL-2R) antagonists and Alemtuzumab demonstrated neutral effects. Combined ATG + IL-2R therapy comparatively increased the hazard of graft failure (HR 1.09). Recipient diabetes, dialysis dependence, older age, and higher Kidney Donor Profile Index (KDPI) were strong adverse predictors. Traditional Cox regression achieved robust discrimination (graft failure concordance index: 0.685; patient mortality concordance index: 0.704) comparable to ML survival models.
These findings reinforce CNI and MMF maintenance regimens as foundational to contemporary immunosuppression while demonstrating differential effectiveness across induction strategies. The dual analytical framework, which integrates classical Cox PH modeling with ML survival models, shows that Cox models remain highly competitive for clinical inference while ML approaches offer complementary predictive value to support individualized post-transplant risk stratification.
Introduction
Kidney transplantation is the gold standard treatment for end-stage renal disease, offering superior survival, cost-effectiveness, and quality of life compared to long-term dialysis [1,2]. The long-term success of a transplant, however, is threatened by the recipient’s immune response to the foreign graft. This response is primarily triggered by the disparity in human leukocyte antigens (HLAs) between the donor and recipient, which activates the recipient’s T cells and can lead to graft failure through two principal pathways: antibody-mediated and cellular-mediated rejection [3]. Antibody-mediated rejection involves B-cells producing donor-specific antibodies, a process dependent on CD4+ T-cell help [4,5]. In contrast, cellular rejection is driven directly by the cytotoxic activity of T cells, alongside other immune cells such as macrophages and natural killer cells [6]. Without tailored immunosuppressive medications to modulate the immune response, a persistent immune attack leads to progressive immune-mediated injury, marked by inflammation, tissue damage, and potential graft failure [7]. Such injury may present as acute rejection early after transplantation or evolve into chronic rejection over time, thereby highlighting the vital role of immunosuppressive treatment.
Immunosuppressive therapies aim to prevent or control this immune-mediated injury by suppressing the recipient’s immune system. By doing so, they reduce the immune response against the allograft, attenuate inflammation, and help preserve its function and viability. Thus, the imperative for post-transplant immunosuppression emerges, with the principal objective of modulating and mitigating immune responses to safeguard the viability and functionality of the transplanted kidney within the recipient’s body.
Despite the crucial role of immunosuppressive therapy, it carries potential risks and side effects, emphasizing the need to balance immune suppression and complications. The definitive protocol remains undetermined [8–10], with most centers employing an approach involving induction therapy with interleukin-2 receptor (IL-2R) antibodies or antithymocyte globulin (ATG), along with a maintenance regimen comprising steroids, calcineurin inhibitors (CNIs), and mycophenolate mofetil (MMF) [11,12]. Although these advances have substantially improved short-term graft survival, the challenge of achieving durable long-term outcomes persists [13–15]. Therefore, ongoing research continues to seek regimens that maximize short-term benefits while minimizing the risk of long-term deterioration [16].
Predicting long-term outcomes is fundamental to personalizing care and improving graft survival. For decades, survival analysis methods, particularly Cox proportional hazards (PH) regression, has been the cornerstone of outcome evaluation in kidney transplantation. Cox models allow estimation of hazard ratios (HRs), providing clinicians with interpretable measures of the relative risk of graft failure or patient death associated with specific therapies or clinical covariates [17–19]. These models are well-suited to accommodate censoring, varying follow-up times, and the multifactorial nature of post-transplant outcomes.
At the same time, the growing availability of large-scale transplant datasets has created opportunities for machine learning (ML) methods to complement traditional survival models. More recently, ML survival models such as random survival forests (RSFs), support vector machines (SVMs), and gradient boosting survival models, have demonstrated the potential to improve risk prediction in transplantation by modeling nonlinear interactions and high-dimensional patterns that may not be fully represented in standard Cox regression [20–22]. Yet, many prior ML studies in kidney transplantation have been limited by small sample sizes, older cohorts, or lack of direct comparison with classical survival models using the same covariate structure [23–26]. Additionally, few have explicitly examined both induction and maintenance immunosuppressive strategies within ML frameworks, and even fewer have evaluated their performance against death-censored graft survival and patient mortality outcomes using contemporary national data.
The current study addresses these gaps by leveraging a large and recent national cohort of deceased-donor kidney transplant recipients and examining both induction and maintenance immunosuppressive therapies in relation to long-term outcomes. Death-censored graft survival and all-cause patient mortality were evaluated using multivariable Cox proportional hazards models to provide clinically interpretable estimates of relative risk associated with specific therapeutic regimens. In parallel, multiple ML survival models were developed using the same covariate structure to determine whether they offer incremental predictive value beyond classical Cox regression. Model performance was evaluated using concordance index (C-index) and time-dependent area under the curve (tdAUC) metrics at clinically relevant follow-up intervals, enabling direct comparison of inference-focused and prediction-focused approaches within a unified analytical framework.
By integrating classical survival modeling with contemporary ML survival methods in a large and up-to-date national dataset, this study provides a rigorous evaluation of immunosuppressive regimen effectiveness while simultaneously assessing the extent to which advanced predictive algorithms offer added clinical value. This dual analytical perspective is intended to support both evidence-based regimen selection and the advancement of individualized post-transplant risk stratification.
