
Abstract
Introduction Autoimmune diseases are heterogeneous and often lack specific or sensitive diagnostic tests. Increased percentages of CD4+CXCR5+PD1+ circulating T follicular helper (cTfh) cells and skewed distributions of cTfh subtypes have been associated with autoimmunity. However, cTfh cell percentages can normalize with immunomodulatory treatment despite persistent disease activity, indicating the need for identifying additional cellular and/or serologic features correlating with autoimmunity.
Methods The cohort included 50 controls and 56 patients with autoimmune cytopenias, gastrointestinal, pulmonary, and/or neurologic autoimmune disease. Flow cytometry was used to measure CD4+CXCR5+ T cell subsets expressing the chemokine receptors CXCR3 and/or CCR6: CXCR3+CCR6− Type 1, CXCR3−CCR6− Type 2, CXCR3+CCR6+ Type 1/17, and CXCR3− CCR6+ Type 17 T cells. IgG and IgA autoantibodies were quantified using a microarray featuring 1616 full-length, conformationally intact protein antigens. The 97.5th percentile in the control cohort defined normal limits for T cell subset percentages and total number (burden) of autoantibodies.
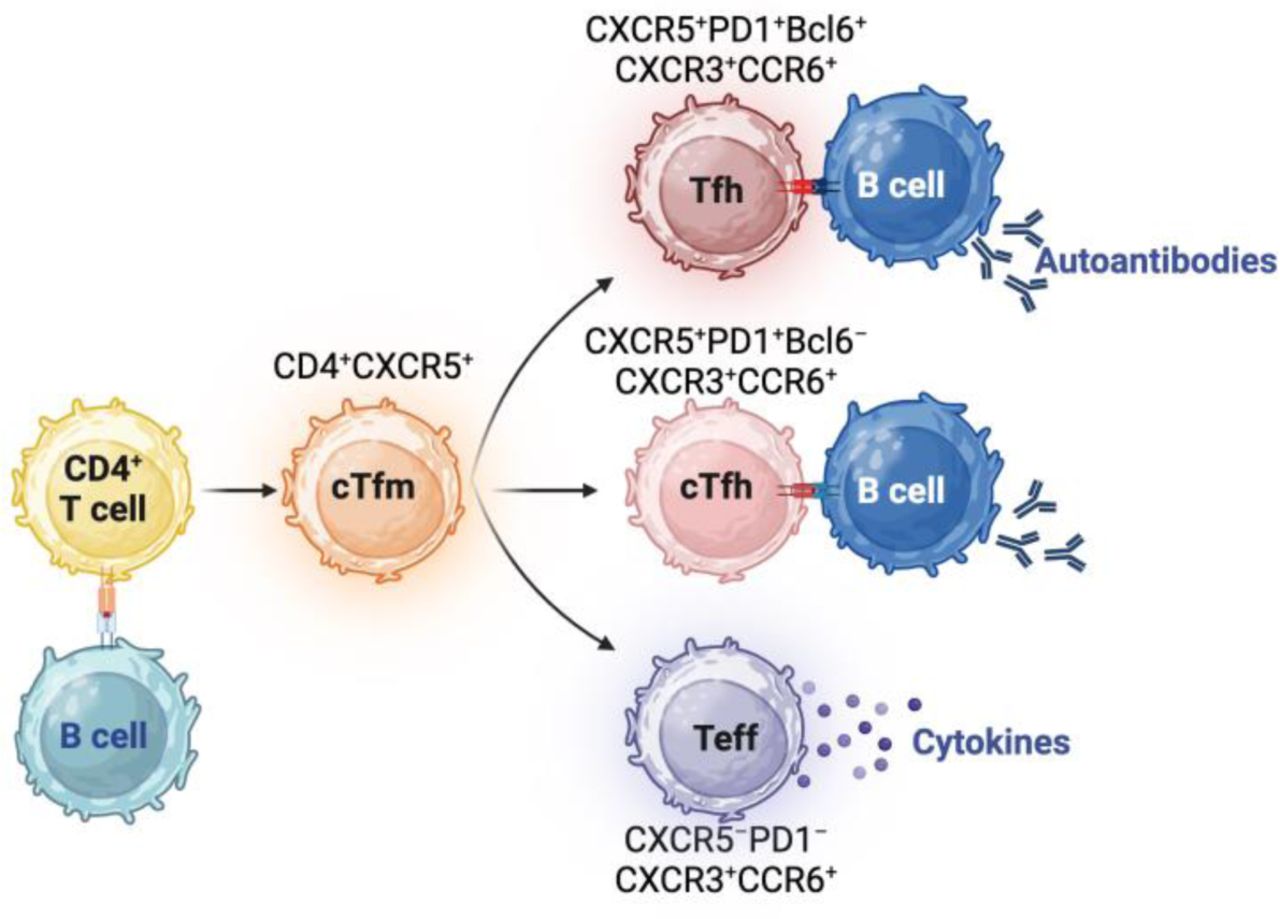
Results This study focused on CD4+CXCR5+ T cells because CXCR5 upregulation occurs after cognate T-B cell interactions characteristic of autoimmune diseases. We refer to these cells as circulating T follicular memory (cTfm) cells to acknowledge the dynamic nature of antigen-experienced CXCR5+ T cells, which encompass progenitors of cTfh or Tfh cells as well as early effector memory T cells that have not yet lost CXCR5. Compared to controls, 57.1% of patients had increased CXCR5+CXCR3+CCR6+ cTfm1/17 and 25% had increased CXCR5+CXCR3−CCR6+ cTfm17 cell percentages. Patients had significantly more diverse IgG and IgA autoantibodies than controls and 44.6% had an increased burden of autoantibodies of either isotype. Unsupervised autoantibody clustering identified three clusters of patients with IgG autoantibody profiles distinct from those of controls, enriched for patients with active autoimmunity and monogenic diseases. An increased percentage of cTfm17 cells was most closely associated with an increased burden of high-titer IgG and IgA autoantibodies. A composite measure integrating increased cTfm1/17, cTfm17, and high-titer IgG and/or IgA autoantibodies had 91.1% sensitivity and 90.9% specificity for identifying patients with autoimmunity. Percentages of cTfm1/17 and cTfm17 percentages and numbers of high-titer autoantibodies in patients receiving immunomodulatory treatment did not differ from those in untreated patients, thus suggesting that measurements of cTfm can complement measurements of other cellular markers affected by treatment.
