
Abstract
Aims In elderly patients with and without left ventricular dysfunction (LVD) we compared ventilatory parameters from before to after exercise-based cardiac rehabilitation (exCR) and assessed their prognostic value for major adverse cardiovascular events (MACE).
Methods and Results Patients aged ≥65 years with acute or chronic coronary syndromes (ACS, CCS) without cardiac surgery who participated in a multicentre study on effectiveness of exCR from seven European countries were included. Cardiopulmonary exercise testing (CPET) was performed before, at termination of exCR and at 12 months follow-up. Ventilation (VE), breathing frequency (BF), tidal volume (VT) and end-expiratory carbon dioxide pressure (PETCO2) were measured at rest, at first ventilatory threshold and peak exercise.
In 818 patients, age was 72.5±5.4 years, 21.9% were women, 79.8% had ACS, and 151 (18%) had LVD. NYHA functional class was not different between LVD and noLVD (86% NYHA I in each group). Compared to noLVD, in LVD resting VE was increased 8%, resting BF 6%, peak VE, peak VT, and peak PETCO2 reduced by 6%, 8%, and 5%, respectively, and VE/VVCO2 slope increased by 11%. From before to after exCR, resting VE decreased and peak PETCO2 increased significantly more in LVD compared to noLVD. In LVD, higher resting BF, higher nadir VE/VCO2, and lower peak PETCO2 at baseline were associated with MACE
Conclusions In elderly patients with ischemic LVD, exaggerated resting ventilation and impaired pulmonary gas exchange during exercise was related to worse outcomes. ExCR was associated with an improvement of abnormal breathing patterns and gas exchange parameters.
Introduction
Ischemic heart disease is the most prevalent risk factor for left ventricular dysfunction (LVD) and chronic heart failure (HF), both for woman and men.(1) Impaired pulmonary gas exchange, quantified as an increased ventilation (VE) to carbon dioxide exhalation (VCO2) slope during exercise, and a low end-tidal pressure of carbon dioxide (PETCO2) is a landmark of heart failure patients.(2, 3) These parameters received attention when several studies found higher VE/VCO2 slopes and lower PETCO2 to be associated with poorer prognosis.(4-6) The components of the VE/VCO2 slope are the arterial CO2 partial pressure (PaCO2), that is affected by ventilation, and the pulmonary dead space to tidal volume ratio (VD/VT) that is affected by pulmonary perfusion abnormalities.(3, 7) As nicely summarised by Cross and colleagues, exercise hyperventilation is a hallmark of the failing heart.(2) They proposed several mechanisms as mediators of this excessive ventilatory response, including: 1) alveolar ventilation-perfusion mismatching, 2) increased humoral stimuli (e.g., lactate and H+) due to skeletal muscle hypoperfusion and deconditioning, 3) juxta-capillary receptor stimulation consequent to pulmonary vascular congestion and/or hypertension, 4) augmented central and peripheral chemosensitivity, and 5) an inordinately high degree of afferent neural traffic originating from within the locomotor muscles (i.e., the ergoreflex or “skeletal muscle” hypothesis). Hyperventilation is well known to stimulate sympathetic nervous activity.(8) Chronic sympathetic nervous hyperactivity in turn may decrease aerobic capacity of skeletal muscles by reducing capillarisation(9) and red blood cell flux,(10) which lead to a shift in muscle fibre type towards a lower content on type I fibres.(11) The ensuing anaerobic muscle metabolism leads to increased muscle fatiguability(12) and acidosis already at low levels of exercise, which trigger exaggerated responses in ventilation.(13) While exaggerated ventilation has been found to be a strong predictor of mortality and adverse cardiac events in patients with established heart failure, this has not been assessed in patients with LVD.
Comprehensive exercise-based cardiac rehabilitation (exCR) has the potential to improve cardiorespiratory fitness (CRF) and quality of life,(14) cardiovascular risk factors (15), and reduce hospitalisations and cardiovascular mortality.(15, 16) In HFrEF patients, studies assessing the effects of exercise have focussed largely on circulatory parameters,(17) peak oxygen uptake (VO2) and muscle strength.(18) Some studies have also reported changes in ventilatory efficiency in response to exercise during exCR.(19, 20) However, data in elderly patients with LVD are sparse and no data exists on how exCR influences breathing patterns at rest.
The purpose of the present study in elderly patients with and without ischemic LVD was to 1) describe breathing patterns and pulmonary gas exchange parameters at rest and during exercise; 2) assess the association of exCR with a change of these parameters; and 3) assess the prognostic value of these parameters on major adverse cardiac events (MACE).
Methods
The EU-CaRE observational study was a European project focusing on the effectiveness and sustainability of exCR programs in the elderly (65 years or above). EU-CaRE involved eight participating CR sites in seven countries (Denmark, France, Germany, Italy, the Netherlands, Spain and Switzerland).(21)
Study population
The study population and outcome data have been reported previously.(21-25) For the present study, only data from patients with acute or chronic coronary syndromes (ACS/CCS) with or without percutaneous coronary intervention (PCI) but without open-chest surgery were included. Patients were assessed at baseline before commencing exCR (T0), after completing the exCR program (T1) and at 1-year follow-up (T2). They were grouped according to left ventricular ejection fraction (LVEF) determined by the patient’s most recent echocardiography into patients with LVD (LVEF<45%), versus those without LVD (noLVD, LVEF≥45%). At the time when this study was designed, this cut-off was one of the more widely used and accepted cut-offs for systolic LVD and HF with reduced LVEF (HFrEF).(26)
The study was approved by all relevant medical ethics committees, registered at trialregister.nl (NTR5306). The participants gave written informed consent before they were included in the study.
Data collection
Recorded information included demographics, index event, socioeconomic factors, medical history including co-morbidity, and clinical information such as weight, blood pressure (BP), resting heart rate (HR), medication, SF36 quality of life questionnaire, and patient reported physical activity as number of days per week with at least moderate physical activity of minimally 30 min. Details on the collected data have been provided elsewhere.(21, 27, 28)
CRF and breathing parameters were assessed by cardiopulmonary exercise testing (CPET). After reporting to the laboratory, patients rested supine for 10-15 min during which a resting 12-lead electrocardiogram (ECG) was performed. Then patients stood up and performed a resting spirometry with determination of forced vital capacity (FVC) and forced expiratory volume during the first second (FEV1). After this, patients mounted the cycle ergometers and were fitted with a facemask. Then they remained sitting quietly for 3 min during which heart rate, blood pressure and breathing parameters were measured. As an average of the last minute of the 3-min resting period while sitting on the ergometer, the following parameters were determined: minute ventilation (VE), breathing frequency (BF), tidal volume (VT), partial pressure of carbon dioxide (PETCO2), and heart rate. After a 3-min warm-up at 5 Watt an individual ramp was chosen to achieve a test duration of 8-12 min until exhaustion and kept constant in follow-up tests. Data was analysed at the CPET core lab in Bern as previously described.(24, 28) During the ramp, VE/VCO2 slope, and the nadir of the VE/VCO2 ratio were determined. Oxygen consumption (VO2), VE, BF, VT, PETCO2, and heart rate were determined at the first ventilatory thresholdas previously described.(24) Peak values of the same parameters were determined as the highest value of a 30 s moving average. Ventilatory parameters were excluded when respiratory quotient was below 0.7 at resting and below 0.8 at peak exercise due to suspected presence of mask leakage.
MACE was defined as combined incidence of all-cause mortality, ACS, cardiac related emergency visit, hospitalisation for cardiac reason, near sudden cardiac death and cardiac intervention. MACE was recorded by monthly telephone calls and assessed individually by an independent Clinical Event Committee.(24)
Statistical analysis
All statistics were performed with R (Version 3.5.1, R Core Team, 2017). Changes in ventilatory and circulatory parameters were calculated between T0 and T1. Mixed linear models were performed for ventilatory parameters VE, BF, VT, and PETCO2 at rest and peak exercise, as well as VE/VCO2 slope and peak VO2 relative to body weight for interaction effects between time points T0, T1 and T2 and group (with and without LVD), adjusted for age, sex, and body mass index (BMI) and patients nested within centres entered as random factor (intercepts).
The association of ventilatory parameters at rest and during exercise with MACE were also assessed with mixed linear models for patients with and without LVD and with and without MACE.
