
ABSTRACT
Chronic pain (CP) can profoundly strain family systems, yet few population studies have explored CP with high impact on families. We used 2023 National Health Interview Survey Data (n=29,522) to characterize CP with high impact on families of U.S. adults. Findings are: (1) the prevalence of CP with high impact on families (HICP-Family) is 4.4% in U.S. adults and 18.1% in U.S. adults with CP; (2) HICP-Family is almost exclusively reported by those who have high impact chronic pain (HICP) that limits their individual functioning in life and work; (3) yet, among those with HICP, not all (46.3%) report HICP-Family; (4) HICP-Family can feasibly be modeled as a latter transition stage in a tiered cascade of advancing CP-associated impacts; (5) there is a strong association between clinically significant mental health symptoms and HICP-Family; HICP-Family is six times more prevalent among those who screen positive for moderate-to-severe anxiety or depression symptoms. Families highly impacted by CP may not be adequately resourced for adaptive functional resilience. HICP-Family may form an underappreciated barrier to achieving optimal pain and mental health outcomes for people with HICP. Further, without intervention, members of families highly impacted by CP may face heightened susceptibility to onset of suboptimal pain and mental health trajectories of their own. The need to develop effective supports and promote adaptive resilience in families highly impacted by CP is clear. Clinical tools to support person-centered assessment of family and relational functioning, effective family-level interventions, and innovative models of care are needed.
IN BRIEF Establishes prevalence of chronic pain with high impact on families (HICP-Family); situates HICP-Family within emerging pain research frameworks.
1. INTRODUCTION
Chronic pain (CP) can profoundly impact family systems[75,76,96,97]. CP may challenge the family’s shared expectations[58,70,78,95,118] including who provides financial resources and emotional support [61,74], the conditions under which pain is considered a ‘legitimate’ rationale for functional limitations[14,75], and the acceptable forms, intensities, and frequencies of pain communications[33,48,49,116]. Research in mental health suggests the possibility of functional spillover effects as a mechanism for CP’s impact on families[71].
The gap between the family’s needs and their current reality greatly influences resilience to CP; mitigating factors can include the flexibility with which expectations are held, individual or interpersonal coping skills and supports, and the availability of financial and community resources promoting effective adaptation[30,41,42,52,63,66,97,119,123].
If the challenge presented by CP outmatches the family’s capacities and resources, relationships are likely to settle into dysfunctional patterns[4,38,42,97,113]. Families highly impacted by CP can be marked by cycles of emotional dysregulation and reactivity[16,17]; invalidation and stigma[33,129,130], catastrophic thinking[49]; frequent conflict[113]; role tension[2,115]; insufficient care and monitoring of children[126]; children acting as caregivers and surrogate parents [20,35,57,106,109,111]; dysfunctional regulation of relational closeness and distance[9,104,113,114]; overidentification with the subjective experiences of others[2,114]; infantilization of children and adults [84,98]; spousal and marital stress[62,74,122]; withdrawal from social networks and resultant isolation, loneliness, abuse or neglect[6,72,105]; and the suppression– or overly demonstrative expression of–anger, frustration, resentment, anxiety, despair, hopelessness, and pain[1,5,7,34,114].
Early pain socialization and family relational patterns are heavily intertwined: humans tend to express their pain to those with whom they feel relationally connected and from whom they anticipate the possibility of authentic experiences of care[2,18,30]. Maladaptive pain responses– overprotective/disempowering[19,21,40] or invalidating/dismissive[12,94]–to acute or chronic pain may frequently be associated with reduced or excessive family cohesion[93,107], marital dissatisfaction[74,92] and pain-attributed distress and disability[15]. Pain responses that effectively resolve the tension between acceptance and change may reduce pain intensity, [2,18,46] and build trust into the family system[60,133]. However, CP may also strain or upend previously positive patterns of communication and relational security[11,30]. Co-occurring mental health challenges may create a mutually reinforcing cycle with CP in families[8,11,25,26,31,73]. Family dysfunction is strongly predictive of pain-related disability and, like mental health, may confound the measurement of pain intensity[70,70,75,108].
Family members may blame themselves for being unable to soothe their loved ones’ pain[37]. They may feel that their supportive behaviors are not fully acknowledged nor reciprocated[3,65]; over time they may begin to experience burnout, resentfulness, and mistrust[137]. At the same time, people living with CP frequently report significant unmet needs for emotional validation and support and experience that they are being stigmatized, disbelieved, and isolated[94]. They may blame themselves for causing problems in the family and for the continuation of CP[22,69,88].
The clinical importance of CP’s impact on families is clear, yet few studies have explored population dynamics of CP with high impact on families (HICP-Family). We used 2023 National Health Interview Survey data to advance population-level understanding of HICP-Family in U.S. adults, aligning our analysis with emerging pain research frameworks that emphasize functional impact as a bridge between population and clinical studies[29,45,53,79,91,99,131].
2. METHODS
2.1 Study Design and Analysis Plan
We estimated the prevalence of U.S. adult chronic pain with high family impact as a proportion of the U.S. population and in millions of people. We evaluated the two-way interaction of chronic pain’s impact on individuals and chronic pain’s impact on families to assess whether family impact of pain is feasibly modeled as an advancement of functional impact beyond the individual. We then visualized the data as a cascade of functional impact in U.S. adults. Because high-impact pain in both individuals and families is so closely connected to mental health status[25,26,39], we estimated the prevalence of clinically significant anxiety and/or depression symptoms within each step in the CP-attributed functional impact cascade. Subsequently, we evaluated this relationship from the other direction, grouping the cascade by the presence/absence of clinically significant mental health symptoms a priori in order to examine and differences and commonalities between the two groups in terms of functional impact.
2.2 Data Source
We use data from the National Health Interview Survey (NHIS), a nationally representative, publicly available, deidentified data set suitable for calculating prevalence statistics about chronic pain in the noninstitutionalized U.S. adult population. The NHIS has been identified as the best data source for population-level surveillance of chronic pain[28]. Detailed information on the survey methodology has been published by the National Center for Health Statistics[90].
2.3 Measures
Chronic Pain (CP) was measured using the survey item “In the past 3 months, how often did you have pain? Would you say never, some days, most days, or every day?” Those who answered “Most days” or “Every day” were considered to have chronic pain, while those endorsing “Never” or “Some days” were considered not to have chronic pain. This is consistent with the International Association for the Study of Pain’s (IASP) definition of chronic pain as implemented in the International Classification of Disease (ICD-11)[121,136], and is the standard operationalization used by the National Center for Health Statistics.
High-Impact Chronic Pain (HICP) was measured using the survey item “Over the past three months, how often did your pain limit your life or work activities? Would you say never, some days, most days, or every day?” Those with chronic pain and who answered “Most days” or “Every Day” to this item were considered to have high-impact chronic pain (HICP); this is the standard operationalization used by the National Center for Health Statistics[77].
Chronic Pain with high impact on Families (HICP-Family) is a novel construct developed in this study. We operationalized HICP-Family using the survey item “Over the past three months, how often did YOUR pain affect your family and significant others? Would you say never, some days, most days, or every day?” For analysis of national prevalence (Tables 1 and 2), we considered those who answered “Most days” or “Every day” to this item to have chronic pain with high impact on families. For the analyses situating HICP-Family as part of CP-attributed functional impact cascade, the measurement of HICP-Family was constrained to U.S. adults who endorsed concomitant HCIP.
Anxiety and/or Depression Symptoms (A/D) were measured using two brief screeners for symptoms of anxiety and depression: 1) the General Anxiety Disorder-2 (GAD-2)[59], a validated brief scale used to screen for probable anxiety, and (2) the Patient Health Questionnaire-2 (PHQ-2)[67], a validated brief scale used to screen for probable depression. We operationalized positive screening results in line with the standard cut-points. Respondents who scored 3 or higher on the GAD-2 were considered to have anxiety symptoms[59]; respondents who scored 3 or higher on the PHQ-2 were considered to have depressive symptoms[68]. Survey respondents were coded as having anxiety and/or depression symptoms (A/D) if they scored greater than or equal to 3 on the PHQ-2 the GAD-2, or both.
2.4 Missing Data
Responses recorded as “Refused,” “Don’t Know,” or “Not Ascertained” in responses to questions used for the above measures were considered missing data. Missing data for questions used to operationalize chronic pain CP, HICP, HICP-Family, and A/D included a total of 1101 observations, representing 3.7% of overall data. Complete case analysis was used.
2.5 Analysis Details
Population prevalence and population mean estimates presented in all tables and figures were calculated using SAS statistical software version 9.4 accounting for the stratification, clustering, and weighting procedures of the complex NHIS survey design.
3. RESULTS
An estimated 4.4% [95% CI: 4.1, 4.7] of the U.S. adult population—18.1% of U.S. adults with CP—report HICP-Family (Table 1).
If high impact of chronic pain on families could be feasibly conceptualized as an advancement in pain’s impact spilling over from the individual and into the family system, we would expect to see few respondents endorsing HICP-Family who did not concomitantly endorse HICP. We explored the interaction of HICP and HICP-Family (Table 2). Just 2.1% of U.S. adults with chronic pain endorsed high family impact without also endorsing HICP; the small amount of non-conforming data suggest the empirical feasibility of modeling HICP-Family as an advancement of chronic pain’s functional impact beyond the directly affected individual.
Next, we tabulated and visualized model-conformant data (100% - 2.1% = 97.1% of data was conformant) as a tiered “cascade” of advancing functional impact (Table 3, Figure 1). The presence of high-impact pain did not deterministically predict high family impact: fewer than half (46.3% [95% CI: 44.1%, 48.5%]) of U.S. adults with high-impact chronic pain endorsed high family impact. Among all those who endorsed high family impact of chronic pain, 88.5% [95% CI: 86.4%, 90.6%] concomitantly endorsed HICP.

Prevalence of chronic pain (CP) and associated impacts in U.S. adults: a tiered cascade of advancing functional impact
Data Source: National Center for Health Statistics, National Health Interview Survey, 2023
Because the literature so closely links the impact of chronic pain with mental health status[25,26,39], we estimated the prevalence of clinically significant anxiety/depression symptoms within each step in the functional impact cascade (Table 4):
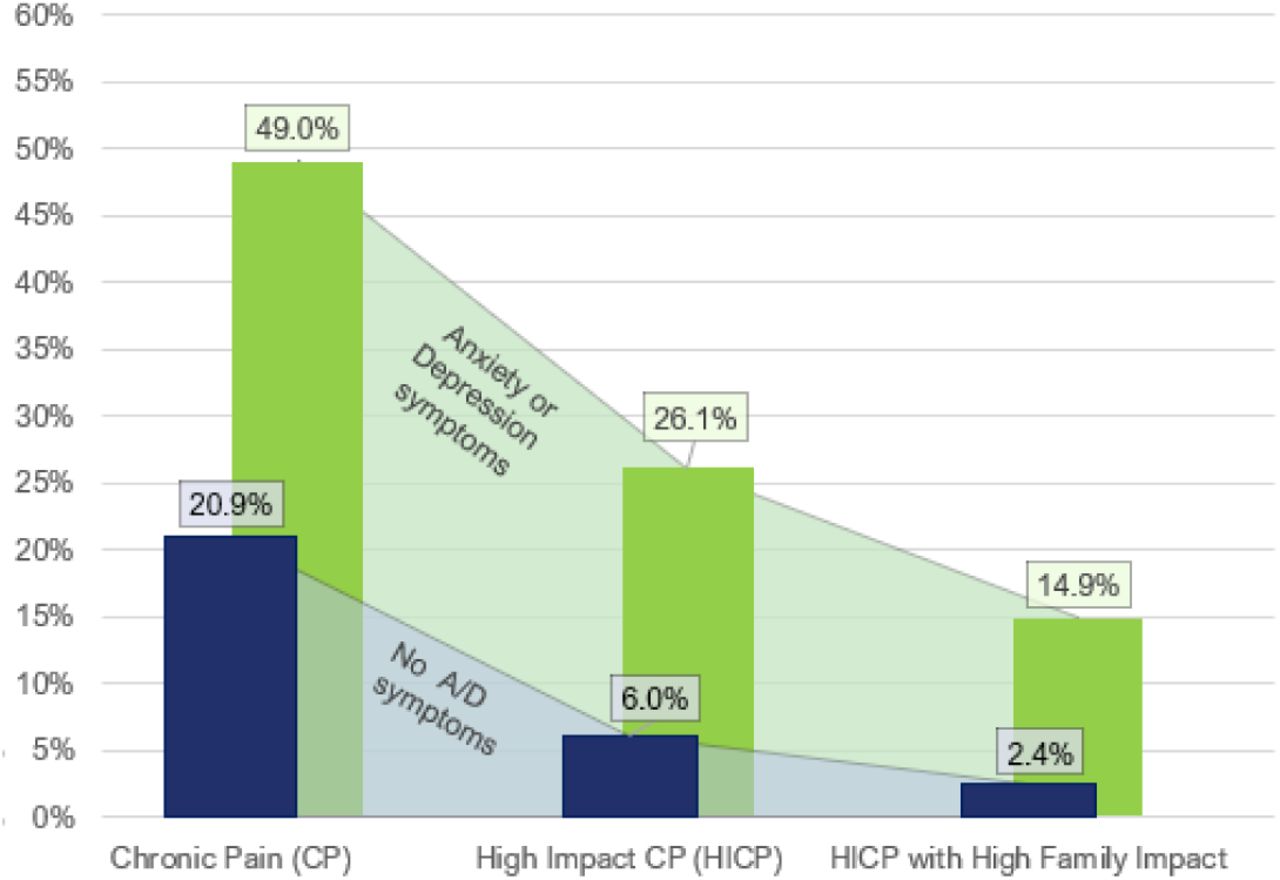
To further assess the intersection of A/D with CP, HICP, and HICP-Family, we separated the functional impact cascade into two groups based on positive/negative screening for clinically significant anxiety and depression symptoms (Figure 2, Table 5). The prevalence of chronic pain and CP-attributed impact on individuals and families is markedly elevated in those who screened positive for A/D symptoms compared to others. The magnitude of this disparity increases exponentially as functional impact advances: CP is (49.0%/20.9%) =2.35 times more prevalent in those with A/D. HICP is (26.1%/6.0%) = 4.35 times more prevalent in those with A/D; and family impact of pain is (14.9%/2.4%) = 6.20 times more prevalent in those with A/D (Figure 2, Table 5).

Prevalence of chronic pain (CP) and associated impacts as a proportion of U.S. adults: modeled as a tiered cascade of advancing functional impacts, grouped by presence of clinically significant anxiety/depression symptoms
Data Source: National Center for Health Statistics, National Health Interview Survey, 2023
4. DISCUSSION
Pain is mainly communicated and attended to in families; families are a primary building block of communities; community-level disparities in chronic pain may likely be reinforced and maintained through its unequal concentration in families, across geographies and generations. Health conditions associated with chronic pain may run in families biologically and/or environmentally, such that families experience repeated burden of similar types of pain at similar points in the life course[117]. Family systems already highly impacted by CP may be under-resourced to provide caregiving and support to family members; evidence suggests that these family members may become especially susceptible to onset of their own suboptimal pain and mental health trajectories[24,55,55,86,117,124].
The degree to which the chronic pain of U.S. adults impacts their family systems has not been well characterized. The present study represents an initial step in advancing population-level understanding. We estimated that 11 million U.S. adults, 4.4% of the U.S. adult population, report chronic pain that affects their families most days or every day (HICP-Family) U.S. adults whose chronic pain has high impact on their family make up 18.1% of all U.S. adults living with chronic pain. (Table 1).
We found no empirical difficulty in aligning HICP-Family with the field’s general effort to capture and catalogue dynamic temporal transitions in pain’s functional impact. HICP could be conceptualized as a necessary, but not sufficient, condition—fewer than half (46.3%) of U.S. adults with HICP endorsed high family impact (Figure 1, Table 3). The data are consistent with conceptualizing HICP-Family as a distinct transition in CP impact: representing unmitigated advancement of CP-attributed functional limitations in the individual and creating spillover impacts on family systems (Table 2). Finally, we documented (bidirectionally) the association between anxiety/depression and chronic pain’s functional impact cascade. Clinically significant anxiety and depression symptoms were increasingly prevalent at each subsequent step in the chronic pain impact cascade: among all U.S. adults, the prevalence of clinically significant anxiety/depression symptoms is 12.0%. In U.S. adults with CP, 24.4% have A/D symptoms; among U.S. adults with HICP, 37.1% have A/D symptoms; and among U.S. adults with HICP-Family, 46.1% have A/D symptoms (Table 4). Upon reversing the contingency and comparing the functional cascade among those with A/D to those without A/D, we found that the prevalence of chronic pain and downstream functional impact is markedly higher in those with anxiety/depression symptoms compared to others and that the magnitude of the disparity between those with and without A/D increases exponentially as functional impact increases (Figure 2, Table 5).