Materials and Methods
Data Source and Study Population
This retrospective cohort study used data from the United Network for Organ Sharing (UNOS) registry. Two data extracts were provided: an earlier file covering January 1, 2000, through May 29, 2021, and a subsequent update containing transplants from January 1, 2015, through October 30, 2024. These datasets were merged using transplant recipient identifiers and procedure-level record keys, with harmonization of variable definitions and removal of duplicate entries during overlapping years, to create a unified dataset spanning January 1, 2000, to October 30, 2024. The analysis was restricted to adult recipients of deceased-donor kidney transplants, identified using the donor type variable. Living-donor kidney transplants were excluded, as were observations with incomplete or non-positive follow-up times as well as extensive missing values for some critical variables. The final analytic cohort included 228,855 deceased-donor kidney transplant recipients.
Study Outcome
Two clinically relevant post-transplant outcomes were examined. The primary endpoint was death-censored graft failure, defined as the time from kidney transplantation to return to dialysis or re-transplantation, with deaths occurring in the presence of a functioning graft treated as censored events at the time of death. The secondary endpoint was all-cause patient mortality, defined as time from transplantation to death from any cause, regardless of graft function. Follow-up time for both outcomes was calculated from transplantation date to event occurrence or administrative censoring on October 30, 2024, whichever occurred first. Both outcomes were analyzed using time-to-event methods appropriate for right-censored data.
Predictor Variables and Data Preprocessing
Candidate predictors encompassed donor, recipient, and transplant characteristics, including demographic, clinical, and immunologic factors (e.g., age, Kidney Donor Profile Index [KDPI], HLA mismatches, calculated panel-reactive antibody [cPRA]). Immunosuppressive regimens were the key focus. ATG constituted the predominant induction therapy in the cohort (59.6%, n = 136,458), with IL-2R antagonists (19.4%, n = 44,512) and Alemtuzumab (12.2%, n = 27,982) used less frequently. For maintenance therapy, a triple regimen of CNI, MMF, and steroids predominated (67.1%, n = 153,515), while a steroid-free combination of CNI + MMF accounted for 24.3% (n = 55,637). Other regimens were used less frequently.
Missing data were handled with a combination of complete-case analysis and imputation. The proportion of missing data was low (<1%) for most variables. Continuous variables (e.g., serum creatinine, body mass index [BMI]) were imputed with medians, and categorical variables (e.g., diabetes) were imputed with modes. Missing cPRA values (14.8%) was imputed as 0 (unsensitized) and flagged with a binary indicator; Cold ischemic time (1.4%) was imputed with the median and similarly flagged.
Statistical Analysis
Descriptive and Survival Analysis
Continuous variables were presented as medians with interquartile ranges (IQRs), whereas categorical measures were reported as counts and corresponding percentages. Kaplan–Meier survival curves were generated for graft and patient survival, including subgroup comparisons by donor and recipient factors (e.g., donation after circulatory death [DCD] vs. non-DCD, expanded criteria donor [ECD], KDPI quartiles, recipient diabetes). Group differences in survival were assessed using the log-rank test.
Multicollinearity Assessment and Model Specification
Prior to multivariable modeling, variance inflation factors (VIF) were calculated to assess multicollinearity among candidate predictors. A systematic approach was employed where categorical variables with inherent collinearity (geographic sharing, recipient race, donor race) were coded using reference category exclusion. Geographic sharing utilized ‘local’ as reference, while race variables used ‘white’ as reference category for both recipient and donor. Variables with VIF exceeding 10 were iteratively removed until all remaining predictors demonstrated acceptable collinearity levels (VIF < 10). Continuous variables were maintained in their natural units to preserve clinical interpretability of HRs.
Cox Regression
A multivariable Cox PH model was fitted separately for death-censored graft failure and all-cause patient mortality. All models were constructed using the final predictor set identified after assessing and addressing multicollinearity among covariates. HRs with 95% confidence intervals (CIs) were estimated. The PH assumptions were assessed using Schoenfeld residuals and graphical diagnostics. Final models balanced clinical interpretability and statistical parsimony.
Machine Learning Survival Models
Multiple ML survival algorithms were implemented using identical predictor variables to enable direct comparison with classical Cox regression. The ensemble included: RSF with memory-optimized implementation using warm-start and batch training to prevent computational overload; SVM with kernel optimization; extreme gradient boosting optimized with the Cox partial likelihood (XGBoost-Cox); and penalized Cox regression (CoxNet) with elastic net regularization. Data were randomly split into training (75%) and testing (25%) sets stratified by event status to maintain outcome distribution. Model parameters were selected based on established defaults and transplantation literature, with computational efficiency considerations for the large-scale national dataset. Continuous predictors were standardized for algorithms requiring feature scaling (CoxNet, SVM), while tree-based methods utilized natural units.
Model Evaluation
Each model’s predictive accuracy was assessed using the independent test set not used during training. The concordance index (C-index) was used to evaluate overall discrimination. Time-dependent Area Under the Curve (tdAUC) was computed at 1-, 3-, 5-, and 10-years post-transplant, and the mean tdAUC was used as a summary measure of longitudinal predictive performance. All analyses were performed in Python 3.13.7 using lifelines, scikit-survival, sand scikit-learn libraries.
Results
Cohort Characteristics
The study cohort comprised 228,855 recipients of deceased-donor kidney transplants from 2000-2024. Recipients had a median age of 55 years (interquartile range [IQR] 44-63), with 60.4% male and 36.3% with diabetes. Racial distribution included 39.5% White, 33.5% Black, 17.8% Hispanic, and 7.0% Asian recipients. Diabetes was present in 36.3% of recipients, and 83.0% were receiving dialysis at the time of transplantation. The median BMI was 27.8 kg/m² (IQR 24.2–32.0), and the median cPRA was 0% (IQR 0–29). Approximately 12.2% were retransplants, and the median waiting time prior to transplantation was 639 days (IQR 193–1314).
Donor characteristics reflected a median age of 41 years (IQR 29–52), with 61.3% male donors. DCD accounted for 22.2% of transplants, while 16.2% met expanded-criteria donor ECD definitions. The median KDPI was 40% (IQR 20–62), and the median donor creatinine was 1.0 mg/dL (IQR 0.7–1.4).
Immunosuppressive regimens were heterogeneous: ATG was the most common induction agent (59.6%), followed by IL-2R (19.4%) and Alemtuzumab (12.2%). For maintenance therapy, the majority received a triple regimen of CNI + MMF + steroids (67.1%), with an additional 24.3% maintained on CNI + MMF without steroids. Full characteristics are presented in Table 1.
Overall Graft and Patient Survival
During a median follow-up of 4.0 years (IQR 1.9–7.0), there were 55,346 death-censored graft failures (24.2%) and 43,772 all-cause patient deaths (19.1%) among 228,855 deceased-donor kidney transplant recipients. The distribution of events, censoring, and follow-up time is summarized in Table 2.
