
ABSTRACT
Background The CoBaTrICE program (Competency Based Training Program in Intensive Care Medicine) has been instrumental in standardizing intensive care training across Europe. Among the various procedures taught, pericardiocentesis is notably challenging due to its high-risk nature. This study aims to compare the efficacy and stress levels induced by two simulation models for pericardiocentesis training: a traditional 3D-printed mannequin and a virtual reality (VR) model.
Methods A pilot, before and after study was conducted with last-year medical students. Participants were trained using both a 3D-printed mannequin and a VR model. Learning outcomes were assessed using a questionnaire modeled after the Objective Structured Clinical Examination (OSCE). Stress levels were measured through Heart Rate Variability (HRV) analysis, supplemented by the Biosignal plux system for real-time biometric data collection.
Results Thirty-six students participated, with no significant differences in learning outcomes between the two models, except in parameters requiring fine motor skills. Stress levels, as measured by HRV, showed no statistically significant differences between the two simulations models.
Conclusion The study suggests that VR model is as effective as 3D printed for pericardiocentesis training.
Take Home Message The study demonstrates that virtual reality (VR) and traditional 3D-printed mannequins are equally effective for training medical students in pericardiocentesis, with no significant difference in learning outcomes or induced stress levels. This suggests that VR could be a viable, resource-efficient alternative in intensive care medicine training, particularly for high-risk procedures.
Tweet Study finds VR as effective as 3D mannequins for pericardiocentesis training in med students, offering equal learning and stress levels. #MedEd #VRinMedicine
INTRODUCTION
Since its inception in 2003, the Competence Based Training in Intensive Care (CoBaTrICE) program has served as a cornerstone in standardizing intensive care medicine training across Europe [1]. This program not only unifies learning procedures in intensive care units but also offers an extensible framework for academic training programs aimed at students in the final stages of their medical education [2]. Among the critical procedures taught in intensive care medicine, pericardiocentesis stands out as particularly challenging due to its inherent invasiveness and risks as well as the low frequency thar it is performed at bedside [3,4]. Given these fact conventional learning methods often prove insufficient for effectively preparing physicians [5,6].
This is where clinical simulation has proven its worth. Over the years, simulation has evolved from basic models to the current High-Fidelity Clinical Simulation utilizing computerized systems [5-8]. These advancements, although significant, come with their own set of challenges. The most prominent is the high cost associated with the required technology and infrastructure, such as specialized simulation rooms. Additionally, effective simulation training requires highly specialized instructors and presents a steep learning curve. [9,10]
In this evolving landscape, virtual reality (VR) emerges as a potentially revolutionary solution [11] [12,13]. VR offers several key advantages over traditional simulation methods, including deeper immersion in clinical scenarios, near-perfect reproducibility, standardization of training scenarios, the incorporation of an emotional component, and scalability. Scalability refers to the fact that, unlike traditional simulation methods, which require significant hardware investment, VR can adapt to new procedures and scenarios with simple software iterations. This flexibility not only broadens educational possibilities but could also democratize access to high-quality medical training, especially in resource-limited countries [14,15].
This study hypothesizes that learning the pericardiocentesis procedure based on VR model is similar than based on the traditional mannequin. Thus, we compare learning outcomes and stress levels between these two simulation models for pericardiocentesis training (traditional mannequin model and a VR model). This study is not only an academic exercise because if both methods are equivalent; we will provide one of the earliest proofs of concept for using VR in complex procedures. Likewise, it would be a really important tool for teaching medical centers and universities; especially those located in low- and middle-income countries.
MATERIAL AND METHODS
This pilot, prospective, before and after study compared two different pericardiocentesis training models: one based on a self-made mannequin using 3D design and 3D printing technology (mannequin model), and the other based on a virtual reality environment programmed in Unity (VR model).
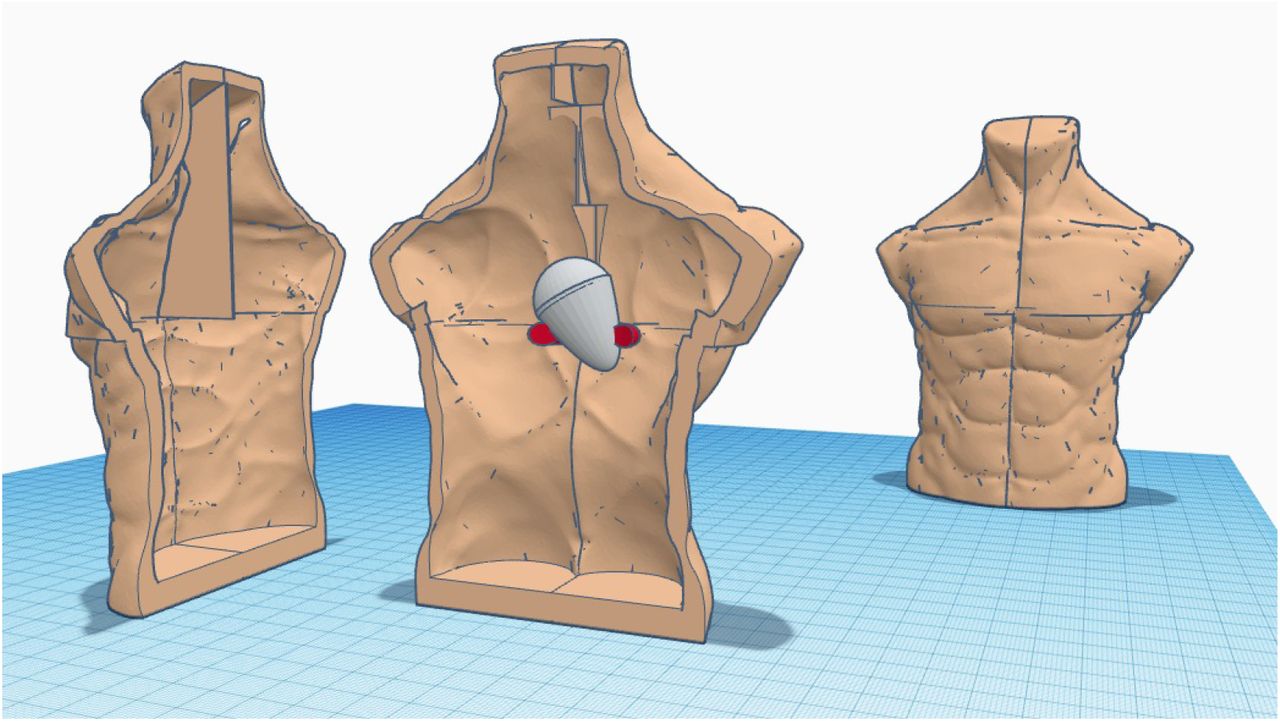
The mannequin model was designed using 3D modeling software (Tinkercad and Adobe Fusion 360). The process involved the creation of a digital representation of the model, considering the anatomical structures relevant to the pericardiocentesis procedure. Once the design was completed, the model was constructed using 3D printing technology. We employed optimized rendering software (MeshMixer), a specific laminator (Ultimaker Cura), and an Ender 3 printer to create the physical mannequin, the pericardial model, and its support (supplementary figures 1-5). On the other way, the VR model was designed and developed using the Unity game engine. This virtual model was designed to be homologous to the physical model, ensuring that both training environments were comparable. The virtual reality environment was made compatible with the HTC Vive, and Oculus Rift platforms, allowing for a broad range of hardware options for trainees (supplementary figure 6)
Finally, both models were adjusted and validated by a panel of five senior intensivists (none of them related to this study) from the Cardiac Intensive Care Unit of HM Montepríncipe University Hospital in Madrid-Spain.
The study was carried out with the approval of the Research Ethics Committee at HM Montepríncipe University Hospital. Verbal consent was obtained from each participant and the recruitment period for the study took place between November 7, 2021 and February 15, 2022.
Inclusion criteria
All last-year medical students from CEU University were invited to participate in the study. All who accepted to participate received a link to a video demonstrating the pericardiocentesis procedure performed by an instructor using a standard simulation mannequin. This video served as a baseline for the trainees’ understanding of the procedure (supplementary material).
Exclusion criteria: incomplete questionnaires
With the aim to assess learning parameters, an external evaluator assessed the students’ performance during both procedures using pre-established questionnaires, modeled after the Objective and Structured Clinical Evaluation (ECOE) tool, commonly used in the assessment of procedural skills in the educational program of the last year of the medical degree. Parameters that were scrutinized included aspects of diagnosis and clinical reasoning (rapid response, saturation analysis, cardiac rhythm analysis), and procedural skills (pulse oximeter placement, sphygmomanometer staining, material handling, glove placement, asepsis, surgical field placement, puncture site location, correct needle angulation, proper guidewire placement, proper drain placement). Each of item were punctuated from 0 (minimun) to 5 (maximum) and finally, two global assessment items (total score and grade).
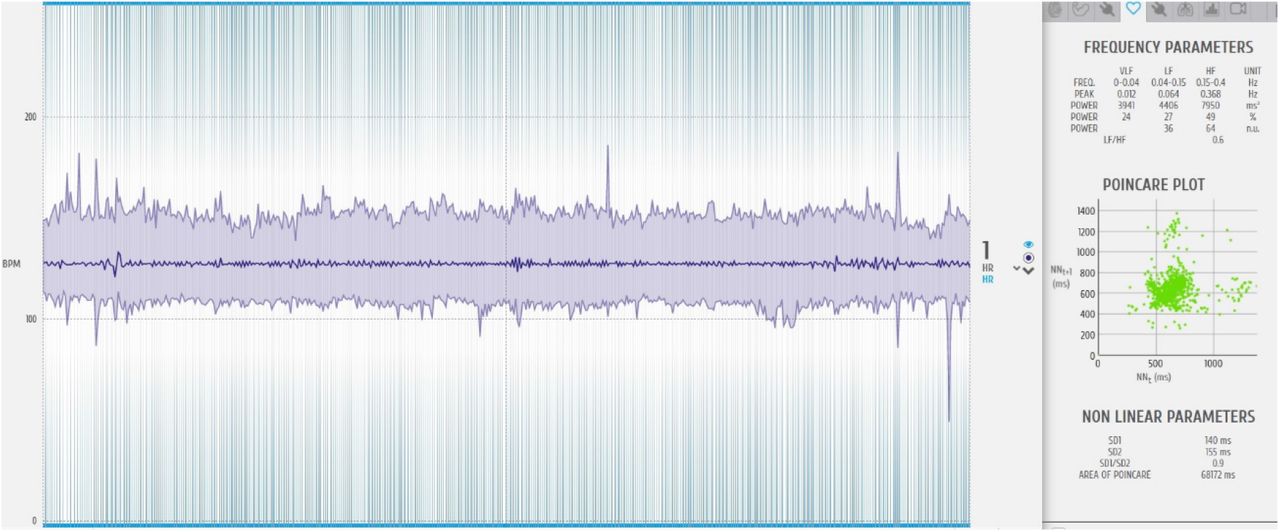
With the aim to assess stress responses, prior to the initiation of the simulation, students were equipped with continuous heart rate recording electrodes via the biosignal plux system. Additional electrodes were strategically placed: two on the forehead for electrodermal activity, two at the masseter level for electromyography, and three on the torso for heart rate monitoring. Data acquisition and subsequent processing were executed using opensignals digital signal processing software (supplementary figure 7). Stress parameters were assessed according to five variables, heart rate variability parameters, both in the time domain (rMSSD, PNN50) and frequency domain (LH, HF, and their LF/HF ratio), as well as nonlinear parameters (SD1/SD2 ratio). HRV [16]serves as a highly sensitive marker for dysregulation in the Autonomic Nervous System (ANS) and is defined as the temporal variation in the intervals between consecutive heartbeats over a predefined time period. Electrocardiographic recording of HRV enables the analysis of various temporal and frequency parameters. The most used parameters include: 1) 1. Frequency-domain parameters: Low Frequency (LF): Typically associated with sympathetic activation but also has a parasympathetic component; High Frequency (HF): A selective indicator of parasympathetic nervous system (PNS) activity, related to stress relief; LF/HF Ratio: Serves as an indicator of sympathetic activity, associated with increased stress levels. 2) Time-domain parameters: rMSSD: The root mean square of successive differences between normal heartbeats, closely related to the PNS; and PNN50: The percentage of differences associated with the number of intervals between heartbeats that vary by more than 50 milliseconds, closely correlates with the PNS; and 3) Non-linear parameters (derived from the Poincaré plot, which is a visual representation of temporal intervals between consecutive heartbeats) [17]: SD1/SD2 Ratio: Correlates with the LF/HF ratio.
Phases of recording
The data collection was segmented into four distinct phases (Figure 1):

Initial Resting Phase: Students were seated in a stimulus-free environment.
Virtual Reality Simulation: Students donned Oculus Rift virtual reality goggles, simulating a clinical scenario involving a patient with tachycardia, dyspnea, and hypotension due to cardiac tamponade. The task required rapid diagnosis and emergent pericardiocentesis, adhering to clinical protocols (supplementary figure 8).
Second Resting Phase: A period of rest without external stimuli.
Mannequin Procedure: Students replicated the pericardiocentesis procedure on a 3D-printed mannequin, adhering to the same clinical steps as in the virtual reality simulation.
Statistical Methods
Continuous variables were expressed as mean +-SD, and categorical variables as proportions. The two phases (“mannequin” and “VR”) for the study were compared using T-paired test. A two-sided P < 0.05 was considered statistically significant.
RESULTS
Thirty-six students were recruited, mean age 23.6 (± 2.0) years, 75% females.
Learning outcomes can be appreciated in Table 1.
There were no differences in the diagnostic assessment, clinical reasoning and overall procedural skills between the classic mannequin model and the virtual scenario.
However, differences between procedural parameters assessing fine motor skills were identified.
Regarding the analysis of induced stress, no differences were identified (Table 2).
DISCUSSION
As far as we know, this is the first study that demonstrate the fact that learning a complex and risky procedure (pericardiocentesis) based on a model of VR is similar than based on a mannequin model. Our result opens a great opportunity for democratizing the learning of complex procedures; specially in LMCI where facilities sometimes are scarcy or areas far from academic centers.
The advent of 3D modeling in medical education, particularly using free software, marks a significant stride in the evolution of clinical training and patient education. The integration of these technologies addresses a critical need for interactive, cost-effective, and accessible educational tools in the medical field. The utilization of interactive 3D modeling tools in cardiovascular surgery education as explored by Gerrah and Haller (2021) exemplifies the transformative potential of these technologies [18]. Furthermore, the effectiveness of open-source software in creating detailed 3D organ models as demonstrated by Cross et al (2018) provides a viable and cost-effective alternative to proprietary software [19].
The creation of a 3D-printed mannequin for pericardiocentesis training involved advanced 3D modeling and practical design considerations resulting in a realistic and educationally valuable model. Transitioning from digital to physical the model was rendered and printed with precision focusing on anatomical accuracy and replicating tactile feedback essential for training.
The application of VR in intensive care training as explored by Horwitz (2022) addresses the challenges posed by the continuous evolution of high-tech medicine and the need for specialized training for healthcare professionals [20]. VR’s ability to simulate complex medical scenarios provides a safe and controlled environment for trainees to hone their skills without the risks associated with real-life patient interactions. In this paper. the mannequin was adapted into a virtual reality (VR) environment ensuring procedural and anatomical consistency with the physical model. The creation of immersive VR medical simulations for trauma training demonstrates the versatility of VR technology. These simulations provide a realistic environment for training medical personnel in managing high-stress and high-risk scenarios such as battlefield injuries [21]. The ability of VR to replicate real-world trauma management scenarios underscores its potential as a comprehensive training tool. In our case. despite the VR model’s limitations in simulating tactile nuances both the 3D-printed and VR models effectively imparted essential skills for pericardiocentesis with no significant differences in learning outcomes for diagnostic assessment and clinical reasoning. Moreover, the immersive nature of VR training enhances the acquisition and transfer of skills among healthcare professionals. Mantovani et al. (2003) emphasize that VR training raises interest and motivation in trainees leading to better skill retention and application [22]. This aspect is crucial in intensive care training where quick decision-making and precision are vital. The usability of VR in emergency simulation training as studied by Lerner et al. (2020) demonstrates VR’s potential in emergency medicine a key component of intensive care [21].
The development of immersive VR stations for OSCE as explored by Rodríguez-Matesanz et al. represents a significant advancement in clinical skills assessment [23]. Adapting OSCE to a virtual platform. as described by Watson et al further underscores the versatility of VR in medical education [24]. Our pilot study corroborates that the learning efficacy is comparable between the two models except for parameters requiring fine motor skills. This limitation is consistent with the current state of VR technology which offers restricted fine motor skill replication through haptic devices although ongoing research aims to ameliorate this with design and optimization of haptic devices.
The utilization of Heart Rate Variability (HRV) analysis in virtual reality (VR) simulations, particularly in the context of medical education, presents a novel approach to evaluating stress levels and physiological responses. Aganov et al further explore the effect of VR on stress management demonstrating that modified VR interventions can significantly influence short-term HRV and perceived anxiety levels in individuals exposed to moderate stress [25]. This finding is particularly relevant in medical education where managing stress and anxiety is crucial for effective learning and performance. Our study employed heart rate variability as a metric and found no statistically significant differences between the two models across multiple domains (temporal frequency or nonlinear). This is particularly pertinent given the high-stakes time-sensitive nature of procedures like pericardiocentesis suggesting the VR model’s efficacy in replicating a high-stress training environment.
The primary outcome of this investigation is the demonstration that the acquisition of pericardiocentesis skills is comparably effective when utilizing either a mannequin model or a virtual reality (VR) system. This study serves as a foundational proof of concept validating the use of VR as an innovative and cost-effective means for learning complex medical procedures. Far from being a mere theoretical exercise. our findings provide robust evidence supporting the global adoption of this technology particularly in low- to middle-income countries.
In essence our results contribute to the democratization of advanced clinical simulation especially in economically challenged environments. Moreover, the versatility of these 3D models extends beyond pericardiocentesis to encompass a variety of invasive procedures including thoracentesis paracentesis and central venous catheterization. This adaptability enhances the potential for widespread application and utility in diverse medical training scenarios.
The low development cost of VR coupled with its scalability allows for a more inclusive educational experience extending from medical students and nurses to seasoned professionals like residents and consultants at the hospital level. The study also highlights the adaptability of these models. With simple software programming adjustments. a wide array of invasive procedures such as thoracentesis. paracentesis and central line cannulation can be simulated thereby broadening the scope of training scenarios available. Furthermore, the VR model’s multi-platform compatibility enhances its versatility making it applicable in diverse learning environments.
This limitation has some limitations. Firstly, it’s non-randomized study thus it is not possible to rule out the aliasing effect. Secondly, it was performed in a unique center from a high-income country thus is extrapolation to other settings could be reduced. Thirdly, as only model was evaluated, we cannot know what would happen with other techniques. Conversely, this study has several strengths. Undoubtedly, the first lies in its innovative approach to medical education. bridging the gap between traditional clinical simulation and emerging virtual reality (VR) technologies. This fusion not only democratizes access to high-fidelity advanced clinical simulation but also significantly reduces the associated costs. Secondly, both models have been clinically validated by physicians with well demonstrated expertise in the field. This fact maximizes the probability of extrapolate our result to the real life. Thirdly, the sample size was enough for validating the procedure. Fourth, the two approaches used to assess learning and stress features were objective and reproducible.
CONCLUSION
The study demonstrates that a virtual reality model for pericardiocentesis is as effective maniquinn model in terms of learning achievement without relevant impact in student’s stress.
The study thus serves as a foundational piece of evidence advocating for the broader integration of such technologies in medical training curricula. It offers a compelling case for the cost-effectiveness. adaptability. and educational efficacy of these models. setting the stage for more comprehensive studies in the future.
Data Availability
All relevant data are within the manuscript and its Supporting Information files
DECLARATIONS
Ethics approval and consent to participate
The present study was approved by the Ethics Committee of HM Hospitals. All members of the study were final-year medical students who voluntarily participated in the study.
Consent for publication
Not applicable
Availability of data and materials
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request
Competing interests
The authors declare that they have no competing interests
Authors’ contributions
ARL designed the study, collected the data, performed the statistical analysis and wrote up the study as principal investigator.
RG participated in the development and correction of the virtual scenario
LZ performed the programming of the virtual scenario according to the created model
ARN participated in the performance tests and in the design and collection of biometric parameters
AGP participated in the design and adaptation of the simulated scenarios
PCF participated in proofreading and supervision of the study design, statistical analysis and supervision of the writing of the paper
SUPPLEMENTARY MATERIAL
Links to pericardiocentesis procedure video:
https://youtu.be/ox-2LP_3q_k?si=S93Dr3aB27IizWrr
https://youtu.be/OGhQYUfpX2I?si=nvTU0-yv9qGT36YI
Torso creation: from design to 3D printing



Pericardial design and 3D printed mold.

Process of creating the simulated pericardium


VR Final version


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgements
Not applicable
References



