
ABSTRACT
Introduction Shared decision making is as an essential principle for cardiovascular disease (CVD) prevention, where asymptomatic people are considering lifelong medication and lifestyle changes. This project aimed to develop and evaluate the first literacy-sensitive CVD prevention decision aid (DA) developed for people with low health literacy, and investigate the impact of literacy-sensitive design and heart age.
Methods We developed the standard DA based on international standards. The literacy-sensitive version included simple language, supporting images, white space and a lifestyle action plan. A randomised trial included 859 people aged 45-74 using a 3 (DA: standard, literacy-sensitive, control) x 2 (heart age: heart age + percentage risk, percentage risk only) factorial design, with outcomes including prevention intentions/behaviours, gist/verbatim knowledge of risk, credibility, emotional response and decisional conflict. We iteratively improved the literacy-sensitive version based on end user testing interviews with 20 people with varying health literacy levels.
Results Immediately post-intervention (n=859), there were no differences between the DA groups on any outcome. The heart age group was less likely to have a positive emotional response, perceived the message as less credible, and had higher gist/verbatim knowledge of heart age risk but not percentage risk. After 4 weeks (n=596), the DA groups had better gist knowledge of percentage risk than control. The literacy-sensitive decision aid group had higher fruit consumption, and the standard decision aid group had better verbatim knowledge of percentage risk. Verbatim knowledge was higher for heart age than percentage risk amongst those who received both.
Discussion The literacy-sensitive DA resulted in increased knowledge and lifestyle change for participants with varying health literacy levels and CVD risk results. Adding heart age did not increase lifestyle change intentions or behaviour but did affect psychological outcomes, consistent with previous findings.
MeSH Terms Health Literacy, Cardiovascular Diseases, Decision Making (Shared), Life Style, Decision Support Techniques
INTRODUCTION
Prevention of cardiovascular disease (CVD) includes lifestyle interventions and medication for those at highest risk who are most likely to benefit. An “absolute risk” approach is supported by clinical evidence and endorsed by most national guidelines around the world1–5. The absolute risk of a heart attack or stroke in the next 5-10 years can be assessed using widely available calculators1, but there is substantial underuse of these tools in practice6–11. Providing medication to high risk and not low risk patients is a cost-effective approach6. However, up to 75% of high risk patients are not receiving recommended medication to prevent death and disability from CVD, while 25% of low risk patients are taking medication they are very unlikely to benefit from7. Recent guideline changes have led to calls for a shared decision making approach, to ensure medication prescribing for blood pressure and cholesterol is more in line with patient values12–14.
We also know that health literacy plays a role in CVD prevention. Low health literacy is common in many countries, with estimates ranging from 36 – 60% of the population in Australia, Europe and the US15–17. This is associated with poorer self-management, less access to the health system, increased chronic disease including CVD, and increased mortality18. It is therefore important to specifically engage this group in communication strategies about CVD prevention. This requires changes to the design of online patient resources, since most consumers seek health information online, but fewer than 1% of health information websites meet recommended readability levels; Grade 8 is recommended to meet the needs of people with varying health literacy19,20.
Some countries have used online CVD risk assessment tools for absolute risk and heart age to engage consumers in CVD prevention, with millions of users worldwide21–24. However, our systematic review of 73 online CVD risk assessment tools available to consumers found they were not suitable for people with lower health literacy: their readability level was too high; they frequently used unexplained medical terms; few used best practice risk communication formats such as frequencies in icon arrays; and they rated poorly on actionability (i.e. clarity in instructions of what actions/steps to take), which makes it hard for the average person to know what to do about the risk assessment result25. Our review of 25 online decision aids for CVD prevention found similar issues with understandability and actionability26, and few included lifestyle change as an option reduce risk with many focusing on medication only.
There are several evidence-based strategies to address the issue of communicating CVD risk to people with lower health literacy:
Use literacy-sensitive design to improve the readability of health information and reduce the cognitive load of action plans for behaviour change27–29.
