
Abstract
Background Cystic echinococcosis (CE) is a widespread neglected zoonotic disease caused by Echinococcus granulosus sensu lato (EG) with a global burden of control in the billions of dollars. E. granulosus’ life cycle involves definitive, intermediate, and humans as dead-end hosts. Echinococcosis control programs use strategies that focus on any of these hosts. We aimed to provide a comprehensive and up-to-date overview of the EG control interventions worldwide.
Methods We conducted a scoping review by mapping all studies on interventions for EG control following the Arksey and O’Malley Framework. We screened identified articles, and charted and coded selected papers. We classified the data based on target host, type of study, and control mechanism. We described the efficacy or safety outcomes, and the associated barriers/facilitators for the intervention. Critical appraisal was conducted.
Results From 7,853 screened studies, we analyzed 45: seven centered on human interventions, 21 on animals, and 17 on both. Studies on humans focused on educational strategies and human CE monitoring. The studies on animals were field trials and most were based on Praziquantel (PZQ) for dogs. Studies focused on both animals and humans had, in general, more participants, lasted longer, and covered larger geographical areas. Overall, the quality of studies was moderate to low.
Conclusions Available evidence suggests that long-term interventions aimed at both animals and humans can achieve significant reduction in EG transmission, particularly when PZQ treatment for dogs is included. Higher quality evidence, standardization of methodologies, and better reporting on post-intervention outcomes are necessary for drawing stronger conclusions. Further evidence is needed to assess the sustainability and scalability of control measures. Nonetheless, an integrative One Health approach is essential for overcoming the multiple challenges associated with sustaining long-term control efforts for Echinococcosis.
Funding RCN was supported by the National Institute of Allergy and Infectious Diseases (grant nos. K01AI139284 and R01AI168291). LOC, JAB, and RCN was supported by the Fogarty International Center (grant no. D43TW012741).
Author Summary Cystic echinococcosis is a disease caused by the parasite Echinococcus granulosus sensu lato. This parasite can be found in specific areas on all continents, especially in poverty-stricken regions, increasing costs and losses. Some countries have achieved control, but most are still in the process. Our review provides a clear picture of what we currently know about these control strategies and points out where more research is needed. It highlights how the findings can improve control practices by showing what works best and address practical challenges. The review also identifies gaps in current knowledge and suggests that comparing different control methods could help find the most effective and cost-efficient solutions.
Key areas needing attention include increasing support and funding for echinococcosis, as the disease is often overlooked. More research from different fields is needed to better understand and manage the disease’s complexities. Better and ongoing surveillance is crucial for maintaining effective control strategies. Finally, comprehensive reviews that bring together findings from different studies are needed to identify what works best and improve and combine future control efforts.
Introduction
Cystic echinococcosis (CE) is a zoonotic disease caused by the tapeworm Echinococcus granulosus sensu lato (EG)1–3. CE is most prevalent in the Mediterranean area, Eurasia, North and East Africa, and South America, where the dissemination is closely linked to home sheep slaughtering and dog feeding raw viscera4–7. However, human CE cases are also reported in the USA8, Canada9,10, Europe11,12, and Japan13. High infection rates among dogs, coupled with socioeconomic and ecological factors, lead to extensive human exposure14–16. The global burden of CE includes 184,000 disability-adjusted life years (DALYs) annually, human-associated economic losses of $764 million per year17, and a global cost for controlling the disease in animals and humans estimated at $3 billion3. Inadequate reporting of CE cases due to poor surveillance is also common globally and prevents accurate estimates of the burden of disease18. Despite its widespread distribution and significant global impact on human health, CE is considered a neglected tropical disease, more specifically a neglected zoonotic disease (NZD)19–21. CE does not receive enough attention and funding, which results in limited research efforts compared to other diseases. EG transmission involves mainly canines and ruminants, so research initiatives and intervention approaches are hindered by intersectoral work, complexities associated with ecological factors, and intricate economics related to animal husbandry22. Controlling NZDs offers a cost-effective chance to reduce poverty in rural regions where they are most prevalent23. Rural determinants of health involve social, psychological, economic and spiritual aspects that should be specifically addressed in control strategies24.
EG has a complex life cycle involving definitive hosts, intermediate hosts, and humans as dead-end hosts3,25. Intermediate hosts, primarily herbivores like sheep, develop larval cysts in organs such as the liver and lungs after ingesting pastures contaminated with parasite eggs. Definitive hosts, typically domestic or wild canids, become infected by consuming the organs of intermediate hosts containing these cysts3,25. In hyperendemic regions, it is common for humans to reside closely with livestock and shepherd dogs, sharing water from natural sources; however, the evidence supporting infection through contaminated water is tenuous26–31. In these areas, the infected shepherd dogs become the primary source of infection for both humans and livestock6,15.
CE control programs primarily aim to stop the transmission of the causative agent to the hosts18,32. Strategies targeting definite or intermediate hosts may include regular dog deworming33,34, dog population control35,36, improved management of infected viscera37, sheep vaccination38, health education programs39, epidemiological surveillance strategies40–42, improvement of diagnostic tests and infrastructure19,43, and integrative One Health initiatives44, among others. However, a common barrier to effective control programs is the lack of sufficient information needed to design, implement, and evaluate them.
A literature review is essential to identify the effective components of control and elimination interventions, aiding in strategy development and policy formulation. We conducted a comprehensive literature review, using a scoping review methodology, a useful tool in the arsenal of evidence synthesis approaches45. Our goal was to identify the scientific rationale, objectives, and efficacy of various interventions, providing a current overview of the current status of EG control interventions worldwide. This study provides new insights for future research and public health efforts for CE control.
Methods
The protocol of this review is registered on the Open Science Framework (www.osf.io) with DOI 10.17605/OSF.IO/48AZR. We mapped all available evidence on interventions for EG control. We followed the Arksey and O’Malley Framework consisting of five stages: (i) Identifying the research question, (ii) Identifying relevant studies, (iii) Study selection, (iv) Charting the data, and (v) Collating, summarizing and reporting the results46,47,45,48,49.
Identifying the research questions
With this review we aimed to (i) map all evidence available regarding field interventions looking to control, reduce or eliminate echinococcosis in endemic areas and, (ii) identify research gaps that can lead to future studies and, potentially, successful interventions. The following questions guided this review:
What strategies have been implemented, piloted, or tested to reduce, control, or eliminate EG infection in animals and/or humans?
What was the rationale for the study/intervention?
Who/what were the targets?
What barriers and facilitators were encountered?
For each intervention found in question 1
What was the efficacy/effectiveness outcome?
Was there any safety metric/outcome?
How long has the program/intervention worked? Is it still in place?
What kind of modifications/changes has the intervention undergone over time?
Identifying relevant studies
We initially outlined a search strategy for databases and search engines for published data, followed by reference scanning and gray literature search for unpublished or difficult-to-find studies. For published data, we included MEDLINE (via PubMed), EMBASE, SCOPUS, Web of Science, Global Index Medicus and Google Scholar. The search strategy was outlined by the research team with the support of a librarian. (Appendix 1: search strategy) The search included all studies until May 2024. The results from all searches were imported and organized in Covidence™ (Melbourne, Australia), a web-based software platform that streamlines the literature review process.
Study selection
We included all available evidence, including published, preprint, or gray literature, evaluating interventions to reduce, control, or eliminate echinococcosis by EG infections in animals and humans. Our search was global; we did not restrict studies by region. We included publications in English, Spanish, and Portuguese. Studies that included vaccines as components of field interventions were included. However, studies whose primary endpoint was to evaluate the efficacy of vaccines or deworming treatment under controlled conditions were considered out of the scope of this review and were excluded.
We screened the articles in two stages: first, by titles and abstracts, and second, by full-text. Titles and abstracts were imported into Covidence™ where reviewers assessed eligibility and filtered duplicates. The final list was evaluated by two pairs of reviewers. Both screening processes were preceded by a pilot to compare the results of the review teams, align criteria, and discuss discrepancies to reach a consensus. For quality appraisal, we used the Mixed Methods Appraisal Tool (MMAT) which allows the evaluation of multiple types of studies50.
Data charting, synthesis, and reporting results
We used an electronic form/Excel® spreadsheet developed by the research team for the full-text stage for reviewers referencing, tracking, and documentation of excluded studies. Key information recorded included, but was not limited to, author(s), year of publication, methodology, and intervention characteristics. We piloted the abstraction chart to assess consistency between reviewers and calibrate the chart if needed.
The included papers were divided into types of intervention and classified according to the associated control mechanism (elimination of parasites, population control of hosts, and management of sick human/animal population, among others) and their target host. For each type of intervention, we described the efficacy or effectiveness and the safety outcome, if available, and the associated variables and the barriers/facilitators found. The results are presented in figures and tables. For studies with qualitative results, a synthesis of the main variables is presented.
Quality appraisal
We used the Mixed Method Appraisal tool (MMAT), which allows for the appraisal stage of reviews that include qualitative, quantitative and mixed methods studies. It presents two general questions followed by five sections corresponding to different study designs, each section having five questions that evaluate quality criteria50,51. Each question can be answered as “yes”, “no” or “can’t tell”. The “yes” is considered as the fulfillment of the criterion. The tool does not present a cut-off point, so the score of the studies was presented descriptively as suggested by Reporting the results of the MMAT (version 2018)52 as follows:
5***** or 100% quality criteria met
4 **** or 80% quality criteria met
3 *** or 60% quality criteria met
2 ** or 40% quality criteria met
1 * or 20% quality criteria met
In the case of mixed studies, we followed the recommendation of the MMAT manual: we asked a total of 15 questions (5 questions for qualitative studies, 5 for quantitative studies and 5 for mixed studies) and considered the lowest score as the overall quality score.
Results
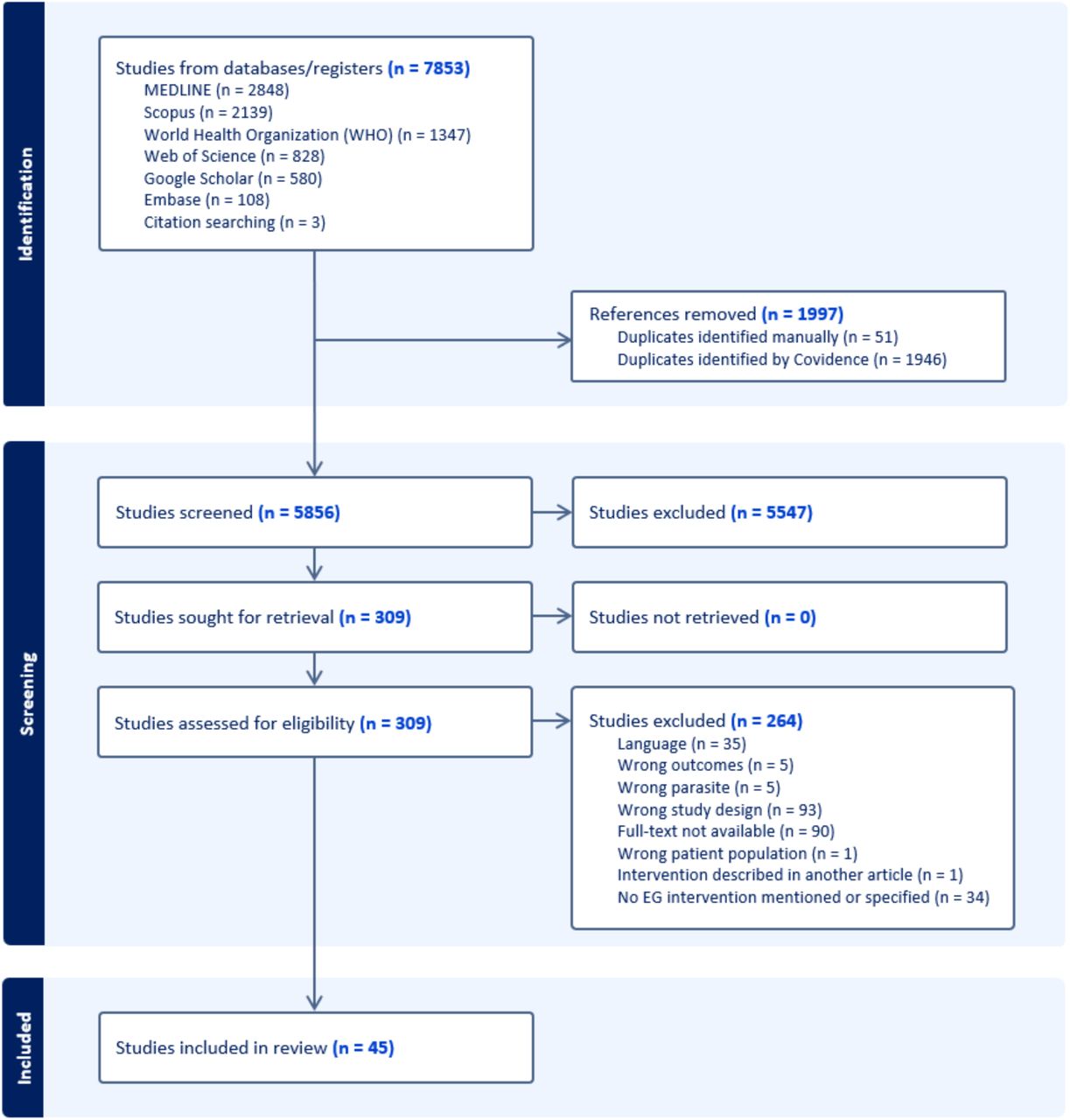
We found a total of 7,853 potentially relevant studies, with 2,848 from MEDLINE, 2,139 from Scopus, 1,347 from WHO, 828 from Web of Science, 580 from Google Scholar, 108 from Embase, and 3 from gray literature. A total of 1997 duplicates were removed either manually or identified by Covidence. After screening the titles and abstracts, 309 met the eligibility criteria. Subsequently, 264 studies were excluded during full-text review, and finally, 45 studies were included in this scoping review (Fig 1). We mapped these studies across various regions globally, as depicted in Fig 3. Most of these studies were conducted in Argentina and China (n=7, each), where there are high endemicity areas. Other highly endemic areas such as Turkey and Kenya have been the subject of at least one study each. However, several other hyperendemic regions around the world have yet to be represented in the literature.

Interventions in humans
Of the 45 articles reviewed, seven studies reported interventions aimed only at humans (Table 1a). Six studies primarily focused on education and awareness and one study focused on CE monitoring. In Portugal, a 13-year program unveiled 62 CE cases via ultrasound, 24 cases via serology, and 21 cases via both. Health information was provided to adults, with specific activities designed for children. CE prevalence decreased by 20% midway through the study and by the end, feeding raw viscera to dogs dropped from 60% to 20%53. In Peru, nine educational sessions were applied to 28 school children. A high-level knowledge of CE increased from 50% to 100% in the intervention group54. In Chile, a 7-level educational intervention run over 4 years for 3,145 participants aged 2 to 20 improved knowledge at all levels. Compared to urban, rural schools showed greater improvement. The biggest changes were in knowledge about hand washing, washing fruits and vegetables, and avoiding dog licking. Knowledge of responsible dog ownership was highest before the intervention and showed the least change55. In the USA, a 73-item questionnaire was applied to evaluate an educational program, including knowledge and the willingness to engage in preventive actions. In 8 years, awareness increased from 28% to 83%56. In Turkey, awareness interventions were applied to children, the general public, and health care professionals. In children, knowledge increased from 5.8% to almost 90%. No efficacy measure is provided for adults39. In Morocco, an integrated health messaging intervention was implemented including EG, rabies, and other zoonoses. “Piggy-backing” on high priority diseases like rabies allowed participants to better retain information on EG57. In Argentina, an ultrasound monitoring trial in humans was implemented to support a comprehensive control program. The trial revealed that prevalence reduced from 5.5% to 4.04%. Additionally, high-risk groups were identified and this evidence informed program actions58. Details about these interventions focused on humans are found in Table 1a.
Interventions in animals
We reviewed 21 articles of interventions aimed only at animals (Table 1b). Six interventions targeted both dogs and sheep, 12 targeted only dogs, and 3 only sheep. Most studies were based on the delivery of Praziquantel (PZQ). In Australia, an intervention included testing dogs, treating positive dogs with bunamide at days 0 and 14, and recommendations for home slaughtering. The incidence in dogs dropped from 11.3% to 2.1% in a 4-year period59. In Uruguay, different PZQ frequencies in dogs were compared. One year of PZQ treatment every 6 weeks reduced the prevalence in lambs to 0, while in the 12- and 16-week schemes, as well as in the control group, the prevalence ranged from 4.3 to 18.6%60. Also in Uruguay, a PZQ-based 9-years control program in dogs reduced the prevalence in dogs from 22.7% to 1.5% and, in 4-year-old sheep from 49.3% to 18.5%61. Similarly in Brazil and China, dogs that were treated with PZQ every 30 days had their prevalence reduced from 10.67% to 0.74%62 and from 7.3% to 1.7%63 respectively. In Peru, an interesting PZQ regimen was implemented: two treatment cycles were administered to dogs with a 12-month interval between them. In each cycle, dogs received three doses of PZQ, one dose per month. Prevalence in dogs reduced from 47.2% to 1.3%. Unfortunately, prevalence was only evaluated once one month after the last dose64. In Argentina, a control program that started in 1980 had multiple modifications. It began with an EG baseline for dogs, sheep, and the environment. Later lambs received EG95 vaccine and multiple boosters. Female sheep got an extra dose for colostral immunity. After 3 years, prevalence in sheep dropped from 26.2% to 7.8%65. This program, updated in 2009, was later evaluated through copro ELISA in dogs, necropsy of adult sheep, and ultrasound screening in children. By 2017, infection in 6 y.o. sheep decreased from 56.3% to 21.6%, in dogs from 9.6% to 3.7%, and in children from 38 cases to only one66. In the same program, between 2018-2022, in addition to EG95 in sheep, dogs were treated with PZQ 4-times a year. Prevalence among vaccinated and unvaccinated sheep was 21% and 66%, respectively67. In Chile, a neighboring country to Argentina, a 3-year program vaccinated sheep with EG95 vaccine at 2 and 3 months old, and then annually. By the end of the program, cyst fertility dropped from 28.1% to 8%68. Another multi-pronged intervention was conducted in Morocco, a 4-year program compared PZQ for dogs every 4 months, EG95 vaccination of lambs, and both combined. Dog prevalence dropped from 35% to 9%. Post-intervention, the prevalence of viable cysts in sheep was 5% with combined intervention, 8% with sheep vaccination, 69% with dog treatment only, and 77% with no intervention69.
Cyprus and Norway provided data from a hypoendemic areas. In Norway, dogs were treated with PZQ biannually first and annually in the following years. After 4 years, the prevalence in reindeer reduced from 1.5% to 0.11%70. In Cyprus, infected livestock were identified in slaughterhouses, dogs were tested using arecoline and Copro ELISA, and infected dogs were euthanized and examined or treated with PZQ. Sheep prevalence reduced from 0.033% to 0.007%71. Several studies did not report efficacy metrics or reported negative results. In Kenya, a 16-month control program included dog population control, administering arecoline, and treating infected dogs with PZQ every six weeks. Prevalence reduced but remained high and returned to pre-control levels within three months72. In Kyrgyzstan, dogs were treated with PZQ four times for a year. Pre-intervention copro ELISA prevalence was 20.1%; however, post-intervention prevalence was not reported73. In China, multiple studies have been reported. Baits with PZQ were tested to treat dogs and other canids every other month; however, after 7 months, no significant effect was detected in high-prevalence areas74. In Buddhist areas, where dog culling is not accepted, administering PZQ twice a year for five years reduced EG prevalence in dogs only from 27% to 20%75. In a different study, after 3 years of implanting slow-released PZQ-medicated bars in dogs, copro ELISA positivity in dogs plummeted from 41.2% to 3%, seropositivity in children reduced from 41.2% to 5.4%, and prevalence in sheep dropped from 44.8% to 10.7%76. Some interventions have explored innovative approaches. In China, smart collars enabled automatic delivery of PZQ baits to dogs. Collars also had sensors to provide real-time data that could be used to study trends of echinococcosis. Post-intervention prevalence was not provided77. In Italy, carcass disposal was enhanced through vulture feeding stations. CE prevalence in sheep was 65.3% and, though no post-intervention estimates are provided, the authors concluded that the program reduced CE risk and burden78. Also in Italy, GPS data loggers were attached to a sheep leader and two shepherd dogs to delimit grazing areas. Grazing areas’ perimeters were baited with anthelmintics for free-roaming dogs, proposing another method of control79. Details of these interventions focused on animals can be found in Table 1b.