Kaplan–Meier analyses demonstrated progressive decline in both graft and patient survival over time, with relatively high early post-transplant survival that gradually decreased during long-term follow-up (Table 3, Figs 1–2). The estimated death-censored graft survival was 95.7% at 1 year, 88.5% at 3 years, 80.1% at 5 years, and 57.8% at 10 years, corresponding to a median graft survival of approximately 12.0 years (95% CI, 11.9–12.0). In comparison, patient survival was 96.8% at 1 year, 91.4% at 3 years, 85.1% at 5 years, and 66.5% at 10 years, with a median all-cause survival of approximately 15.0 years.


Subgroup Survival Analyses
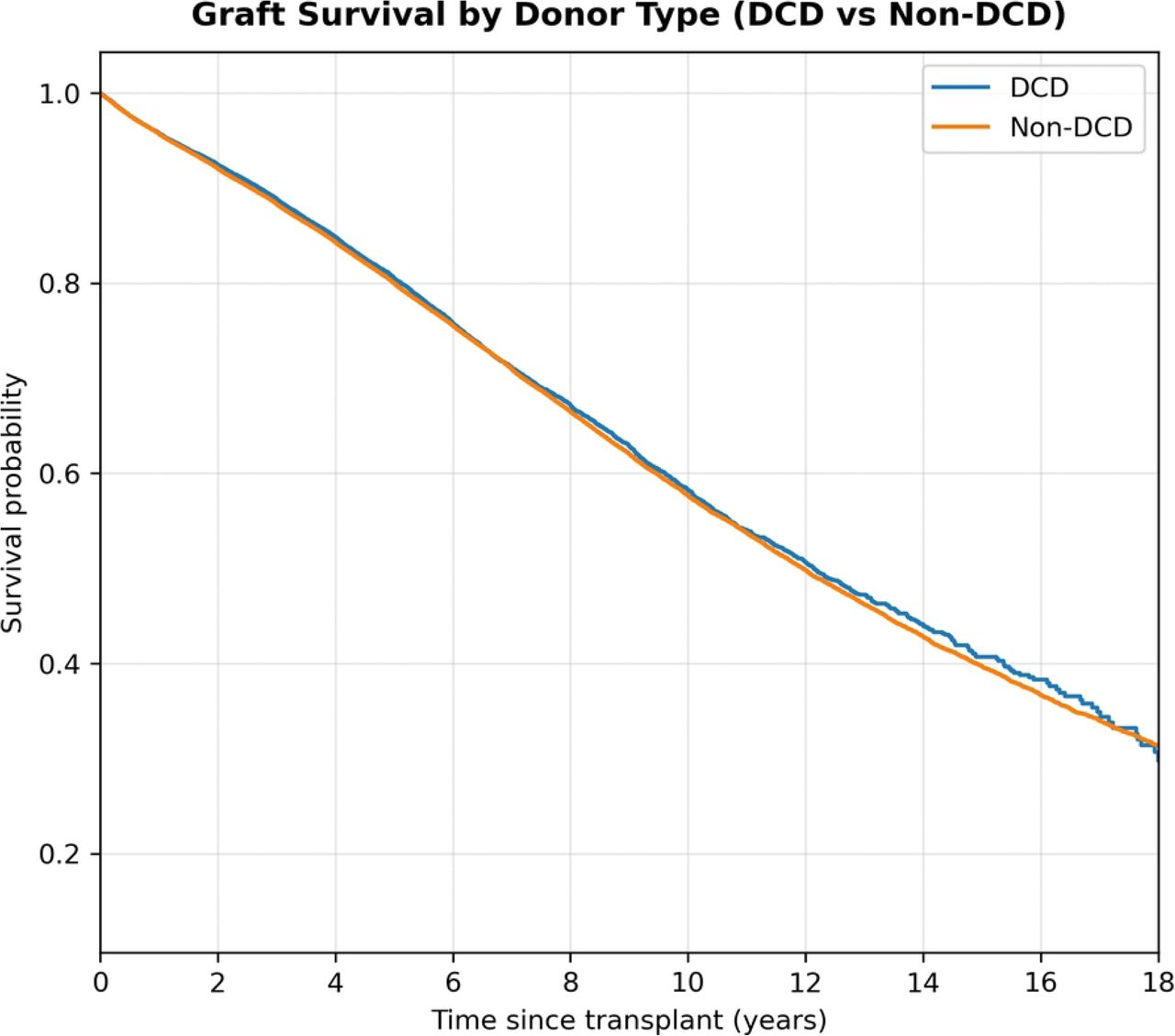
Graft and patient survival differed significantly across key donor and recipient subgroups (Fig 3–10). Recipients of kidneys from DCD had slightly shorter graft survival compared with non-DCD transplants (median 12.1 vs 12.0 years; log-rank χ² = 4.87, p = 0.027). Differences in patient survival were more pronounced, with DCD recipients exhibiting a shorter median survival (14.3 vs 14.9 years; log-rank χ² = 40.11, p < 0.001). In contrast, kidneys from ECD showed markedly reduced outcomes. Median graft survival was 8.1 years for ECD versus 13.0 years for non-ECD donors (log-rank χ² = 4150.03, p < 0.001), and median patient survival was 10.4 vs 15.8 years, respectively (log-rank χ² = 2961.72, p < 0.001).

Kaplan–Meier curves comparing graft survival between DCD and non-DCD donors. Log-rank χ² and p-values are derived from univariate comparisons.

Kaplan–Meier curves comparing patient survival between DCD and non-DCD donors. Log-rank χ² and p-values are derived from univariate comparisons.

Kaplan–Meier curves comparing graft survival for expanded-criteria donors (ECD) versus non-ECD donors. Log-rank χ² and p-values are derived from univariate comparisons.

Kaplan–Meier curves comparing patient survival for ECD versus non-ECD donors. Log-rank χ² and p-values are derived from univariate comparisons.

Kaplan–Meier curves comparing graft survival between diabetic and non-diabetic recipients at the time of transplantation. Log-rank χ² and p-values are derived from univariate comparisons.

Kaplan–Meier curves comparing patient survival between diabetic and non-diabetic recipients. Log-rank χ² and p-values are derived from univariate comparisons.
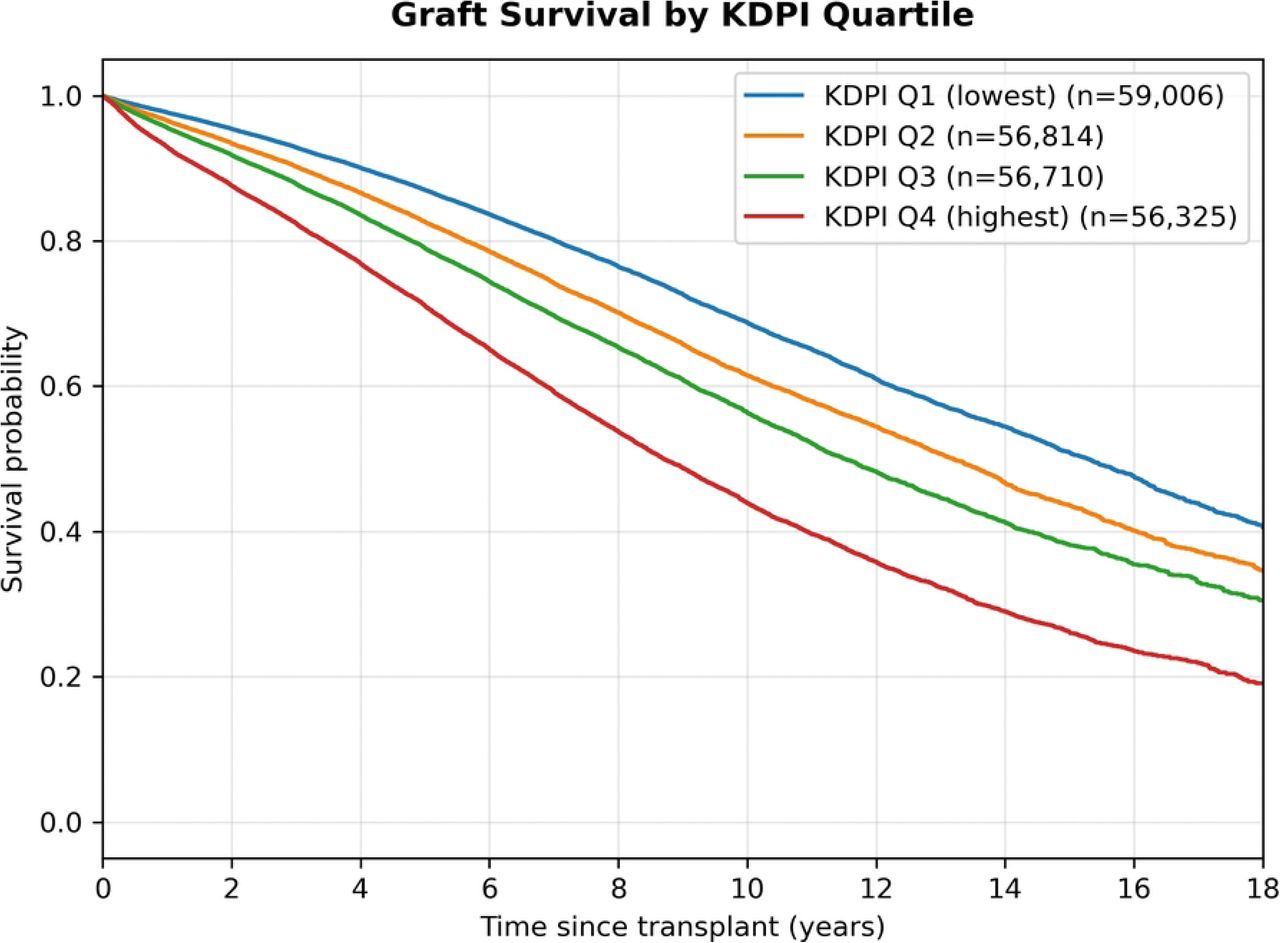
Recipient diabetes was associated with striking survival disparities. Graft survival differed sharply by diabetic status, with recipients who had diabetes experiencing a median survival of 8.4 years, whereas those without diabetes reached 15.3 years (log-rank χ² = 8463.18, p < 0.001). Median patient survival followed a similar pattern (10.1 vs 17.9 years; log-rank χ² = 7871.70, p < 0.001). The KDPI quartiles showed a stepwise gradient (Fig 9–10). Graft and patient survival declined progressively from the lowest KDPI quartile (Q1) to the highest (Q4) (multigroup log-rank χ² = 5420.45 and 3746.92, respectively; p < 0.001 for both).

Kaplan–Meier curves stratified by KDPI quartiles (Q1–Q4). Log-rank χ² and p-values are derived from a multigroup comparison.

Kaplan–Meier curves stratified by KDPI quartiles (Q1–Q4). Log-rank χ² and p-values are derived from a multigroup comparison.
Multivariable Cox Proportional Hazards Models
Multivariable Cox regression models identified distinct risk factor profiles for graft failure and patient mortality while controlling for comprehensive donor, recipient, and transplant characteristics (Table 4-5). Immunosuppressive regimens demonstrated significant associations with both outcomes, though with varying effect magnitudes across therapeutic classes. For maintenance immunosuppression, CNI + MMF regimens provided substantial protection against both graft failure (HR 0.72, 95% CI 0.70-0.74, p < 0.001) and patient mortality (HR 0.78, 95% CI 0.76-0.81, p < 0.001). The addition of steroids to this backbone in triple-therapy regimens (CNI + MMF + steroids) also conferred significant protection, though with more modest effect sizes (graft failure HR 0.84, 95% CI 0.82-0.87; patient mortality HR 0.90, 95% CI 0.88-0.93; both p < 0.001).
Among induction therapies, ATG demonstrated protective effects for both graft failure (HR 0.93, 95% CI 0.89-0.97, p = 0.002) and patient mortality (HR 0.93, 95% CI 0.89-0.98, p = 0.004). IL-2R showed neutral association with graft failure (HR 1.04, 95% CI 0.99-1.09, p = 0.102) and patient mortality (HR 0.95, 95% CI 0.91-1.00, p = 0.070). Alemtuzumab demonstrated neutral effects for both outcomes (graft failure HR 0.97, 95% CI 0.92-1.02, p = 0.234; patient mortality HR 0.95, 95% CI 0.90-1.01, p = 0.103). Combination therapy with ATG + IL-2R was associated with increased hazard for graft failure (HR 1.09, 95% CI 1.03-1.16, p = 0.002) but showed neutral association with patient mortality (HR 1.02, 95% CI 0.96-1.09, p = 0.470).
Recipient diabetes was among the strongest predictors of adverse outcomes, increasing the risk of graft failure by 63 % (HR 1.63, 95 % CI 1.60–1.66, p < 0.001) and patient mortality by 67 % (HR 1.67, 95 % CI 1.63–1.70, p < 0.001). Older recipient age was also independently associated with higher hazards for both graft failure (HR 1.04 per year, 95 % CI 1.04–1.04) and mortality (HR 1.05 per year, 95 % CI 1.05–1.05; both p < 0.001). Being on dialysis at the time of transplantation conferred approximately 1.5-fold greater risk for both outcomes. Both retransplantation (graft HR 1.27; mortality HR 1.22) and male recipient (graft HR 1.15; mortality HR 1.19) showed increased risks for each outcome. By contrast, recipients of Asian and Hispanic ancestry experienced significantly lower hazards for both graft loss and death compared with White recipients (graft: HR 0.61 and 0.74; patient: HR 0.64 and 0.76, all p < 0.001). Black recipients showed modest protection for graft failure (HR 0.97, 95% CI 0.95-0.99, p = 0.010) but more substantial protection for mortality (HR 0.92, 95% CI 0.90-0.94, p < 0.001).
Among donor factors, a higher KDPI was consistently associated with 68 % higher risk of graft failure (HR 1.68, 95% CI 1.57–1.81) and 37% higher risk of mortality (HR 1.37, 95% CI 1.26–1.48; both p < 0.001). Older donor age demonstrated a small but significant association with graft failure (HR 1.00 per year, 95% CI 1.00–1.00, p < 0.001) and patient mortality (HR 1.00 per year, 95% CI 1.00–1.00, p < 0.001). Higher donor serum creatinine was weakly but significantly associated with greater risk of graft failure (HR 0.99 per mg/dL, 95% CI 0.98–1.00, p = 0.027) and neutral association with mortality (HR 1.00, 95% CI 0.99–1.01, p = 0.420). Donor diabetes conferred a higher risk of both graft failure and patient mortality (graft HR 1.05, p = 0.002; patient HR 1.05, p = 0.013). Black donor race modestly increased hazards for both outcomes (graft failure HR 1.08, 95% CI 1.05–1.11; mortality HR 1.05, 95% CI 1.02–1.09), whereas Hispanic donor ethnicity conferred a small protective effect for graft failure (HR 0.96, 95% CI 0.94–0.99, p = 0.006).
Among transplant-related factors, prolonged cold ischemia time showed a small but statistically meaningful increase in risk for both graft failure and patient death (HR ≈ 1.00 per hour, p < 0.001), reflecting cumulative ischemic injury over time. Interestingly, after adjustment, DCD status was associated with slightly lower hazards for graft loss (HR 0.91, 95% CI 0.89–0.93, p < 0.001) and neutral association with patient mortality (HR 1.01, 95% CI 0.98–1.04, p = 0.488). This reversal from the unadjusted Kaplan–Meier results reflects adequate model control for confounding donor and recipient variables. As shown in Fig 11, the pattern of risk differs between graft failure and patient mortality, with several predictors demonstrating distinct effect sizes for the two endpoints.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot depicting adjusted hazard ratios (HRs) and 95% confidence intervals (CIs) for major predictors of graft failure. Values to the left of the vertical line (HR = 1) indicate lower risk and those to the right indicate higher risk. Model adjusted for donor, recipient, and transplant factors.
Prediction Performance
The predictive performance of the classical Cox PH model was benchmarked against four ML-based survival algorithms using an independent test cohort (Table 6). For graft failure, the classical Cox PH model achieved a C-index of 0.687 and mean tdAUC of 0.706, with horizon-specific AUCs of 0.692, 0.688, 0.699, and 0.746 at 1, 3, 5, and 10 years, respectively.
Among the ML survival models, XGB-Cox demonstrated the best overall discrimination (C-index = 0.689, mean tdAUC = 0.710), followed closely by CoxNet (C-index = 0.686, mean tdAUC = 0.707) and SVM (C-index = 0.687, mean tdAUC = 0.705). The RSF yielded slightly lower but comparable performance (C-index = 0.680, mean tdAUC = 0.703).
For patient mortality, all models achieved higher concordance than in graft prediction, with C-index values above 0.70. XGB-Cox again outperformed other models (C-index: 0.705, mean tdAUC: 0.727), followed closely by the Cox PH (C-index: 0.703, mean tdAUC: 0.726) and CoxNet (C-index: 0.703, mean tdAUC: 0.725). The SVM (C-index: 0.703, mean tdAUC: 0.724) and RSF (C-index: 0.700, mean tdAUC: 0.723) models also showed stable predictive accuracy across time horizons.
Discussion
In this large, contemporary national cohort of deceased-donor kidney transplant recipients, immunosuppressive regimen selection emerged as a critical determinant of long-term graft and patient survival. Standard maintenance therapy comprising a CNI and MMF, with or without steroids, was consistently associated with lower risks of graft failure and patient mortality, confirming these as the predominant maintenance strategies associated with optimal long-term outcomes in contemporary practice. The substantial protective effects of CNI + MMF regimens (graft failure HR 0.72, patient mortality HR 0.78) align with established evidence supporting CNI and MMF based combinations as the cornerstone of contemporary maintenance immunosuppression, which balance effective rejection prevention with manageable toxicity profiles [27, 28]. The observed protective effect of CNI+MMF+steroid triple therapy (graft HR 0.84; mortality HR 0.90) is consistent with clinical trials and registry studies that support the use of steroid-containing regimens, particularly in the early post-transplant period for immunologically high-risk recipients [12, 29–31].
Among induction strategies, ATG only induction demonstrated consistent protective effects across both outcomes (HR 0.93), supporting its established role in high-risk or sensitized recipients where potent T-cell depletion is warranted [10,11,32]. In contrast, IL-2R antagonists showed neutral associations with both graft failure and patient mortality, reflecting their appropriate application in lower-risk populations where safety profile may outweigh efficacy considerations [8,33,34]. Similarly, Alemtuzumab demonstrated neutral effects, consistent with prior reports indicating that its benefits may be limited to specific induction scenarios (8). Notably, combination therapy with ATG + IL-2R antagonists was associated with increased hazard for graft loss but not for patient death, suggesting potential immunologic redundancy or excessive immunosuppression from dual antibody exposure.
Recipient characteristics also exerted profound influence on long-term outcomes. Diabetes mellitus was the most potent adverse predictor, increasing the hazards of graft loss and mortality by more than 60%. This finding aligns with prior studies linking diabetic nephropathy and systemic metabolic inflammation to accelerated graft loss [18,35,36]. Older age, dialysis dependence, and retransplantation were similarly associated with increased hazards, reflecting cumulative vascular and immunologic injury in these populations [37,38]. In contrast, recipients of Asian and Hispanic ancestry demonstrated superior adjusted survival for both graft and patient outcomes relative to White recipients. This observation, replicated in prior registry analyses, may reflect complex interactions between pharmacogenomics, socioeconomic access, and immunologic adaptation [39]. The finding of modestly reduced mortality among Black recipients requires careful interpretation within the context of documented higher immunologic graft loss in this population, suggesting influences from strong selection factors and competing risks.
Among donor characteristics, a higher KDPI was associated with substantially elevated risk of graft failure and mortality, reaffirming the prognostic utility of this composite measure in organ allocation and risk counseling [40,41]. Donor age showed a statistically significant but clinically small association with both graft failure and mortality (HR ≈ 1.00 per year), consistent with donor age being a primary, though not exclusive, component of the KDPI score [40,42]. Donor terminal serum creatinine demonstrated a statistically borderline, inverse association with graft failure (HR 0.99, 95% CI 0.98–1.00, p = 0.027) and a neutral association with patient mortality (HR 1.00, p = 0.420). Although the graft-related association reached statistical significance, the extremely small effect size suggests this finding more likely reflects clinical allocation patterns, such as younger DCD donors with transient creatinine elevation rather than a physiologic benefit.
Donor diabetes was associated with modestly increased hazards for both outcomes (HR 1.05 each), a finding that is consistent with the established microvascular pathology observed in diabetic donor kidneys [43,44]. The modest effect size likely reflects the heterogeneity of diabetic donor organs; while some studies show excellent outcomes when diabetic donor kidneys are carefully selected [43], others document poorer survival when diabetes is long-standing or accompanied by marked histopathologic injury [44]. The present findings therefore reflect this heterogeneity, indicating a small population-level risk rather than a uniformly detrimental effect. Black donor race was also associated with slightly higher hazards of graft loss and mortality (graft HR 1.08; mortality HR 1.05). In contrast, Hispanic donor ethnicity conferred a small protective effect for graft failure (HR 0.96, 95% CI 0.94–0.99, p = 0.006). The biologic and sociodemographic underpinnings of these donor race-based associations warrant further investigation.
Transplant-specific factors, particularly prolonged cold ischemia time, were also associated with marginally increased hazards for both endpoints (HR ≈ 1.00 per hour, p < 0.001), underscoring the ongoing relevance of logistical efficiency and rapid organ revascularization in optimizing graft preservation [45,46]. Notably, after adjustment, kidneys from DCD donors demonstrated slightly lower hazards for graft loss (HR 0.91, 95% CI 0.89–0.93) and a neutral association with patient mortality (HR 1.01, 95% CI 0.98–1.04). This contrasts with unadjusted Kaplan–Meier findings and highlights the role of confounding factors, particularly donor age, ischemia times, and recipient selection in shaping observed outcomes.
Beyond these clinical associations, the present analysis introduces a novel dual-framework modeling approach that integrates classical Cox PH modeling with a suite of ML survival models. Prior transplant survival studies have typically employed either traditional Cox PH regression [17,19] or, more recently, small-scale ML models limited to single outcomes or older datasets [23,25,26,47]. To our knowledge, few if any national analyses have concurrently applied multiple ML survival algorithms including, XGB-Cox, CoxNet, SVM, and RSF alongside Cox model in a dataset exceeding 228,000 recipients and extending to 2024. This dual analytical framework provides both interpretability and predictive benchmarking, addressing the interpretability accuracy tradeoff that often limits ML adoption in clinical transplant research [20–22].
Across both outcomes, ML survival models achieved performance metrics comparable to or slightly exceeding the classical Cox model (C-index ≈ 0.69–0.71; mean tdAUC ≈ 0.71–0.73). While the marginal improvement in discrimination was modest, these results represent an improvement in predictive accuracy over earlier national registry analyses, where traditional Cox and tree-based ML approaches typically achieved C-indices of 0.63–0.68 [48,49]. Recent deep learning applications to Scientific Registry of Transplant Recipients (SRTR) data have similarly shown only modest improvements compared to their own baseline Cox models, with reported C-indices of 0.65–0.66 [50]. International efforts such as the Australian Registry study by [51] reported comparable performance for Cox and RSF models (C-index ≈0.67), reinforcing the observation that ML survival algorithms frequently offer incremental rather than transformative gains when applied to clinical registry data. The enhanced model performance observed in the present analysis likely reflects both methodological refinement and the use of a temporally expansive dataset extending to 2024, which captures contemporary shifts in donor utilization, immunosuppressive practice, and organ allocation. Collectively, the results affirm the continued value of Cox regression for clinical inference while demonstrating the feasibility and robustness of ML survival models as complementary tools for risk stratification in modern transplant research.
Strengths and Limitations
This study offers several important strengths. It leverages a large, contemporary national cohort spanning 2000–2024, providing exceptional statistical power and broad generalizability across diverse transplant populations. The dual outcome analysis examining both death-censored graft failure and patient mortality provides comprehensive insights into transplant success, allowing a more complete characterization of long-term transplant outcomes than studies limited to a single metric. A major methodological strength is the use of a dual analytical framework that integrates classical Cox PH modeling with multiple ML survival algorithms. This approach enables a direct comparison of inference-driven and data-driven methods, addressing a frequent gap in transplant analytics where interpretability and predictive performance are rarely examined in parallel.
These findings should, however, be interpreted in the context of certain limitations. The observational nature of this retrospective analysis limits causal interpretation, and the potential for residual confounding persists due to unmeasured variables including medication compliance, immunosuppressive drug levels, detailed biopsy results, and granular center-specific practice patterns. Furthermore, immunosuppressive therapy was assessed based on the regimen recorded at the time of transplantation, which may not reflect subsequent dose adjustments, medication switches, or discontinuations over the follow-up period. Finally, while the study captures long-term graft and patient survival with high completeness, it does not include other clinically relevant outcomes such as rejection episodes, patient-reported quality of life or specific adverse events related to immunosuppression.
Conclusion
In this large national analysis of deceased-donor kidney transplant recipients, maintenance regimens incorporating a CNI and MMF either as dual therapy or as part of a steroid-containing triple regimen, were consistently associated with superior long-term graft and patient survival compared with alternative combinations, reinforcing their status as the foundation of modern immunosuppressive therapy. T-cell–depleting induction with ATG demonstrated protective associations for both endpoints, whereas IL-2R antagonists and Alemtuzumab showed neutral effects. These results highlight the dominant influence of maintenance immunosuppression on long-term graft survival and emphasize the need for personalized induction strategies.
Beyond identifying clinical determinants of long-term outcomes, this study makes several methodological contributions. The comparative modeling framework revealed that the traditional Cox PH model achieved discrimination comparable to ML survival models, while providing superior clinical interpretability through HR estimation. This supports the continued primacy of Cox models for clinical inference in transplantation research, with machine learning serving complementary roles for specific prediction tasks requiring complex feature interactions.
This study advances kidney transplantation analytics through three principal contributions. First, it provides one of the most extensive and temporally comprehensive national evaluations of immunosuppressive therapy to date. Second, it introduces a comparative modeling paradigm that bridges interpretable hazard-based inference with predictive ML approaches, offering a practical template for future transplant analytics. Third, it highlights the translational potential of ML survival frameworks to support individualized risk stratification, particularly as transplant registries evolve to include richer clinical and biomarker data.
Future research should build upon these foundations by incorporating time-varying immunosuppressive exposures, therapeutic drug monitoring, center effects, and dynamic clinical variables. Integration of molecular, genomic, and digital biomarkers may ultimately enable the development of precision immunosuppressive strategies and refined prognostic tools that support personalized care throughout the post-transplant lifespan.
Author Contributions
Conceptualization: Kunle Timothy Apanisile, Naoru Koizumi
Methodology: Kunle Timothy Apanisile, Hadi El-Amine, Meng-Hao Li, Naoru Koizumi
Formal analysis: Kunle Timothy Apanisile, Meng-Hao Li
Writing – original draft: Kunle Timothy Apanisile
Writing – review & editing: Naoru Koizumi, Hadi El-Amine
Supervision: Naoru Koizumi, Hadi El-Amine, Meng-Hao Li
Funding
This study was partially funded by the National Science Foundation (NSFeIIS/ENG: SCH:/2123683).
Competing Interests
The authors declare that they have no competing interests.
Ethics Statement
This study used de-identified, publicly available registry data from the United Network for Organ Sharing (UNOS). Therefore, institutional review board approval and informed consent were not required.
Data Availability
All relevant data are available from the United Network for Organ Sharing (UNOS) database, subject to data access agreements.
Acknowledgments
The authors acknowledge that this work originated from the doctoral research of Kunle Apanisile under the supervision of Dr. Naoru Koizumi at George Mason University. The study was independently developed and refined by the authors for publication.
References



