
Abstract
There is an increasing interest in developing massive-size deep learning models in natural language processing (NLP) - the key technology to extract patient information from unstructured electronic health records (EHRs). However, there are limited studies exploring large language models in the clinical domain; the current largest clinical NLP model was trained with 110 million parameters (compared with 175 billion parameters in the general domain). It is not clear how large-size NLP models can help machines understand patients’ clinical information from unstructured EHRs. In this study, we developed a large clinical transformer model – GatorTron – using >90 billion words of text and evaluated it on 5 clinical NLP tasks including clinical concept extraction, relation extraction, semantic textual similarity, natural language inference, and medical question answering. GatorTron is now the largest transformer model in the clinical domain that scaled up from the previous 110 million to 8.9 billion parameters and achieved state-of-the-art performance on the 5 clinical NLP tasks targeting various healthcare information documented in EHRs. GatorTron models perform better in understanding and utilizing patient information from clinical narratives in ways that can be applied to improvements in healthcare delivery and patient outcomes.
Introduction
There has been an increasing interest in developing artificial intelligence (AI) systems to improve healthcare delivery and health outcomes by leveraging medical knowledge in electronic health records (EHRs). A critical step in developing medical AI systems is training machines to understand patients’ clinical characteristics captured in longitudinal EHRs. The more information we know about the patients, the better medical AI systems that we can develop. In recent decades, hospitals and medical practices in the United States (US) rapidly adopted EHR systems1,2, resulting in massive stores of electronic patient data, including structured (e.g., disease codes, medication codes) and unstructured (i.e., clinical narratives such as physicians’ progress notes and discharge summaries). Physicians and other healthcare workers widely use clinical narratives to document detailed patient information in free text, leading to >80% of important patient information buried in unstructured text.3 There is an increasing number of studies exploring the rich, more fine-grained information about the patients in clinical narratives that led to improved diagnostic and prognostic models.4,5 Nevertheless, free-text narratives cannot be easily used in computational models that usually require structured data. Researchers have increasingly turned to natural language processing (NLP) as the key technology to enable machines to understand clinical language used by humans to support various downstream clinical studies6.
Historically, researchers designed several critical subtasks in clinical NLP such as clinical concept extraction7 and relation extraction8. For a long time, researchers had to train different models for different NLP subtasks. Today, most NLP solutions are based on deep learning models9 implemented using neural network architectures – a fast-developing sub-domain of machine learning. Convolutional neural networks10 (CNN) and recurrent neural networks11 (RNN) have been successfully applied to NLP in the early stage of deep learning. More recently, the transformer architectures12 (e.g., BERT) implemented with a self-attention mechanism13 have become state-of-the-art, achieving best performance on many NLP benchmarks. 14–17 In the general domain, the transformer-based NLP models have achieved state-of-the-art performance for many NLP tasks including name entity recognition18–20, relation extraction21–25, sentence similarity26–28, natural language inference28–31, and question answering28,29,32,33. Notably, transformers perform more effectively by decoupling of language understanding (i.e., learning of language models using large unlabeled text corpora) and language utilization (i.e., applying the learned language models solving specific tasks often with labeled training data) into two independent phases, i.e., pretraining and fine-tuning. After successful pretraining, the learned language model can be used to solve a variety of NLP subtasks through fine-tuning, which is known as transfer learning – a strategy to learn knowledge from one task and apply it in another task34. Human language has a very large sample space – the possible combinations of words and sentences are innumerable. Recent studies show that large transformer models trained using massive text data are remarkably better than traditional NLP models in terms of emergence and homogenization.34
The promise of transformer models has led to further interest in exploring how increases in model and data size may improve massive-size (e.g., >billions of parameters) transformer models understanding clinical narratives. The Generative Pre-trained Transformer 3 (GPT-3) model35, which has 175 billion parameters and was trained using >400 billion words of text demonstrated superior performance and capability in many NLP tasks. In the biomedical domain, researchers developed BioBERT12 (with 110 million parameters) and PubMedBERT36 (110 million parameters) transformer models using text from PubMed literature. Nvidia developed BioMegatron models in the biomedical domain with different sizes from 345 million to 1.2 billion parameters37 using PubMed literature. However, few studies have explored large-size transformer models in the clinical domain due to the sensitive nature of clinical narratives that contain Protected Health Information (PHI) and the requirement of massive computing power. By developing not only larger models, but models that use clinical narratives, NLP may perform better in understanding and utilizing patient information in ways that can be applied to improvements in healthcare delivery and patient outcomes. To date, the largest transformer model using clinical narratives is ClinicalBERT38. ClinicalBERT has 110 million parameters and was trained using 0.5 billion words from the publicly available Medical Information Mart for Intensive Care III39 (MIMIC-III) dataset. It is unclear how transformer-based models developed using significantly more clinical narrative text and more parameters may improve medical AI systems in understanding, extracting, and utilizing patient information.
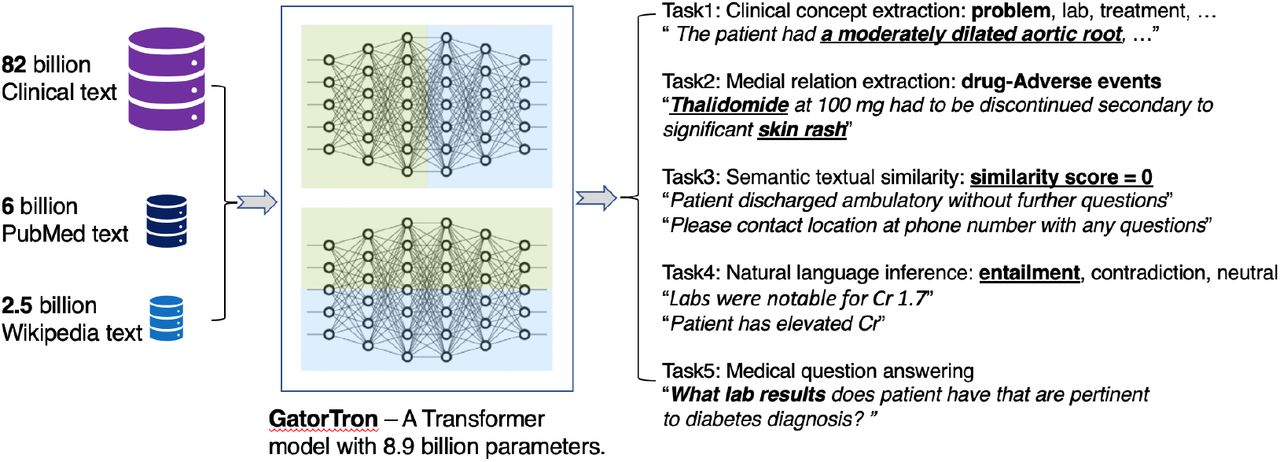
In this study, we developed a large clinical transformer model, GatorTron, using >90 billion words of text from the University of Florida (UF) Health, PubMed articles, and Wikipedia. We trained GatorTron from scratch and empirically evaluated three models with different settings including (1) a base model with 345 million parameters, (2) a medium model with 3.9 billion parameters, and (3) a large model with 8.9 billion parameters. We compared GatorTron models with existing large transformer models trained using biomedical literature and clinical narratives using 5 clinical NLP tasks including clinical concept extraction (or named entity recognition [NER]), medical relation extraction (MRE), semantic textual similarity (STS), natural language inference (NLI), and medical question answering (MQA). GatorTron outperformed previous transformer models from the biomedical and clinical domain on 5 clinical NLP tasks at different linguistic levels targeting various patient information. This study significantly scaled up transformer models in the clinical domain from 110 million to 8.9 billion parameters and improved our understanding of how large transformer models help AI systems understand and utilize patient information documented in clinical narratives.
Results
We collected all clinical narrative notes from the UF Health Integrated Data Repository (IDR) from 2011 to early 2021. The data included >82 billion medical words from >290 million notes related to >2 million patients and >50 million patient care encounters. We applied a standard preprocessing pipeline to remove duplicated notes and clean the clinical text – unify character encoding, identify tokens and sentence boundaries. Then, we merged the >82 billion words of clinical corpus with 6 billion words from PubMed (articles and abstracts)37, 2.5 billion words from Wikipedia37, and 0.5 billion words from the MIMIC-III corpus39 to generate a corpus with > 90 billion words. Using this corpus, we trained GatorTron with different settings (base - 345 million, medium - 3.9 billion, and large - 8.9 billion parameters) from scratch and fine-tuned GatorTron models for 5 clinical NLP tasks at different linguistic and complexity levels. Fig. 1 shows an overview of the study design. We used 6 public clinical benchmark datasets (Table 1 and Table 2) following the default training/test settings and calculated evaluation scores using official evaluation scripts associated with each benchmark dataset. Table 1 and Table 2 compare GatorTron models with two existing biomedical transformer models (BioBERT and BioMegatron) and one clinical transformer model (Clinical BERT) on the 5 clinical NLP tasks.
Comparison of GatorTron with existing biomedical and clinical transformer models for clinical concept extraction and medical relation extraction.
Comparison of GatorTron with existing biomedical and clinical transformer models for semantic textual similarity, natural language inference, and question answering.

An overview of study design.
Recognize clinical concepts and medical relations
Clinical concept extraction is a phrase-level task to identify the boundary of concepts with clinical meanings and classify their semantic categories (e.g., diseases, medications). As shown in Table 1, all three GatorTron models outperformed existing biomedical and clinical transformer models in recognizing various types of clinical concepts on the three benchmark datasets (i.e., 2010 i2b240 and 2012 i2b241: problem, treatments, lab tests; 2018 n2c242: drug, adverse events, and drug-related attributes). The GatorTron-large model outperformed the other two smaller GatorTron models and achieved the best F1-scores of 0.8996, 0.8091, and 0.9000, respectively, demonstrating performance gain from scaling up the size of the model. For medical relation extraction – a task to identify medical relations between two clinical concepts, the GatorTron-large model also achieved the best F1-score of 0.9627 for identifying drug-cause-adverse event relations outperforming existing biomedical and clinical transformers and the other two smaller GatorTron models. We consistently observed performance improvement when scaling up the size of the GatorTron model.
Assess semantic textual similarity
The task of measuring semantic similarity is to determine the extent to which two sentences are similar in terms of semantic meaning. As shown in Table 2, all GatorTron models outperformed existing biomedical and clinical transformer models in assessing the semantic similarity between two sentences. Among the three GatorTron models, the GatorTron-medium model achieved the best Pearson correlation score of 0.8903, outperforming both GatorTron-base and GatorTron-large. Although we did not observe consistent improvement by scaling up the size of the GatorTron model, the GatorTron-large model significantly outperformed GatorTron-base and its performance is very close to the GatorTron-medium model (0.8896 vs. 0.8903).
Natural language inference
The task of NLI is to determine whether a conclusion can be inferred from a given sentence – a sentence-level NLP task. As shown in Table 2, all GatorTron models outperformed existing biomedical and clinical transformers, and the GatorTron-large model achieved the best accuracy of 0.9020, outperforming the BioBERT and ClinicalBERT by 9.6% and 7.5%, respectively. We observed a monotonic performance improvement by scaling up the size of the GatorTron model.
Medical question answering
MQA is a complex clinical NLP task that requires understand information from the entire document. As shown in Table 2, all GatorTron models outperformed existing biomedical and clinical transformer models in answering medication and relation-related questions (e.g., “What lab results does patient have that are pertinent to diabetes diagnosis?”). For medication-related questions, the GatorTron-large model achieved the best exact match score of 0.3155, outperforming the BioBERT and ClinicalBERT by 6.8% and 7.5%, respectively. For relation-related questions, GatorTron-large also achieved the best exact match score of 0.9301, outperforming BioBERT and ClinicalBERT by 9.5% and 7.77%, respectively. We also observed a monotonic performance improvement by scaling up the size of the GatorTron model.
Discussion
In this study, we developed the largest clinical transformer model, GatorTron, using a corpus of >90 billion words from UF Health (>82 billion), Pubmed (6 billion), Wikipedia (2.5 billion), and MIMIC III (0.5 billion). We trained GatorTron with different model sizes including 345 million, 3.9 billion, and 8.9 billion parameters and evaluated its performance on 5 clinical NLP tasks with different complexity (phrase level, sentence level, and document level) using 6 publicly-available benchmark datasets from the clinical domain. The experimental results show that GatorTron models outperformed existing biomedical and clinical transformers for all 5 clinical NLP tasks evaluated using 6 different benchmark datasets. We observed monotonic improvements by scaling up the model size of GatorTron for 4 of the 5 tasks, excluding the semantic textual similarity task. Our GatorTron model also outperformed the BioMegatron37, a transformer model with a similar model size developed in our previous study using >8.5 billion words from PubMed and Wikipedia (a small proportion of the >90 billion words of corpus for developing GatorTron). This study scaled up the clinical transformer models from 345 million (ClinicalBERT) to 8.9 billion parameters in the clinical domain and demonstrated significant performance improvements. To the best of our knowledge, GatorTron-large is the largest transformer model in the clinical domain.
Scaling up model size and performance improvement
There is an increasing interest in examining massive-size deep learning models in NLP as they demonstrated novel abilities such as emergence and homogenization34, which are more close to human intelligence than previous models. In the general domain, the Megatron-Turing NLG model has scaled up to 530 billion parameters following the GPT-335 model with 175 billion parameters. However, there are limited studies examining large transformer models in the clinical domain due to the sensitive nature of clinical text and massive computing requirements. Prior to our study, the largest transformer in the clinical domain was ClinicalBERT with 110 million parameters trained using 0.5 billion words. Our study successfully scaled the transformer from 110 million to 8.9 billion parameters and demonstrated performance improvement for 5 clinical NLP tasks on 6 public benchmark datasets. Among the 5 tasks, GatorTron achieved significant improvements for complex NLP tasks such as natural language inference and medical question answering, but moderate improvements for easier tasks such as clinical concept extraction and medical relation extraction, indicating that large transformer models are more helpful to complex clinical NLP tasks.
Model size and converge speed
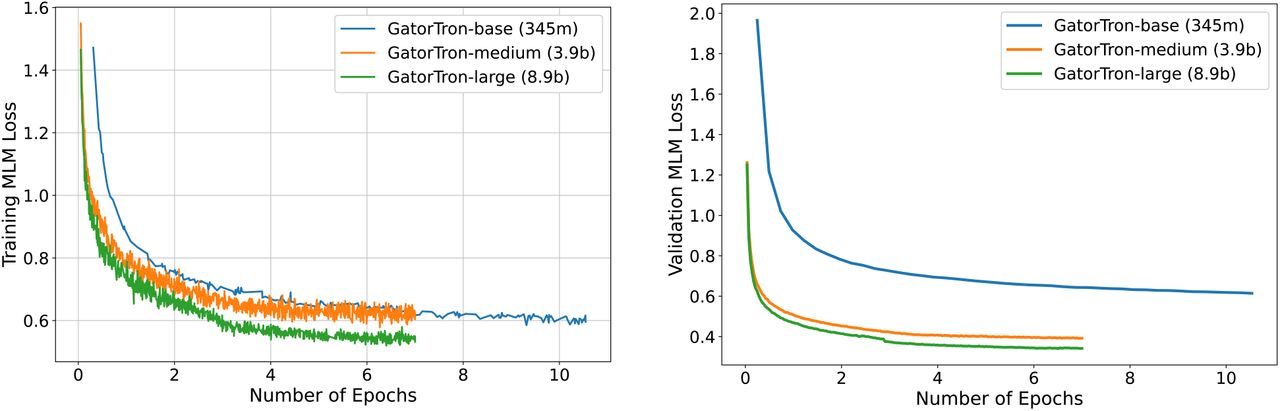
GatorTron was pretrained using unsupervised learning to optimize a mask language model (MLM). We monitored training loss and calculated validation loss using a subset set of the clinical text (5%) to determine when to stop the training. Fig. 2 shows the training loss and validation loss for GatorTron models with three different settings. We observed that the larger GatorTron models converged faster than the base model. For example, the GatorTron-base model converged in 10 epochs, whereas the medium and large models converged in 7 epochs. This may indicate that larger transformer models learn faster than smaller models. The training of the GatorTron-large model used about 6 days on 992 GPUs from 124 Nvidia SuperPOD nodes.

{kind=link}
{kind=link}
Training loss and validation loss for GatorTron base (345 million), medium (3.9 billion), and large (8.9 billion) models.
Potentials in improving healthcare delivery and patient outcomes
GatorTron models perform better in understanding and utilizing patient information in clinical narratives, which can be applied to various medical AI systems to improve healthcare delivery and patient outcomes. The rich, fine-grained patients’ information captured in clinical narratives is a critical resource powering medical AI systems. With better performance in information extraction tasks (e.g., clinical concept extraction and medical relation extraction), GatorTron models can provide more accurate patients’ information to identify research-standard patient cohorts using computable phenotypes, support physicians making data-informed decisions by clinical decision support systems, and identify adverse events associated with drug exposures via pharmacovigilance. The significant improvements in semantic textual similarity, natural language inference, and medical question answering can be applied for deduplication of clinical text, mining medial knowledge, and developing next-generation medical AI systems that can interact with patients using human language. The emergence and homogenization abilities34 inherited from a large transformer architecture make it convenient to apply GatorTron to many other AI tasks through fine-tuning. We believe that GatorTron will improve the use of clinical narratives in developing various medical AI systems for better healthcare delivery and health outcomes.
Methods
Data Source
The primary data source for this study is the clinical narratives from UF Health IDR, a research data warehouse of UF Health. We collected a total of 290,482,002 clinical notes from 2011-2021 from over 2 million patients and 50 million encounters. After removing empty notes and duplicated notes, we generated a UFHealth clinical corpus with over 82 billion tokens. Then, we merged the UFHealth clinical corpus with three additional corpora, including the MIMIC-III corpus39 in the clinical domain with 0.5 billion words, a PubMed (combining PubMed abstracts and full-text commercial-collection) collection37 in the biomedical domain with 6 billion words, and a Wikipedia articles dump37 in the general domain with 2.5 billion words, to generate a corpus with >90 billion words. We performed minimal preprocessing including tokenization and sentence boundary detection.
Study design
We seek to train a large clinical transformer model, GatorTron, using >90 billion words and examine how and whether scaling up mode size improves model performance on clinical NLP tasks. Following standard practice, we first pretrained GatorTron using the >90 billion words as an unsupervised learning procedure and then applied GatorTron to 5 different clinical NLP tasks using a supervised fine-tuning procedure. We adopted the BERT architecture implemented in MagaTron-LM and explored three different settings including a base model of 345 million parameters (i.e., GatorTron-base), a medium model of 3.9 billion parameters (i.e., GatorTron-medium), and a large model of 8.9 billion parameters (i.e., GatorTron-large). Then we compared the three GatorTron models to an existing transformer model from the clinical domain, ClinicalBERT (trained with 110 million parameters) and two transformer models from the biomedical domain, including, BioBERT (345 million parameters) and BioMegatron (1.2 billion parameters). We examined the models on 5 clinical NLP tasks, including clinical concept extraction, relation extraction, semantic textual similarity, natural language inference, and medical question answering. We used 6 public benchmark datasets in the clinical domain.
Training environment
We used a total number of 992 Nvidia DGX A100 GPUs from 124 superPOD nodes at UF’s HiperGator-AI cluster to train GatorTron models by leveraging both data-level and model-level parallelisms implemented by the Megatron-LM package46. We monitored the training progress by training loss and validation loss and stopped the training when there was no further improvement (i.e., the loss plot became flat).
GatorTron Model Configuration
We developed GatorTron models with three configurations and determined the number of layers, hidden sizes, and number of attention heads according to the guidelines for optimal depth-to-width parameter allocation proposed by Levin et al47 as well as our previous experience in developing BioMegatron. Table 3 provides detailed information for the three settings. The GatorTron-base model has 24 layers of transformer blocks, which is similar to the architecture of BERT large model. For each layer, we set the number of hidden units as 1024 and attention heads as 16. The GatorTron-medium model scaled up to 3.9 billion parameters (~10 times of the base setting) and the GatorTron-large model scaled up to 8.9 billion parameters, which is similar to BioMegatron46 (with 8.3 billion parameters).
Existing transformer models for comparison
BioBERT
12 The BioBERT model was developed by further training the original BERT-large model (345 million parameters, 24 layers, 1024 hidden units, and 16 attention heads) using biomedical literature from PubMed Abstracts (4.5 billion words) and PMC Full-text articles (13.5 billion words). In this study, we used version 1.1.
ClinicalBERT
38 The ClinicalBERT model was developed by further training the BioBERT (base version; 110 million parameters with 12 layers, 768 hidden units, and 12 attention heads) using clinical text from the MIMIC-III39 corpus.
BioMegatron
37 The BioMegatron models adopted the BERT architecture with a different number of parameters from 345 million to 1.2 billion. Different from BioBERT and ClinicalBERT, the BioMegatron was trained from scratch without leveraging the original BERT model.
Clinical NLP tasks, evaluation matrices, and benchmark datasets
We evaluated GatorTron models using five clinical NLP tasks at different linguistic levels.
Clinical concept extraction
This is a task to recognize phrases with important clinical meanings (e.g., medications, treatments, adverse drug events). The NLP system has to determine the boundaries of a concept and classify it into predefined semantic categories. Early systems for clinical concept extract are often rule-based, yet, most recent systems are based on machine learning models such as conditional random fields (CRFs)48,49, convolutional neural networks (CNN)10,50, and recurrent neural networks (RNN) implemented with long short-term memory strategy (LSTM)11,51. Current state-of-the-art models are based on transformers such as the ClinicalBERT. We used three benchmark datasets developed by the 2010 i2b2 challenge, 2012 i2b2 challenge, and 2018 n2c2 challenge to evaluate GatorTron models focusing on identifying important medical concepts (e.g., medications, adverse drug events, treatments) from clinical text. We used standard precision, recall, and F1-score for evaluation.
Medical Relation extraction
MRE is to establish medical-related relations (e.g., induce relation) among clinical concepts (e.g., drugs, adverse events), which is a crucial task for high-level clinical NLP applications. MRE is usually approached as a classification problem – identify and classify pairs of concepts with valid relations. Various machine learning-based classifiers such as support vector machines (SVMs), random forests (RF), and gradient boosting trees (GBT)42 have been applied. With the emergence of deep learning models, researchers have explored the long-short term memory (LSTM) architecture for RE in both general and clinical domains52,53. Most recently, several studies adopted the BERT architecture and demonstrated superior performance for MRE on various datasets54–59. In this study, we used the dataset developed by the 2018 n2c2 challenge with a focus on relations between medications and adverse drug events. The standard precision, recall, and F1-score were used for evaluation.
Semantic textual similarity
The STS task is to quantitatively assess the semantic similarity between two text snippets (e.g., sentences), which is usually approached as a regression task where a real-value score was used to quantify the similarity between two text snippets. In the general domain, the STS benchmark (STS-B) dataset curated by the Semantic evaluation (SemEval) challenges between 2012 and 201760 is widely used for evaluating STS systems14. Various machine learning methods have been examined61–63 but transformer-based systems such as RoBERTa26, T528, and ALBERT29 are leading the state-of-the-art models for STS. In the clinical domain, the MedSTS dataset64 that consists of over 1000 annotated sentence pairs from clinical notes at Mayo Clinic was widely used as the benchmark. MedSTS was used as the gold standard in two clinical NLP open challenges including the 2018 BioCreative/Open Health NLP (OHNLP) challenge65 and 2019 n2c2/OHNLP ClinicalSTS shared task43. Similar to the general domain, pretrained transformer-based models using clinical text and biomedical literature, including ClinicalBERT and BioBERT66, are state-of-the-art solutions. In this study, we used the dataset developed by the 2019 n2c2/OHNLP challenge on clinical semantic textural similarity43. We used the Pearson correlation score for evaluation.
Natural language inference
NLI is also known as recognizing textual entailment (RTE) - a directional relation between text fragments (e.g., sentences)67. The goal of NLI is to determine if a given hypothesis can be inferred from a given premise. In the general domain, two benchmark datasets - the MultiNLI68 and the Stanford NLI69 are widely used. On both datasets, pretrained transformer models achieved state-of-the-art performances28,30. There are limited resources for NLI in the clinical domain. Until recently, the MedNLI – a dataset annotated by doctors based on the medical history of patients44 was developed as a benchmark dataset in the clinical domain. A previous study38 showed that a pretrained clinical BERT model achieved the state-of-the-art performance and outperformed the baseline (InferSent70) by ~9% accuracy. In this study, we evaluated the Gatortron models on NLI using the MedNLI dataset and used accuracy for comparison.
Medical question answering
The MQA task is to build NLP systems that automatically answer medical questions in a natural language, which is the most complex challenge among the 5 tasks. Unlike other tasks focusing on phrases and sentences, MQA is a document-level task that requires information from the whole document to generate answers according to questions. In the general domain, the Stanford Question Answering Datasets (SQuAD 1.1 and 2.0)71,72 have been widely used as benchmarks. Transformer-based models are the state-of-the-art for both SQuAD1.119 and SQuAD2.032. There are several MQA datasets developed in the past few years such as the MESHQA73, MedQuAD74, and emrQA45. In this study, we used the emrQA dataset, which is widely used as a benchmark dataset for MQA. We particularly focused on medications and relations-related questions as Yue et al.75 found that the two subsets are more consistent. We utilized both F1-score and exact match score for evaluation.
Data Availability
All data produced are available online at N2C2 https://n2c2.dbmi.hms.harvard.edu/data-sets
Funding
This study was partially supported by a Patient-Centered Outcomes Research Institute® (PCORI®) Award (ME-2018C3-14754), a grant from the National Cancer Institute, 1R01CA246418 R01, grants from the National Institute on Aging, NIA R56AG069880 and R21AG062884, and the Cancer Informatics and eHealth core jointly supported by the UF Health Cancer Center and the UF Clinical and Translational Science Institute. The content is solely the responsibility of the authors and does not necessarily represent the official views of the funding institutions.
Support from UF Research Computing
We would like to thank the UF Research Computing team, led by Dr. Erik Deumens, for providing computing power through UF HiperGator-AI cluster.
Author contributions
YW, JB, MGF, NP, and XY were responsible for the overall design, development, and evaluation of this study. XY had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis. YW, XY JB, and WH did the bulk of the writing, EAS, DAM, TM and CAH also contributed to writing and editing of this manuscript. All authors reviewed the manuscript critically for scientific content, and all authors gave final approval of the manuscript for publication.
Competing interests
Authors have no competing financial interests.
Materials & Correspondence
Yonghui Wu, PhD
Statistical information
N/A
Data availability
The benchmark datasets that support the findings of this study are available from the official websites of natural language processing challenges.
Computer code
The computer codes to train GatroTron models are available from: https://github.com/NVIDIA/Megatron-LM and https://github.com/NVIDIA/NeMo.
Acknowledgments
References and Notes