Interventions in animals and humans
We reviewed 17 articles focused on both animals and humans (Table 1c). Multiple long-term programs and short-term studies are reported from South America and described integrated interventions dosing dogs, vaccinating sheep, educating and screening humans, and enhancing abattoir surveillance. In Argentina, dogs received PZQ more frequently in high-risk areas and were monitored using arecoline and in-situ analysis. Education was provided to schools, homes, and to rural populations through accessible media. Sheep were inspected at abattoirs and surveillance data collection improved. After two years, dog prevalence decreased from 31.5% to 4.24%80. After 17 years of implementation, new human cases in children under 11 decreased by 77%81. Also in Argentina, ultrasound surveys in children and copro ELISA surveys in dogs were used to identify hotspots of transmission and strengthen control program activities (education, diagnosis and treatment in humans, deworming of dogs, and vaccination of sheep). Dog prevalence reduced from 32% to 15.6%82. In Uruguay, a rural intervention included monthly PZQ plus broad-spectrum anthelmintics 1 to 3 times a year, copro ELISA diagnosis, free dog castration, and ultrasound diagnosis for people. Ultrasound training and EG education were provided at health centers and routine surveillance was conducted in abattoirs. Over five years, dog prevalence dropped from 10% to 1.6%35. In Chile’s Aysen region, from 1982 to 2001, dogs were usually dosed every 6 weeks. Human prevalence decreased from 75% to 32% and sheep prevalence from 90% to 9%. In 2020, sheep vaccination was added, and surveillance was enhanced by examining sheep cysts and by communities reporting cysts via WhatsApp. Cyst size was negatively correlated with vaccination status83. In another study in Chile, infected dogs were identified and treated with PZQ. Health education was provided to farm family members, and they were asked to pledge to educate their neighbors, to practice what was learned, to buy PZQ as a group for their dogs. Serology was conducted on dog-owners. Unfortunately, only pre-intervention prevalence was reported84. In the US, a decade-long control program in Utah involved PZQ treatment for dogs (frequency unspecified), educational initiatives through press releases, filmstrips, and children’s coloring books, diagnostic clinics for humans and dogs, and surveillance and proper disposal of viscera at abattoirs. Over seven years, infection rates in dogs dropped from 28% to 1%, but later rose to 10% due to some dog owners’ noncompliance. Concurrently, EG infection in sheep steadily declined, and public knowledge about the disease significantly increased85.
Studies and programs from other parts of the world used a similar integrative approach. In New Zealand, a 21-year program involved treating dogs regularly with arecoline, banning raw offal feeding, and promoting safe sheep slaughtering practices. The authors used the age at which 20% of lambs had ‘parasitic’ liver damage as an efficacy metric. Over the trial, this age increased from 4 to 9 months86. In Cyprus, education was carried out over 5 years, targeting school children, housewives, and dog owners. Dogs were screened and infected dogs were euthanized or arecoline was given according to the owner’s consent. After three years, dog prevalence dropped from 50% to 6.8%87. In Wales and Morocco education alone was compared to education plus PZQ. In Wales, after the intervention, lamb prevalence was 4.3% in the education area, 6% in the education plus PZQ area, and 10.4% in the control area. Education significantly increased PZQ usage among farmers88. In Morocco, an integrated intervention targeted dog rabies, echinococcosis, and canine leishmaniasis. Dogs were treated 3 times a year and purged with arecoline at the end of the study. Dogs receiving PZQ had lower infection rates than those in the only education arm, but the difference was not statistically significant. Education increased knowledge but did not affect risky behaviors89. In Spain, dogs were treated with PZQ every 6 weeks for 6 years, health education targeted high-risk groups for the first 3 years, and stray dogs were removed. Sheep were inspected and sanitary pits were provided to dispose of carcasses. New human cases decreased from 19 to 4 per 100,000 people90. Also in Spain, a comprehensive program is reported though it lacks detailed descriptions of each component. Nonetheless, the program achieved an overall efficacy of 67% and, importantly, reported a profitability of 970%91. In China, in hyperendemic areas a combination of monthly PZQ, culling unwanted dogs, restructuring and training of the EG management teams, and public education reduced prevalence in dogs from 14.7-18.6% to zero after 4 years92. Another intervention consisted of education, improved sanitation, ultrasound screening of humans, surgical and albendazole treatment, and management and monthly PZQ for dogs. Interestly, the authors report measures of efficacy different from disease burden. After 11 years, surgeries rose by 32.4%, albendazole treatment by 81.3%, and dog deworming by 58.6%93. In Italy, an 8-year program used sentinel sheep abattoirs, analyzed national slaughterhouse data annually, treated farm dogs with PZQ, and diagnosed dogs with molecular and fill-FLOTAC techniques. Livestock were diagnosed with ultrasound and human CE surveillance was based on medical records. Public health education was delivered through multiple media formats. The program reduced sheep prevalence by 30%, and all dogs were negative 50 days post-PZQ44. In the Falklands, legally imposed control activities between 1965 and 1981 included purging dogs, banning offal feeding, and enforcing shepherd dog movement restrictions. Dogs were treated with PZQ every 6 weeks. Education was conducted through various media formats. Sheep prevalence dropped from over 40% to below 1% by 199394. Details of these interventions focused on animals and humans can be found in Table 1c.
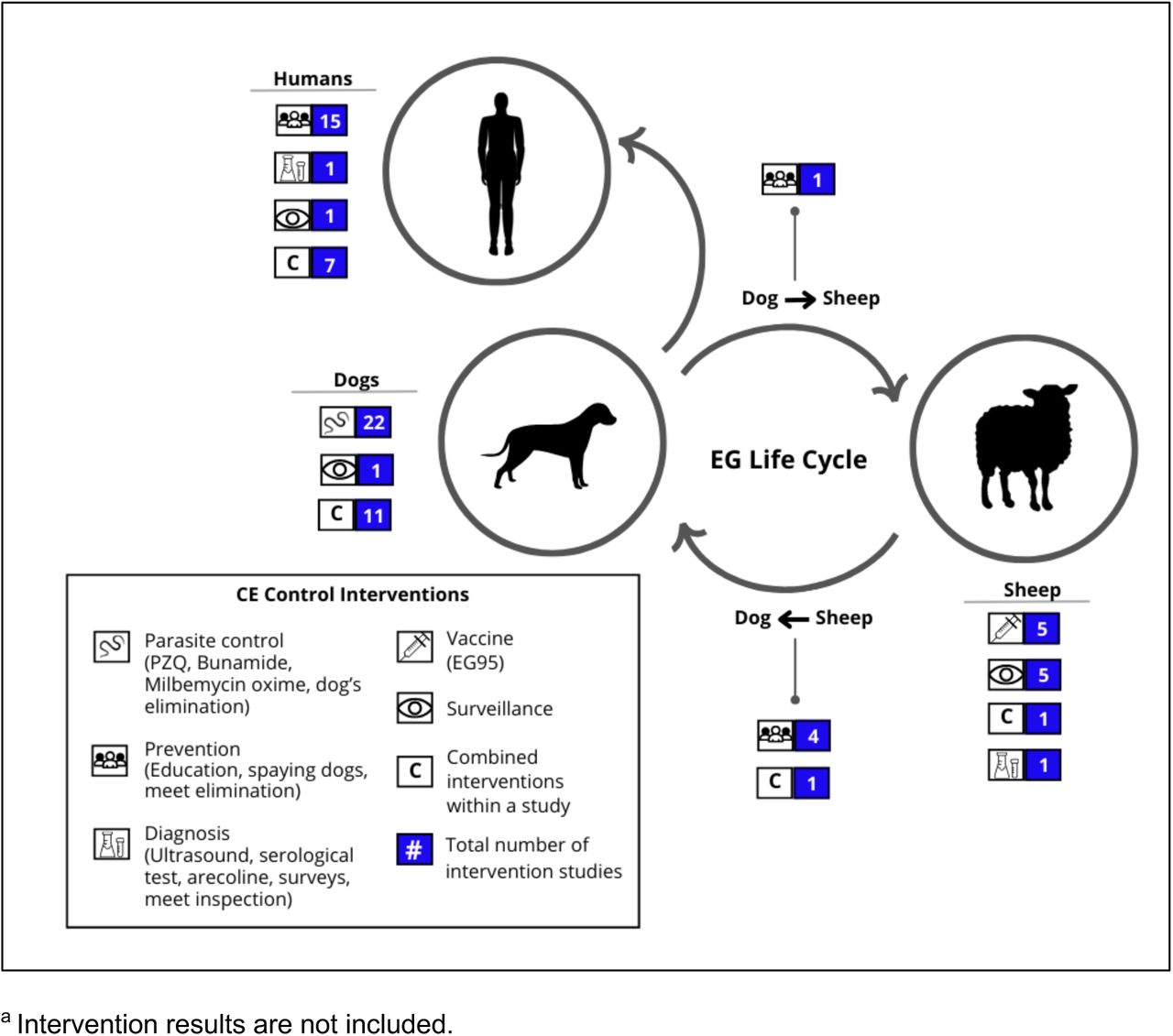
In Fig 2, we illustrate the points within the EG life cycle where different studies aimed to interrupt transmission. As numerous studies implemented multiple interventions targeting various components of the life cycle, the count of interventions depicted in Fig 2 exceeds the total number of papers analyzed.

Quality Appraisal
Of the 45 studies in our review, 40 were evaluated with the quantitative non-randomized studies questions (section 3 of MMAT). The average fulfillment with the quality criteria was 57%: five studies59,70,83,86,91 did not meet any criteria or their compliance could not be determined, three58,71,88 met 20%, one84 met 40%, 16 studies44,54,61,62,65,72,73,75,78,80,81,87,89,90,93,94 met 60%, 14 studies35,55,61,63,64,66,67,74,76,77,79,82,85,92 met 80%, and only one study68 met 100% of the quality criteria. The main criterion for noncompliance/undetermined compliance was the evaluation of possible confounding factors; only one study68 fully addressed them. The second most frequent challenge was determining representativeness; sampling estimates or clear description of sample selection were not always provided. Another criterion with inadequate or undetermined answers was completeness of the outcome data. Three studies were evaluated with the quantitative descriptive study questions (section 4 of MMAT). The average overall quality was 47%; one39 met 20% of the criteria, one53 met 40%, and one56 met 80%. The main criterion for compliance was the evaluation of risk of nonresponse bias and we found that the information provided was insufficient to comply with the criterion. The second most frequent problem was evaluation of representativeness. The three studies described their target population and elegibility, but in two39,53 it was difficult to determine if their sample was representative. One study69 was evaluated with the quantitative randomized controlled trials questions (section 2 of MMAT), and it met 60% of the quality criteria. In this study, the information provided was insufficient to fully evaluate if the randomization was appropriately performed and no information about blinding was provided. One study57 was evaluated with the mixed methods study questions (sections 5, 1 and 4 of MMAT) and met 40% of the overall quality criteria. This mixed methods study had a predominance of qualitative methods and results. When evaluated by components, it scored 100% of compliance in the qualitative criteria (section 1), 60% in the mixed methods criteria (section 5) and 40% in the quantitative criteria (section 4).
Discussion
We mapped and analyzed 45 articles on interventions for the control, prevention, or elimination of EG from all regions (Fig 3). The primary goal of control interventions is to halt the transmission of EG to its hosts. Compared to earlier interventions72,86,87, recent advances have significantly enhanced EG control. Key developments include the incorporation of the EG95 vaccine for sheep95, improved diagnostic techniques for early detection in dogs (e.g., ELISA)96,97, and the use of PZQ for dog treatment98. Despite these advances, progress in EG control remains inconsistent, with mixed results reported99, and overall, limited advancement in endemic regions100–102. We found articles of heterogeneous and generally low quality, often lacking clear post-intervention outcomes, which hampers the ability to inform future interventions. Studies varied in scale but provided limited information for scale-up implementation or replication in different settings. Common barriers are often mentioned, but few studies explore real-world barriers and facilitators in depth or address the feasibility of interventions. Additionally, implementation costs are rarely reported, yet cost-benefit analyses are essential for the scalability and sustainability of these strategies103–105. In addition, effective EG control requires collaborations, partnerships, and community engagement. The educational interventions we reviewed here were aimed at increasing awareness and knowledge among various stakeholders39,54–57, but did not report measures of long-term impact. However, the primary value of these interventions may lie in promoting community engagement, which is crucial for the success of control and elimination efforts106,107. Future studies could aim at building and examining stakeholder and community engagement for enforcement and sustainability of control activities.

Among the reviewed studies, those focused solely on interventions on animals were the most numerous, while studies focused solely on interventions on humans were the fewest. However, studies focused on both animals and humans had, in general, more participants, lasted longer, and covered larger geographical areas. The majority of these articles on integrated strategies described national multi-pronged programs including population screening and diagnosis, sanitation improvement, human and animal treatment and surveillance, among others. However, most of these articles came from a few countries who have been able to sustain these massive efforts to control EG. However, a significant challenge in the control programs for cystic echinococcosis (CE) is ensuring government commitment108,109. These programs require substantial effort and financial investment, funding that should come from government sources, such as Ministries of Health and Ministries of Agriculture, and participation of other sectors such as education and environment109,110. Short-term programs spanning only a few years are inadequate; CE must be treated as a chronic endemic disease requiring sustained efforts over many years18,111. Countries, such as Uruguay and Argentina, have been implementing control programs for over 50 years with important successes but they continue to face challenges despite their long-term commitment30,112.
Others have conducted reviews on EG and its control. For ours, we used the PRISMA-ScR framework and the Arksey and O’Malley method, focusing on studies in English, Spanish, and Portuguese. Others have used various guidelines and checklists, including PRISMA15,113, MeSH26, and Medline18, to evaluate articles across multiple languages and databases. We used MMAT for quality appraisal, while others used RCVS, CASP and JBI114. Despite the lack of detailed methodologies in other reviews on EG, they provide comprehensive summaries of the determinants and control programs associated with EG infection. A review26 highlighted projects like HERACLES (Human Echinococcosis ReseArch in Central and Eastern Societies)115,116 and MEmE (Multi-centre study on Echinococcus multilocularis and EG in Europe: development and harmonization of diagnostic methods in the food chain)117,118, which have created a comprehensive database with the latest epidemiological data from various regions. Multiple reviews18,26,119,120 agreed with us that sheep vaccination emerged as a promising strategy to complement and reduce the time of the control efforts. However, it is important to recognize that logistical and financial challenges remain in endemic countries, impacting the effectiveness of these interventions. Similar to our results87,94, others have found that island control programs tend to have higher success rates possibly due to easier disease containment and more manageable populations99. Interestingly, one review suggested sustained vertical campaigns that include treatment of dogs, community education, surveillance in rural areas, although they warn about significant time and resources99. We found vertical programs with strict enforcement measures in the Falklands and Cyprus87,94, both with positive results; however, the insular context might have played a bigger role in the success of those programs. Key challenges reported in these reviews and also found in our review are reliance on rural dog owners for implementing dog treatment, inadequate funding and staffing of programs, and political instability or insufficient political will6,18,119. The One-Health approach is recommended to address these issues effectively120–122. Other frequently encountered implementation barriers that most studies fail to report are limited surveillance71,81, followed by the presence of ownerless dogs60,81,89, and two barriers that are assumed common in many endemic countries: geographic accessibility and the semi-nomadic lifestyle of some communities73.
Multiple animal-targeting studies reviewed here have tested and refined interventions for the main definitive EG host, the domestic dogs. Since the development of PZQ (Fig 4), an effective cestocide for the mature and immature adult stages of EG123, that drug has been the primary intervention for dogs, with treatment schemes varying from monthly to quarterly, depending on the disease burden in the area. Challenges for the effectiveness of PZQ include maintaining treatment, achieving high coverage, owner compliance, and government enforcement18,124. One of the fundamental causes for not achieving high coverage is the inability to find the dog at the house to receive the treatment. Recent innovative interventions involve advanced tools like geolocation devices to treat hotspots, smart collars for automatic baiting, and dropping PZQ baits with drones74,77,79, which could improve efficiency and reduce costs in control campaigns. Currently, logistical costs are too high for sustained PZQ-based control programs125,126. Some of the studies we discuss here report a payment from the dog owners127, others promote dog owners to buy PZQ in bulk to treat their animals84, other require an annual registration fee for the dog to support PZQ treatment among other dog-related interventions87, while in a few countries PZQ is provide free of cost to dog owners63,73,81.

From the beginning of PZQ and other oral treatments for dogs, palatability and acceptability studies have been conducted to improve mass use of these drugs128. More recent studies have focused on understanding reinfection rates after PZQ125 and testing slow-release PZQ formulations to reduce frequency of treatment76,126. A formulation that protects dogs for long periods (similar to what is expected from a vaccine) would be a real game changer. Equally important are studies on stakeholder acceptability of interventions. For example, some studies found conflicting perspectives coming from breeders and their wifes, and local authorities, and health providers related to EG control actions38,129. To enhance the feasibility, sustainability, and ultimate success of elimination and control programs, it is imperative to conduct implementation research130,131 studies that delve into the agendas and motivations of various stakeholders132,133. Understanding the perspectives and priorities of these stakeholders can increase community engagement and inform the design and implementation of more effective interventions133. Active participation from the community ensures better acceptance and adherence to control measures, fostering a sense of ownership and responsibility towards the program’s goals134,135. This multifaceted program would align well with the One Health approach136–138 not only addressing the technical and logistical challenges, but also building a supportive environment that can sustain long-term efforts against the disease.
Our study had some limitations. The final set of articles included a wide range of study designs and approaches, which led to significant heterogeneity in the data. This heterogeneity made it challenging to summarize findings across studies. Differences in the reported methods and results between studies made the classification of studies especially challenging for the quality appraisal. As with other types of reviews, our scoping review could be susceptible to publication bias, due to unpublished or inaccessible studies. Also, we made a strong effort to balance breadth and depth; however, it is possible we prioritized more breadth making it difficult to synthesize findings comprehensively. A challenge we faced was the reduced number of studies included for full-text review. With sparse data, generalizability may be limited and there may be a risk of overinterpreting the significance of findings. Moreover, this limited number of studies impeded identifying trends. Despite these limitations, we conducted a rigorous quality assessment of the included studies and implemented a detailed protocol to reduce subjectivity in study selection and data extraction.
Conclusion
In sum, the literature on control, prevention, or elimination of E. granulosus sensu lato shows key advancements in diagnosis, treatment, and vaccines for the intermediate and definitive hosts. However, progress remains inconsistent, particularly in endemic regions, and many studies lack clear post-intervention outcomes, impeding the ability to inform future programs. Standardization in the reporting of studies is necessary for comparability of results and scaling-up of interventions. Effective EG control requires sustained government commitment, funding, and active participation from various sectors, including health, agriculture, and education. Long-term programs are necessary, as demonstrated by the decades-long efforts in Uruguay and Argentina. Innovative strategies, such as geolocation devices and drones for PZQ baiting, show promise but face logistical and financial challenges. To enhance the feasibility and sustainability of elimination and control programs, implementation research focused on understanding stakeholders’ agendas and increasing community engagement is crucial. Multi-pronged integrative One Health approaches are essential for overcoming the logistical, economical, and political challenges of sustaining long-term efforts for echinococcosis control.
Data Availability
The protocol of this review is registered on the Open Science Framework (www.osf.io) with DOI 10.17605/OSF.IO/48AZR. URL: https://osf.io/agsfh URL: https://osf.io/48azr All other articles included in results of this scoping review are published in their respective journals.
Supporting information
Acknowledgments
We are grateful to Fredy Daniel Bustamante Villanueva for his support during article retrieval.
References
- 1.↵
- 2.
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.
- 28.
- 29.
- 30.↵
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.↵
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.
- 102.↵
- 103.↵
- 104.
- 105.↵
- 106.↵
- 107.↵
- 108.↵
- 109.↵
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.↵
- 137.
- 138.↵
- 139.
- 140.
- 141.
- 142.
- 143.
- 144.




{kind=link}
{kind=link}
{kind=link}
{kind=link}