Use best practice risk communication formats to explain abstract probabilities (e.g. 16%) using icon arrays and more concrete frequencies (e.g. 16 out of 100 people like you)30–33.
Use patient decision aids to improve understanding and decision making, including both lifestyle change and medication as clear actions that patients can take to reduce their risk27,34,35.
This project aimed to develop and test a new consumer engagement tool for CVD prevention based on the above strategies, to address the needs of Australians with different levels of health literacy. It builds on our previous development of a GP-focused risk calculator and decision aid36, and evaluation of the national heart age calculator24.
METHODS
Stage 1: Develop consumer engagement tool
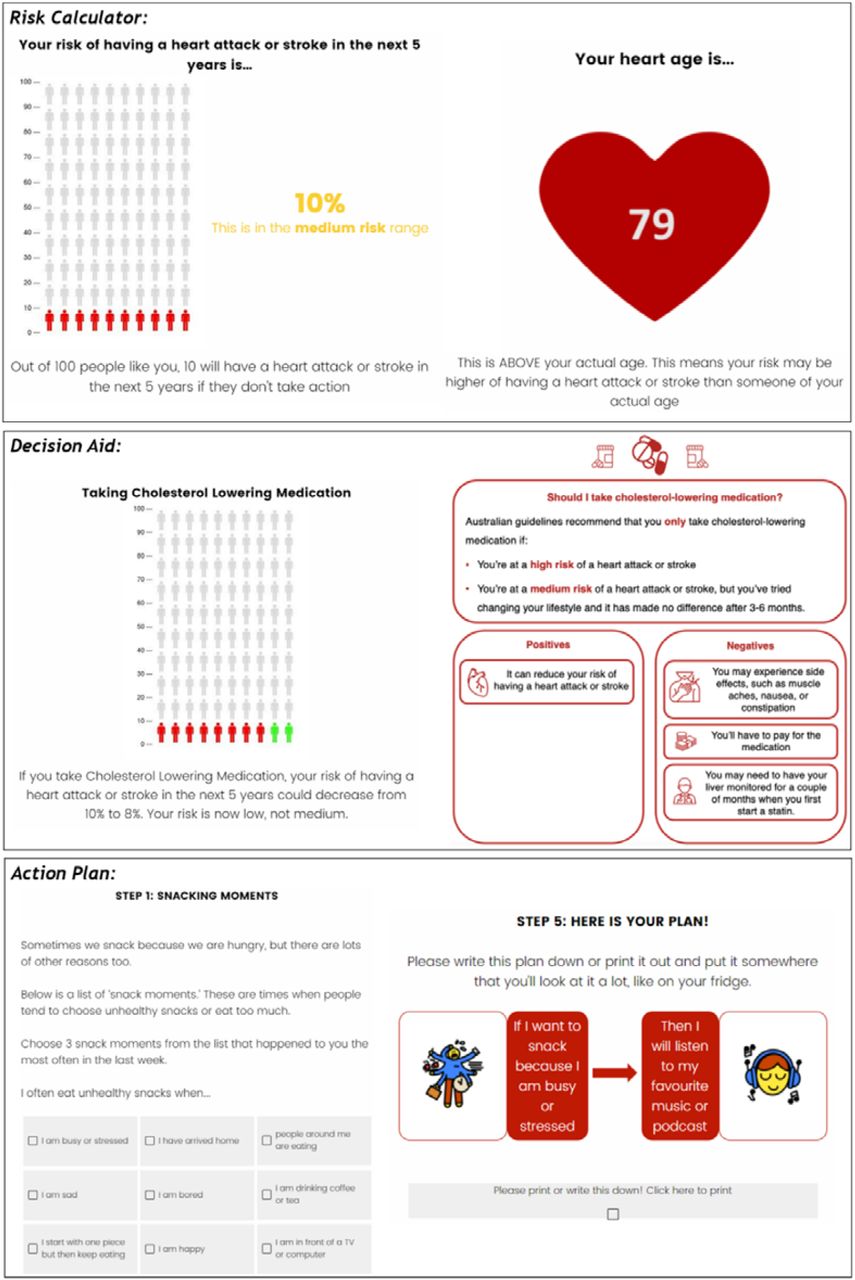
In stage one we developed the literacy-sensitive version of our existing GP decision aid37, which calculates 5 year risk of a CVD event based on current guidelines1 and shows the effects of 9 lifestyle, medication and supplement interventions36. We added heart age to the absolute CVD risk calculation based on published methods38. The literacy-sensitive design included simple language, supporting images and white space to improve readability and understandability28, and a novel action plan format our team developed that has been shown to reduce unhealthy lifestyle behaviours amongst people with low health literacy29. We added options for physical activity and smoking to the existing tool to reduce unhealthy snacking, drawing on previous literature on effective if-then plans in these areas39,40.
Stage 2: Randomised trial to identify best formats for low vs high health literacy
Design
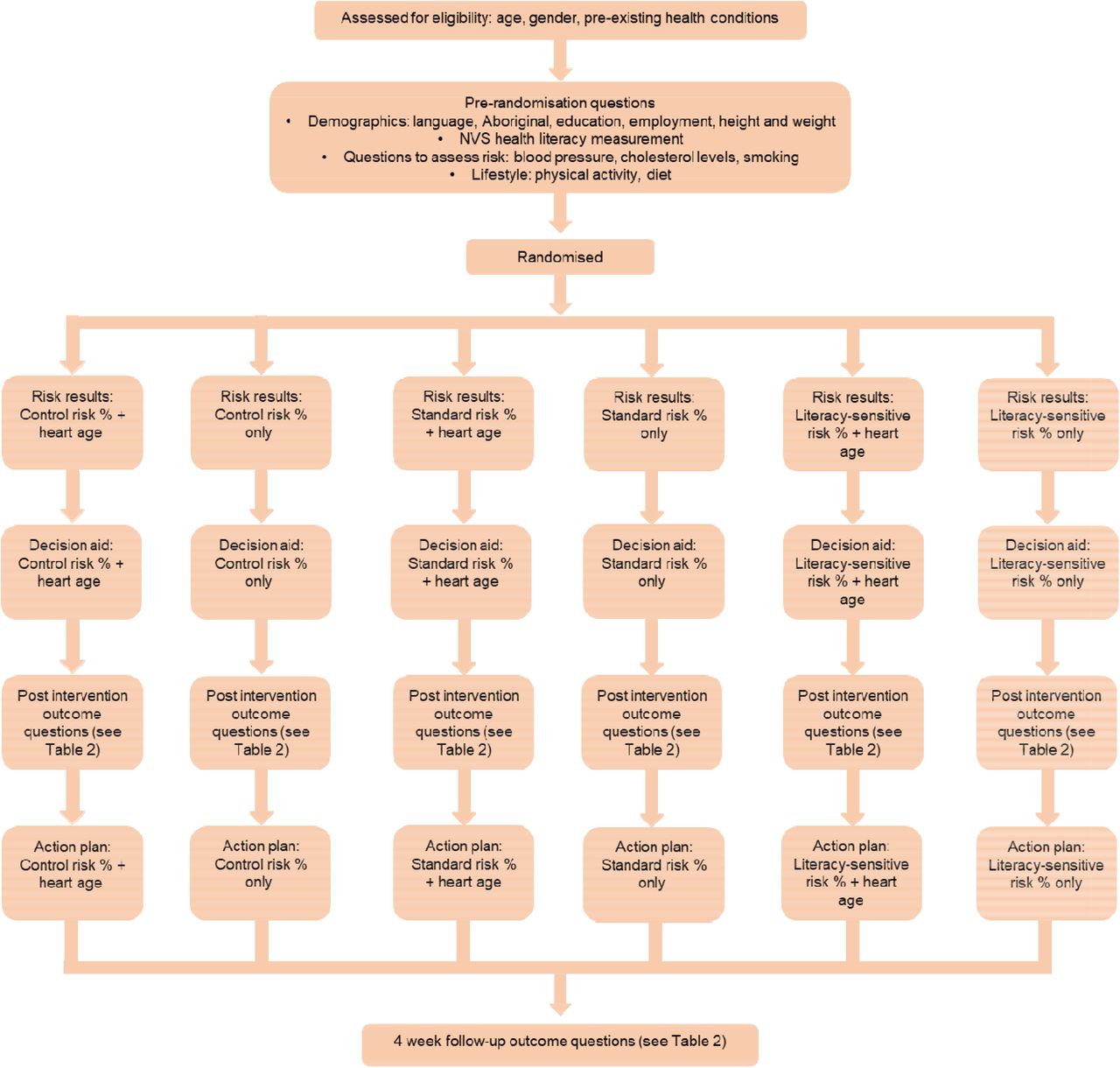
The randomised trial was based on a 3×2 factorial design to test the effect of literacy-sensitive design (literacy-sensitive DA, standard DA, or control: Heart Foundation patient information) and risk format (explaining CVD risk only (as a percentage risk), or CVD risk percentage + heart age) on psychological and behavioural outcomes. See Table 1/Figure 1 for study design, and Figure 2/Appendix 1 for example intervention content. The trial was pre-registered at ANZCTR (Trial number ACTRN12620000806965).
Recruitment
A national sample was recruited through Qualtrics, an online social research agency, with stratified sampling based on gender/age groups (5 year age groups from 45-74 years). Participants completed a CVD risk assessment based on Australian guidelines and the New Zealand approach to calculating heart age1,38. If blood pressure or cholesterol were not known, the average by age/gender based on non-diabetic participants in the AusDiab cohort was used (accessed via JD), and all participants were advised to see a GP for a more accurate risk assessment. Those with established CVD or taking CVD prevention medication were excluded. Duplicate IP addresses were replaced, and stratified sampling was relaxed with additional quality checks added if hard to reach groups did not reach quota after 2 weeks.
Measures
Established measures were used for the primary outcome of behavioural intentions (validated Theory of Planned Behaviour scale applied to smoking, diet, exercise and GP visit)45–47. Secondary outcomes included: self-reported behaviour after 4 weeks compared to national guidelines for diet and physical activity46,47; gist and verbatim knowledge (absolute risk percentage and heart age); emotional response using the PANAS scale (three positive emotions e.g. hopeful, three negative emotions e.g. anxious)48; credibility of the information (that the information is personally relevant)49; and decision conflict scale (uncertainty in decision making)50. Full details are in Table 2.
Analysis
A priori sample size calculations determined that 85 participants per randomised group (total n=510) would yield 90% power to detect a moderate effect size of d=0.5 (standardised difference) in the primary outcome of intention to change lifestyle or any of the secondary outcomes, assuming a two-sided alpha of 0.05. We aimed to recruit 20% more cases to account for potential missing values, totalling 600 participants (100 per group) at follow-up. This sample was inflated for recruitment to 850 to account for potential attrition of up to 30% between the intervention and follow-up.
Continuous outcome variables were modelled using linear regression. Dichotomous outcomes were analysed using modified Poisson regression (using a log-link function with robust error variances). Ordinal logistic regression was used to analyse ordered categorical outcomes. Count outcomes were modelled using negative binomial regression. All regression models included decision aid group (literacy-sensitive decision aid; standard decision aid; or basic Heart Foundation patient information) and risk format (CVD risk percentage only, or CVD risk percentage + heart age) as categorical variables and controlled for health literacy adequacy (categorical based on the Newest Vital Sign (NVS) measure51,52: low; moderate; adequate) and absolute risk (percentage). Post-intervention and follow-up outcomes were analysed separately, with follow-up analyses controlling for pre-intervention values where available. Pairwise comparisons were conducted to address the hypotheses. We also conducted exploratory analyses of potential differences in decision aid effects between health literacy levels by including a literacy-sensitive-by-decision aid interaction term, and by heart age category for heart age groups (younger/same vs older in stratified analyses). McNemar’s Chi-squared test for paired proportions was used to compare knowledge of heart age versus percentage risk amongst those who saw both. Analyses were conducted using Stata/IC v16.1 (StataCorp, College Station, TX, USA).
Hypotheses
The 2 decision aid formats will be more effective than standard Heart Foundation information;
The literacy-sensitive decision aid will be more effective than the standard decision aid for everyone (not just people with lower health literacy);
Adding heart age to absolute risk will be more effective than absolute risk alone.
Stage 3: Iterative end user testing with varying health literacy levels
Participants in the trial were invited to opt-in to a “think aloud” interview to provide further end user testing and feedback for the literacy-sensitive version of the intervention. Participants went through the risk calculator in full, while saying out loud everything they were thinking, for example any areas of confusion. Further questions were also asked to prompt more discussion or elaboration. Transcripts were thematically coded and discussed after each set of 4-5 interviews, and improvements were made to the intervention before the next set of interviews. We conducted 2 rounds of interviews for people with low health literacy as our key target group (n=8), and then tested the improved tool with people who had higher health literacy to ensure it was suitable for these users in another two rounds (n=12).
RESULTS
Stage 1
We used the question format and style of the current national heart age calculator as the basis for the risk factor questions in all groups, and also based the heart age presentation on that tool. The CVD risk results and decision aid were presented based on: 1) our existing GP decision aid tool37 (standard decision aid group); 2) a simplified version of the standard decision aid with supporting images (literacy-sensitive decision aid group, see Figure 2); and 3) the current risk calculator from the National Vascular Disease Prevention Alliance41. See Appendix 1 for example intervention content in each group.
Stage 2
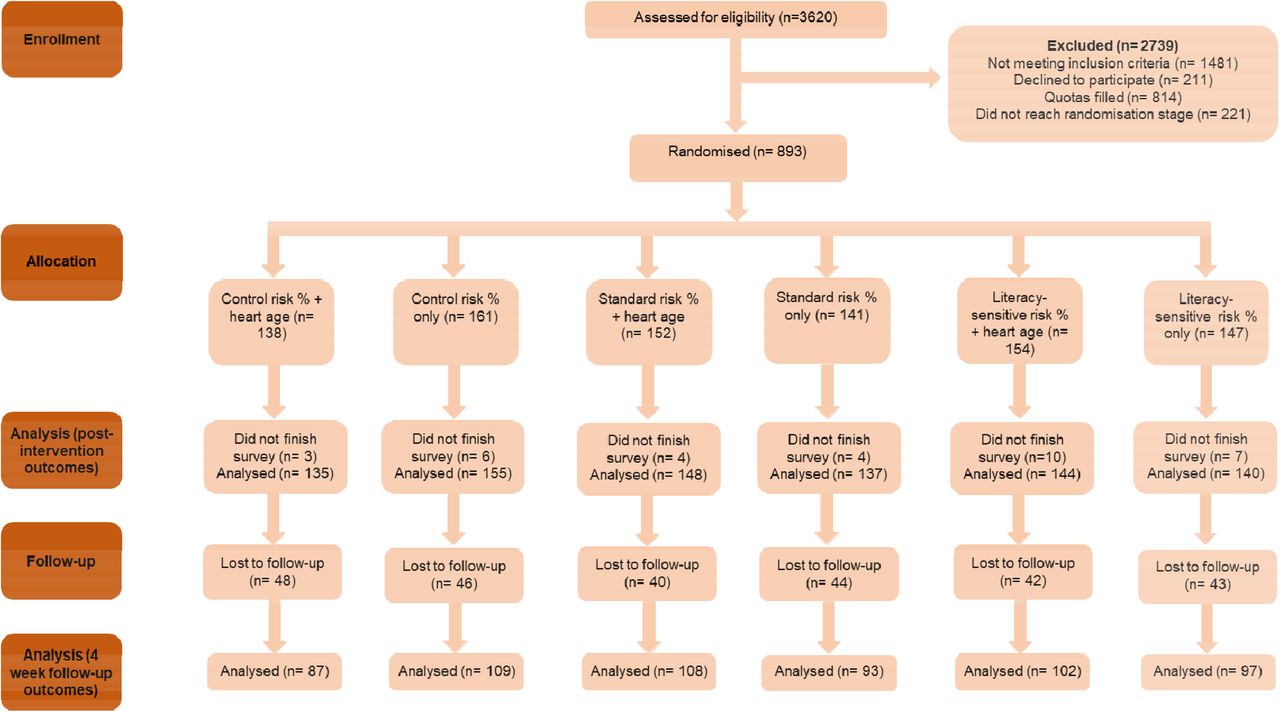
The CONSORT diagram is shown in Figure 3, and characteristics of all participant groups in the intervention are shown in Table 3. We conducted a soft launch of n=100 participants to check we had an adequate low health literacy sample and adequate follow-up considering COVID-19 disruptions in 2020, before proceeding with the full trial with no changes to the pre-registered method. We recruited 859 participants for the intervention (including the 100 in the soft launch), with a target of 600 at 4 week follow-up, for which we recruited 596. Characteristics were similar between groups for age and gender, but some differences were observed for health literacy (relating to education) and absolute risk (relating to smoking and heart age), so these two factors were controlled for in the analyses. In terms of drop-out, there was no difference in randomised decision aid group (p=.71), randomised to heart age shown (p=.91), health literacy level (p=.69), CVD risk level (p=.56), or heart age result (p=.30) between those who returned for follow-up and those who did not. Outcomes by trial group are shown in Table 4; and analyses for each of the 3 hypotheses are shown in Tables 5-7.
{kind=link}
{kind=link}
{kind=link}
Post-intervention differences between decision aid groups
Immediately post-intervention, there were no differences between the 3 decision aid groups for the primary outcome of lifestyle intentions, or secondary outcomes of risk perception, credibility, emotional response or decisional conflict. For Hypothesis 1, the combined decision aid groups were no different to the control condition for any outcome (Table 5). For Hypothesis 2, there was no difference between the standard and literacy-sensitive decision aids for any outcome (Table 6). There were significant interactions between decision aid and health literacy for intention to talk to a doctor about medication (p=0.019) and emotional response (positive p=0.010; negative p=0.006). Participants with lower health literacy who received the literacy-sensitive decision aid had a more negative/less positive emotional response and had stronger intentions to see a doctor about medication, compared to the other groups (Table 6).
4 week differences between decision aid groups
At follow-up after 4 weeks, there were no significant differences between the control and decision aid groups for most self-reported behaviours. However, the literacy-sensitive decision aid group had higher fruit consumption compared to both control (difference in predicted counts = 0.69 (95%CI: 0.32 to 1.06); p<.001) and the standard decision aid group (difference in predicted counts = 0.48 (95%CI: 0.11 to 0.86); p=.012). The decision aid groups were both more likely to know whether their risk was low, medium or high than the control group (literacy-sensitive DA: IRR=1.28 (95%CI: 1.04 to 1.58); p=.021; standard DA: IRR=1.41 (95%CI: 1.14 to 1.74); p=.002). The standard DA group was more likely to know their exact risk percentage result compared to control (IRR=3.25 (95%CI: 1.31 to 8.07); p=.011); see Table 5. There were significant differences between decision aid groups by health literacy levels for self-reported calls to the Heart Foundation helpline (p<0.001) and verbatim knowledge of CVD percentage risk at follow up (p<0.001). No one with low health literacy reported calling the helpline or remembered their exact CVD risk in the control group. The standard decision aid increased both outcomes in all health literacy groups, and the literacy-sensitive decision aid increased both outcomes in low and high health literacy groups but not medium (Table 6).
Post-intervention differences between heart age groups
Immediately post-intervention, there were no differences between the two heart age groups for the primary outcome of lifestyle intentions, or secondary outcomes of risk perception or decisional conflict. For Hypothesis 3, the heart age group was less likely to have a positive emotional response (mean difference = -0.56 (95%CI: -0.88, -0.24); p=.001), less likely to perceive the message as credible (−0.20 (−0.35, -0.05); p=.010), and more likely to know whether their risk was low, medium or high (2.03 (1.33, 3.08); p=.001), compared to the percentage risk only group (Table 7). When the heart age result was older, there were significant differences indicating less positive (−0.75 (−1.19, - 0.31); p=.001) and more negative (0.57 (0.12, 1.02); p=.014) emotional responses, lower credibility (−0.29 (−0.49, -0.09); p=.005) and higher perceived risk level (2.11 (1.31, 3.39); p=.002) when heart age was shown. No such differences were found for those who received the same age or younger results (Table 7).
4 week differences between heart age groups
At 4 week follow-up there were no significant differences between the heart age groups in terms of lifestyle behaviour change, seeing a doctor for a Heart Health Check or gist knowledge of risk level (Table 7). Unsurprisingly, being shown heart age led to greater gist knowledge of heart age (2.90 (2.10, 3.99); p<.001) and verbatim knowledge of heart age (18.13 (4.36, 75.48); p<.001) compared to the those who weren’t shown their heart age, but there was no difference between the heart age and percentage risk only groups for knowledge of percentage risk. Within the heart age group who saw both risk formats, participants were more likely to have verbatim knowledge of their heart age (11%) than their percentage risk (6%) (McNemar’s chi-squared test for paired proportions: χ^2 (1)=6.10, p=.014, difference in proportions: 5.4%, 95%CI: 0.8% to 10.0%). When the heart age result was older, there were significant differences indicating more vigorous exercise (0.58 (0.09, 1.07); p=.021), more vegetable serves (0.57 (0.05, 1.09); p=.032), higher chance of meeting guidelines for exercise (1.23 (1.05, 1.45); p=.010) and diet (1.48 (1.00, 2.18); p=.048), when heart age was shown. When the heart age result was the same or younger than current age, there were significant differences indicating fewer soft drink serves (−0.34 (−0.61, -0.07); p=.012), and higher chance of calling the Heart Foundation helpline (12.66 (1.76, 4.03); p<.001), when heart age was shown (Table 7).
Stage 3
As part of the follow up survey, participants were asked if they’d like to be interviewed about the risk calculator. Twenty-seven of those indicated that they would. From this pool, 20 were selected to represent a range of ages, genders, risk levels, and health literacy. The interviews were done in four stages so that any user feedback from the interviews could be discussed amongst the team (CB, CAB and JA) and then implemented into the calculator for the next interviews, in an iterative process. The issues addressed in each round of interviews are shown in Appendix 2.
DISCUSSION
We used both a mixed methods development and evaluation process to produce a CVD decision aid that is effective for improving verbatim and gist knowledge of CVD risk and fruit consumption after 4 weeks. The resulting intervention is a scalable ehealth tool suitable for people with varying health literacy. This consumer tool will supplement a GP version to use within consultations36,37, providing GPs with a clear action for their patients to follow up when lifestyle change is recommended.
The paper provides an example of how to apply literacy-sensitive design principles to evidence-based decision making and behaviour change tools. The results show literacy-sensitive decision aids can support people with lower health literacy to make informed decisions, while still being suitable for the general population. A recent review of decision aids for people with lower health literacy53,54 showed that decision aids that used health literacy design strategies led to improved knowledge, decisional conflict and decision making outcomes. Further, decision aids that used explicit strategies to reduce cognitive burden showed greater improvements knowledge for people with low health literacy and from disadvantaged backgrounds54. The review highlighted the need for more consideration of health literacy in decision aid development. This study addresses the findings in the context of CVD prevention for the first time.
We observed a number of interactions with health literacy, showing the importance of considering this as a covariate when investigating shared decision making and behaviour change outcomes. The literacy-sensitive version of the decision aid produced more negative emotional responses and greater intentions to speak to a doctor about medication options to reduce CVD risk, amongst those with lower health literacy. This may reflect risk and choice awareness in this group, if they had not previously considered themselves to have risk factors for heart disease that could be addressed with preventive medication. As this sample was predominantly low risk, we would not want a decision aid to lead to greater actual medication uptake in this group, but speaking with a doctor about risk and how to reduce it may be a positive outcome in line with guidelines to assess risk in this age group1. We replicated previous decision aid studies in finding increased knowledge of risk amongst the decision aid groups compared to control35. We also replicated our previous finding that a literacy-sensitive action plan can improve diet outcomes across different levels of health literacy, although this was more marked for people with low health literacy29,55.
This study also replicated a number of heart age effects found in reviews of previous research, in that it leads to a more negative emotional response, increased gist and verbatim knowledge of heart age but not percentage risk, and reduced credibility, but is neutral for lifestyle change overall56,57. Our subgroup analyses suggest that more nuanced study designs may be required to better understand the effects of heart age. Firstly, amongst those who were shown their heart age, gist knowledge of percentage risk was initially improved, but after 4 weeks gist and verbatim knowledge were higher for heart age than for percentage risk. Previous studies have shown that people receiving an older heart age may react defensively and focus on other information, such as a low short-term risk level, which in turn may reduce credibility of the risk result24,58. Analyses of people who received an older heart age result suggests it may be useful as a marketing tool to get attention and initiate behaviour change, but knowledge of heart age did not translate to knowledge of risk. For the intended purpose of a decision aid to be used in a clinical context, the focus needs to be on validated risk results to make informed decisions about medication. For this reason, we made the decision to use the non-heart age version of the literacy-sensitive decision aid for future research in general practice. However, online heart age tools could incorporate decision aid and action plan elements with no detrimental effects. Future trials need to be designed differently to isolate older heart age results and follow-up behaviour over time. In considering how to power such trials, researchers will need to consider how the specific heart age tool they are using is calibrated for the intended population (e.g. ∼50% older in our sample using NZ method versus ∼80% in Australian/UK HF tool23,24). The primary outcome also needs to carefully considered. Most heart age research has been done with a primary outcome of immediate lifestyle change intentions, where we found no differences. More research could be done to verify the self-reported behaviour change amongst people receiving older heart age results we observed after 4 weeks, using more objective measures such as pedometers.
The end user interviews were helpful for improving simple navigation and wording issues in the literacy-sensitive version of the decision aid, but there were some larger issues that cannot be resolved in an online tool. Most users did not know their blood pressure or cholesterol results, but even if they had been assessed recently, they had difficulty understanding where the different numbers should be entered. This was particularly difficult for cholesterol results in pathology test reports. We will therefore test the final revised tool in clinical practice to address the issue of unknown blood pressure and cholesterol which reduces the accuracy, and limit display of options in line with current medication guidelines.
Strengths and limitations
A major strength of this study is that we were able to recruit a large, diverse sample in terms of health literacy and risk results. We had sufficient follow-up to run the study per protocol despite COVID-19 disruptions, and observed no difference in dropouts for key variables. A limitation is that the online panel sample may not be representative of the general population, and may better reflect users of online heart age tools than patients presenting to primary care for CVD risk assessment. Different countries use also different CVD risk models/heart age algorithms, which may affect the results given the differences we observed in the older heart age sample. Finally, we used validated outcomes where possible, but behaviour change was self-reported. Future research on heart age could consider using objective measures over time.
Conclusion
This study shows the value of combining health literacy-sensitive design with best practice risk communication and behaviour change tools. Although aimed at addressing the needs of people with lower health literacy, this approach improved knowledge of CVD risk and heart age, and behaviour, in a sample with varying health literacy levels. The role of heart age remains somewhat unclear, with both advantages and disadvantages, but no clear evidence of an effect on lifestyle change intentions or behaviour overall. Further research should investigate implementation pathways for integrating such consumer tools with clinical practice, and distinguish between older and younger heart age results.
Acknowledgments
This study was funded by a Vanguard Grant from the National Heart Foundation of Australia (ID 102215)
Footnotes
Ethics approval: This study has ethics approval from the University of Sydney Human Research Ethics Committee (ID 2019/774).
Trial registration: The trial protocol was pre-registered at ANZCTR (Trial number ACTRN12620000806965).
REFERENCES




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos