
Abstract
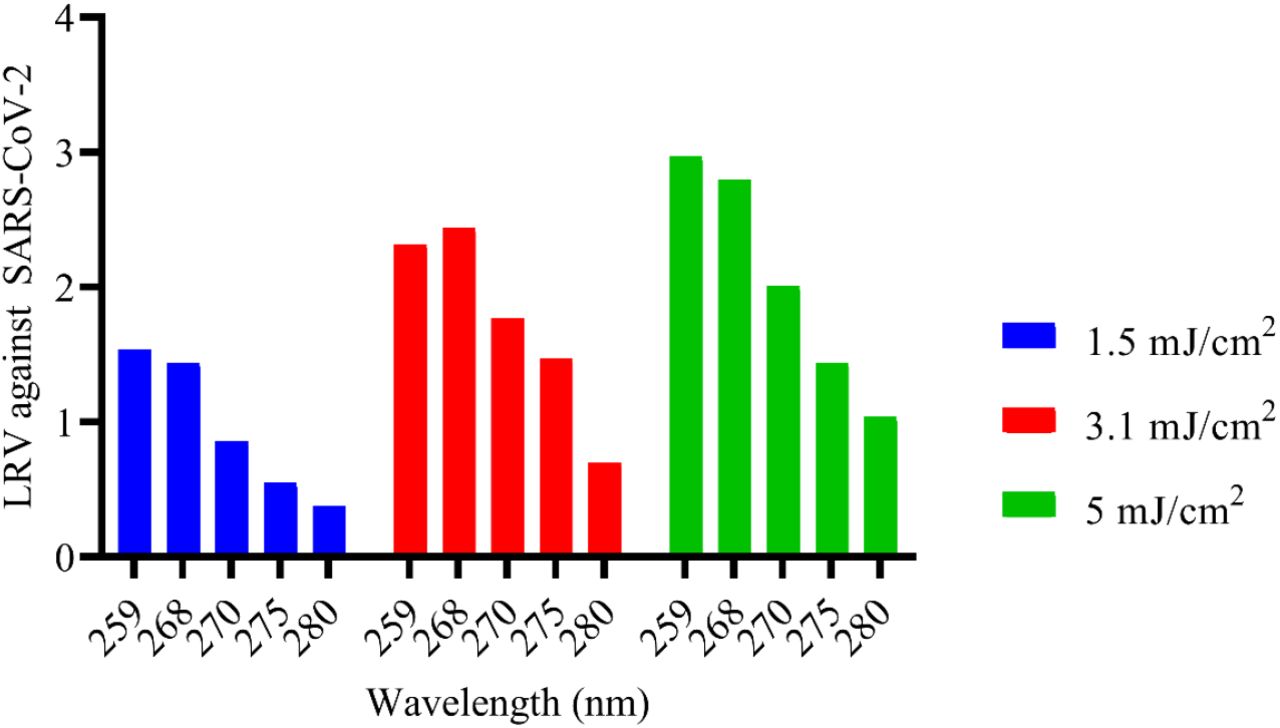
SARS-CoV-2 is a pathogen that can be disinfected using UVC. For effective inactivation strategies, design and implementation of UVC disinfection, knowledge of wavelength sensitivity, and disinfection rate of the relevant pathogen are required. This study aimed to determine the inactivation profile of SARS-CoV-2 using UVC irradiation with different wavelengths, in addition to validating surrogate models for SARS-CoV-2. Specifically, the study determined dosage, inactivation levels, and wavelength sensitivity of SARS-CoV-2. Assessment of SARS-CoV-2 (Strain USA/WA1-2020) inactivation at peak wavelength of 259, 268, 270, 275 and 280 nm was performed using plaque assay method. The UVC dose of 3.1 mJ/cm2 using 259 and 268 nm arrays yielded LRV2.32 and LRV2.44 respectively. With a dose of 5mJ/cm2, arrays of peak wavelengths at 259 and 268 nm obtained similar inactivation (LRV2.97 and LRV 2.80 respectively). The remaining arrays of longer wavelength, 270, 275 and 280 nm, demonstrated lower performances (LRV2.0 or less) with 5mJ/cm2. Additional study with the 268 nm array revealed that a dose of 6.25 mJ/cm2 (with 5 seconds or irradiation) is enough to obtain LRV3. These results determine that 259 and 268 nm are the most efficient wavelengths compared to longer UVC wavelengths, allowing the calculation of disinfection systems efficacy, and providing a benchmark for surrogates.
Background
Covid-19, a pandemic disease caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), has been determined to be highly susceptible to ultraviolet light [1]. At wavelengths between 100 and 280 nm (UVC range), viral inactivation is achieved by photochemical damage to nucleic acids, which results in reduced or inhibited viral replication [2]. Because UVC products are small and quiet, can disinfect surfaces as well as air, and are increasingly efficient, interest has increased dramatically [3]. Due to this increased interest in UVC products [4], evaluations to determine efficacy of room sanitization by UVC are being carried out [5] and the user feedback after in-use testing for prevention of hospital acquired infections is enthusiastic [6]. Recent findings have shown effective inactivation of SARS-CoV-2 by UVC irradiation at 254 nm using a commercial lamp [7]. One study, utilizing culture media, has demonstrated that shorter wavelengths are more effective than longer wavelengths (265nm>280nm>300nm) [8]. This has led to the general understanding that UVC irradiation, especially in the range between 200-290 nm, has great inactivation potential [9].
Unfortunately, the data available do not establish an inactivation profile of SARS-CoV2 or wavelength sensitivity. This means that system design and implementation requires guessing as to how much UVC light is needed. It also prevents the use of a surrogate to SARS-CoV2 in testing, thus requiring dangerous, expensive, and difficult tests for validation. In the present study, we describe experiments conducted to investigate wavelength sensitivity of SARS-CoV-2 on surface. The study investigated the inactivation rates of SARS-CoV-2 at a range of UVC wavelengths (259, 268, 270, 275 and 280 nm) with closely similar doses in a controlled and repeatable manner.
Material and methods
A USB4000 photospectrometer (Ocean Optics, https://www.oceaninsight.com/) and X1 handheld optometer (Gigahertz-Optik, https://www.gigahertz-optik.com/en-us/product/x1/) were used to confirm emitted radiation peak wavelength and UVC dose of the UVC arrays respectively. Experiments were carried out in a biosafety level 4 laboratory of the National Emerging Infectious Diseases Laboratories of Boston University (https://www.bu.edu/neidl/). Specifically, 100 μL SARS-CoV-2 (7.33 × 103 PFU/mL) (USA/WA1-2020) [10] was plated onto the surface of 60 mm plastic coupons (tissue culture dishes) in 5 μL aliquots. The virus was then dried in the biosafety cabinet in the dark before irradiating with UVC LED arrays.
A pair of tissue culture dishes (one to be irradiated and one control wrapped tightly in aluminum foil) were placed in the chamber of the device and UVC irradiated for a specified number of seconds, with each irradiation time tested in triplicate and averages used in statistical analyses. Following treatment, the virus was resuspended in 2 mL high glucose Dulbecco’s Modified Eagle Medium (DMEM) (Gibco) containing 0.04 mM phenol red, 1 × antibiotic-antimycotic (Gibco), 1 × non-essential amino acids (Gibco), 1 × GlutaMAX-I (Gibco), 1 mM sodium pyruvate (Gibco) and 2% fetal bovine serum (FBS)(Gibco). The resuspended virus was then serially diluted from 1 × 100 to 1 × 10−2.5 using half-logarithmic dilutions before performing a plaque assay after inactivation with UVC at a specific height, dose and time (Table 1). Semi-solid overlay plaque assay was carried out following Honko et al.,[11] protocol. Quantitation of plaques was carried out to determine viral titer, which was used to calculate log reduction value (LRV).
Timepoints, UVC doses obtained at a given distance, and irradiation at different LED wavelengths revealed lower inactivation of SARS-CoV-2 at >270 nm compared to 259 and 268 nm.
Results and discussion
The study developed an irradiation apparatus (Fig 1a) to quantitatively analyze inactivation of SARS-CoV-2 with different wavelengths. A USB4000 photospectrometer (Ocean Optics) was used to confirm the emitted radiation peak wavelengths of the UVC LED arrays at 259, 268, 270, 275 and 280 nm (Fig 1b). The UVC dose was confirmed using X1 handheld optometer (Gigahertz-Optik) (Table 1).

a). SARS-CoV-2 array set-up for disinfection study. A pair of dishes (one to be irradiated and one control wrapped tightly in aluminum foil) were placed in the chamber of the device and UVC-irradiated for a specified number of seconds, with each irradiation time tested in triplicate. Plaque assay technique was used to test the performance of the arrays. b). Confirmation of wavelength peak emissions for each array used in the study.
SARS-CoV-2 showed high susceptibility to UVC radiation, especially at peak emissions of 259 and 268 nm (Fig 2). There was strong association between wavelength and inactivation efficacy of the test arrays. Specifically, within UVC doses of 1.5mJ/cm2, 3.1 mJ/cm2 and 5mJ/cm2, there were significant differences in inactivation efficacy between arrays (p=0.0245, R2=0.8551, p=0.0497, R2=0.7723 and p=0.0186, R2=0. 8788 respectively). Inactivation performances increased with UVC exposure (dose) (Fig 3). Additionally, because the performance of 259 and 268 nm arrays was similar, the study went further and confirmed that with 6.25 mJ/cm2 in 5 seconds, LRV3 is obtained at 268 nm array. SARS-CoV-2 was reduced to below detectable levels within 7 seconds at a UVC wavelength of 268 nm.

Effects of UVC LEDs with different peak emissions on SARS-CoV-2 (Strain USA/WA1-2020) inactivation. Inactivation efficacy of wavelengths was carried out at similar UVC doses. Inactivation of SARS-CoV-2 revealed wavelength sensitivity, with the 268 nm array obtaining comparable performance with the 259 nm.

{kind=link}
{kind=link}
{kind=link}
Effects of low UVC doses on SARS-CoV-2. It was confirmed that an increased in UVC dose led to increased inactivation.
Findings from the current study are consistent with previous findings that UVC is very effective at inactivating SARS-CoV-2, that shorter wavelengths are more effective, and reveal the approximate required dosing [1], [7]. These results are somewhat consistent with a study of 280 nm, in which it took 37.5mJ/cm2 to obtain LRV3 against SARS-CoV-2, in that longer wavelengths were much less effective [12]. For emphasis, shorter wavelengths easily achieve target inactivation with less dose [13]. These findings also support the use of HCoV-43 as a surrogate pathogen to SARS-CoV-2 as used by Gerchman et al., [14].
Furthermore, unlike previous studies, the current study employing SARS-CoV-2 and utilizing more wavelengths enabled a deeper assessment of their inactivation efficiency under similar conditions, leading to sensitivity determination. This confirms the cumulative benefit of UVC with time even at low UVC doses found by Pavia et al.,[15] which observed a potentially compounding benefit of UVC when used over time in long-term care facilities.
However, the exact calculation of air disinfection is still not possible because this study only examines SARS-CoV-2 on dried surfaces and does not explore it as either a particulate or aerosolized SARS-CoV-2. Furthermore, SARS-CoV-2 was considered and therefore these results may not be used as baseline for other viruses, especially non-enveloped viruses. These findings also do not account for varied humidity and temperature, nor other types of surfaces. Still, this study allows the design and implementation of many new UVC systems based on the inactivation profiles found for varying UVC radiation sources.
Conclusions
Our findings provide a basic knowledge that SARS-CoV-2 is more sensitive at shorter wavelengths (<268 nm, as opposed to >270 nm). UVC LEDs with the most effective peak emissions could serve as effective and rapid tools in the fight against SARS-CoV-2 and other pathogenic viruses. This is an important result for designing UVC-based solutions, as engineers need to consider the effectiveness of the wavelengths used and the tolerance around rated peak wavelength and supports the use of HCoV-43 as a surrogate.
Data Availability
Original SARS-CoV-2 disinfection data and laboratory report is available upon reasonable request. Spectral confirmation data is available via https://doi.org/10.6084/m9.figshare.14884743.v1
Data availability
Original SARS-CoV-2 disinfection data and laboratory report is available upon reasonable request. Spectral confirmation data is available via https://doi.org/10.6084/m9.figshare.14884743.v1
Competing interest
R.M. Mariita, A.C.W. Miller and R.V. Randive work for Crystal IS, an Asahi Kasei company that manufactures UVC LEDs.
Author Contributions
R.M. Mariita, A. C. W. Miller, R. V. Randive: study design; R.M. Mariita: literature search, data analysis and figure design; R.M. Mariita, A. C. W. Miller: Manuscript writing and data interpretation; R. V. Randive: supply of study materials. R.M. Mariita, A. C. W. Miller, R. V. Randive: read, revised and approved final manuscript.
Acknowledgements
Authors especially thank the Boston University’s National Emerging Infectious Diseases Laboratories (BSL-4 laboratory), especially Dr. Anthony Griffiths, Dr. Lindsay McKay and Dr. Nadia Storm for utilizing their virology capabilities in the SARS-CoV-2 experiments. Authors are also grateful to Dr. Kevin Kahn and James Davis for proofreading the manuscript.