Results
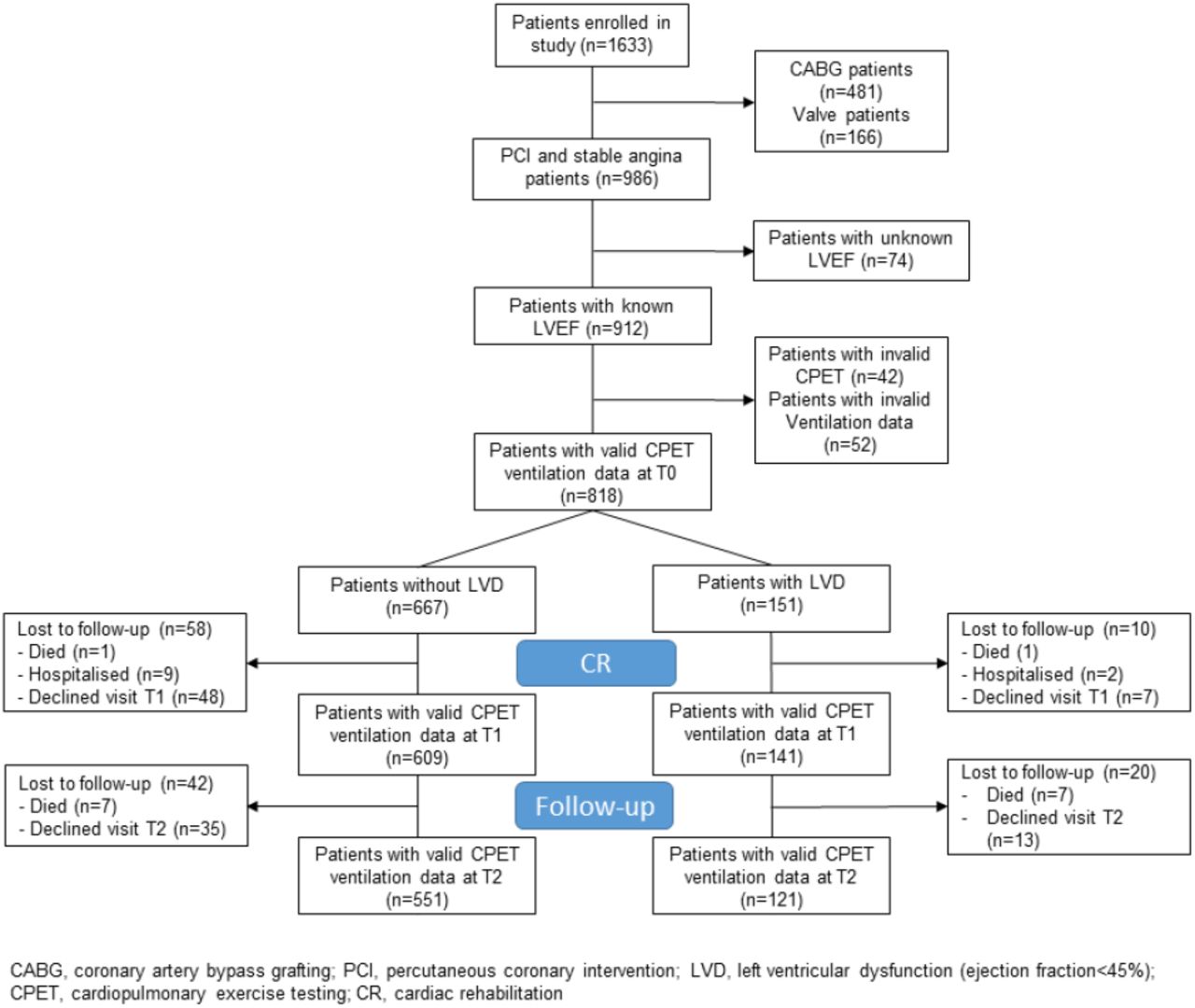
Of 1633 enrolled EU-CaRE patients, 986 patients had an ACS or CCS with percutaneous coronary intervention or no revascularisation. Of these, 79.8% had an ACS and 90.2% a PCI as indication for exCR. LVEF was known in 912 patients. Of these, valid CPET at T0 was available in 867 patients of whom 707 had no LVD and 166 had LVD. Amongst these, data on breathing pattern was available from at least one time point in 151 with and 667 patients without LVD (Figure 1). Baseline data of the two patient groups are shown in Table 1. Patients with LVD were older, were less often female, and had lower BMI and FVC/BSA. An equal prevalence of 86% of patients with NYHA functional class I existed in patients with and without LVD, and NYHA III class was present in 2% and 3% of patients with and without LVD, respectively. Patients with LVD had significantly lower physical component score of the SF36 indicating poorer health status. Patients with LVD had a higher percentage of pre-existing chronic heart failure and anaemia, and higher prescription rate of betablockers and ACE inhibitors or ARBs. With regard to ventilatory parameters, two centres did not record data on BF and VT, therefore, these parameters were missing in 5 and 51 patients with and without LVD, respectively. Due to an insufficient ventilation monitoring duration (≤1 min) during the 3-min resting phase, VE and PETCO2 at rest were missing in 9 and 68 patients with and without LV dysfunction at T0, respectively, in 6 and 82 at T1, respectively, and in 4 and 46 at T2, respectively. The first ventilatory threshold could not be determined in 38 and 130 patients with and without LV dysfunction, respectively, at T0, in 20 and 71 at T1, respectively, and in 16 and 61 at T2, respectively. The largest relative adjusted (for sex, age and BMI) differences of the LVD group compared to the noLVD group at baseline were found for VO2 peak (−12.6%), VE/VCO2 slope (11.0%), nadir VE/VCO2 (8.8%), and resting VE (8.1%) (Table 2).
Baseline characteristics of patients without vs. with LVD. Parameters are indicated as mean ± SD, n (%), or median [1st, 3rd quartile].
Ventilatory and circulatory parameters at rest, during ramp exercise (at first ventilatory threshold) and at peak exercise for patients without vs. patients with LVD before start of exCR as well as change until completion of CR. Shown are medians and first and third quartiles in round brackets. Relative difference between groups is derived from group effect from adjusted models and is relative to values from group without LVD. P-values are derived from mixed linear models adjusted for age, sex and body mass index and with patients nested within centres as random intercepts.
Association of MACE with CPET parameter. Shown are estimates and 95% CI for MACE from the mixed linear models with the respective CPET parameter as dependent variable and covariates age and sex, and with site as random factor. Models were performed for patients with and without LVD and for the total population to test for a group interaction.

Study flow.
Regarding the changes in ventilatory parameters from before to after CR, patients with LVD had significantly greater reductions in resting VE (Table 2). They also had greater reductions in nadir VE/VCO2 (graphical abstract), and a greater increase in PETCO2 and RER at peak exercise.
Results from the mixed linear models including data also for the 1-year follow-up measurement as well as confounding factors age, sex and BMI showed a significantly greater reduction of VE at rest in the group of patients with LVD not only from before to after exCR but also to 1-year follow-up (Figure 2, Supplement Table 1a). BF at rest was higher in patients with LVD at all time points (Figure 2, Supplement Table 1a), and resting PETCO2 increased significantly at 1-year follow-up in both groups (Figure 3, Supplement Table 1a). At peak exercise, VE was reduced in the patients with LVD due to a significantly lower VT in the patients with LVD but increased with exCR and to 1-year follow-up in both groups (Figure 2, Supplement Table 1b),. Resting PETCO2 was lower by trend (p=0.0537) in patients with LVD and significantly lower at peak exercise at all time points (Figure 3, Supplement Table 1a and b). Accordingly, VE/VCO2 slope was increased in patients with LVD at all time points (Figure 3, Supplement Table 1c). VO2 relative to body weight was greatly reduced in patients with LVD at peak exercise (Figure 3, Supplement Table 1c) at all time points. Peak VO2 increased in both groups from before to after exCR and VE/VCO2 slope decreased over time. The physical component score was consistently lower by 3 points in patients with LVD but significant consistent improvements in SF36 PCS between time points were comparable in both groups with nearly 3 points between T0 and T2 (Supplement Table 1c).

Predicted means with 95% confidence intervals based on the mixed linear models for ventilation (a), breathing frequency (b), and tidal volume (c) at rest and at peak exercise (d-f) adjusted for age, sex, and body mass index, with patients nested within centres as random intercepts.

Predicted means with 95% confidence intervals based on the mixed linear models for VE/VCO2 slope (a), peak VO2 (b), and end-tidal carbon dioxide partial pressure at rest (c) and at peak exercise (d) adjusted for age, sex, and body mass index, with patients nested within centres as random intercepts.
Approximately 20% of patients with and without LVD had a MACE within 1-year follow-up with no difference between groups (p-value for Chi-square test 0.069). Nadir of VE/VCO2 significantly discriminated patients with and without MACE in patients with and without LVD (graphical abstract), while VE/VCO2 slope and peak VO2 discriminated for MACE only in patients without LVD, and peak PETCO2 and resting BF discriminated for MACE only in patients with LVD.
Discussion
This study provides four clinically relevant and novel aspects in a representative European cohort of elderly patients with coronary artery disease undergoing exCR: 1) Nearly one fifth of patients had asymptomatic LVD at the start of exCR; 2) LVD was associated with elevated ventilation at rest and an impaired pulmonary gas exchange during exercise; 3) exCR was associated with an improvement of ventilation at rest and gas exchange parameters during exercise, but ventilatory efficiency and PETCO2 remained significantly reduced in patients with LVD, compared to patient without LVD in the 1-year follow-up; and 4) BF at rest, ventilatory efficiency and PETCO2 during exercise were associated with worse outcome in patients with LVD.
This is the first large study demonstrating an increased resting ventilation and impaired pulmonary gas exchange during exercise in patients with LVD without major signs and symptoms of congestive heart failure. NYHA functional class did not differ between patients with and without LVD and 86% of patients in both groups were in NYHA functional class I. Furthermore, self-reported physical activity did not differ between the groups. Although the median physical component score of the SF36 questionnaire was 3 points lower in patients with LVD compared to patients without LVD, the values of 44.3 at T0 and 47.5 at T2 were clearly above the median of 35.3 found in patients with chronic heart failure.(29)
We suggest that signs of an exaggerated ventilatory drive are already apparent in patients with LVD at rest (higher resting VE and BF), during exercise (increased VE/VCO2 slope and nadir VE/VCO2), and at peak exercise (lower VO2, VT and PETCO2). Reductions of the exaggerated ventilatory drive seen with exCR were similarly beneficial in patients with and without LVD. The decrease in nadir VE/VCO2 was significantly greater in patients with LVD than in those without LVD, with similar magnitude of the difference between changes in VE/VCO2 slope, albeit not reaching statistical significance. This is in accordance to some previous studies that found ventilatory efficiency to improve most in patients with most severe ventilatory inefficiency at baseline. For example, in a study with 131 patients after acute myocardial infarction without HF participating in exCR, VE/VCO2 slope improved most in patients with VE/VCO2 slope>32,(30) which was also confirmed by a study comparing the effect of aerobic training to a combination of aerobic and strength training.(31) Similarly, a study in patients with HFrEF by Servantes et al. found large decreases in VE/VCO2 slopes with mean pre-exercise values of 36.(32) In part, a larger decrease in patients with higher starting values may be due to a phenomenon referred to as “regression to the mean”.(33) In a study including 123 CAD patients, patients in the group with peak VO2<17.5 ml/kg/min also had the highest nadir VE/VCO2.(34) This group also had the highest improvement in peak VO2 and nadir VE/VCO2 after exCR. Likewise, in 37 CAD patients completing exCR, PETCO2 at the first and second ventilatory threshold and peak exercise were improved after the programme. On the contrary, Fu et al. did not demonstrate an improvement of the VE/VCO2 slope with exercise training in patients with HFrEF and VE/VCO2 slope of 35 at baseline.(19)
At peak exercise, peak ventilation was 3 l/min (6%) less in patients with compared to patients without LVD, while peak VO2 was reduced by 2.2 ml/kg/min (12%). The disproportionate reduction in gas exchange was likely to be due to the significantly smaller peak VT (150 ml or 8%) in patients with LVD at an insignificantly increased peak BF, resulting in a larger anatomical dead space. This is in line with observation in patients with HFrEF,(35) and the emerging evidence that HF patients adopt a “rapid shallow” breathing pattern to avoid the adverse effects of large intrathoracic pressure swings on cardiac pre- and afterload.(2) Importantly, our study extends the evidence on abnormal breathing patterns and hyperventilation in patients with HFrEF to patients with LVD. The significantly higher resting HR in patients with LVD compared to patients without LVD is compatible with sympathetic hyperactivity.(2, 36) This finding suggests that several proposed mechanisms for exaggerated ventilation in HFrEF (e.g. augmented peripheral and central chemosensitivity and an inordinately high degree of afferent neural traffic originating from within the locomotors muscles) may already be present in patients with asymptomatic LVD starting the vicious cycle that may progress LVD to HFrEF.(2) Interestingly, the models corrected for age, sex and BMI showed a significant positive relationship of BMI with PETCO2 at rest and at AT, and a significant inverse relationship with nadir VE/VCO2. This raises the question whether the obesity paradox not only applies to patients with HF but already to elderly patients with (and without) LVD.(37)
The observed normalisation of the excessive ventilation of patients with LVD after exCR may partly be ascribed to the beneficial effects of exercise training on ergoreflex sensitivity, and/or chemoreceptor activation.(36) Importantly, guideline directed medical and device therapies for HFrEF improve chemo- and baroreceptor function insufficiently, highlighting the importance of exercise in this population.(38)
While the VE/VCO2 slope is an established prognostic parameter in patients with HFrEF, only few studies have reported the physiologically inversely related parameter PETCO2 at rest and at peak exercise.(39, 40) Matsumoto and colleagues have found severity of HF in 112 patients with cardiac disease to be negatively associated with PETCO2 at rest and at peak exercise.(39) They found PETCO2 at peak exercise to be negatively associated with VE/VCO2 slope and VD/VT, but not with PaCO2. Arena and colleagues found a resting PETCO2 of <33 mmHg to discriminate significantly for cardiac events at 1-year follow-up and to significantly add discriminative power to VE/VCO2 slope.(40) Our study demonstrated consistent findings on the prognostic value of pulmonary gas exchange parameters in patients with LVD. The nadir VE/VCO2 and peak PETCO2 were associated with MACE. Moreover, as a novel finding, BF at rest was associated with MACE. The discriminative value of resting ventilation parameters for MACE deserves further investigation as both resting PETCO2 and BF have been found to be predictive for cardiovascular complications also in lung resection patients.(41)
The important role of low PETCO2 in patients with HFrEF and periodic breathing has been pointed out by a study by Apostolo and colleagues who restored a normal breathing pattern with inhalation of 2% CO2 in 95% of their study patients.(42) Likewise, inhalation of CO2 has been shown to stabilise breathing in patients with periodic breathing and Cheyne-Stokes respiration during sleep.(43-45) Breathing instabilities are recognised markers for poor prognosis in patients with HFrEF and highlight the central role of breathing patterns in the progression of HF.(46) Nevertheless, few therapies have been developed to address breathing patterns. A few small studies with encouraging results have employed slow breathing training in patients with heart failure.(47, 48)
Strengths of this study are the large sample size of a representative European cohort of elderly patients with coronary artery disease undergoing exCR, and the longitudinal as well as comprehensive assessment of ventilatory parameters at rest, during ramp exercise and at peak exercise. Furthermore, this is the first documentation of improved breathing pattern and pulmonary gas exchange both at rest and with exercise after completion of exCR in both patient with and without LVD.
This explorative study is limited by multiple testing. Therefore, confidence intervals and p-values have to be interpreted accordingly. Unfortunately, we did not have data on betablocker classes. Previous studies showed that carvedilol, an unselective ß1- and ß2-blocker, was associated with a lower VE/VCO2 slope and nadir VE/VCO2.(49, 50) However, standard treatment of ACS and CCS includes cardioselective betablockers like metoprolol. We can therefore only speculate that only a small proportion of the 93% of our patients have received an unselective betablocker. Further, ACE inhibitors have been shown to improve gas transfer and ventilation-perfusion.(51) Nevertheless, the higher percentage of ACE in patients with LVD could not completely offset their less efficient ventilation.
Logistic regressions for identification of CPET variables significantly improving MACE prediction were performed for the whole EU-CaRE cohort (including patients with open heart surgery and valve replacement) recently.(24) Due to the small sample size of our subgroup of patients with LVD, we did not perform logistic regression models in the present study.
Conclusion
Patients with LVD had an exaggerated BF at rest and an impaired pulmonary gas exchange during exercise. Abnormal breathing patterns may be an early and clinically relevant sign of LVD and linked to increased ergoreflex sensitivity and/or abnormal chemosensitivity. ExCR may contribute to improvements of breathing patterns and pulmonary gas exchange in this population. However, interventions aimed at specifically improving altered breathing patterns at rest and during exercise may have additive value and should be investigated.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgements
We would like to thank Judith Peterhans for her valuable contributions to study logistics and data collection, and Susana Pérez-Alves for the graphical abstract design.
Footnotes
Funding disclosure: The study was funded by the European Union’s Horizon 2020 research and innovation program under grant agreement number 634439 and by the Swiss State Secretariat for Education, Research and Innovation for the Swiss consortium partner.
Conflict of interest statement: AWJvH reports grants from Medtronic, grants and personal fees from Astra Zeneca, outside the submitted work, UZ reports grants and personal fees from Astra Zeneca, Bayer, BMS, Novartis, and MSD, and personal fees from Boehringer Ingelheim, Daiichi Sankyo, Eli Lilly, Trommsdorf, and Amgen, all outside the submitted work.
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos