
Abstract
It has been proven that inactivated COVID-19 vaccines are safe and effective in general population with intact immunity. However, their safety and immunogenicity have not been demonstrated in people living with HIV (PLWH). In this study, we compared the immunogenicity of an inactivated COVID-19 vaccine between healthy individuals (n=28) and HIV-1 infected participants stable on combined antiretroviral treatment (cART) (n=42). All the HIV-1 infected participants had a CD4+ T cell count of above 200 cells/μL both at baseline and 4 weeks after vaccination. Comparable RBD binding antibody and neutralizing antibody responses were elicited in PLWH and healthy individuals after two-dose vaccination. Further analyses showed that PLWH with low baseline CD4+/CD8+ T cell ratios (<0.6) responded poorly to the vaccination compared with PLWH with medium (0.6∼1.0) or high (≥1.0) baseline CD4+/CD8+ T cell ratios (P<0.01). No solicited adverse reaction was observed in both cohorts. The CD3+, CD4+ and CD8+ T cell counts of PLWH decreased significantly after vaccination, but it did not lead to any adverse clinical manifestation. On the contrary, we found that the general burden of HIV-1 among PLWH decreased significantly (P=0.0059) after two doses of vaccination. Collectively, our data demonstrate that the inactivated COVID-19 vaccine is safe and immunogenic in PLWH who are stable on cART with unsuppressed CD4 counts.
Introduction
Even though the well-controlled HIV infection per se is not found as a risk factor of increased SARS-CoV-2 prevalence [1, 2], it is alerted that the compromised immunities and the high frequencies of comorbidities may render excessive challenges to this population [3, 4]. A more recently released WHO report (WHO reference number: WHO/2019-nCoV/Clinical/HIV/2021.1) suggests that HIV infection appears to be a significant independent risk factor for both severe/critical COVID-19 presentation at hospital admission and in-hospital mortality. Vaccination against SARS-CoV-2 for PLWH has also been recommended by WHO and health authorities of many countries. However, as a clinical observation showed that SARS-CoV-2 natural infection induced lower protective antibody responses in people with HIV [5], it is concerned that the immunogenicity of COVID-19 in PLWH might be weak. The anxiety escalated when the news released from the Novavax COVID-19 vaccine study suggested that HIV infection might dampen the vaccine effectiveness [6].
Reassuringly, more recently published data showed that both the messenger RNA vaccine [7, 8] and the ChAdOx1 nCoV-19 vaccine [9, 10] could elicit protective antibody responses in PLWH comparable with those in healthy individuals. In this study, we compared the antibody responses to two-dose inactivated SARS-CoV-2 vaccination between healthy vaccinees and HIV-1 infected individuals stable on cART. We demonstrated that the inactivated COVID-19 vaccine was immunogenic and safe in PLWH. Baseline CD4+/CD8+ T cell ratios were found to be associated with both the RBD binding antibody and the neutralizing antibody responses.
Materials and methods
Study design and participants
In this open-label two-arm non-randomized study, we enrolled a cohort of HIV-1 infected individuals (n=42) who were stable on cART and under routine follow-up at Hubei Provincial Center for Disease Control and Prevention, China and a cohort of healthy individuals (n=28). Written informed consent was obtained from all participants, and the study was approved by the Research Ethics Committee of Hubei CDC (approval reference number: HBCDC-AF/SC-08/02.0). The demographical characteristics of the enrolled vaccinees were depicted in Table 1.
Demographical characteristics of enrolled vaccinees
Peripheral lymphocyte count and plasma HIV-1 viral RNA detection
The peripheral lymphocyte counts and plasma HIV-1 viral RNA detections for HIV-1 infected individuals were performed using the BD Multitest™ CD3 FITC / CD8 PE / CD45 PerCP / CD4 APC reagent and the COBAS® AmpliPrep / COBAS® TaqMan® HIV-1 Test (v2.0) kit, respectively. All the detections were conducted following the manufacturers’ instructions in the clinical laboratory of Shanghai Public Health Clinical Center.
Titration of SARS-CoV-2 RBD binding antibody
In-house enzyme-linked immunosorbent assays (ELISA) were developed to measure SARS-CoV-2 RBD specific binding antibodies. High-binding 96-well EIA plates (Cat# 9018, Corning, USA) were coated with purified SARS-CoV-2 RBD protein (Cat# 40591-V08H, Sino Biological, China) at a final concentration of 1µg/ml in carbonate/bi-carbonate coating buffer (30mM NaHCO3,10mM Na2CO3, pH 9.6). Subsequently, the plates were blocked with 1×PBS containing 5% skimmed milk for 1 hour at 37°C. Next, 50μl of diluted human plasma was added to each well. After 1-hour incubation at 37°C, the plates were washed with 1×PBS containing 0.05% Tween20 for 5 times. Then, 50μl of an HRP labeled goat anti-human IgG antibody (Cat# ab6759, Abcam, UK) diluted in 1×PBS containing 5% skimmed milk were added to each well and incubated for 1 hour at 37°C. After a second round of wash, 50μl of TMB substrate reagent (Cat# MG882, MESGEN, China) was added to each well. 15 minutes later, the color development was stopped by adding 50μl of 1M H2SO4 to each well and the values of optical density at OD450nm and OD630nm were measured using 800 TS microplate reader (Cat# 800TS, Biotek, USA).
Quantification of SARS-CoV-2 neutralizing antibodies
The neutralizing antibodies against SARS-CoV-2 were detected using a commercialized surrogate neutralization test developed by Suzhou Xinbo Biotechnology Ltd. Company (PerkinElmer, China). The rationale and method of this assay have been elaborated in previous studies [11, 12]. Briefly, plasma samples were firstly incubated with acridinium ester labeled SARS-CoV-2 RBD for 15 min at room temperature. Then, magnetic beads coated with purified human ACE2 protein were added into the mixture and incubated for 15 min. After washing, the acridinium ester labeled RBD bound with the magnetic beads were measured by a chemiluminescent reaction. The concentrations of SARS-CoV-2 neutralizing antibody correlate negatively with the luminescence intensities, which can be quantified by establishing a standard curve.
Statistical analysis
All the statistical analyses were conducted using Graphpad Prism 9 (GraphPad Software, USA). Normality tests were performed before all downstream statistical analyses except the Chi square test. Comparisons between two groups were performed by the method of t-test. Differences among multiple groups were compared by the method of one-way ANOVA. The contingency analysis was done using the method of Chi-square test.
Results
Baseline characteristics of PLWH and HIV related events after vaccination
In this study, 28 healthy individuals and 42 PLWH were inoculated with two doses of the inactivated vaccine (BIBP-CorV) produced by Beijing Institute of Biological Products on 22 April 2021 and 25 May 2021, respectively. PLWH were slightly older than the control (42.74 ± 10.17 versus 37.79 ± 8.804 years, p=0.0392). The gender composition and the mean BMI were similar between PLWH and healthy individuals (Table 1). All the HIV-1 infected individuals have been on cART since being diagnosed with HIV-1 and have a peripheral CD4+ T cell count of >200 cells/μL. No solicited clinical adverse reaction was observed among all participants. None of PLWH developed HIV-related clinical events during the study period from 22 April 2021 to 25 June 2021.
At the beginning of vaccination, 21 patients had an undetectable plasma viral load, 9 patients had detectable viral loads below 20 copies/ml and 12 patients had detectable viral loads beyond 20 copies/ml (Table 2). Unexpectedly, we found that the general viral burden among PLWH decreased after vaccination: 35 patients had an undetectable plasma viral load, 3 patients had detectable viral loads below 20 copies/ml and 4 patients had detectable viral loads beyond 20 copies/ml (P=0.0052) (Table 2). Meanwhile, our data also showed that the peripheral T cell counts decreased significantly after vaccination, but the CD4+/CD8+ T cell ratios remained stable (Table 2).
Peripheral T cell counts and plasma viral loads of PLWH
The inactivated SARS-CoV-2 vaccine elicited comparable antibody responses in PLWH with those in healthy individuals
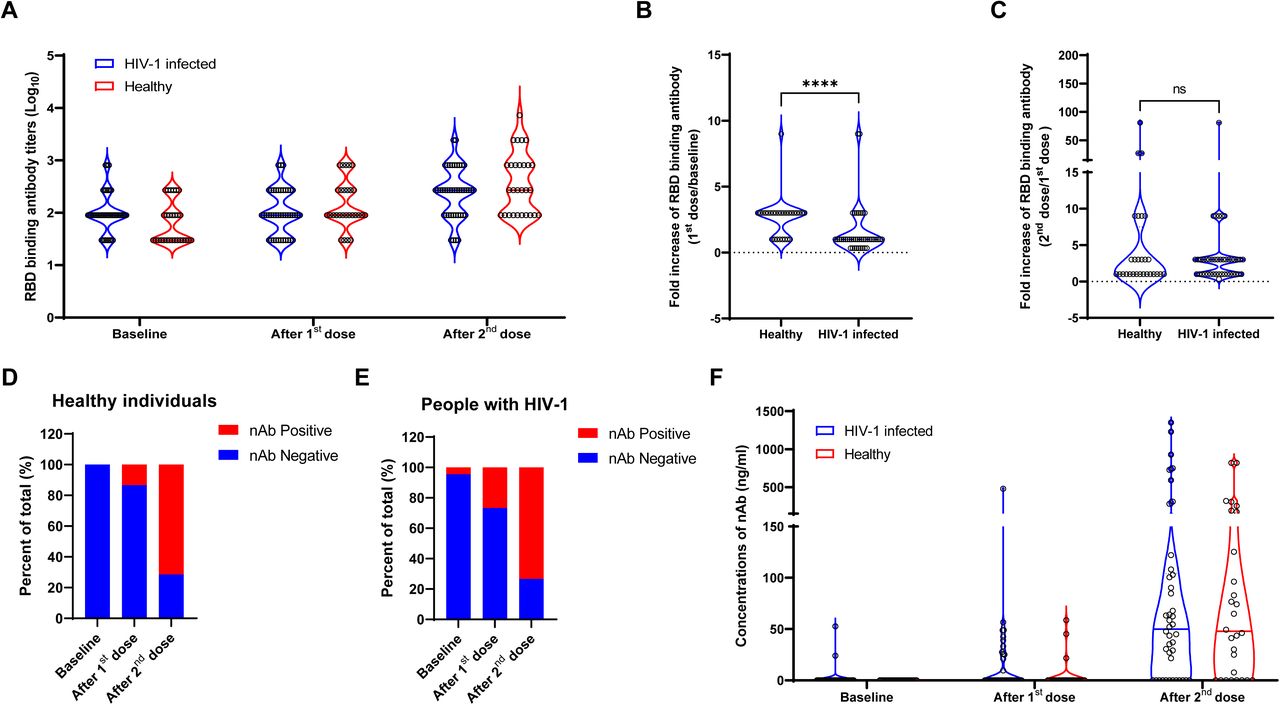
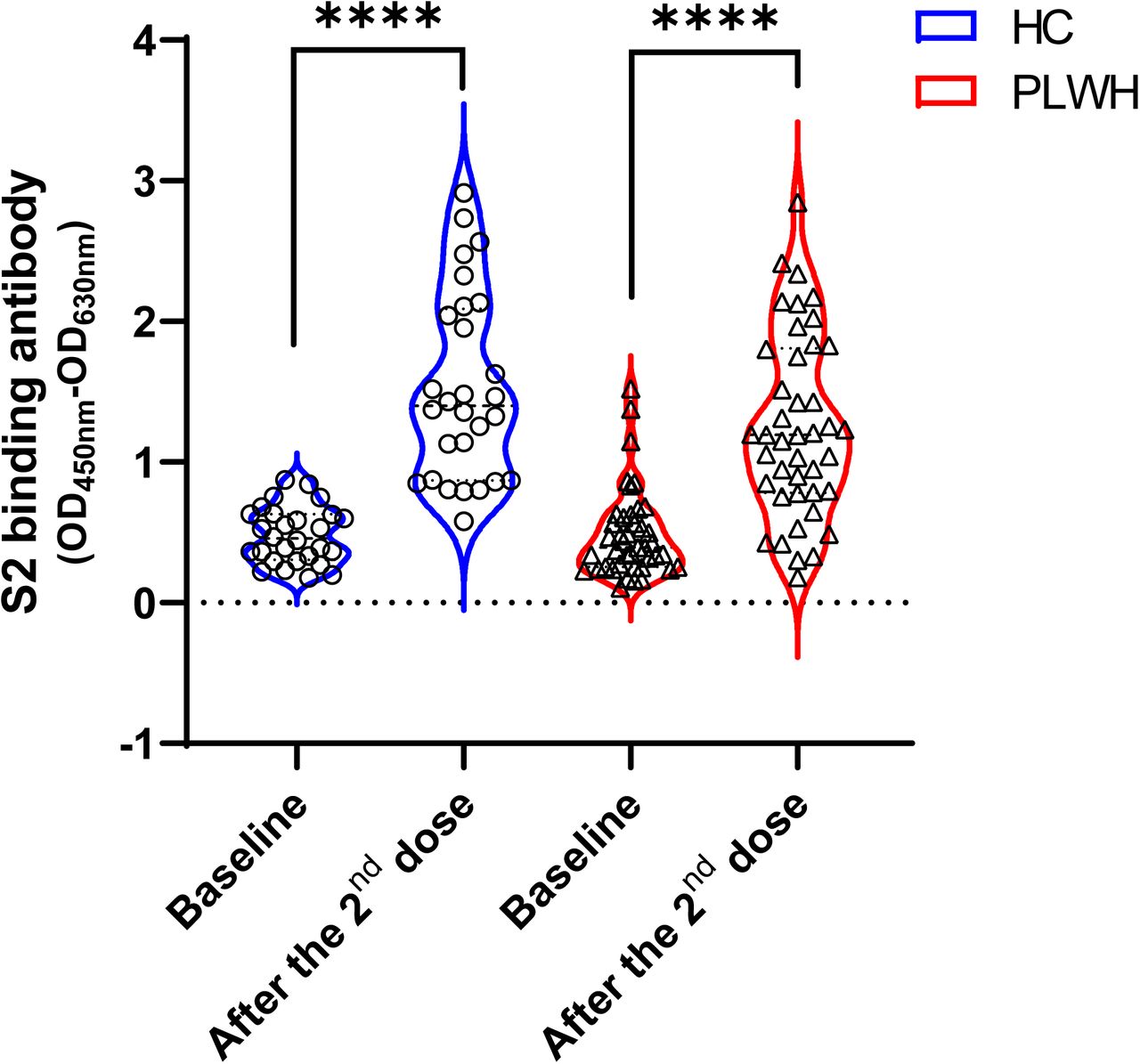
To evaluate the immunogenicity of the inactivated SARS-CoV-2 vaccine in our cohorts, peripheral blood samples were collected at baseline, 4 weeks after the first dose and 4 weeks after the second dose, respectively. The results of RBD binding antibody assays showed that the inactivated vaccine induced comparable levels of RBD binding antibodies in the two cohorts after both the first and the second dose (Fig. 1A). We found that the average fold increase of RBD binding antibody was significantly lower in PLWH (Fig. 1B), which was presumably due to the relatively high background antibody levels in this cohort (Fig. 1A). Neutralizing antibody responses were elicited in most participants after two doses of vaccination (Fig. 1D and 1E) and the magnitudes were similar between PLWH and the healthy control (Fig. 1F). In addition, we also found that the mean levels of S2 binding antibodies were similar between PLWH and healthy individuals both at baseline and 4 weeks post second vaccination (Supplementary Figure 1).

All participants in our study received two doses of the inactivated SARS-CoV-2 vaccine (BIBP-CorV) produced by Beijing Institute of Biological Products at an interval of 4 weeks. Peripheral blood samples were collected at baseline, 4 weeks post the 1st dose and 4 weeks post the 2nd dose. RBD binding antibody (A, B, C) and neutralizing antibody (D, E, F) responses were measured and compared between PLWH (n=28) and healthy individuals (n=42).
Baseline CD4/CD8 ratios were associated with antibody responses after the vaccination in the cohort of PLWH
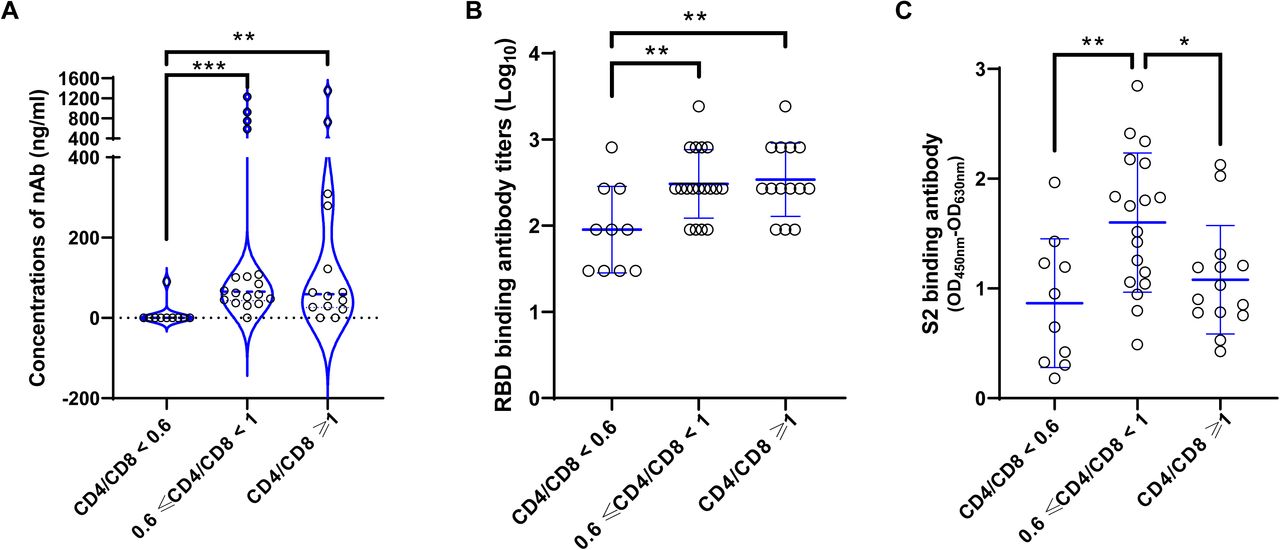
To understand whether the baseline immune status can influence the vaccine induced antibody responses in PLWH, we further analyzed the relationships between baseline T cell counts and post vaccination antibody responses. Our data showed that neither the CD4+ T cell counts nor the CD8+ T cell counts at baseline correlated with the vaccine induced antibody responses (Data not shown). While, the CD4+/CD8+ T cell ratios at baseline were found to be associated with antibody responses after the second dose of vaccination (Fig. 2). More specifically, the average RBD binding and neutralizing antibody responses of HIV-1 positive vaccinees with low baseline CD4+/CD8+ T cell ratios (<0.6) were significantly lower than those with medium (0.6-1.0) or high (≥1.0) baseline CD4+/CD8+ T cell ratios (Fig. 2A and 2B). Slightly different from the RBD binding antibody and the nAb responses, we observed that S2 binding antibody responses in HIV-1 positive vaccinees with medium baseline CD4+/CD8+ T cell ratios were significantly higher than those with both low and high baseline CD4+/CD8+ T cell ratios (Fig. 2C).

HIV-1 infected participants were stratified into 3 subgroups according to their baseline CD4+/CD8+ T cell ratios (<0.6, 0.6∼1.0 and ≥1.0). RBD binding antibody (A), neutralizing antibody (B) and S2 binding antibody (C) responses were compared among the three subgroups.
Discussion
Even if the replication of virus is controlled by cART, it can still be harder for HIV-1 infected individuals to defend against infectious diseases [13]. Therefore, vaccination is recommended for PLWH whose peripheral CD4+ T cell counts are more than 200 cells/μL [14]. However, due to the compromised immune status, the vaccine elicited immune responses might be impaired in PLWH [15-18]. As it has been suggested that HIV-1 infection could also alter the host immune responses against SARS-CoV-2 [19], the efficacies of COVID-19 vaccines in PLWH were seriously concerned. Here, we provided evidence showing that an inactivated SARS-CoV-2 vaccine (BIBP-CorV) was immunogenic and safe in PLWH. Importantly, our data showed that both the vaccine induced binding and neutralizing antibody responses were similar to the control at 4 weeks after two-dose vaccination.
All the HIV-1 positive participants in our cohort had a CD4+ T cell count of >200 cells/μL both at baseline and 4 weeks post vaccination. We found a statistically significant decrease in CD4+ T cell count between the baseline levels and those measured following the second vaccination. The decrease of CD4+ T cell count after vaccination had also been observed in PLWH inoculated with the BNT162b2 mRNA vaccine [20] and several other vaccines usually recommended for PLWH [21]. Increases in activated T cells were found to be associated with decreases in CD4+ T cell count [21], however the mechanism underlying this phenomenon is still not clear. Of note, both our and other studies [20, 21] did not identified any adverse clinical manifestation that was associated with the drop of CD4+ T cell count. Stable cART might be crucial to counteract the potential vaccine related deleterious effect in PLWH according to a recently published case report, which observed viral activation and CD4+ T cell loss in a treatment-naïve HIV-positive patient after receiving two doses of inactivated COVID-19 vaccines [22].
Quite surprisingly, we observed a significant drop of general viral burden in the PLWH cohort after vaccination. We speculate that the annihilation of vaccine activated HIV-1 infected CD4+ T cells might account for this phenomenon. However, the exact underlying mechanism need to be further investigated.
Despite the generally comparable antibody responses between PLWH and healthy individuals, we demonstrated that HIV-1 infected vaccinees with low baseline CD4+/CD8+ T cell ratio (<0.6) responded poorly after vaccination. TheCD4+/CD8+ T cell ratios were shown to be able to predict vaccine induced antibody responses in HIV-1 infected patients [23] and HIV negative elderly [24], but the underlying mechanism is still not clear. Considering that most vaccine induced antibody responses are CD4+ T cell dependent, we speculate that the low CD4+/CD8+ T cell ratio might reflect the relatively weak CD4+ T cell responses, which could not provide optimal help for antibody responses.
A major limitation of this study is the inadequate follow up, which do not allow us to compare the persistence of antibody responses between PLWH and the healthy control. Despite of this limitation, our study demonstrates that the inactivated COVID-19 vaccine was immunogenic and safe in PLWH stable on cART.
Data Availability
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflict of interest
The authors declare no conflict of interest.
Author contributions
YW and HT were involved in the study design and supervision; YMF, YFZ, ZYFH, XXT GW, DHC and LQJ were involved in data collection; YQR, WHW, JW, LYS, WHZ and YW performed the data analysis; YW, YMF and HT drafted the manuscript; WHZ, LYS, YW and HT revised the manuscript. HJH coordinated the enrollment of PLWH.
Supplementary figure legend

{kind=link}
{kind=link}
{kind=link}
The SARS-CoV-2 S2 specific binding antibodies were detected using an in-house ELISA method. The inactivated COVID-19 vaccine elicited significant S2 binding antibodies in both PLWH and heathy individuals and there was no statistically significant difference between the two cohorts.
Acknowledgments
We thank Dr. Lianguo Ruan from Wuhan Jinyintan Hospital for his help in PLWH cohort enrollment. We thank the volunteers who participated in this study. This work was funded by the National Natural Science Foundation of China (Grant No. 81971559, 82041010).
References



