
Abstract
Background There is limited empiric evidence on the coverage of pneumococcal conjugate vaccines (PCV) required to generate substantial indirect protection. We investigate the association between population PCV coverage and indirect protection against invasive pneumococcal disease (IPD) and pneumonia hospitalisations among under-vaccinated Australian children.
Methods Birth and vaccination records, IPD notifications and hospitalisations were individually linked for children aged < five years, born between 2001 and 2012 in two Australian states (New South Wales and Western Australia; 1.37 million children). Using Poisson regression models, we examined the association between PCV coverage, in small geographical units, and the incidence of (1) 7-valent PCV (PCV7)-type IPD, (2) all-cause pneumonia and (3) pneumococcal and lobar pneumonia hospitalisation in under-vaccinated children. Under-vaccinated children received < two doses of PCV at < 12 months of age and no doses at ≥ 12 months of age. Potential confounding variables were selected for adjustment a priori with the assistance of a directed acyclic graph. The main limitations of this study include the potential for differential loss to follow-up, geographical misclassification of children (based on addressed at birth only) and unmeasured confounders.
Findings There were strong inverse associations between PCV coverage and the incidence of PCV7-type IPD (adjusted incidence rate ratio [aIRR] 0.967, 95% CI 0.958-0.975, p-value <0.001), and pneumonia hospitalisations (all-cause pneumonia: aIRR 0.991 95% CI 0.990-0.994, p-value<0.001) among under-vaccinated children. Subgroup analyses for children < four months old, urban, rural and Indigenous populations showed similar trends, although effects were smaller for rural and Indigenous populations. Fifty-percent coverage of PCV7 among children < five years of age prevented up to 72.5% (95% CI 51.6-84.4) of PCV7-type IPD among under-vaccinated children, while 90% coverage prevented 95.2% (95% CI 89.4-97.8).
Conclusions In this study we observed substantial indirect protection at low PCV coverage, challenging assumptions high vaccine coverage is required.
Why was this study done?
Pneumococcal conjugate vaccines (PCVs) reduce the burden of pneumococcal disease in vaccinated and unvaccinated populations through both direct and indirect (herd) effects.
The indirect effects comprise a substantial component of overall vaccine impact, contributing to the cost-effectiveness of the vaccine but little is known about what factors contribute to herd protection, including vaccination coverage.
In this study, we examined association between PCV coverage and indirect effects within in diverse populations within Australia
What did the researchers do and find?
Using a large dataset of 1.3 million children from two states in Australia, we quantified the relationship between PCV coverage within small geographical units and indirect protection against pneumococcal disease. We also performed similar analyses for infants too young to be fully vaccinated, urban, rural and Indigenous populations.
There were strong inverse relationships between PCV coverage and the incidence of severe invasive disease due to vaccine types and pneumonia hospitalisations among under-vaccinated children i.e. higher coverage were associated with greater reductions in disease due to indirect effects. We also found substantial indirect effects at relatively low levels of PCV coverage. We estimated that 50% and 90% coverage of 7-valent PCV (PCV7) among children under five years of age prevented almost three-quarters (72.5%, 95% CI 51.6-84.4) and almost all (95.2%, 95% CI 89.4-97.8) of PCV7-type severe invasive disease, respectively. For pneumonia, we estimated that 50% and 90% coverage was sufficient to prevent one-third (33.3%, 95% CI 27.3-38.8) and about half (51.7%, 95% CI 43.7-58.6) of all-cause pneumonia hospitalisations among under-vaccinated children.
These trends were similar for children less than four months old, urban, rural and Indigenous populations, although these effects were smaller for rural and Indigenous populations. There was also a trend towards decreasing incidence of PCV13-type IPD among under-vaccinated children as PCV13 coverage increased.
What do these findings mean?
Our results challenge existing assumptions that high PCV coverage is required to achieve substantial indirect protection.
Understanding the determinants of indirect effects are particularly urgent as countries that have controlled vaccine-type pneumococcal disease consider using reducing the number of PCV doses (from three to two). Reduced dose schedules have the potential to significantly lower program costs while maintaining vaccine impact, providing indirect protection is achieved and preserved.
Introduction
Infections due to Streptococcus pneumoniae, the pneumococcus, are a leading cause of morbidity and mortality among children globally [1]. Pneumococcal conjugate vaccines (PCVs) have been successful in reducing pneumococcal disease through the direct protection of vaccinated individuals and indirect protection of both vaccinated and unvaccinated individuals [2]. Following the introduction of PCV to childhood immunisation schedules, many high-income countries, including Australia, have observed the near elimination of vaccine-type (VT) invasive pneumococcal disease with impacts extending beyond targeted age groups due to reduced transmission of VT pneumococci [3–5].
The 13-valent PCV (Prevnar 13, Pfizer) and 10-valent PCV (Synflorix, GSK) are costly and infant immunisation schedules are becoming increasingly crowded due to multiple vaccines. Therefore a PCV schedule comprising only two doses as opposed to three or four doses, once vaccine-types have been controlled, is an attractive policy option [6]. In 2020, the UK became the first country to move to a two dose (1+1) schedule for 13-valent PCV (PCV13) in the childhood vaccination program [7]. However, evidence to support the use of 1+1 schedules in settings with low or heterogenous vaccine coverage is not available.
Conceptually, indirect effects are achieved through sufficient vaccination coverage among age groups primarily responsible for transmission [8]. With sufficient indirect effects, near elimination of VT transmission and disease can be achieved. Near-elimination of VT disease has largely occurred in settings that have rapidly reached very high rates of coverage, hence it is often assumed that high PCV coverage is required to achieve elimination but there is limited evidence for this [9]. Settings with lower rates of coverage often lack the disease surveillance required to demonstrate indirect effects. It is therefore not clear whether VT elimination is possible for nearly half of the countries that have introduced PCV, which have less than 90% PCV coverage [10]. To date, most studies evaluating indirect effects from PCV have used aggregate data and ecological study designs, such as before-and-after or time-series analyses. Few have incorporated PCV coverage into their analyses.
Australia is a geographically diverse setting with a combination of dense urban populations and sparsely populated rural areas. Within Australia, Aboriginal and Torres Strait Islander children (henceforth referred to as Indigenous children), experience significantly higher rates of morbidity across a range of infectious diseases including pneumococcal disease, likely related to higher levels of social disadvantage [11,12]. Pre-PCV introduction, invasive pneumococcal disease rates in Indigenous children from Central Australia, were some of the highest in the world [13].
In June 2001, 7-valent PCV (PCV7) was introduced for high risk children, including Indigenous children and children with specified medical conditions, at ages two, four and six months. Children who were medically at risk received a fourth dose of PCV7 at 12 months and a dose of 23-valent pneumococcal polysaccharide vaccine (PPV23) at 5 years of age, while Indigenous children in high-incidence jurisdictions received PPV23 at 18-24 months of age. A three-dose PCV program (2, 4 and 6 months) became universal in January 2005, with catch-up doses for children aged less than two years of age. In July 2011, PCV13 replaced PCV7 with a catch-up program funding a supplemental dose of PCV13 for children 12-35 months of age [14]. For Indigenous children in high-incidence jurisdictions, a fourth dose of PCV13 replaced the PPV23 vaccine at 18-23 months.
Using the same large linked immunisation and hospitalisation dataset, indirect protection following PCV introduction previously in Australia has been reported previously at the State level for children less than two years of age, register with all-cause pneumonia declining among unvaccinated Indigenous (12% reduction; 95% CI 3-25) and non-Indigenous children (45% reduction; 95% CI 41-49) [15].
In this study, we extended this analysis by examining the association between PCV coverage in small geographic units within two states for both incidence of invasive pneumococcal disease (IPD) and hospitalised pneumonia among under-vaccinated children, in periods when coverage was changing rapidly. Our study provides a unique opportunity to evaluate indirect protection against pneumococcal disease in the absence of the widespread use of the booster dose making this analysis more applicable to many low-income countries where, at the time of the study, the 3+0 schedule is primarily used [16].
Methods
Study design
Our study design was a retrospective population-based cohort that used a subset of children under five years of age from a dataset of all children born in New South Wales (NSW) and Western Australia (WA) between 2001 and 2012, a combined birth cohort of approximately 1.37 million.[17]. Birth records were probabilistically linked (using name, date of birth, residential address and sex) to health data including vaccination register, IPD notification data and hospitalisation data [17].
Linked data sources
Vaccination status was obtained from the Australian Childhood Immunisation Register (ACIR), which includes all children enrolled in the publicly funded healthcare system and comprises ∼99% of children in Australia by age 12 months [18]. IPD cases, defined as isolation of S. pneumoniae by culture or detection of nucleic acid from a normally sterile, are notified as part of state-based passive surveillance systems [18]. Hospitalisation data covered all inpatient separations (discharges, transfers and deaths) and included primary diagnosis, and up to 50 (NSW) or 20 (WA) secondary diagnoses (coded using the Australian version of the International Classification of Diseases [ICD-AM] coding system). IPD data was available from January 2001 onwards, while hospitalisation data were available from July 2001 onwards. Demographic and health risk factor data were obtained from state perinatal data collection and birth registries (S1 File, Table 1) [18]. See S1 File (Fig 1) for a flow chart of the study cohort and data sources.

*Vaccinated defined as two or more PCV doses administered at < 12 months of age, or at least one PCV dose administered after the age of 12 months
Study definitions
PCV7-type IPD was defined as IPD due to serotypes in PCV7 i.e. serotypes 4, 6B, 9V, 14, 18C, 19F and 23F. PCV13, non-PCV7 type IPD, was defined as IPD due to the additional 6 serotypes in PCV13 i.e. serotypes 1, 3, 5, 6A, 7F and 19A. For all-cause pneumonia, we identified all hospitalisations with a pneumonia-related diagnostic code in the principal or additional diagnosis fields. Pneumococcal or lobar pneumonia hospitalisations were restricted to hospitalisations coded as either pneumococcal pneumonia (J13) or lobar pneumonia (J18.1) (S1 File, Table 2). Inter-hospital transfers and admissions within 14 days of a previous separation date were merged and classified as a single episode as per previous analyses [19]. All outcomes were evaluated for children under five years of age.
We defined a child as vaccinated with PCV if they received an adequate number of doses to develop a protective immune response against vaccine serotypes at least 14 days prior to onset of any study outcomes i.e. two or more PCV doses administered at less than 12 months of age, or at least one PCV dose administered after the age of 12 months [20]. Otherwise cases were classified as under-vaccinated. Given children who have received one dose of PCV at less than 12 months of age may have partial protection, we have also completed sensitivity analyses examining indirect effects among completely unvaccinated children (S1 File, Tables 14 and 15).
Statistical analyses
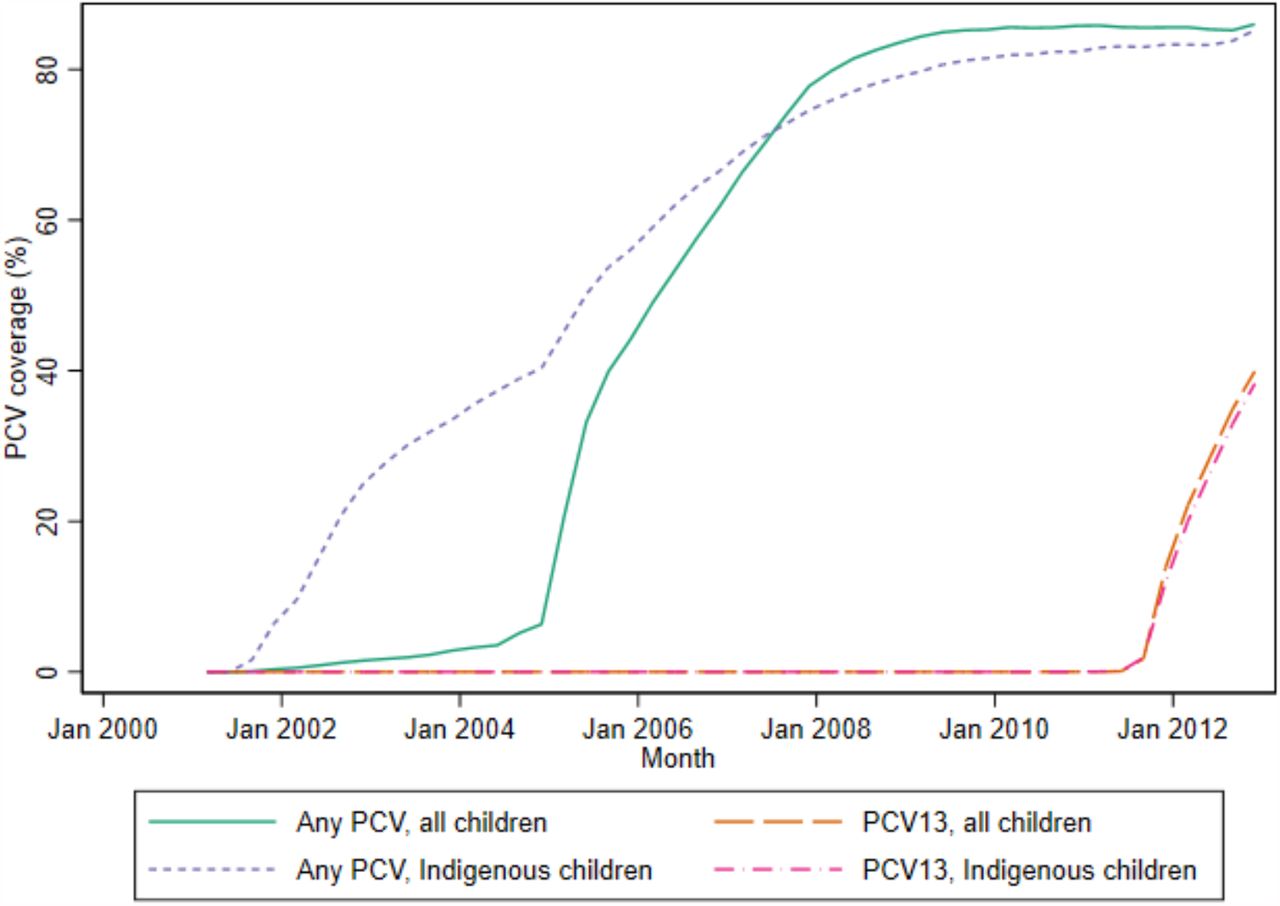
For descriptive analyses of PCV coverage over time, we calculated and graphed coverage among children less than five years of age at three-monthly intervals (31 March, 30 June, 30 September and 31 December) from 2001 to 2012. For example, PCV coverage among children less than five years of age at the final quarter of 2012 (assessed at 31 December), would be calculated for those born between 31 December 2007 and 30 December 2012. Coverage was calculated among children under five years of age to aid comparison with previous studies [21,22] and because previous research suggests that vaccination of children up to five years of age are key for the generation of indirect effects [21,23].
To visualise any geographic heterogeneity in PCV coverage, PCV coverage was mapped within Statistical Local Areas among children under five years of age at three time points – December 2005, December 2009 and December 2012. The three time points were chosen to represent the early post-PCV7 period, the late post-PCV7 period and the early PCV13 period. Statistical Local Areas (SLA) are the second smallest geographical spatial unit used by the Australian Bureau of Statistics [24]. In NSW and WA, there are 199 and 155 SLAs, respectively. SLAs vary in population size from less than 100 children in some rural areas to around 11 000 children under five years of age in urban areas. SLAs with fewer than 100 children under five years of age were excluded to enable meaningful estimates of PCV coverage for the different age groups.
Crude rates of IPD and pneumonia hospitalisation among all children and under-vaccinated children under five years of age over three time periods were calculated: targeted PCV program (2001-04), universal PCV7 program (2005-10) and universal PCV13 program (2011-12). Person-time for each child started at birth and was censored at the earliest of the following: death, when the child reached five years of age or at the end of the study period. For the under-vaccinated group, person-time was also censored when the child was considered vaccinated as previously defined.
To determine the association between PCV coverage and indirect effects against IPD and hospitalised pneumonia (primary analysis), we first calculated the incidence of each disease outcome during the person-time for which children were under-vaccinated up to five years of age. We divided each child’s under-vaccinated person-time into successive three-month intervals and linked the intervals to PCV coverage in their SLA of residence at that same time period. SLA of residence was based on mother’s residence at child’s birth. Using Poisson regression models, we examined the association between SLA-level PCV coverage and disease incidence in under-vaccinated children. We used robust variance estimates to account for clustering, accommodating multiple coverage estimates for each individual and checked linearity assumptions by plotting the log of the disease rates against PCV coverage.
Analyses relating to PCV7-type IPD used the full study period from January 2001 and December 2012, while analyses relating to PCV13, non-PCV7-type IPD were restricted to from January 2009 onwards –18 months prior to PCV13 introduction. Analyses relating to pneumonia hospitalisations used data from July 2001 onwards due to lack of availability of hospitalisation data in NSW prior to this date.
Potential confounding variables were selected a priori using a directed acyclic graph (DAG), informed by relevant literature and refined through expert consultation (S1 File, pp 6). These were age group, calendar year, Indigenous status, season, Index of Relative Socio-economic Advantage and Disadvantage (IRSAD) score, Accessibility or Remoteness Index of Australia (ARIA) category, birth weight, gestational age, maternal smoking during pregnancy, number of previous pregnancies, and previous hospitalisation with an ICD code corresponding to the presence of a medical condition increasing risk of IPD.
We graphed predicted incidence rates of each outcome among under-vaccinated children under five at each decile of PCV coverage, accounting for the balance of covariates across all the individuals [25]. We also calculated the estimated population preventable fraction of PCV7-type IPD and all-cause pneumonia hospitalisations for each decile of PCV coverage, defined as the proportion of disease among under-vaccinated children estimated to be preventable by increasing vaccine coverage among different age groups [26].
We conducted subgroup analyses, examining PCV7-type IPD and all-cause pneumonia hospitalisations among (1) children too young to be vaccinated (under four months of age); (2) under-vaccinated children in urban and rural Australia; and (3) under-vaccinated Indigenous children. We expected that associations for these subgroups may vary as the relationship between PCV coverage and pneumococcal disease is modulated by the dynamics of pneumococcal transmission, which in turn differs with population density, age group, risk factors and household structure [12,27].
Statistical analyses were performed according to a prospective data analysis plan (see S1 Text, Protocol).
Ethical approval was obtained from: The Aboriginal Health and Medical Research Council Ethics Committee (approval ID: 931/13), AIHW Ethics Committee (approval ID: EC 2012/4/62), Department of Health Human Research Ethics Committee (approval ID: 1/2013), Department of Health - WA Human Research Ethics Committee (approval ID: 2012/75), NSW Population and Health Service Research Ethics Commit-tee (approval ID: HREC/13/CIPHS/15), and Western Australian Aboriginal Health Ethics Committee (approval ID: 459).
Results
Study cohort and outcomes
The cohort comprised 1 365 893 singleton children born between January 2001 and December 2012, of which 1 223 803 lived in urban areas, 106 470 lived in rural areas, and 66 484 were Indigenous [15,28]. During 5 852 233 person-years of follow-up among children under five years of age, 1,427 cases of IPD were notified: 43.2% due to PCV7 serotypes, 28.4% due to PCV13-non-PCV7 serotypes, 17.7% due to non-PCV serotypes, and 10.7% lacked serotype data. Over the same period, 34 757 children experienced at least one episode of pneumonia hospitalisation, of which 799 (2.3%) were coded as pneumococcal or lobar pneumonia. Children were under-vaccinated against any PCV during 1 823 401 person-years of follow-up (31.2% of total person-years), with 83% of this time in children who had received no PCV doses.
Incidence of invasive pneumococcal disease (IPD) and pneumonia hospitalisations by period
Among under-vaccinated children, rates of all-cause IPD decreased from 73.3 in the targeted PCV7 period to 17.1 per 100 000 person-years in the universal PCV13 period (Table 1). Rates of PCV13, non-PCV7-type IPD increased in the universal PCV7 period, before decreasing in the universal PCV13 period (Table 1). In the universal PCV7 period, rates of PCV7-type IPD were higher in under-vaccinated children compared to all children. Comparable trends were observed among different age groups and among both Indigenous and non-Indigenous children (S1 File, Table 4). Annual rates of PCV7 and PCV13, non PCV7-type IPD are presented alongside annual PCV coverage estimates in S1 File, Tables 6 and 7.
Among under-vaccinated children, rates of all-cause pneumonia decreased from 90.7 to 50.3 per 10 000 person-years from targeted PCV7 to universal PCV13 periods (Table 2). Substantial reductions were observed for both all-cause pneumonia and pneumococcal or lobar pneumonia across different age groups by vaccination period (S1 File, Table 5).
PCV coverage
Among children under five years, coverage of any PCV increased steeply to 40% reflecting a catch-up program up to two years of age, then more gradually over the next four years as vaccinated children aged into older age groups, reaching 86% by December 2012.
Figs 2 and 3 depict the geographical heterogeneity in PCV coverage at the SLA level among children aged 12-23 months at the end of each of the following years: 2005, 2009 and 2012, with greatest heterogeneity in the year of universal PCV introduction (2005). The median and interquartile ranges of SLA-level PCV coverage in both age categories by year are presented in S1 File, Tables 6 and 7.
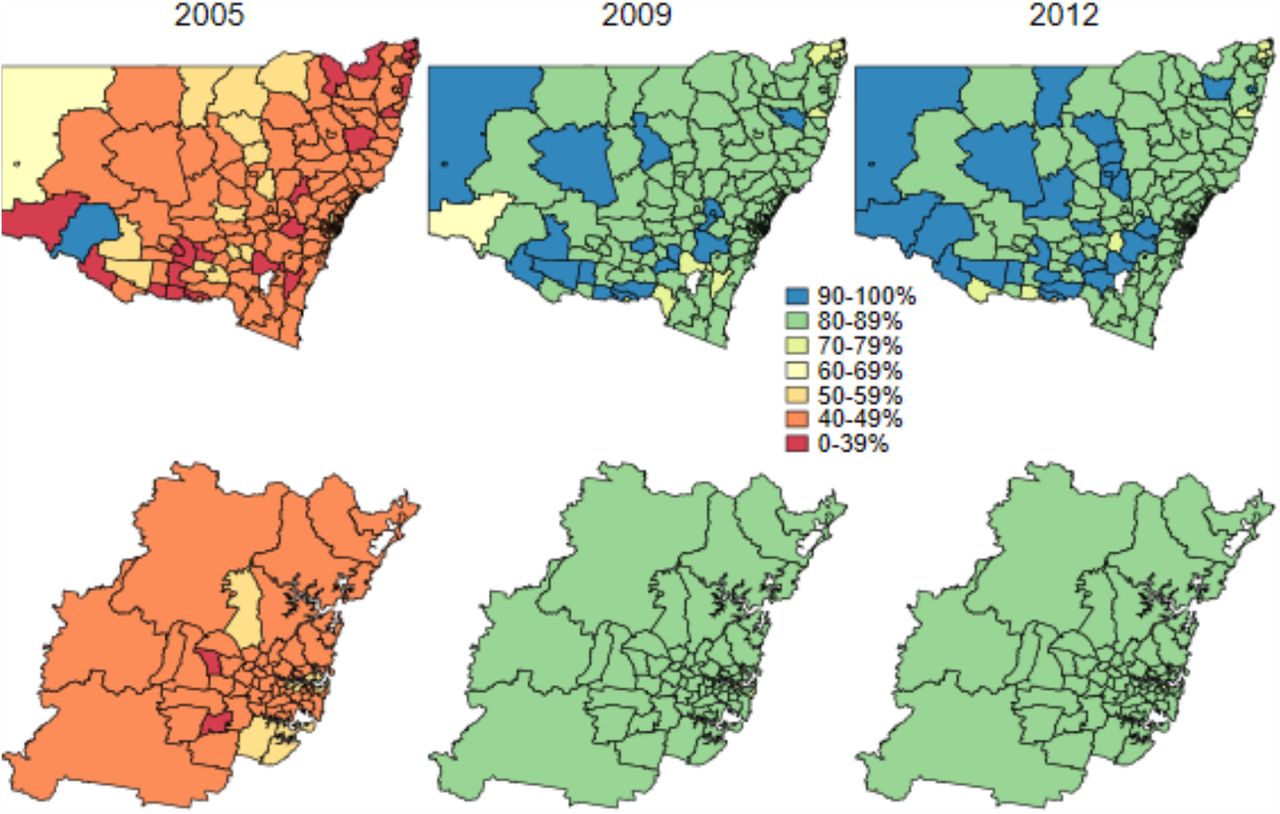
*Vaccinated defined as two or more PCV doses administered at < 12 months of age, or at least one PCV dose administered after the age of 12 months
Statistical Local Area Digital Boundaries (ASGC 2006) obtained from the Australian Bureau of Statistics (https://www.abs.gov.au/) CC BY 4.0
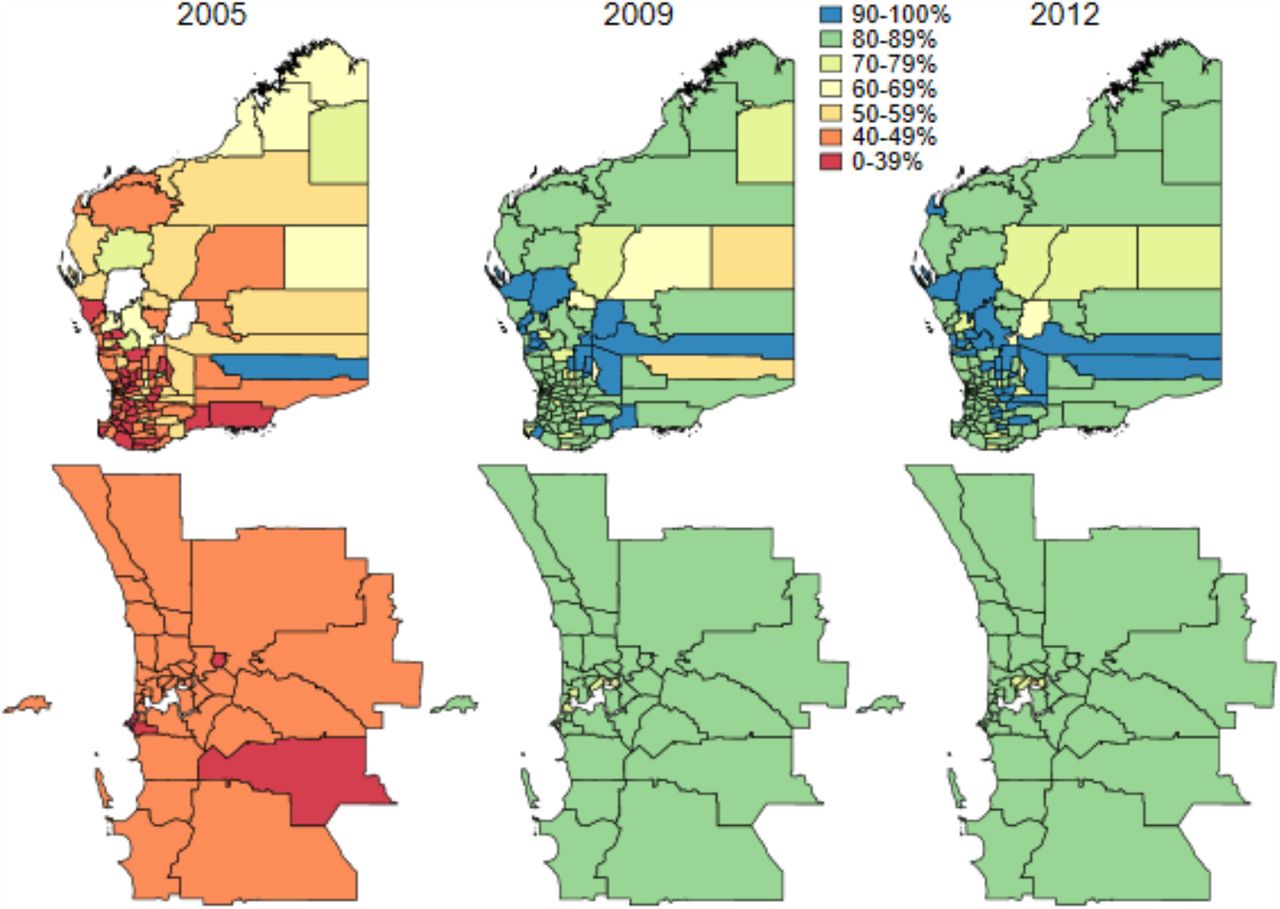
Coverage* of any pneumococcal conjugate vaccine among children 12-23 months of age by statistical local area and year, Western Australia, 2001-2012; top row: Western Australia (state), bottom row: Perth (capital city); SLAs coloured white have been excluded due to small numbers of children
*Vaccinated defined as two or more PCV doses administered at < 12 months of age, or at least one PCV dose administered after the age of 12 months
Statistical Local Area Digital Boundaries (ASGC 2006) obtained from the Australian Bureau of Statistics (https://www.abs.gov.au/) CC BY 4.0
PCV coverage and indirect protection against vaccine-type IPD
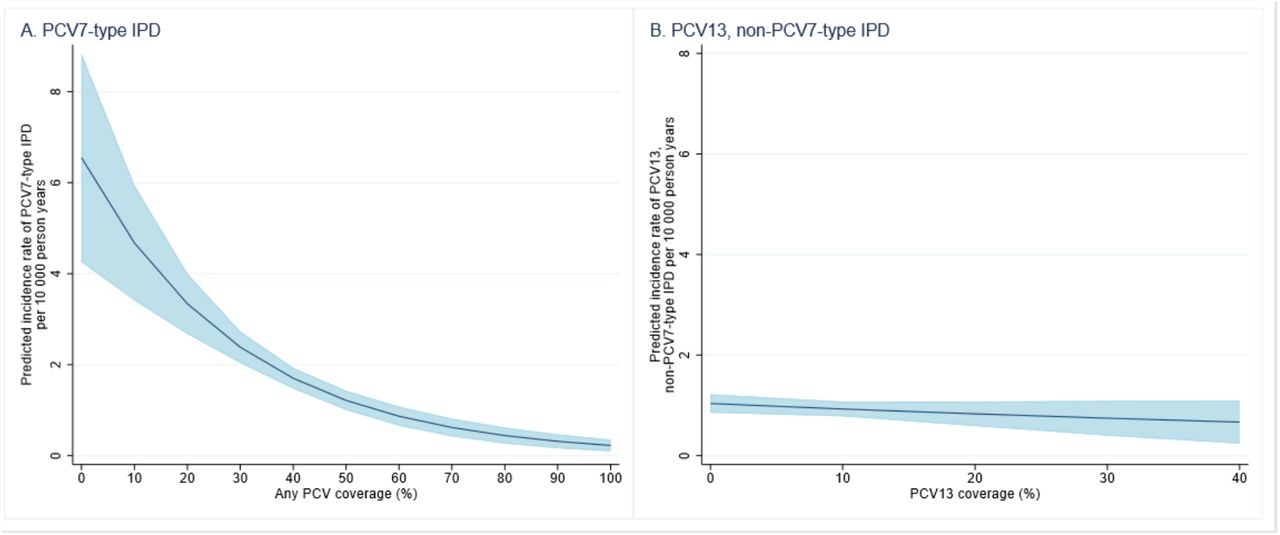
Fig 4 shows the association between PCV coverage and incidence of PCV7-type IPD for under-vaccinated children aged under five years. The number of IPD cases and the under-vaccinated person time available for analysis at different levels of PCV coverage are provided in S1 File, Table 8.

Estimated rate of vaccine-type invasive pneumococcal disease incidence* and 95% confidence intervals (blue shading) among under-vaccinated children under five years, at each decile of pneumococcal conjugate vaccine (PCV) coverage, New South Wales and Western Australia, 2001-12.
*PCV13, non-PCV7-type IPD incidence was only estimated up to 60% as there were few data points available
For each percentage point increase in PCV coverage among children 0-59 months of age, the adjusted incidence of PCV7-type IPD decreased by 3.3% (95% CI 2·5-4·2, <0.001) among under-vaccinated children under five years of age (S1 File, Table 10). The steepest declines in PCV7-type IPD occurred between 0% and 50% coverage among children 0-59 months of age (Fig 4).
Additionally, there was a trend towards decreasing incidence of PCV13-type IPD among under-vaccinated children as PCV13 coverage increased, however confidence intervals were wide (adjusted incidence rate ratio [aIRR] 0.989; 95% CI 0.971-1.007; p=0.241). (Fig 4 and S1 File, Table 10).
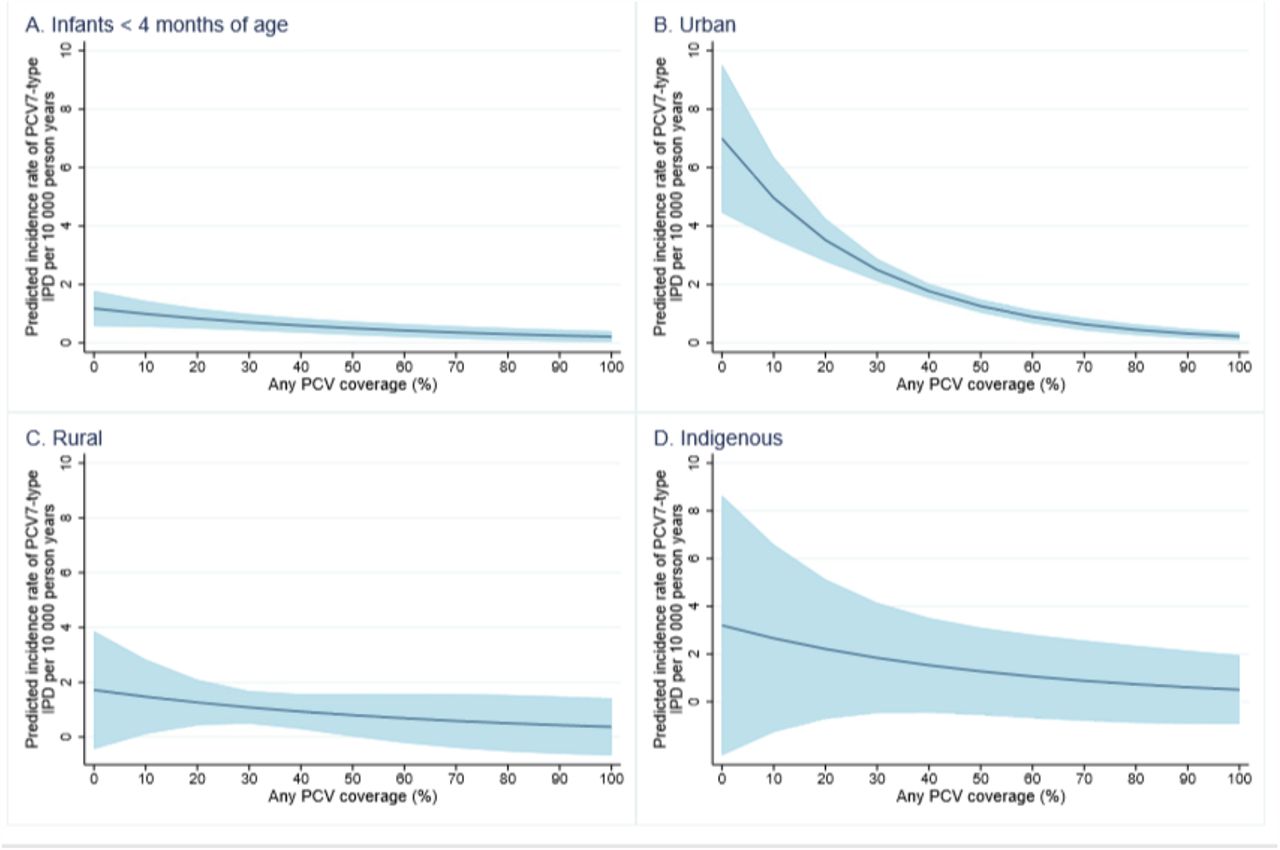
Subgroup analyses among children less than four months of age, children living in urban areas, children living in rural areas and Indigenous children showed similar trends, although confidence intervals for Indigenous and rural subgroup analyses were wide as sample sizes were small (see Fig 5 and S1 File, Table 12).
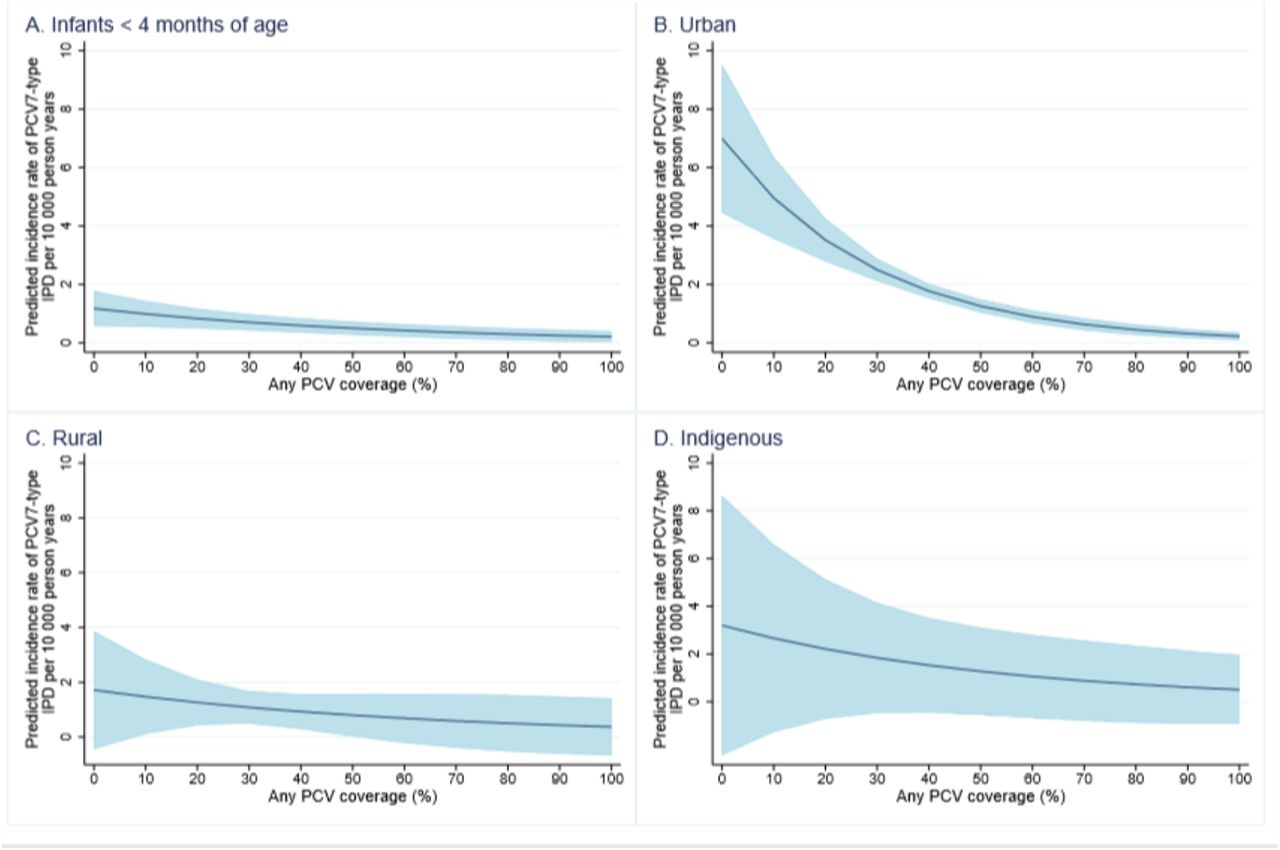
Estimated rate of vaccine-type invasive pneumococcal disease incidence* and 95% confidence intervals (blue shading) among three subgroups of under-vaccinated children under five years (urban, rural and Indigenous), at each decile of pneumococcal conjugate vaccine (PCV) coverage, New South Wales and Western Australia, 2001-12.
Table 3 shows the estimated preventable fraction of PCV7-type IPD in under-vaccinated children less than five years of age for each decile increase in PCV coverage. Vaccinating half of children less than five years of age is estimated to prevent 81.4% (95% CI 71.2-88.0) of PCV7-type IPD, while 90% coverage prevents 95.2% (95% CI 89.4-97.8).
PCV coverage and indirect protection against pneumonia hospitalisations
Similarly, there were inverse associations between PCV coverage and incidence of both all-cause pneumonia and pneumococcal or lobar pneumonia hospitalisations among under-vaccinated children (Fig 6 and S1 File, Table 11). The number of pneumonia hospitalisations and under-vaccinated person-time at the different levels of PCV coverage are provided in S1 File, Table 9. For each percentage point increase in PCV coverage among children less than five years of age, the adjusted incidence of pneumococcal or lobar pneumonia hospitalisations decreased by approximately 1.5% (95% CI 0.7-2.6; p=0.001) (S1 File, Table 11). For each percentage point increase in PCV coverage among children 0-59 months of age, the adjusted incidence of all-cause pneumonia hospitalisations decreased by approximately 0.9% (95% CI 0.6-1.0; p<0.001) (S1 File, Table 11).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Subgroup analyses for all-cause pneumonia hospitalisations among children living in urban areas, children living in rural areas and Indigenous children showed similar trends, although again confidence intervals for Indigenous and rural subgroup analyses were wide as there were fewer cases and individuals in these subgroups (S1 File, Table 13).
Table 4 shows the preventable fraction of all-cause pneumonia hospitalisations in under-vaccinated children less than five years of age by each decile increase in PCV coverage. We estimate that vaccinating 50% of children less than five years of age will prevent 33.3% (95% CI 27.3-38.8) of all-cause pneumonia hospitalisations in under-vaccinated children less than five years, while vaccinating 90% prevents 51.7% (95% CI 43.7-58.6).
Discussion
Our novel analyses highlight the relatively low levels of coverage required to generate indirect protection in children against IPD and pneumonia hospitalisations in Australia. These results challenge pre-existing ideas that high coverage is required for substantial indirect protection. Consistent with previous studies, we demonstrated an inverse relationship between PCV coverage and indirect effects on vaccine-type IPD [29]. A meta-analysis of PCV impact studies reported a 0.5% reduction in IPD (95% credible interval 0.2-1.1%) among children and adults for each percentage increase in vaccine coverage among children, accounting for country-level confounders [30]. However, in contrast to previous pneumococcal carriage studies, which reported statistically significant indirect effects at 58-75% coverage, we identified substantial indirect effects at lower rates of PCV coverage [21,22,31]. While not directly comparable, the indirect effect of PCV against disease can be expected to reflect indirect effects on carriage, since these effects are mediated by reductions in carriage.[23] The variation in results may be due to differences in analytic method. Compared to annual carriage surveys conducted by Hammitt et al. [31], we analysed at quarterly intervals allowing us to detect indirect effects at lower coverage rates. Grant et al. defined indirect effects as a statistically significant reduction in vaccine-type carriage prevalence, a measure which depends on both the effect size and sample size [22]. While Loughlin et al. chose to define indirect effects a priori as a 50% decline in vaccine-type carriage [21]. By modelling the association, we were able to quantify degree of indirect effects at varying coverage rates, facilitating future comparisons between studies with varying sample sizes and methods. Differences in the relationship between PCV coverage and indirect effects between studies may also be due to differences in the vaccine type studied (i.e. PCV7, PCV10 or PCV13) or context.
Importantly, we found similar trends among rural populations and Indigenous populations, although these effects were smaller and had large confidence intervals which likely reflects the smaller sample size available for analysis. These findings are important as they reflect indirect effects in different settings with different patterns of social mixing and therefore patterns of pneumococcal disease transmission. The modelled incidence of PCV7-type disease at zero coverage was lower than expected, given Indigenous children are known to be at high risk of pneumococcal disease. This is likely due to the earlier introduction of PCV for Indigenous children in 2001, which meant under-vaccinated Indigenous children were already benefiting from some degree of indirect effects at the start of our study’s observation period. Without sufficient baseline data prior to vaccine introduction, our analyses likely underestimate the full extent of indirect effects among Indigenous children. Given that Indigenous children make up 17.3% of our rural cohort, the earlier introduction of PCV among Indigenous children may also have impacted on our estimates of indirect effects in rural settings. However, the low baseline rates of disease may also be attributable to a more sparsely populated rural population with less social mixing compared to urban settings [32].Previous studies on the direct effect of PCV, found the vaccine to be equally effective among Indigenous children and children from rural areas, suggesting that our results are not due to reduced vaccine effectiveness in these groups.. Evidence of indirect effects among children under four months of age, albeit not statistically significant, is also important to note since these children are too young to be fully vaccinated across the time period while vaccine eligibility and coverage changes for other age groups.
Our analyses also demonstrated increasing indirect protection against pneumonia hospitalisations with rising PCV coverage. Pneumonia comprises a substantially larger disease burden than IPD and is a crucial determinant of vaccine cost-effectiveness of a PCV program. Our findings are consistent with previous analysis using the same dataset, which found 38% and 28% reductions in all-cause pneumonia hospitalisations among children <2 and 2-4 years of age, respectively, two years post-PCV7 introduction in Australia [33]. Similar relationships have been reported for PCV uptake and pneumonia hospitalisations in Brazil [29]. While our analyses, accounted for individual-level risk factors for pneumonia, it did not account for temporal trends, including changes admission practices or pneumonia epidemiology, which could account for an overall decline in pneumonia across this time period. This may explain the unexpectedly large estimate that over 50% of all-cause pneumonia among under-vaccinated children is preventable at 90% PCV coverage among children under five.
Our analyses did not identify a clear threshold at which PCV7-type IPD was eliminated – with 5% of PCV7-type remaining at 90% coverage. Similarly, a prior study of the long-term impacts of PCV against IPD in Australia reported reductions of 98% and 96% in vaccine-type IPD among children <2 and 2-4 years old eight years after vaccine introduction [3]. Our results may reflect the inherent limitations of the vaccine or schedule or insufficient period of monitoring post-PCV introduction to see full vaccine impacts; alternatively there may be a lag in observing the full effects of indirect protection after reaching a certain PCV coverage [8], which was not accounted for in this model.
While our analyses of PCV7-type IPD showed the steep declines in disease, especially up to 50% PCV coverage, we observed flatter associations between PCV coverage and both PCV13-type IPD and all-cause pneumonia hospitalisations. These results are consistent with previous studies indicating higher coverage rates (58-75) were required for substantial indirect effects using PCV10 and PCV13. This may be explained by previous research indicating lower vaccine effectiveness against the additional serotypes in PCV13[34,35].
However, there is a high degree of uncertainty around our PCV13 estimates since we have limited data post-PCV13 introduction (1.5 years) and a small number of PCV13, non-PCV7 type IPD cases. At the end of our study period, PCV13 coverage had only reached a median of 32.1% among children under five. Therefore our analyses are unable to capture the full indirect effects of PCV13, which are likely to increase as vaccine coverage rises over time. Smaller effect sizes for the indirect vaccine effects against all-cause pneumonia hospitalisations may be due to the non-specific nature of the outcome and/or differences in vaccine efficacy against the different spectrum of serotypes causing pneumonia, compared to IPD [36].
The availability of a large population-based linked dataset and analyses at fine spatial and temporal resolutions enabled precise evaluation of indirect effects in Australia, however there are some limitations. While our cohort is estimated to represent 97·5% of live births, it does not include children who have migrated into the two states or children who were never registered at birth. SLA of residence was based on the mother’s SLA of residence at the time of the child’s birth and we do not have updated data on SLA of residence if a family or child moved. We acknowledge that SLAs will not perfectly capture the boundaries of communities which interact socially, in which to measure indirect protection. As with all observational studies, causation cannot be assured. However, we observed a “dose effect” of PCV-for each decile increase in coverage there was a decline in pneumococcal disease and with the exception of parental smoking, the prevalence of measured confounders changed very little over time. Our definition of under-vaccinated included children who received one dose of vaccine under 12 months of age who may benefit from some direct protection, however majority of under-vaccinated person-time was in children who had no doses (83%) and sensitivity analyses among completely unvaccinated children yielded similar results [37,38]. We consider the risk of misclassification of vaccination status to be low, since vaccination status was determined using an immunisation registry, which has previously been demonstrated to underestimate coverage by less than 5% [39]. Lastly, an important limitation of this study is the potential for loss to follow-up in children who have moved interstate (missing outcome data) or overseas (missing vaccination and outcome data). From 2001 to 2012, the annual interstate out-migration of children less than five years of age ranged from 1.6-2.2% in New South Wales and 1.4-2.1% in Western Australia [40]. Data available from 2004-2012 indicates that overseas out-migration was less common, ranging from 0.9-1.2% [41]. Since our analyses are for children up to five years of age, we estimate that the cumulative unobserved loss to follow-up time to be less than 15% - in line with recommendations for cohort [42]. Furthermore, we do not expect differential loss to follow-up between vaccinated and under-vaccinated children or as vaccine coverage rises over time, since migration patterns have remained constant.
Our results support continuing efforts to increase vaccine coverage to maximise indirect protection from PCV in Australia. In our study, PCV7-type IPD continue to decline as coverage increases among children under five years, suggesting that catch-up vaccination up to five years of age may be important to maximise indirect effects – in line with previous research [43]. Indirect protection is important because it comprises a substantial component of overall impact, improves cost-effectiveness of the vaccine and protects infants too young to be vaccinated and adults. While our study does not include indirect effects on adult disease, prior research suggests that in low-transmission settings indirect effects in children are effectively translated to indirect effects in adults, since children are the primary drivers of pneumococcal transmission [44,45].
Understanding the coverage required to achieve indirect protection is of considerable global interest in the potential for reduced dose (1+1) schedules [6] as the success of this program relies on the continued generation of indirect protection for infants who have not received sufficient doses to mount individual level protection [6]. Our findings suggest that lower rates of vaccine coverage may still be confer considerable indirect effects and therefore a 1+1 schedule may be suitable despite low coverage PCV coverage. Additionally, we found evidence that these trends are similar across a range of subgroups. However, our findings cannot be directly extrapolated to other settings since degree of indirect protection is highly dependent on local factors influencing pneumococcal transmission [27]. Other studies have demonstrated lower than expected direct and indirect effects following PCV13 introduction in Australia, which used a 3+0 schedule, compared to countries using a booster dose, such as the UK (2+1 schedule) and US (3+1 schedule) [16,46]. As a result, Australia implemented a switch from the 3+0 to 2+1 schedule in 2018. Further research beyond the timeframes available in this analysis is needed to document the longer-term impacts of PCV13 introduction and the schedule change on indirect effects in Australia. Further research, using consistent and robust methodology, is also required to understand the relationship between PCV coverage and indirect protection in a range of settings, particularly in high-transmission settings. This will assist with understanding the role of PCV coverage as an alternative metric to determine if indirect effects are present in settings with insufficient disease surveillance.
Data Availability
The custodians of the data used for this analysis are the New South Wales Centre for Health Record Linkage (https://www.cherel.org.au/) and Western Australia - Data Linkage (https://www.datalinkage-wa.org.au/). Interested researchers may apply at these sites for data access.
Contributors
FMR and JC conceptualised and designed the study. JC performed the analysis and drafted the initial manuscript. CDN provided expert statistical advice. PF and HFG assembled the cohort used for the pneumococcal analyses. HFG, PBM, CB, PF, HM, KM, and RA provided expert clinical and epidemiological advice, and assisted with the interpretation and presentation of results. All authors reviewed and revised the manuscript and approved the submitted final manuscript.
Funding
This study was funded by the Population Health Research Network Proof of Concept Project, a capability of the Commonwealth Government Collaborative Research Infrastructure Strategy and Education Investment Fund Super Science Initiative, and the Australian National Health and Medical Research Council (project grant GNT1082342, chief investigator HFG). HFG, CCB, HCM and FMR are funded by Australian National Health and Medical Research Council (NHMRC) fellowships. Specifically, FMR is funded by an NHMRC Translating Research into Practice (TRIP) fellowship and Investigator grant. JC is funded by the Australian Research Training Program scholarship. HCM is further supported by a Telethon Kids Institute Emerging Research Leader Fellowship. The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Supporting information
S1 RECORD Checklist
S1 Text. Protocol
S1 File. Supplementary Methods and Additional Analyses
Acknowledgements
We thank the staff at the Population Health Research Network (PHRN), participating PHRN data linkage and infrastructure nodes (the Western Australian Data Linkage Branch, the New South Wales Centre for Health Record Linkage, and the Australian Institute for Health and Welfare), the Western Australia and Commonwealth Departments of Health and New South Wales Ministry of Health who provided advice and the data, and the Aboriginal and Torres Strait Islander community and members of the Aboriginal Immunisation Reference Group for their contribution to this research project.
References



