
Abstract
Background The COVID-19 pandemic significantly disrupted primary care in Canada, with many walk-in clinics and family practices initially closing or being perceived as inaccessible, pharmacies remaining open with restrictions on patient interactions, rapid uptake of virtual care, and reduced referrals for lab tests, diagnostics, and specialist care. The PUPPY Study seeks to understand the impact of COVID-19 across the quadruple aim of primary care, with particular focus on the impacts on patients without attachment to a regular provider and those with chronic health conditions.
Methods The PUPPY study builds on an existing research program exploring patient access and attachment to primary care, pivoted to adapt to the emerging COVID-19 context. We will undertake a longitudinal mixed methods study to understand critical gaps in primary care access and coordination, comparing data pre- and post-pandemic in three Canadian provinces (Quebec, Ontario, and Nova Scotia). Multiple data sources will be used including: a policy review; qualitative interviews with primary care policymakers, providers (i.e., family physicians, nurse practitioners, and pharmacists), and patients (N=120); and medication prescribing and healthcare billings. The findings will inform the strengthening of primary care during and beyond the COVID-19 pandemic.
Interpretation This is the first study of its kind exploring the impacts of COVID-19 on primary care systems, with particular focus on the issues of patient’s attachment and access to primary care. Our multi-stakeholder, cross-jurisdictional team will collaborate to rapidly disseminate findings and share implications for future policy and practice.
Background
More than 75% of healthcare visits in Canada are within primary care.(1) Access to primary care is the foundation of a strong healthcare system; vital to achieving the quadruple aim of enhancing patient experience, promoting care-team wellbeing, improving population health, and optimizing costs by managing health in primary care through the life course and reducing burden in acute care.(2) Primary care includes comprehensive and routine care, health promotion, disease prevention, diagnosis and treatment of illness and injury, coordination of care with other specialists and other care services. However, barriers to equitable primary care access were present prior to the COVID-19 pandemic.(3–5)
Early findings of COVID-19 Impact
COVID-19 caused unprecedented disruption to primary care in Canada and internationally. During the peak of the COVID-19 first wave in Canada, many primary care clinics reduced hours,(6) leaving patients and caregivers uncertain about how to access care. Primary care providers were required to make rapid shifts in practice to comply with infection prevention and control requirements, incorporate COVID-19 triage and non-acute management, address reduced referral and diagnostics access, and implement virtual care where possible.(7–10) Primary care providers had to engage in practice redesign, secure access to personal protective equipment and, in the case of pharmacists in some jurisdictions, integrate changes in scope of practice.(11) Many primary care providers were also redeployed or prepared to be redeployed to COVID-19 testing and treatment roles.(10,12)
Healthcare access is defined as “the opportunity to have healthcare needs fulfilled”(13) and is influenced by: a) accessibility of providers, organizations, institutions and systems; and b) the ability of individuals, households, communities, and populations to access primary care. These influential elements have had a COVID-19 “anvil” dropped on their capacity to provide, and access, primary care (see Figure 2).
COVID-19 caused delayed and forgone care concurrent with increased mental health needs of providers and patients. As the pandemic continues, there are anticipated waves of COVID-19 fallout (Figure 1).(14,15) While emerging evidence illustrates significant impacts of the pandemic on primary care systems globally,(6) the impacts of COVID-19 on patient attachment and access to primary care remain unclear. Evidence is also mounting on the impact of COVID-19 on patient and provider wellbeing.(16) The current study will address these issues and inform strategies for strengthening primary care during and beyond the pandemic.
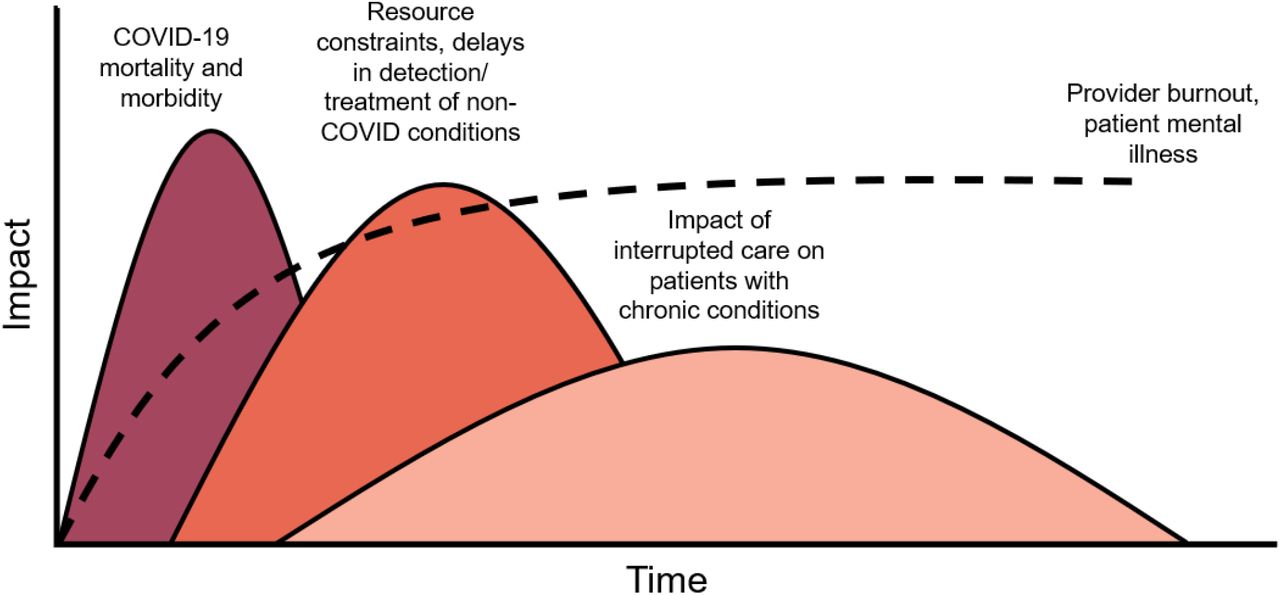
Anticipated waves of COVID-19 pandemic on primary care (adapted from Dr. Victor Tseng, MD)

Depiction of the COVID-19-induced disruption to the accessibility of the healthcare system and the ability of patients to access the system (adapted from Levesque et al. 2013)
{kind=link}
{kind=link}
{kind=link}
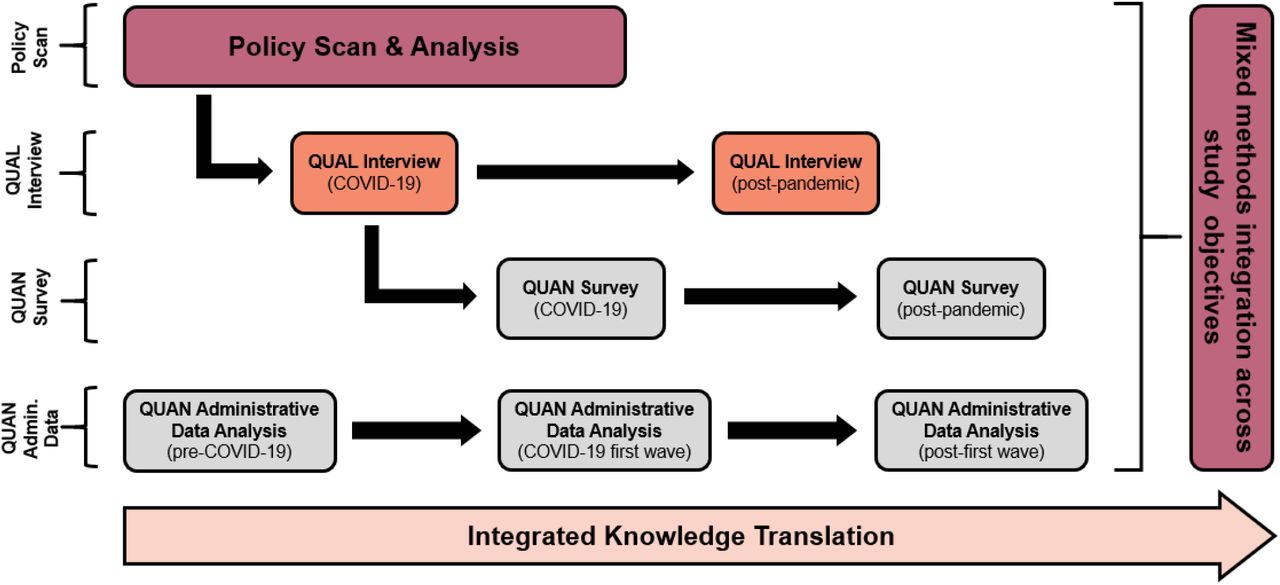
Overview of study objectives, methods, and relationships between activities
Pivoting a program of primary care research to address COVID-19
At the onset of the COVID-19 pandemic, many health research studies in Canada halted while a pandemic plan and appropriate public health measures were created and enacted. For example, our cross-provincial CIHR-funded CUP-Study (Comparative analysis of centralized waitlist effectiveness, policies, and innovations for Connecting Unattached Patients to primary care providers) examining pre-COVID attachment to primary care in three provinces, namely Ontario (ON), Québec (QC), and Nova Scotia (NS), was put on hold for several months.(17)
As the pandemic continued, our team recognized that existing research aims and methods were insufficient to address the impacts of the novel COVID-19 context. Further, new research questions were emerging rapidly due to changes in the policy landscape and provider roles in primary care systems across Canada. Thus, it was necessary to pivot existing studies to include pandemic-specific analyses and capture changes in primary care systems over time, while finding novel ways to collect data in a safe way during a pandemic. We rapidly engaged with our study team, which included Departments and Ministries of Health, Health Authorities, primary care providers and their organizations, and our Patient Partners. The Co-Principal Investigators (EGM, MB, MG, JEI, MM, BC) then developed new strategies for answering emerging questions and updated methods to reflect the new COVID-19 primary health care landscape and ability to work safely. This newly expanded and updated protocol was successfully funded in June 2020.
Purpose and Objectives
This study will identify and evaluate strategies to provide primary care access and COVID-19 triage and care by family physicians, nurse practitioners, and pharmacists that can be scaled-up to promote attachment and improved access for patients across and beyond COVID-19 waves. We will focus particularly on patients who are unattached, with complex care needs, and/or experiencing social barriers to care, as primary care-based support for these populations may lead to better outcomes for these patients and the healthcare system across the quadruple aim.
Objectives:
Identify primary care policies and interventions implemented in response to COVID-19 and describe how they affect primary care attachment (i.e., demand) and accessibility (i.e., supply).
Understand how COVID-19 related changes affect: i) patients’ experience of accessing primary care, considering different needs, identity factors (e.g., age, gender) and access abilities (un- and attached patients, and/or patients with complex needs); and ii) provider health and wellbeing.
Determine how these pandemic-related changes have impacted healthcare utilization, attachment to primary care providers, and medication prescribing, as indicators of access to primary care.
Share promising strategies to provide access to primary care with policymakers, primary care providers and patients across Canada in the immediate, intermediate, and reflective phases of the pandemic.
Methods
Study design and setting
To address rapid COVID-19 impacts on policy, practice, and patient access to primary care in line with the objectives described above, a longitudinal mixed-methods observational study building from our team’s ongoing research is being conducted. Data will be collected in NS, QC, and ON using four methods, namely a) a scan of policies impacting primary care access in the wake of COVID-19; b) qualitative interviews with providers, patients, and policymakers; c) surveys of providers and patients; and d) analysis of administrative data, including centralized waitlists, billing and prescribing data, to track healthcare access and utilization, and primary care provider prescribing patterns before, during, and after the COVID-19 pandemic.
Study participants
Participants will include representation from policymakers, patients and primary care providers via qualitative interviews, surveys, and linked administrative health data. While providers from many professions contribute to primary care across systems, our study will focus on family physicians, nurse practitioners, and community pharmacists. The inclusion of the latter is due to the growing number of publicly-funded services offered by pharmacists in several Canadian jurisdictions in recent years, with limited evaluation (e.g., prescribing for minor ailments, immunizations, reviewing and managing medications, etc.),(18–21) which establish more primary care access options.
Policy Scan
Policies and contextual factors impacting primary care access will be identified through extensive provincial policy reviews and interviews with health authority, government, regulator, and corporate policymakers. The unit of analysis is provincial. We will document primary care changes in context that coincide with key developments related to COVID-19 to inform recommendations for transformation, scale, and spread. Provincial policies may include: provider hiring and funding, delivery models, including the rapid deployment of virtual care modalities across Canada, incentives, programs and innovations to help patient access, meet the needs of unattached and other vulnerable patients, and other policies that may play moderating roles in primary care (e.g., provider wellbeing). We will focus on influential policies, where policies are defined per the World Health Organization as “decisions, plans, and actions…undertaken to achieve specific healthcare goals” and identified contextual factors.(22)
The Tomoaia-Cotisel approach(23) for assessing and reporting contextual factors of primary care innovations will be applied to the qualitative and policy scan components of the study. The framework involves: engaging diverse perspectives, considering multiple policy and context levels, time, formal and informal system/culture, and identifying interactions between policies and contexts. It is tailored specifically to innovations in primary care and considers moderators at multiple levels.
Qualitative Interviews
Qualitative methods are designed to elicit experiences and perceptions of phenomena where little is known-an ideal approach to study the impact of COVID-19 in primary care. Stakeholder groups to be interviewed include patients, family physicians who do and do not take on new patients, nurse practitioners, community pharmacists, and policymakers with roles relevant to primary care access and attachment. The proposed longitudinal data collection will support interviews, n=10 participants per stakeholder group per province (N=120 participants in total), to achieve saturation.(24,25)
Interviews will be conducted during COVID-19 and post-pandemic to elicit current and retrospective lived experiences. Interview guides will be developed to reflect key issues pertinent to stakeholders. For example, providers will be asked questions pertaining to practice changes. Patients will be asked about their experience with primary care changes and the impact of these on access and wellbeing.
Policymakers will be invited to share processes for, and outcomes of, policy change and will be consulted on relevant documents to include in our policy scan for Objective 1.
Purposive and snowball sampling strategies will be used, stratifying by relevant participant characteristics. Invitations for interview participants will be distributed via the provincial centralized waitlists, partnered organizations and social media. We will iteratively revise our sampling and recruitment strategies as we collect data and learn more about patient and provider experiences.(26)
Informed consent discussions and semi-structured in-depth interviews will be conducted virtually using Zoom Videoconferencing (Zoom Video Communications Inc.) by a Masters-trained researcher. Audio recordings of interviews will be transcribed verbatim and coded in NVivo software (QSR International). Coding reports will be generated and examined to uncover themes and patterns in the data.
Preliminary thematic analysis will provide rapid reporting to stakeholders. A Framework Analysis(27) approach will incorporate the Levesque et al. conceptual framework(13) for access to healthcare and be implemented across study phases for comparative analysis. This method allows for inductive and deductive coding approaches.(27) We will code deductively to the Levesque framework and inductively from interview transcripts, allowing emergent themes to enhance what can be gleaned from the framework alone. Intra and cross-case analysis will be conducted by incorporating provincial framework analysis matrices.(27,28)
Surveys
Brief surveys for patients and providers will be developed to determine prevalence of our emerging qualitative themes. Surveys designed for providers will be delivered via the secure online Opinio Survey Tool (ObjectPlanet, Inc.) post-pandemic to measure the degree to which COVID-related policy changes have impacted primary care access and attachment, as well as their personal wellness. Recruitment support will be provided by our partners. An online patient survey at the same time point will explore patient primary care access and attachment during COVID-19. A convenience sample of 1000 patient respondents per province will be recruited using a third-party survey sampling company (N=3000). It is estimated that a sample size of 1000 per province would permit adequate segment sizes for comparison of results among patient groups and provinces. Bivariable and multiple regression models will be generated to show trends and associations on key elements across phases. Follow-up surveys will be conducted at a later point to assess changes over time.
Administrative Data
Analyses of pre-COVID-19 prescription dispensation, centralized waitlist, physician billing, and inpatient and outpatient hospital discharge data has already begun to examine effectiveness of centralized waitlists for a related study,(17) as part of an ongoing program of research into access and attachment.(29–31) As part of the PUPPY Study, we will expand this analysis to explore changes across pre-COVID-19, COVID-19, and post-pandemic periods. Harmonized indicators of health care utilization (e.g., primary care, emergency, hospitalization, and potentially avoidable inpatient care), and primary care attachment indicators (primary care provider attachment, continuity of primary care), and primary care service provision (e.g., frequency and type of primary care encounters, continuity of medication dispensation for maintenance of chronic conditions) will be measured across the three participating provinces. Change in these indicators, and in care continuity, will be estimated and compared over pandemic wave-indexed study periods.
Multivariable regression will be used to identify potential clinical (e.g., patient complexity, comorbidity) demographic and socioeconomic determinants of primary care need, and changes in these indicators over the course of the pandemic. Socioeconomic determinants are derived from the 2016 Canadian census data, including the Canadian Index of Multiple Deprivation, with a focus on dimensions of economic dependency, ethno-cultural composition, and situational vulnerability.(32) Centralized waitlist data will be used to measure primary care attachment and assess changes in access to primary care. Building on ongoing work, variation in patient primary care provider attachment rates, demand for attachment, and time to attachment among those identified on centralized wait lists will be quantified and changes in these outcomes assessed across study periods. Determinants of these outcomes will be identified, and their relative magnitude estimated, using multivariable techniques. In each province, study populations will be stratified by age, sex (and gender where feasible), degree of comorbidity and geography (i.e., urban versus rural) to identify those at greatest risk of being unattached to a primary care provider.
Ethics Approval
Ethics approval has been granted in Ontario (Queens Health Sciences & Affiliated Teaching Hospitals Research Ethics Board, #6028052; Western University Health Sciences Research Ethics Board, #116591; University of Toronto Health Sciences Research Ethics Board, #40335), Québec (Centre intégré universitaire de santé et de services sociaux de l’Estrie, #2020-3446) and Nova Scotia (Nova Scotia Health Research Ethics Board, #1024979).
Interpretation
This study is designed to provide support for primary care policymaking, provider needs, and patient access to primary care from investigation across the COVID-19 waves. We will regularly communicate emerging recommendations to our partners for timely policy optimization. This information will inform provision of care through changing pandemic contexts, including requirements for physical distancing and safety requirements. Findings will be distributed to study partners and beyond via our networks, (e.g., CanCOVID, pan-Canadian PIHCI Networks, North American Primary Care Research Group), to support cross-jurisdictional pandemic response. Immediate term early data collection will provide feedback on new policies in primary care settings and impacts on patient access, providing insight into possible unintended consequences of rapid policy transformation and revealing promising strategies. In the intermediate term, our study will document changes in the primary care policy landscape to strengthen the response to additional “waves” related to COVID-19. In the long term, findings will help us grasp the impact of these policy changes and events on the ability of systems and providers to coordinate and deliver primary care, patient access to primary care, and on health outcomes. A combination of policy briefs, digital media, and traditional knowledge translation approaches (e.g., conferences and peer-reviewed manuscripts) will be utilized.
Limitations
As the first cross-provincial study of COVID-19 pandemic impacts on primary care, the PUPPY study faces complex research challenges in that the three jurisdictions under study experienced significantly different timelines and caseloads of COVID-19 and have enacted diverse response strategies within primary care systems. While challenging, this complexity will also enable cross-case comparison, allowing analysis of contextual differences between provinces. These challenges will be mitigated by our experienced large inter-professional team, support of our partners, and multiple methods of data collection.
Conclusion
This is the first study of its kind exploring the impacts of COVID-19 on primary care systems, with particular focus on the issues of patient’s attachment and access to primary care. The study team will address rapidly evolving contexts using multiple research methods, including qualitative, quantitative, and mixed methods approaches. Findings will be shared through robust knowledge translation and exchange activities.
Data Availability
No data associated with this study are available at time of development of this protocol.
Funding Statement
We would like to acknowledge the Canadian Institutes of Health Research for their support to conduct this research in the form of a COVID-19 Rapid Funding Opportunity Grant.
Competing Interests Statement
Dr. Green would like to acknowledge that the INSPIRE-PHC research program is supported by the Ontario Ministry of Health.
Data Availability Statement
No data associated with this study are available at time of development of this protocol.
Contributor’s Statement
The study was conceived by the lead author (EGM) who also led the writing of the manuscript with active assistance of the co-authors. All authors made substantive contributions to the conception and design of the study, which includes qualitative, quantitative, mixed methods, patient engagement and/or knowledge translation components. All authors have critically reviewed this manuscript and approve the version to be published.
Participant groups involved in each of the data collection methods
Acknowledgements
We would like to acknowledge the generous support of our PUPPY study organizational partners and team members, including our academic researchers, providers, policymakers, and patient partners Sarah Peddle, Ana Correa Woodrow, Nicole Desjardins, and Danièle Roberge. A full list of our team members and partners can be found on emilygardmarshall.ca/puppy.
References