Despite calls for family-oriented approaches to the treatment of chronic pain by leaders in the field[96], relatively little research has addressed family functioning. This gap is particularly striking in the context of adult chronic pain. Validated, person-centered, culturally resonant approaches to the assessment of family (and individual) functioning are needed[43]. Measurement of family functioning will not be an easy task: chronic pain can have complicated, significant, and widespread impacts across family systems, and it does not restrict its impact to direct caregivers of people living with pain. Chronic pain impacting those who would otherwise be involved in providing care reduces the family’s collective caregiving resources. In this way, family dependents who are not affected by pain, such as children, older family members, and those with disabilities, may suffer lack of care, due to a family member’s reduced capacity to provide it. High-impact parental pain can advance profound adversity on children; these children’s experiences are similar to those reported by children of parents with mental illness and/or substance use disorders[124,125]. The siblings of children with high-impact pain may experience that parents/guardians are distracted and emotionally taxed; the entire family may become primarily focused on the needs of the child with pain. Grandparents and other extended family members who have high-impact pain may be limited in their social engagement and caregiving to children. Family members who do not require caregiving can suffer as well: Pain may put enormous financial and emotional stress on spousal partners and others who pick up the slack created by reductions in the productive capacity of the family unit. Mid-life caregivers of elders with high-impact chronic pain may often be pulled between providing care for the generation above and the generation below, particularly in communities where elder caregiving is culturally expected[44]. In some cases, family conflict related to chronic pain may catalyze estrangement. Providing care for people with high-impact pain may not be as health-promoting as receiving it. It is possible that caregivers of people with chronic pain neglect their own health to focus on their family member. Finally, many families will have more than one individual living with high-impact chronic pain. Research to address family impact of pain will need to grapple with these complexities.
In pain research, family members are often categorized with a binary valence: as a resource promoting resilience, or as a negative influence that may require being “worked around”, clinically. In addition to focusing on attributes (positive and negative) of the individuals and observing pain-related interactions, emerging research exploring the jointly held interactional quality and networked structure of relationships –including but not limited to the context of pain[13,100,127,128,133,134] –may be a productive research direction moving forward.
Outcomes for both chronic pain and mental health are heavily associated with perceived availability of social support[132]. Involving families in treatment, particularly in communities with heavy burden of chronic pain and CP-attributed impacts, may be a more efficacious approach compared to treatment as usual–which considers patients primarily as individuals[13,51,80,81]. Interventions provided by behavioral health peer and family recovery support specialists may offer an opportunity to develop family-systems interventions and natural supports[82,83], particularly in communities affected by shortages of behavioral health care providers. Increased engagement of psychosocial and occupational rehabilitation professionals in multidisciplinary pain care could also be beneficial. As a non-limiting example, occupational therapists may often place less emphasis on a joint’s range of motion, and more emphasis on the adaptive resilience of a human’s daily life, leveraging patients’ innate drive for mastery [50,110,112]. Adaptive recovery of meaningful, self-directed lives is critical to the recovery and sustained resilience of individuals and their families; the effective and adaptive functioning of family systems could become a high-value endpoint for future research.
5. LIMITATIONS
Several limitations are noted. First, persons with no permanent address, persons living on military bases, U.S. expatriates, and individuals residing in long-term care institutions, and correctional facilities are not represented in the NHIS. Second, the 2023 NHIS adult dataset included only the brief forms of the screeners for depression and anxiety; though these have been shown to be viable alternatives to the GAD7 and PHQ-8[56], it is still possible that using the brief form could in some way influence the measurement of anxiety/depression. The NHIS measures the impact of the respondent’s pain on the family, as perceived by the respondent, however, not all individuals may easily recognize the impact of their pain on their family, which could lead to undercounting the true prevalence. Ideally, information on family impact would be collected from family members themselves. Last, contextual information such as how many family members are affected by a respondent’s pain, whether they see themselves as caregivers, care receivers, or some other relationship, whether they currently cohabitate with the respondent, and whether respondents have experienced CP-associated family estrangement, are unavailable in the NHIS public use files, limiting disentangling of cohabitation versus kinship and preventing a more nuanced analysis of the subjective meaning respondents attributed to the survey item concerning family impact of pain.
6. CONCLUSION
“Try imagining a place where it’s always safe and warm / Come in, she said / I’ll give ya, shelter from the storm” --Bob Dylan
Chronic pain is indeed a ‘sensitive barometer of population health’[135] that is disproportionately prevalent in under-resourced and stigmatized individuals, families, and communities[10,64,102,103,120,135]. It is perhaps less widely understood that among individuals living with chronic pain, vulnerability to high-impact functional limitations also exists along a social, cultural, relational, and psychological gradient[23,27,32,36,47,54,77,85,87,89,101]. We suggest that HICP-Family could play an underrecognized role in maintaining feedback loops of anxiety/depression, functional limitations, and chronic pain.
More research is needed to understand transitions in functional impact: including the predictors of transitions from CP to HICP, and the transition from HICP to HICP-Family. To better understand HICP-Family, tools supporting person-centered clinical assessment of family and relational functioning are needed. Investment is needed to learn what can be done to prevent or reverse the spillover effects of CP-associated functional limitations (HICP) on family systems. Helping CP-compromised families to recover represents a meaningful opportunity in improving quality of life for millions of children, adults, and older people who are directly and indirectly affected by high-impact chronic pain, and potentially in addressing recalcitrant disparities across clinical and sociodemographic subpopulations.
Data Availability
No original datasets were generated over the course of this study, all data used in this study are publicly available at: https://www.cdc.gov/nchs/nhis/documentation/2023-nhis.html
7. ACKNOWLEDGEMENTS
Many on our co-author team have had important experiences with their own or a family member’s pain. Our professional activity as clinicians, scientists, and communicators is usefully informed by this experiential expertise. We acknowledge Sally W. Schultz, PhD, OTR, LPC, and Professor Emerita at Texas Woman’s University, and Doreen DeRoss, LPC, for several helpful conversations informing our thinking on pain and families. Funding for this study was provided by the Comprehensive Center for Pain & Addiction at the University of Arizona Health Sciences. The authors have no conflicts of interest to declare. No original data sets were generated over the course of this study; the data used in this study are publicly available on the National Health Interview Survey website.
REFERENCES
- [1].↵
- [2].↵
- [3].↵
- [4].↵
- [5].↵
- [6].↵
- [7].↵
- [8].↵
- [9].↵
- [10].↵
- [11].↵
- [12].↵
- [13].↵
- [14].↵
- [15].↵
- [16].↵
- [17].↵
- [18].↵
- [19].↵
- [20].↵
- [21].↵
- [22].↵
- [23].↵
- [24].↵
- [25].↵
- [26].↵
- [27].↵
- [28].↵
- [29].↵
- [30].↵
- [31].↵
- [32].↵
- [33].↵
- [34].↵
- [35].↵
- [36].↵
- [37].↵
- [38].↵
- [39].↵
- [40].↵
- [41].↵
- [42].↵
- [43].↵
- [44].↵
- [45].↵
- [46].↵
- [47].↵
- [48].↵
- [49].↵
- [50].↵
- [51].↵
- [52].↵
- [53].↵
- [54].↵
- [55].↵
- [56].↵
- [57].↵
- [58].↵
- [59].↵
- [60].↵
- [61].↵
- [62].↵
- [63].↵
- [64].↵
- [65].↵
- [66].↵
- [67].↵
- [68].↵
- [69].↵
- [70].↵
- [71].↵
- [72].↵
- [73].↵
- [74].↵
- [75].↵
- [76].↵
- [77].↵
- [78].↵
- [79].↵
- [80].↵
- [81].↵
- [82].↵
- [83].↵
- [84].↵
- [85].↵
- [86].↵
- [87].↵
- [88].↵
- [89].↵
- [90].↵
- [91].↵
- [92].↵
- [93].↵
- [94].↵
- [95].↵
- [96].↵
- [97].↵
- [98].↵
- [99].↵
- [100].↵
- [101].↵
- [102].↵
- [103].↵
- [104].↵
- [105].↵
- [106].↵
- [107].↵
- [108].↵
- [109].↵
- [110].↵
- [111].↵
- [112].↵
- [113].↵
- [114].↵
- [115].↵
- [116].↵
- [117].↵
- [118].↵
- [119].↵
- [120].↵
- [121].↵
- [122].↵
- [123].↵
- [124].↵
- [125].↵
- [126].↵
- [127].↵
- [128].↵
- [129].↵
- [130].↵
- [131].↵
- [132].↵
- [133].↵
- [134].↵
- [135].↵
- [136].↵
- [137].↵




{kind=link}
{kind=link}