
Abstract
Background Reports on the occurrence and outcome of Visceral Leishmaniasis (VL) in pregnant women is rare in published literature. The occurrence of VL in pregnancy is not systematically captured and cases are rarely followed-up to detect consequences of infection and treatment on the mother and foetus.
Methods A review of all published literature was undertaken to identify cases of VL infections during pregnancy by searching the following database: Ovid MEDLINE®; Ovid Embase; Cochrane Database of Systematic Reviews; Cochrane Central Register of Controlled Trials; World Health Organization Global Index Medicus: LILACS (Americas); IMSEAR (South- East Asia); IMEMR (Eastern Mediterranean); WPRIM (Western Pacific); ClinicalTrials.gov; and the WHO International Clinical Trials Registry Platform. Selection criteria included any clinical reports describing the disease in pregnancy or vertical transmission of the disease in humans. Articles meeting pre-specified inclusion criteria and non-primary research articles such as textbook, chapters, letters, retrospective case description, or reports of accidental inclusion in trials were also considered.
Results We screened 272 publications and identified a total of 70 records (1926–2020) describing 447 VL cases in pregnant women. The disease was detected during pregnancy in 394 (88.1%), retrospectively confirmed after giving birth in 52 (11.6%), and the time of identification was not clear in 1 (0.2%). Of the 394 mothers whose infection was identified during pregnancy, 344 (89.1%) received a treatment, 3 (0.8%) were untreated, and the treatment status was not clear in the remaining 47 (12.2%). Of 344 mothers, Liposomal Amphotericin B (L-AmB) was administered in 202 (58.7%) and pentavalent antimony (PA) in 92 (26.7%). Outcomes were reported in 176 mothers treated L-AmB with 4 (2.3%) reports of maternal deaths, 5 (2.8%) miscarriages, and 2 (1.1%) foetal death/stillbirth. For PA, outcomes were reported in 87 mothers of whom 4 (4.6%) died, 24 (27.6%) had spontaneous abortion, 2 (2.3%) had miscarriages. A total of 26 cases of confirmed, probable or suspected cases of vertical transmission were identified and the median time to detection was 6 months (range: 0–18 months).
Conclusions Outcomes of VL treatment during pregnancy is rarely reported and under- researched. When it is reported, information is often incomplete and it is difficult to derive generalisable information on outcomes for mothers and babies, although reported data favours the usage of liposomal amphotericin B for the treatment of VL in pregnant women.
Author summary Visceral Leishmaniasis (VL) is a neglected tropical disease with an estimated incidence of 50,000 to 90,000 cases in 2019. Women who are susceptible to becoming pregnant or those who are pregnant and lactating are regularly excluded from clinical studies of VL. A specific concern of public health relevance is the little knowledge of the consequences of VL and its treatment on the mother and the foetus. We did a systematic review of all published literature with an overarching aim of identifying cases of VL in pregnancy and assess the risk-benefit balance of antileishmanial therapies to the mother and the child. We identified a total of 70 records (1926–2020) describing 447 VL cases in pregnant women. In 394 mothers, infection was identified during pregnancy of whom 202 received Liposomal Amphotericin B (L-AmB) and 92 received pentavalent antimony (PA). Reports of maternal deaths, abortion, and miscarriages were proportionally lower among those who received L- AmB compared to PA regimens. A total of 26 cases of confirmed, probable or suspected cases of vertical transmission were identified and the median time to detection was 6 months (range: 0–18 months). Our review brings together scattered observations of VL in pregnant women in the clinical literature and clearly highlights that the disease in pregnancy is under-reported and under-studied. Our findings indicate that L-AmB should be the preferred treatment for VL during pregnancy.
Introduction
Visceral Leishmaniasis (VL) is a neglected tropical disease caused by Leishmania sp. parasites transmitted by female sandflies. The disease is endemic in parts of South Asia, East Africa, South America and the Mediterranean region with an estimated 50,000 to 90,000 cases in 2019 [1]. A specific concern of public health relevance is the little knowledge of the clinical aspects of VL and treatment outcomes in pregnant and lactating women [2].
In pregnancy, VL diagnosis relies essentially on symptoms and serology as parasite detection by splenic aspiration is not recommended because of the risk for the foetus. More severe anaemia and increased requirements for blood transfusion have been reported for pregnant women infected with VL [2]. Case management must take into account the consequences of the disease and the therapeutic intervention on the mother-foetus pair [3]. Of note, except amphotericin B, all other available drugs are either contraindicated or subjected to restricted use in pregnant and lactating women and in women of child-bearing age (Table 1) [4–6]. Further complexities arise from potential vertical transmission of the disease either congenitally (maternal–foetal transmission in utero) or through transplacental infection as a result of blood exchange during labour. While vertical transmission of VL is well-studied and established in animal studies, reports in humans are sporadic with observations of clinical manifestation several months post-partum [7–10]. Such vertical transmission can induce in utero death or can be potentially deleterious to the foetus and infant [6,9,11].
Antileishmanial usage during pregnancy
The regulatory restrictions and limited evidence on safety of antileishmanial chemotherapeutics on the mother-foetus pair meant that historically clinicians had to rely on personal experience or limited published case-reports to make a decision. This led to some clinicians delaying the treatment of pregnant women until after delivery, especially when the case was detected closer to the due date [12, 13]. Others had treated them when the adjudicated risk of VL to the mother outweighed the risk posed by the drug to the mother-foetus pair [14]. Similar delays in treatment of pregnant mothers has also been reported in post kala-azar dermal leishmaniasis (PKDL) [15, 16]. Currently liposomal amphotericin B (L-AmB) remains the preferred regimen for the treatment in pregnancy (Table 1). However, pregnant and lactating women are regularly excluded from clinical studies [17] and are considered “therapeutic orphans” [18]. In studies that enrol females of childbearing age, counselling measures are usually set in place to inform the patients regarding the potential teratogenic harms of study drugs and either adoption of suitable contraception methods or observance of abstinence is mandatory (for example in miltefosine trials) [17]. In regular clinical practice and non-clinical trial settings, pregnancy tests and counselling however, might not be done routinely. A study conducted in South Asia found that only one in every six doctors ruled out pregnancy before prescribing miltefosine [19].
Finally, there is a lack of active pregnancy registries for most of the antileishmanial drugs expect for miltefosine. In the context of Impavo® (Profounda Inc.), the commercial name of miltefosine registered to the US medicines regulatory agency (US Food Drug Administration), a pregnancy registry was established to fulfil post marketing requirements [20, 21]. The recruitment of pregnant women as part of the observational study started in 2015 and the study is expected to be completed in 2026, and is estimated to recruit 0–1 patients per year over the 10 year study period, hence unlikely to generate a large volume of new safety data [20]. There are no other active pregnancy registries on exposures to VL treatments from which to derive information on consequences on gestation, mother, foetus, and the newborn. Therefore, to understand the risks and benefits of treatment to the mother and the child, one must turn to the published literature.
The most comprehensive reviews on VL in pregnant women were conducted in the mid 2000s [9, 22]. We therefore conducted a systematic review of all published literature with an overarching aim of identifying cases of VL in pregnancy. The specific objectives were to assess the risk-benefit balance of antileishmanial therapies to the mother and the child and to identify the cases of vertical transmission. The review was not limited by language or any interventions.
Material and Methods
Literature search
A review of all published literature was undertaken on 26th of March 2020 to identify records describing VL in pregnant women or any reports of vertical transmission of the disease in humans by searching the following clinical databases: Ovid MEDLINE®; Ovid Embase; Cochrane Database of Systematic Reviews; Cochrane Central Register of Controlled Trials; World Health Organization Global Index Medicus: LILACS (Americas); IMSEAR (South- East Asia); IMEMR (Eastern Mediterranean); WPRIM (Western Pacific); ClinicalTrials.gov; and the WHO International Clinical Trials Registry Platform (ICTRP). The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic-Reviews and Meta-Analyses (PRISMA) guidelines (S1 Text)[31]. In addition, full text screening of the publications indexed in the Infectious Diseases Data Observatory (IDDO) clinical trials library was carried out to identify any description of VL in pregnant women [32]. The references of all included publications were further checked to identify any relevant articles. This review is not registered and the protocol describing the search strategy including database search strings, search dates and eligibility criteria for screening is presented in supplemental file (S2 Text).
Study screening
Study screening was carried out in two stages to identify the studies fulfilling the inclusion and exclusion criteria (S2 Text): title and abstract screening (stage I) and then full-text screening (stage II). As reports on VL in pregnancy are sparse, articles meeting minimal inclusion criteria and non-primary research articles such as opinion pieces, clinical guidelines, textbooks, chapters, correspondences, reports of accidental inclusion in trials, or case reports of unplanned pregnancies during the study follow-up were also considered for comprehensiveness. No restrictions were applied regarding study design, follow-up duration, sample size, region, or the treatment regimen for eligibility of inclusion in this review. Title and abstracts were screened in the first stage, followed by screening the full- texts. Articles that were not in English language (Spanish, Portuguese, Korean, and German) were evaluated using google translation (https://translate.google.co.uk/).
The articles were screened against eligibility criteria by a single reviewer (PD). A second reviewer was consulted (SSP) when the first reviewer couldn’t reliably assess the eligibility. The first reviewer (PD) extracted data from all the eligible records and it was verified by the second reviewer (SSP) (who was not blinded) on all publications included in the review. Any discrepancy in the extracted information was flagged by the second reviewer and the differences were resolved through consensus. Screening and data extraction was carried out on a prospectively designed Excel database.
Data extraction
The following bibliographic information were extracted: study title, name of the first author, year of publication, name of the study site and country. The following maternal and child characteristics were extracted: age of the mother, period of gestation (or trimester), treatment administered including drug dosage, follow-up duration, the outcome of the treatment for mother (cured, relapsed, death), and foetal outcomes (abortion, stillbirth, premature birth, healthy born, vertical transmission).
Definitions
The records were classified as: case report/case series, prospective cohort or retrospective cohort studies. Records describing one or a small group of patients included as a part of prospective (or retrospective) studies in which VL in pregnancy was not of primary focus were considered as case report/case series. Similarly, studies that described a cohort of pregnant women without selection of a non-pregnant comparator group were also considered as case series. Countries were classified into sub-regions according to United Nations designation of geographical regions [33].
Data analysis
Since majority of the studies included were either case reports or case series, analysis of data was restricted to presentation of descriptive statistics and meta-analysis was not carried out. Descriptive summaries were presented for the characteristics of the studies included in the review, maternal characteristics (trimester, gestational age), treatment regimen including dosage and duration, clinical outcomes on the mother and the child. Graphics were generated using R software [34].
Assessment of risk of bias
The risk of bias in case report/case series was assessed using a checklist proposed in Murad- 2018 [35]. The following domain were assessed: patient selection, ascertainment of exposure, outcome assessment, adequacy of follow-up, and reporting of results. A single case report was considered to be at a high risk of selection bias whereas a series of cases selected based on an audit of complete records over a study period was considered to be at a low risk of selection bias. Bias in ascertainment of exposure was considered to be high if the diagnosis of VL was based solely on clinical features. For cohort studies (prospective or retrospective), risk of bias was assessed using The Newcastle-Ottawa scale. Two authors (PD, SSP) independently assessed the risk of bias in the studies included.
Results
We identified 395 records from the literature searches up until 26th of March 2020, of which 272 were unique after removing duplicate entries. Of the 272 unique records, 99 were excluded at title and abstract screening stage (Fig 1) leaving 173 records for full-text assessment of which 53 met the eligibility criteria for inclusion in the review (Fig 1). An additional 17 records were identified by searching the references of the eligible records and through personal communication. A total of 70 records published from 1926 through 2020 were included in this review of which were 69 were case-reports or case-series and 1 was a retrospective cohort study with non-pregnant patient as a comparative group (Table 2). Further details on the studies included in this review are presented in supplemental files (S1 Data, S2 Data).
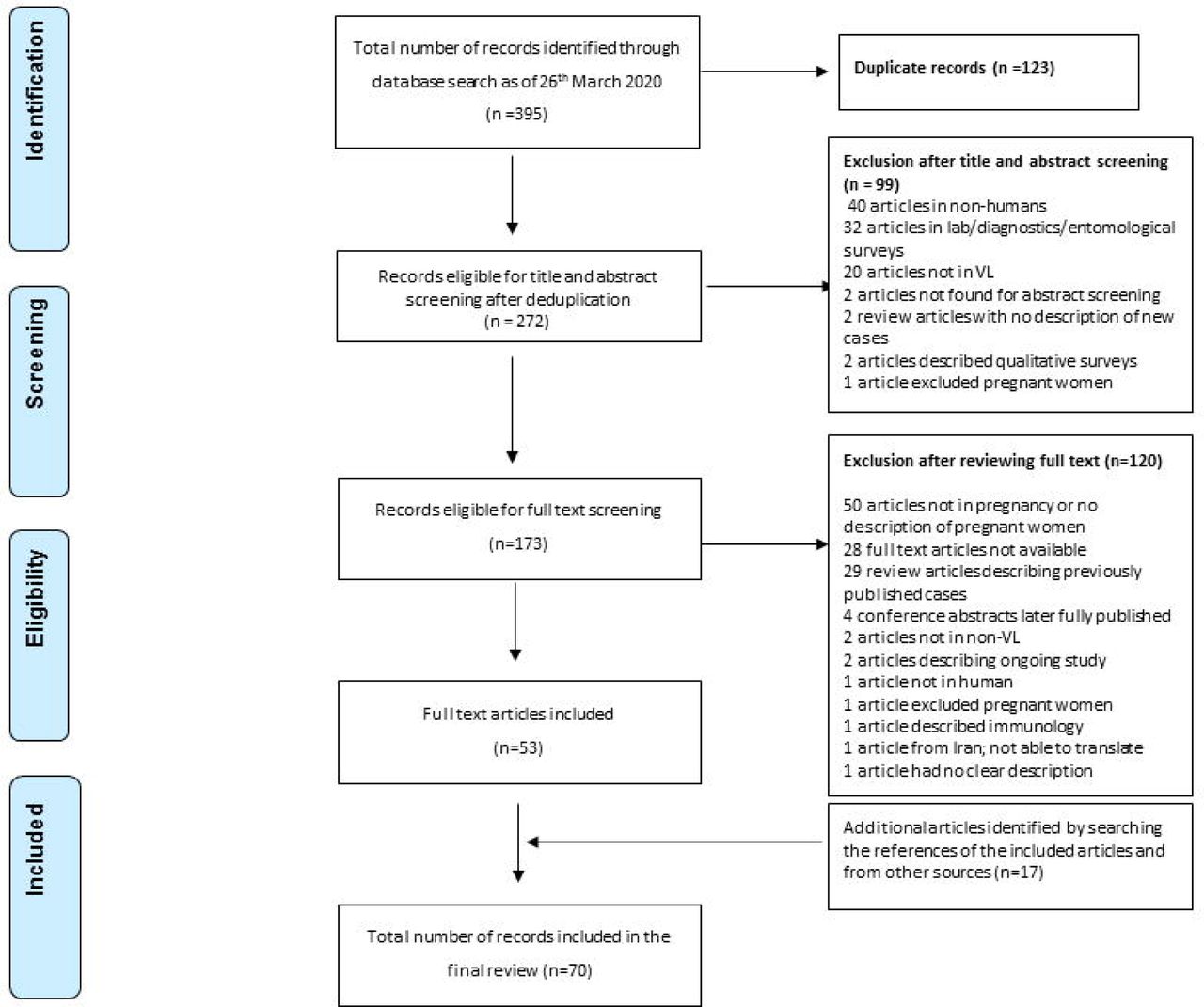
Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram of publications screened
Description of reported 447 cases of VL in pregnancy
Spatial distribution
A total of 21 (30.0%) records were from Europe, 21 (30.0%) from Southern Asia, 13 (18.6%) from South America, 8 (11.4%) from Northern America, 5 (7.1%) from Eastern Africa, and 1 (1.4%) record each were from Eastern and Western Asia. There were 16 records from India (22.8%), 13 (18.6%) from Brazil, 8 (11.4%) from Sudan, and further breakdown by country is presented in Fig 2 (left panel). There were 62 (88.6%) records in English language, 7 (10.0%) in Portuguese, and 1 (1.4%) in French. The 70 records included in this review described 447 cases of VL in pregnant women, of whom 159 (35.6%) were from Sudan, 113 (25.3%) from South Sudan, 80 (17.9%) from India, 23 (5.1%) from Bangladesh, 20 (4.5%) from Brazil, 12 (2.7%) from Italy, 10 (2.2%) from Uganda, and the rest of the breakdown is presented in Fig 2 (right panel).

{kind=link}
{kind=link}
Number of records and patients by country of origin
Treatment regimens
Of the 447 pregnant mothers identified, the disease was detected during pregnancy in 394 (88.1%), retrospectively confirmed after giving birth in 52 (11.6%), and the time of identification was not clear in one (0.2%). Ten (2.2%) were suspected of having carried the infection during their pregnancy, of whom 6 were cases of sub-clinical persistence of the parasites without the mother ever suffering from the disease previously. One case of oligosymptomatic mother was identified in Brazil [36] (Table 2). Of the 394 mothers whose infection was identified during pregnancy, 344 (89.1%) received a treatment, 3 (0.8%) were untreated, and the treatment status was not clear in the remaining 47 (12.2%) (Table 2). Description of characteristics and outcomes among 344 mothers who were treated and 3 untreated mothers are presented next.
Liposomal Amphotericin B (n=202) There were 5 (2.5%) mothers treated in the first trimester, 8 (4.0%) in second trimester, 9 (4.5%) in third trimester, and the time in pregnancy was not clear in 180 (89.1%). Survival status was not reported or was unclear in 26 (12.9%) mothers and from the remaining 176 mothers, a total of four (2.3%) maternal deaths were reported. There were a total of 5st (2.9%) miscarriages (trimester not clear), 1 (0.6%) foetal death (from a mother in 1 trimester), 1 (0.6%) stillbirth (trimester not clear), and 1 (0.6%) premature birth (trimester not clear). Three cases of vertical transmission were identified [37–39]: one was detected immediately after vaginal birth (the baby was treated with L-AmB and recovered successfully), another at 11 months after birth (treatment information not available), and for the third case, vertical transmission was suspected at 8 months after birth (treated with sodium stibogluconate 20 mg/kg IV for 20 days and discharged) (Table 3).
Details of 26 reported cases of confirmed or suspected congenital VL
Pentavalent antimony (n=92)
There were 20 (21.7%) mothers in the first trimester, 45 (48.9%) in the second, 22 (23.9%) in the third, and the time in pregnancy was not clear in 5 (5.4%). Survival status was available on 87 (94.6%) mothers of whom 4 (4.6%, 4/87) died due to hepatic encephalopathy [40]. There were 24 (27.6%) abortions (or spontaneous abortions) [13, 41], 2 (2.3%) miscarriages, 2 (2.3%) pre-term births [40, 42], and 1 (1.1%) mother required splenectomy after delivery due to poor recovery [43]. One of the babies died due to myelomeningocele 3 hours after birth [40], another died one day after being born [44], another died due to VL at 2 months [40], and one was born with Down’s syndrome to a 47 years old mother [40]. There were 3 cases of vertical transmission identified [45–47], detected at 6, 7, and 12 months after birth. All three of them were treated with PA; 1 baby died (who was born with signs of intra- uterine growth retardation and was diagnosed with vertical VL at 7 months) and the other two survived (Table 3).
Amphotericin B deoxycholate (n=20)
Of the 20 mothers treated with amphotericin B deoxycholate, 3 (15.0%) were in their first trimester, 6 (30.0%) in the second, 3 (15.0%) in the third, and the trimester was not clear in 8 (40.0%). There was one (5.0%) maternal death after 7 days of treatment due to haemorrhagic complications occurring after delivery (the mother was in 28.7 ± 7.8 weeks of pregnancy–exact time not available) [48]. The remaining 19 mothers were discharged alive.
The delivery of babies was described as normal for 18 mothers, haemorrhagic complication occurred in a mother after delivery (as described earlier) [48], and the information was not reported on 1. There was no evidence of vertical transmission of the disease in 12 (60.0%) babies in whom the information was reported. Nineteen of the children were alive and the survival status for 1 was missing.
Pentavalent antimony plus paromomycin (aminosidine) (n=11)
Eleven pregnant mothers were treated with sodium stibogluconate plus aminosidine (paromomycin) [14, 49]. Information regarding trimester, maternal survival status, or vertical transmission were not available. One spontaneous abortion was reported [49].
Liposomal amphotericin B plus pentavalent antimony (n=4)
Four mothers were treated with the combination regimen [50], of whom two in the second trimester and two in their third. L-AmB was administered at 3–7 mg/kg daily on days 1, 6, 11 and 16 (or on days 1, 2, 3, 4, 10 and 15), followed by 20 mg/kg sodium stibogluconate intramuscularly once daily for 30 days. All four mothers were discharged alive. At discharge, one mother delivered a healthy baby and the remaining three were still pregnant – no follow-up data was available.
Paromomycin (aminosidine) (n=3)
Three pregnant mothers were treated with paromomycin administered by deep gluteal intramuscular injection once daily for 21 consecutive days [51]. The delivery was described as normal for all three with normal healthy babies at birth and all three mothers were alive.
Unclear drug name (n=12)
Two publications described one case each without reporting the name of the drug administered [52, 53]. In an article, the number of mothers (n=10) allocated to each drug arm (pentavalent antimony or amphotericin B deoxycholate) was not clear [54]. Two (16.7%) of the mothers were in their third trimester and the status was unknown for the remaining 10 (83.3%). There were two (16.7%) maternal deaths [54] and two cases of vertical transmission [52, 53]. The first one was identified at 8 months after birth and another at 6 weeks after birth (the baby died after 3 days). Both babies were administered treatment upon detection of VL.
Untreated (n=3)
Three cases of VL identified during pregnancy were untreated [12,55,56]. Treatment was deferred until after delivery due to safety concerns in one study [12]; there were signs of intra-uterine growth retardation requiring emergency C-section, and both mother and the child were alive. The second mother was not treated due to lack of adequate hospital resources [55]; the baby born to the mother died after 2 months due to malnutrition with no evidence of vertical transmission. In the third case, VL was diagnosed but the mother died after giving birth and before treatment could be administered [56]; the baby also died and foetal part placenta examination revealed presence of Leishman Donovan bodies by PCR indicating vertical transmission.
Confirmed/probable/suspected vertical transmission
We identified a total of 26 cases of confirmed, probable or suspected cases of vertical transmission (Table 3). The median time to detect vertically transmitted VL was 6 months (range: 0–18 months). Eleven children were born to mothers in whom the disease status was confirmed during their pregnancy (3 were treated with L-AmB, 3 were treated with PA, the drug name was not clear in 2, 1 was untreated and the treatment status was not clear in remaining 2). Histopathological examination of the placenta confirmed the vertical transmission of the disease in two cases [47, 56] and this was not reported for the remaining cases. Treatment status was described in 18 children, of whom 11 received pentavalent antimony, 6 received L-AmB and 1 received amphotericin b deoxycholate. Two of the children died (one received pentavalent antimony and the drug name was not clear in the other).
Risk of bias assessment
Of the 69 case reports/case series, 48 (69.6%) were considered to be at a high risk of bias in patient selection, 9 (13.0%) were at high risk of exposure (confirmed VL status) ascertainment bias, 12 (17.4%) were at high risk of outcome ascertainment bias, 13 (18.8%) at high risk of incomplete reporting bias, and 14 (20.3%) studies were at a high risk of bias due to inadequate follow-up (See S1 Table). One retrospective cohort study with a comparative group of non-pregnant patient group was considered of high quality.
Discussion
The occurrence and effects of VL during pregnancy is under-researched and poorly understood as evidenced by having identified only 70 publications describing a total of 447 cases of VL in pregnancy in the past 90 years.
The small case volume reported in the literature could have several explanations. In the first place, there is an apparent imbalance in caseloads with predominance of the disease among males; ascribed to biological or behavioural causes [3,17,63,105–107]. Pentavalent antimony is contraindicated in pregnancy and was the first line therapy before the development of Liposomal amphotericin B (L-AmB) – this might have traditionally dissuaded physicians from treating VL during pregnancy and leaning towards postponing the treatment until after delivery unless treatment is absolutely warranted [12]. However, this situation might have changed recently as liposomal amphotericin B has no contraindication during pregnancy and is the treatment of choice. It has also been postulated that early pregnancies are missed due to spontaneous abortion caused by VL [63]. Women with childbearing potential or those who are already pregnant are systematically excluded from VL clinical studies and only a third of the patients enrolled in clinical trials are females [17]. For example, of the 158 studies indexed (to date) in the IDDO systematic library of VL clinical trials, 52 studies presented details from screening logs of patients (33,455 patients were screened; 17,572 patients were excluded including 32 pregnant women, and 15,883 included) (See S1 Data) [32]. Assuming all those screened for eligibility indeed had the disease, this would give an estimated 0.096% (likely an underestimate) of the total cases of VL to be pregnant women. If there are 100,000 cases per year, this translates to a minimum of 96 cases of the disease in pregnancy per year. It is clear that the likely size of the problem is much bigger than what can be estimated from available reports. For example, during Jan 2016–Jul 2019 in Lankien, Jonglei state, South Sudan, out of 4,448 cases of VL diagnosed, 39% occurred in women of childbearing age, and 13% of the women (2.5% of all cases) were pregnant [2]. It is also likely that the clustering in space and time of reported cases (more than half of all cases in this review were from studies in Sudan or South Sudan after 2005) is more a result of local interest into the subject matter than a true reflection of disease burden.
There was also geographical disparity in the treatment regimens used, reflecting heterogeneity in treatment practices. Only half of the patients received amphotericin B regimens in studies conducted in Africa compared to more than two-thirds of the patients from Asia. There was a total of 11 maternal deaths; four (4.6%, 4/87) occurred in those treated with pentavalent antimony-based regimens, 4 (4/176; 2.3%) among those treated with L-AmB, 1 (1/20, 5.0%) with amphotericin b deoxycholate, and the drug name used for the treatment was not clear in 2 (16.7%,2/12) cases. Spontaneous abortion following PA regimen was observed in just over a quarter of the mothers (24/88, 27.3%) while there were a total of 5 (2.9%) miscarriages and 1 (0.6%) foetal death following L-AmB regimen. Taken together, these results support the use of liposomal amphotericin B for the treatment of VL during pregnancy.
Our review identified 26 cases of vertically transmitted VL with a median time of detection of 6 months (range: 0–18 months). This suggests that children born to mothers with VL during pregnancy require a longer post-treatment follow-up than the standard 6-months follow-up duration among non-pregnant patients to monitor the well-being of the maternal- foetal pair. The underlying mechanism of the onset of clinical leishmaniasis among neonates and infants born to a successfully-treated mother during pregnancy (2.4% overall) is currently not clear; it has been ascribed to imbalances in immune-mechanism modulated by T cell responses (Th1/Th2) [10] or by parasites entering a state of dormancy in the lymph nodes [72].
Our review has identified limitations in reports of VL in pregnancy. Complete information was often not available on treatment administered and on efficacy and safety outcomes for the mother and baby. For 12% of the mothers, it could not be ascertained whether they had received any treatment or not. Majority of the studies were considered to be a high risk of bias for patient selection while some retrospective studies were at high risk of bias for ascertainment of exposure domain as VL diagnosis was purely based on clinical signs and symptoms or suspicion. This suggests that existing practices for management of VL in pregnancy is guided by limited evidence generated from case reports and small case series. High quality studies (such as Pekelharing-2020 [2]) is warranted for generation of a robust evidence regarding safety and efficacy of antileishmanial agents during pregnancy. There was also a lack of standardised reporting as information was missing on several critical parameters such as trimester status, time on detection of VL, and therapeutic outcomes of the mother and the child. Taken together, these findings highlight the need to improve and harmonise the reporting of VL in pregnant women. We have outlined a minimum checklist of items that might be useful for reporting purposes (Box 1).
As conducting randomised controlled trials during pregnancy poses ethical challenges, it is important to maximise currently available information from observational studies and case reports to gauge the potential safety of the therapies in pregnant women. Data from mothers who become pregnant after completion of therapy but within the follow-up period enrolled in trials might provide further resource, especially on the reproductive consequences of the treatment (Table 4). The recently proposed safe ethical framework for the recruitment of women susceptible to and becoming pregnant is an important development towards filling the existing knowledge gap [18]. Like for many NTDs, there is currently an absence of a comprehensive pregnancy-specific registry for exposures to antileishmanials, with the exception of the one dedicated for miltefosine [108]. Therefore, creating an open registry where all these cases are indexed and continually updated would help in better characterisation of the safety aspects of the drugs. Finally, the Infectious Diseases Data Observatory (IDDO) data platform, that is currently standardising individual participant data from several VL clinical studies, offers a unique resource to explore host, parasite, and drug dynamics affecting the safety and efficacy in pregnant populations [109].
Description of patients enrolled in clinical trials who became pregnant after completion of treatment
Conclusions
In conclusion, this review brings together scattered observations on VL in pregnant women and the cases of vertically transmitted VL reported in the clinical literature. Available reports clearly underestimate the scale of the problem. Existing therapeutic guidelines regarding the usage of drugs in pregnancy is guided by limited evidence generated from case reports and small case series. Our review suggests that liposomal amphotericin B should be the preferred treatment for VL during pregnancy.
List of boxes
Proposed minimum variable recording and reporting for studies or case reports for VL in pregnancy
Declarations
Authors’ contributions
Conceptualization : PD, PJG, PLO
Data Curation : PD, SSP
Formal Analysis : PD, SSP, PJG, PLO
Funding Acquisition : PJG
I vestignation : PD, SSP, PJG, PLO
Methodology : PD, SSP, EH, BJM
Project Administration : PD, PLO
Resources : PJG, PLO
Software : PD
Supervision : PJG, PLO
Validation : PD, SSP, PJG, PLO
Visualization : PD
Writing – Original Draft Preparation : PD, PLO
Writing – Review & Editing : PD, SSP, BJM, EH, KR, FA, PJG, PLO
Availability of data and material
The database(s) supporting the conclusions of this article are available within the tables and figures presented within the manuscript along with the supplemental files (S1 Data, S2 Data).
List of supplemental files
S1 Text: PRISMA checklist
S2 Text: Search details
S1 Data: Screening list
S2 Data: Study data
S1 Table: Risk of bias assessment
Ethics approval and consent to participate
Not applicable
Consent for publication
Not applicable
Financial Disclosure Statement
The review was funded by a biomedical resource grant from Wellcome to the Infectious Diseases Data Observatory (Recipient: PJG; ref: 208378/Z/17/Z). The funders had no role in the design and analysis of the research or the decision to publish the work.
Competing interests
None
Acknowledgements
We would like to thank for the Prof. Bernhard Lämmle and his team for helpful responses on queries related to their manuscript.
Footnotes
Email addresses: PD prabin.dahal{at}iddo.org, SSP sauman.singh{at}iddo.org, BJM brittany.maguire{at}iddo.org, EH eli.harriss{at}bodleian.ox.ac.uk, KR koert.ritmeijer{at}amsterdam.msf.org, FA falves{at}dndi.org, PJG philippe.guerin{at}iddo.org, PLO piero.olliaro{at}ndm.ox.ac.uk
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.
- 24.
- 25.
- 26.
- 27.
- 28.
- 29.
- 30.
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.↵
- 52.↵
- 53.↵
- 54.↵
- 55.↵
- 56.↵
- 57.
- 58.
- 59.
- 60.
- 61.
- 62.
- 63.↵
- 64.
- 65.
- 66.
- 67.
- 68.
- 69.
- 70.
- 71.
- 72.↵
- 73.
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.
- 103.
- 104.
- 105.
- 106.
- 107.↵
- 108.↵
- 109.↵
- 110.
- 111.
- 112.
- 113.
- 114.




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos