
Abstract
While mRNA vaccines authorized for emergency use are administrated worldwide in an effort to contain the COVID19 crisis, little is known about the heterogeneity of the immune response they induce. Here, we report the first 6 weeks of a longitudinal study that quantifies the humoral immune response to BNT162b2 mRNA COVID-19 (Pfizer/BioNTech, Comirnaty) in 1245 health care providers, the Lx1000HCW-PZF cohort. We reveal a striking inter-individual variation 3 weeks after the 1st dose administration that only in part related to age and sex. While population homogeneity in robust IgG responses was reached upon 2nd dose administration, IgM and IgA levels remain low and heterogenous. Our findings of isotypic and heterogenous antibody responses to Comirnaty highlight the need for evaluating the efficacy of COVID-19 mRNA vaccine in preventing infection aside disease, and - contrary to what has been proposed – advocate for the interval between the two doses not to be extended.
Introduction
Authorization for emergency use of two mRNA COVID-19 vaccines, both encoding the most immunogenic protein of SARS-CoV-2, spike, was conceded in late 2020 by regulatory agencies such as FDA, WHO and EMA. These authorizations were based on results of phase 3 clinical trials that demonstrated high standards of safety and high levels of efficacy in preventing symptomatic SARS-CoV-2 infections [1, 2]. While these vaccines are introduced around the world and administered to millions of people, there is a growing and acute need to evaluate their effectiveness at the population level, an endeavour that may require months of epidemiological studies. Awkwardly, little attention has been given to whether immune responses triggered by mRNA vaccines encoding SARS-CoV-2-spike are homogenously robust. To date, immune responses have been seldom measured upon mRNA COVID-19 administration, and when this was the case, the observations concerned very small groups of participants ranging from n=8 to 20 [2-5]. Immunogenicity of mRNA COVID-19 vaccines and their inter-individual variation can be easily monitored in medium to large cohorts by measuring serum reactivities to the vaccinal antigen or part of it. Notably, the receptor binding domain of spike contains the AA motifs permitting SARS-CoV-2 binding to ACE2 receptor, a prerequisite for infection, and serum reactivity to this region encompasses neutralizing activity [6]. Anti-spike immunoglobulins are also expected to mediate viral particle removal through antibody-mediated opsonization and phagocytosis, and through the recruitment of the complement system. Beyond their direct functionality, vaccine specific antibodies are markers of adaptive immunity response.
In the vast majority of cases, SARS-CoV-2 infection associates with the induction of robust IgG anti-spike responses lasting for 6 to 8 months, while strong IgM anti-spike reactivities are transient. Strong IgA anti-spike responses are frequent and may be more prevalent in symptomatic patients ([7], and our own observations). IgA are either dimeric or monomeric. Dimeric IgA are produced at mucosal sites and result from bonafide germinal centre reactions involving helper T cells. These have been shown to be part of the humoral response triggered by SARS-CoV-2 and to confer neutralizing capacity [8]. Monomeric IgA are abundant in blood, though partial or total circulating IgA deficiency is common in humans [9]. Neither the function or the origin of circulating IgA is well understood. Astonishingly, it still remains unclear whether mRNA vaccine can be expressed at mucosal sites. Overall, immune responses induced by natural SARS-CoV-2 infection seems to protect from novel infection with the same virus variant. Whether RNA vaccines provide the same broadness of Ig class has not been formally reported.
The COVID-19 vaccination campaign in Portugal was initiated in late December 2020 coinciding with a peak of disease transmission which reached 131 new daily cases per 100,000 inhabitants and caused a most intense demand for hospital care. The vaccination roll-out started with hospital healthcare professionals at the COVID-19 response frontline, who showed during 2020 a level of exposure to the virus somewhat higher than the general population (our unpublished results). Here, we report on the humoral response to BNT162b2 mRNA COVID-19 (Pfizer/BioNTech, Comirnaty) vaccination in healthcare professionals working in a group of hospitals in Lisbon, Portugal.
Results and Discussion
The study enrolled 1245 healthcare providers working at 3 hospitals, administratively grouped in a single regional centre (CHLO), in Lisbon, Portugal. Participants were scheduled to initiate BNT162b2 mRNA (Pfizer/BioNTech, Comirnaty) vaccination in December 2020/January 2021, along the original protocol of 2 doses with a 3 weeks interval. The cohort presents a biased sex ratio (77% female, 23% male), as is common in this professional area, and encompasses a broad age range (19 to 70 years, median 41 years for females, 39 years for males). Venous blood was collected every 3 weeks, at the days of 1st (d0) and 2nd (d21) dose administration, and 21 days after the 2nd dose administration (d42). Drop out was of 14.8% (n=184) with 12.5% (n=156) during the first phase (Figure 1).

Hospital healthcare workers donated blood samples before vaccination with BNT162b2 RNA (day 0), three weeks after the first dose (day 21) and three weeks after the second dose (day 42). A) Cohort description. B) Age distribution of the cohort (19-70 years) stratified by sex. C) Vaccination and sample collection schedule.
Diagnosed COVID-19 prior to vaccination was an exclusion criterion in accordance with the national vaccination plan. It is estimated that only about 10-20 % of COVID-19 cases were diagnosed in 2020 in Europe overall, leaving most a/pauci-symptomatic exposure undetected. To complete the identification of participants with prior infection, the entire cohort was tested at d0 for serum reactivity against SARS-CoV-2 nucleocapsid (N), identifying 39 such cases (3%). In addition, 8 participants were diagnosed COVID-19 during the first week of the study, and an additional 11 showed SARSCoV-2 N antigen reactivity at d21, all cases likely related to an outbreak at the participating hospitals.
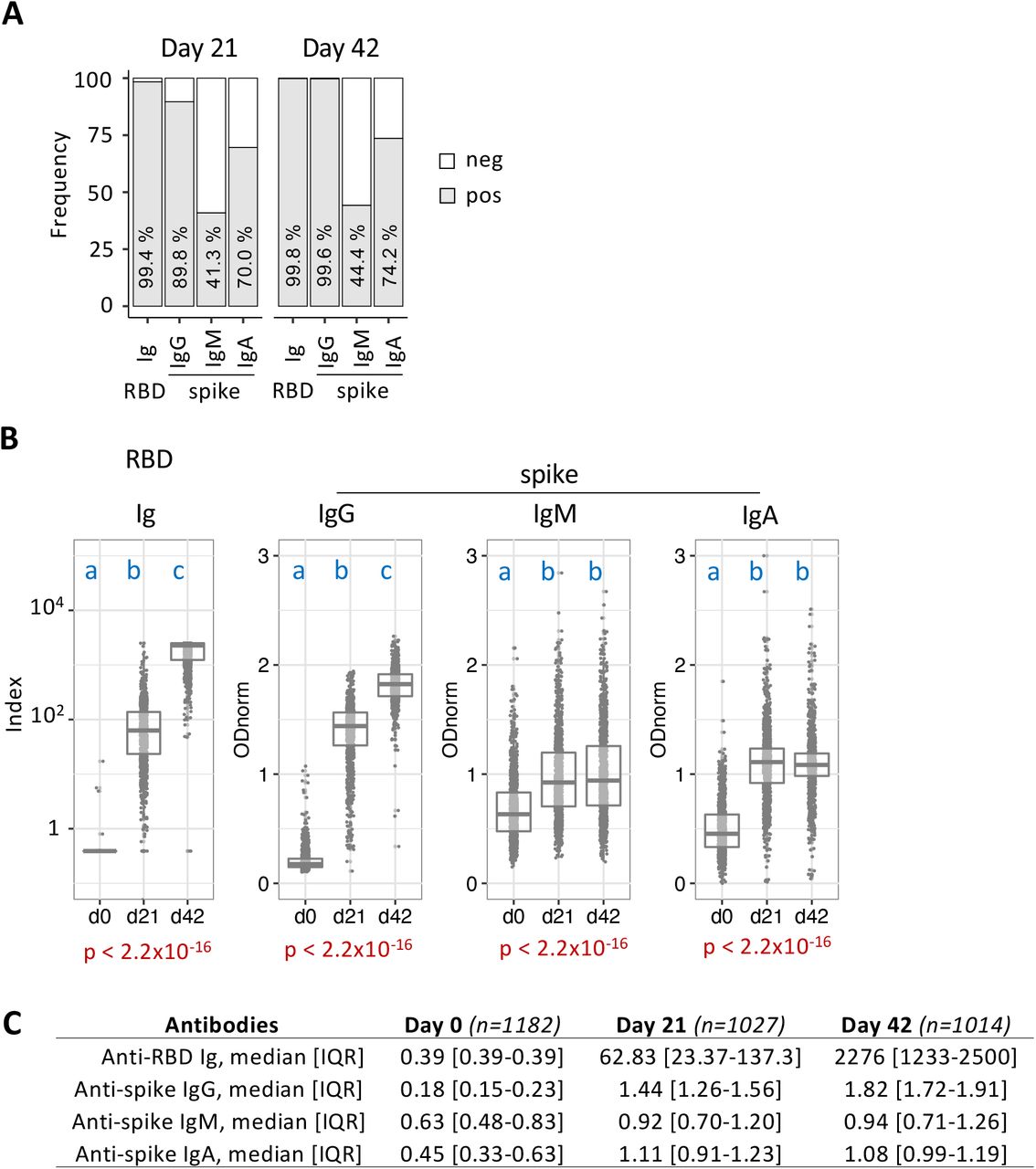
All collected samples were analysed for bulk reactivity against SARSCoV-2-RBD, using a commercial ECLIA, and for isotype specific (IgG, IgM and IgA) anti-SARSCoV-2-Spike using an in-house ELISA assay. To directly determine the immunogenicity of Comirnaty, SARS-CoV-2 naïve participants, defined as negative for serum anti-SARS-CoV-2 N reactivity, were first analysed using a binary classification (Figure 2A). As expected, seroconversion was massive, with bulk anti-RBD reactivity detected at similar frequency whether at 3 weeks post 1st or 2nd injection (99.4 and 99.8%, respectively, d21 and d42). Isotype class analysis of anti-Spike antibodies revealed a heterogeneous response with 90% positivity for IgG, 41% for IgM and 70% for IgA at day 21, with progression by d42 only for the IgG class that reaches 99,6%. This result indicates that immunogenicity of BNT162b2 mRNA COVID-19 vaccine favours the induction of anti-spike IgG.

Sera collected the day of BNT162b2 mRNA 1st dose administration (day 0), three weeks after the 1st dose (day 21) and three weeks after the 2nd dose (day 42) were analysed for anti-SARS-CoV-2-RBD Ig (ECLIA) and anti-SARS-CoV-2 full-length spike protein IgG, IgM and IgA (ELISA). Individuals positive for reactivities against SARS-CoV-2 N antigen were removed from the dataset. A) Seroconversion defined by frequency of samples testing positive (grey bar) at the indicated day and assays. Respective values are indicated inside each grey bar. B) Semi-quantitative measurements, where the data points represent individual participants and overlayed boxes represent median and interquarile range (IQR). Note the y scale differs for the anti-RBD ECLIA and the anti-spike ELISA data. Index =0,9 and ODnorm=1 define the threshold defining positivity in (A). C) Number of participants, median and IQR for each assay at the designated collection days. For each assay, level of significance of overall response across the three collection time points (Kruskal-Wallis test) is represented below the respective panels (red print). Pairwise comparison of collection days used Mann-Whitney statistics with correction for multiple testing. Compared groups are identified by different letters if pairwise p-value <0.05 (blue print).
Quantitative analysis (Figure 2B and C) revealed very large inter-individual heterogeneity in the amplitude of the antibody response at day 21, for both anti-RBD and anti-spike reactivities, and across isotype classes. The ranges of anti-spike responses at d21 post 1st dose vaccination are comparable to those observed in COVID-19 patients, though IgA levels were more frequently higher in the latter group (not shown). The 2nd vaccinal dose resulted in major increment of anti-RBD Ig and anti-spike IgG levels and homogenisation to high values, with both measurements reaching saturation for the vast majority of participants. The median anti-spike IgG response was estimated to correspond to titres of 2×104 at day 42 versus 2×103 at day21, indicating the 2nd dose provides an increment higher than 10 folds. In contrast, the 2nd vaccine dose does not improve spike-specific IgM and IgA responses. Given that the responses were measured 3 weeks after each dose administration, this result is consistent with classical IgM responses that peak during the first week post antigen encounter, and are not significantly boosted through memory cell recall. The unchanged IgA response after the 2nd vaccine injection strongly suggests most of the IgA anti-spike antibodies detected are of the T cell independent class and monomeric, which are unlikely to confer mucosal immunity upon subsequent SARS-CoV2 infection. In turn, this feature suggests RNA vaccine may not prevent the early stages of SARS-CoV2 infection at mucosal site.
Of note, our analysis at day 0 reveals a sizable fraction of participants presenting IgM anti-spike reactivity prior to vaccination (12,5% above threshold as compared to 0,8% when testing sera from 1000 donors collected before COVID19 pandemic). This result corroborates our unpublished longitudinal analysis of 1500 hospital healthcare workers during 2020, and the nature of these peculiar IgM reactivities will be discussed elsewhere.
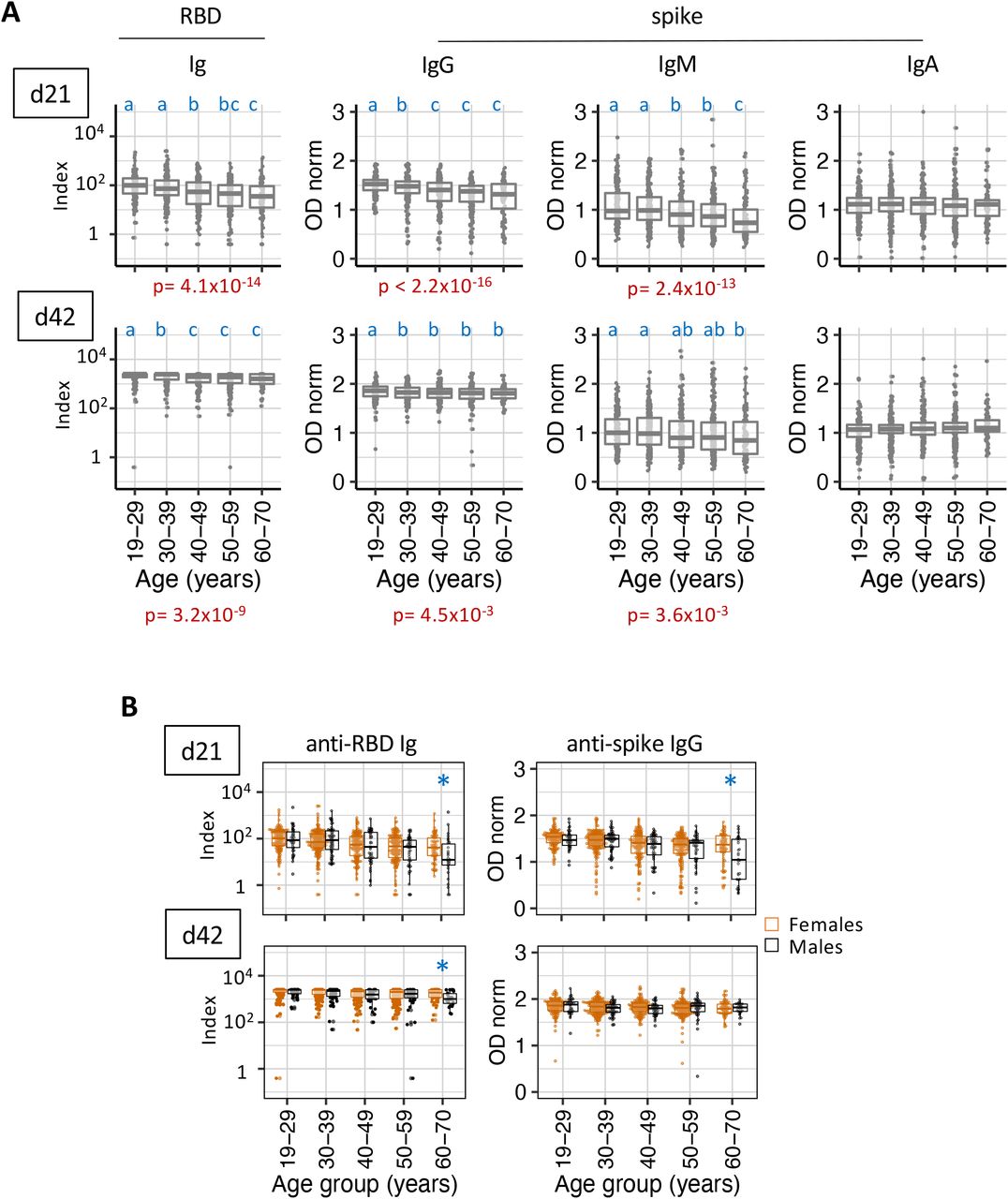
As a first approach to identify the basis of the inter-individual heterogeneity in the response to Comirnaty vaccine, we performed stratified analyses for 3 parameters. We first excluded concerns of RNA vaccine stability, by ascertaining the spread in anti-spike reactivity levels did not differ in groups of participants who received the 1st vaccinal dose at different calendar days (not shown). We next performed stratified analysis by age groups (in 10-year bins) and revealed a cumulative negative effect of age on the level of the humoral response, more marked after the 1st dose administration (d21) but still significant 3 weeks after the 2nd vaccination (d42). The age effect was evident for bulk anti-RBD reactivity and for anti-spike IgG and IgM, but not IgA levels, highlighting again the unconventional nature of the IgA response to this RNA vaccine (Figure 3A and B). Despite the overall higher immuno-competence of the youngest age strata (19-29 years), levels of specific reactivities were still strikingly spread at d21 in this age group (e.g. titre range was estimated from 2×102 to 2×104 or above for IgG). Further stratification of the cohort by age and sex revealed that in the older strata (60-70 years of age) males presented lower anti-RBD and anti-spike responses, as compared to females, a difference more marked at d21 (Figure 3C and D). Sex effect in this older age group affected also the frequency of IgG seroconversion after 1st dose administration, with a positivity of 82.7% for females, and 56.7% for males at day 21. These results warrant a detailed evaluation of COVID-19 mRNA immunogenicity in the elderly, all the more as they are critically affected by this disease.

As in Figure 2, except that the semi-quantitative measurements are stratified by age groups (A), or by age group and sex (B). Data points represent individual participants (grey), females (orange) and males (black) and overlayed boxes represent median and interquarile range (IQR). p-value in red refers to the overall age effect (Kruskal–Wallis test) for each assay. Pairwise comparison of age groups used Mann-Whitney statistics with correction for multiple testing. Compared groups are identified by different letters if pairwise p-value <0.05 (blue print).
Finally, and as reported by others [4, 5], analysis of participants previously exposed to SARS-CoV-2 confirmed the 1st vaccination dose acts as a boost. The full cohort encompassed 31 participants who tested anti-N positive at d0 and complied with the 3 collections schedules. For these participants, anti-RBD Ig and anti-spike IgG levels reached maximal values by day 21 (Figure 4A and B). This result also serves to validate our methods. Supporting again that IgM and IgA do not significantly participate in vaccine responses, neither IgM or IgA responses at d21 or d42 were significantly boosted in this group of participants.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
A) Shown are semi-quantitative measurement of anti-spike IgG levels at day 0, 21 and 42 for participants identified as anti-SARS-CoV-2 N positive at day 0, prior to BNT162b2 vaccination. Grey data points represent individual participants and overlayed boxes represent median and interquarile range (IQR). B) Listed in the table are number of participants per day, median and IQR. p-value in red refers to overall response across the three collection time points (Kruskal–Wallis test). Pairwise comparison of collection days used Mann-Whitney statistics with correction for multiple testing. Compared groups are identified by different letters if pairwise p-value <0.05 (blue print).
This study reveals striking inter-individual variation in the amplitude and nature of the humoral response at day 21 post 1st vaccinal dose, explained only in part by age and gender, which should be taken in account when considering extending the time between first and second administration of BNT162b2 mRNA COVID-19 vaccine.
Material and Methods
Recruitment and enrolment: This study was approved by the Ethics committee of the Centro Hospitalar Lisboa Ocidental in compliance with the Declaration of Helsinki and follows international and national guidelines for health data protection. All participants provided informed consent to take part in the study.
Blood samples processing and storage: Venous blood was collected by standard phlebotomy. Blood collection occurred at the day of the first vaccination (baseline, d0), the day of the second vaccination (d21) and 3 weeks later (day 42). Serum was prepared using standard methodology.
Immunoassays: Electro-chemiluminescence immunoassay (ECLIA) was used to quantify Ig anti-N (Elecsys® Anti-SARS-CoV2 N, Roche) and anti-RBD (Elecsys®Anti-SARS-CoV2 S, Roche), ran (on cobas e602) and analysed as per the manufacturer instructions, with a threshold defining positivity at index value = 0.9. Direct ELISA was used to quantify IgG, IgM and IgA anti-full-length spike. The assay was adapted from [10] and semi-automized to measure IgM, IgG and IgA in 384-well format, according to a protocol to be detailed elsewhere. Briefly, coating was 0.5 µg/ml highly purified spike protein [11]; sera were diluted 1/50 in duplicate, 2nd antibodies were horseradish-peroxidase conjugated goat-anti human IgG, IgM, and IgA (Abcam), developed with TMB (BD OptEIA). Optical density (OD) was determined at 450 nm, and normalization of data across plates were derived from 16 controls and calibrators. Assay performance was determined by testing 1000 pre-pandemic sera and 40 COVID19 patients diagnosed at least 10 days prior to sera collection. ROC curve analysis determined a specificity of 99.3%, 99.2%, 99.2%, and a sensitivity of 95.9%, 61.2%, 73.7% for IgG, IgM and IgA, respectively. The threshold defining positivity correspond to normalised OD (ODnorm) =1. Serial titration of 67 COVID-19 patients established the assay has a dynamic range of 3 logs titre.
Statistical analyses: Statistical analyses were carried out using established R scripts. The Kruskal Wallis test was performed to test for differences between strata (kruskal.test). For pairwise group analysis we performed Mann-Whitney U Test (wilcox.test; Benjamini & Hochberg (BH) with p-value adjustment for multiple testing.
Data Availability
Anonymised raw data for Ig levels will be made available on demand. Biometric data will not be shared.
Funding
This work benefited from COVID19 emergency funds 2020 from Fundação Gulbenkian de Ciência and from Camara Municipal de Oeiras.
Acknowledgements
We thank the healthcare workers who participated to the study. We are indebted to Jorge Carneiro for help with ELISA data analysis and Tiago Paixão for guidance in data processing. We are grateful to Joao Costa and Joana Bom for providing training on highly specialised equipment made available for this work. We acknowledge the serology4covid consortium for joined effort during the implementation of a low-scale pilot version of the ELISA assay. We also thank the healthcare professionals involved in sample collection and local testing: Inês Sousa, Catarina Farinha, Susana Vaz, Helena Fernandes, Carla Castro, Catarina Simões, Joana Soares, Nara Silva, Ana Matos, Isabel Barros and Inês Santos. We are most thankful to all the members of the IGC-COVID19 task force for their continuous support. We thank Antonio Coutinho and Thiago Carvalho for critical reading of the manuscript.