Conclusions This study highlights two new approaches for assessing autoimmunity: measuring CD4+CXCR5+ cTfm subsets as well as total burden of autoantibodies. Our findings suggest that these approaches are particularly relevant to patients with rare autoimmune disorders for whom target antigens and prognosis are often unknown.

{kind=link}
Competing Interest Statement
EMH, SC, AC, LS, MN, AA, BW, EO, SS, CY, RN, PYL, OH, RCH, MD-L, AAN, ME, TKO, MG-A, CDP, BL, JC have no conflicts of interest to disclose. DHK is a consultant for Adivo Associates. LAH received salary support from the Childhood Arthritis and Rheumatology Research Alliance, investigator-initiated research grants from Bristol Myers Squibb, and consulting fees from Sobi. JP is an employee of Sengenics. RFG receives research funding from Novartis, Sobi, and Agios and is a consultant for Agios and Sanofi.
Funding Statement
This work was supported by the National Institutes of Health (T32HL007574 to EMH, T32AI007512 to SC, BL, JC, and R01DK130465 to JC) and the Immune Deficiency Foundation (BL). The Children's Rare Disease Cohort initiative funded the whole exome sequencing of study participants. Sources of funding had no role in the study design or execution, data interpretation, or writing of the manuscript.
Author Declarations
I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained.
Yes
The details of the IRB/oversight body that provided approval or exemption for the research described are given below:
The Institutional Review Board of Boston Children's Hospital gave ethical approval for this work
I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals.
Yes
I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance).
Yes
I have followed all appropriate research reporting guidelines, such as any relevant EQUATOR Network research reporting checklist(s) and other pertinent material, if applicable.
Yes
Abbreviations
- AIHA
- Autoimmune hemolytic anemia
- cTfh
- Circulating T follicular helper cell
- cTfm
- Circulating T follicular memory cell
- ES
- Evans syndrome
- ITP
- Immune thrombocytopenia
- IVIG
- Intravenous immunoglobulin
- SLE
- Systemic lupus erythematosis
The Chan Zuckerberg Initiative, Cold Spring Harbor Laboratory, the Sergey Brin Family Foundation, California Institute of Technology, Centre National de la Recherche Scientifique, Fred Hutchinson Cancer Center, Imperial College London, Massachusetts Institute of Technology, Stanford University, University of Washington, and Vrije Universiteit Amsterdam.




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos