
Abstract
Background Widespread uptake of COVID-19 vaccines will be essential to extinguishing the COVID-19 pandemic. Vaccines have been developed in unprecedented time and hesitancy towards vaccination among the general population is unclear.
Methods Systematic review and meta-analysis of studies using large nationally representative samples (n≥1000) to examine the percentage of the population intending to vaccinate, unsure, or intending to refuse a COVID-19 vaccine when available. Generic inverse meta-analysis and meta-regression were used to pool estimates and examine time trends. PubMed, Scopus and pre-printer servers were searched from January-November, 2020. Registered on PROSPERO (CRD42020223132).
Findings Twenty-eight nationally representative samples (n = 58,656) from 13 countries indicate that as the pandemic has progressed, the percentage of people intending to vaccinate and refuse vaccination have been decreasing and increasing respectively. Pooled data from surveys conducted during June-October suggest that 60% (95% CI: 49% to 69%) intend to vaccinate and 20% (95% CI: 13% to 29%) intend to refuse vaccination, although intentions vary substantially between samples and countries (I2 > 90%). Being female, younger, of lower income or education level and belonging to an ethnic minority group were consistently associated with being less likely to intend to vaccinate. Findings were consistent across higher vs. lower quality studies.
Interpretation Intentions to be vaccinated when a COVID-19 vaccine becomes available have been declining globally and there is an urgent need to address social inequalities in vaccine hesitancy and promote widespread uptake of vaccines as they become available.
Funding N/A
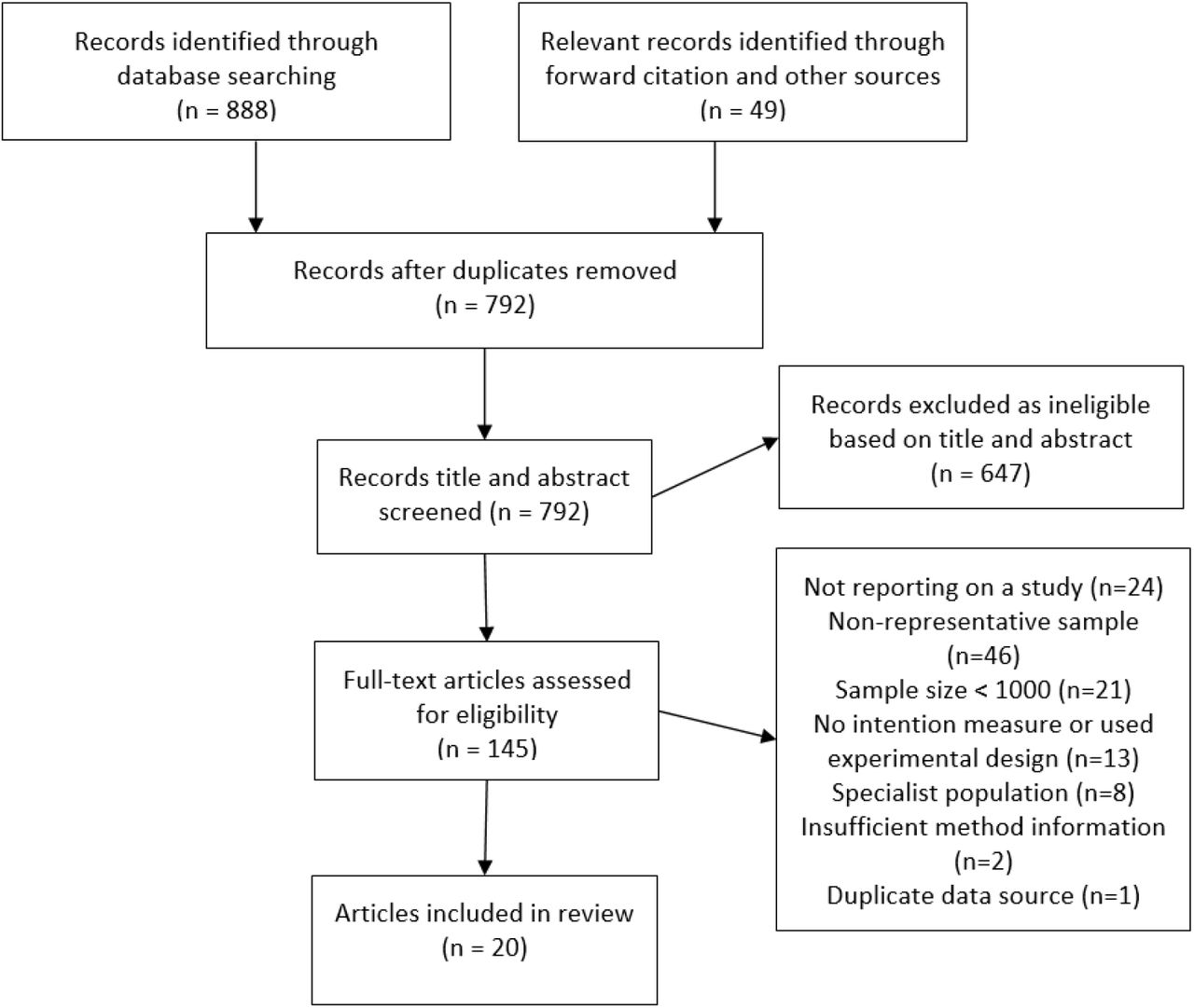
Evidence before this study We searched PubMed, Scopus and pre-print servers for manuscripts from January to November, 2020, reporting on studies examining intentions to be vaccinated against COVID-19 in large nationally representative samples (N≥1000). No language restrictions were applied. Search terms were [(COVID OR coronavirus OR SARS-COV-2) AND (Vaccine OR Vaccination) AND (Inten* OR willing* OR attitud* OR hypothetical)]. From 792 articles, we identified 20 eligible articles reporting on 28 nationally representative samples.
Added value of this study This is the first systematic study and meta-analysis to estimate the proportion of the global population willing to be vaccinated against vs. intending to refuse a vaccine when COVID-19 vaccines become available and how this trend has changed over time, using large and nationally representative samples. Results indicate that COVID-19 vaccination intentions vary substantially across countries, the percentage of the population intending to be vaccinated has declined across countries as the pandemic has progressed (March-May estimate: 79%, June-October estimate: 60%) and a growing number report intending to refuse a vaccine, when available (March-May estimate: 12%, June-October estimate: 20%). There is consistent socio-demographic patterning of vaccination intentions; being female, younger, of lower income or education level and belonging to an ethnic minority group are associated with a reduced likelihood of intending to be vaccinated when a vaccine become available.
Implications of all the available evidence Intentions to vaccinate against COVID-19 among the general public when a vaccine becomes available have been declining and this will limit the effectiveness of COVID-19 vaccination programmes. Findings highlight the need to improve public acceptability, trust and concern over the safety and benefit of COVID-19 vaccines and target vaccine uptake in disadvantaged groups who have already been disproportionately affected by the pandemic.
Introduction
The COVID-19 pandemic has resulted in more than 1 million deaths worldwide from March to October, 20201 and is likely to continue to have far reaching impacts on healthcare systems 2. The development of vaccines against COVID-19 has been occurring at unprecedented speed, and as of November, 2020, there are multiple candidate vaccines in the final stages of testing3. The success of any vaccination programme is dependent on the proportion of the population willing to be vaccinated and based on recent estimates it is likely that up to three quarters of the population may require vaccination to bring an end to the pandemic4,5.
Early in the pandemic a small number of studies surveyed adults to gauge public willingness to be vaccinated against COVID-19 and although a number of studies were reliant on non-representative convenience samples, the majority of the populations sampled intended to vaccinate6-9. For example, a cross country survey found a relatively high average level of intended vaccination (72%), although sample sizes of individual countries were low (N = ∼600-800) and may not provide accurate nationally representative coverage7.
However, as the pandemic has evolved there have been reports of widespread misinformation about COVID-1910, distrust in government11 and public concerns about the safety of COVID-19 vaccines given their rapid development12, all of which may have affected vaccine uptake. It is also unclear whether vaccine acceptability will be socio-demographically patterned. Disadvantaged minority groups have previously been shown to be less likely to intend to be vaccinated for influenza13,14, although a systematic review concluded that other demographic patterning of previous influenza vaccination programmes is inconsistent15. Given that current evidence on socio-demographic patterning of COVID-19 vaccination intentions is lacking, it will be important to understand how vaccination intentions differ within and across countries to inform measures to improve public acceptability and uptake of vaccination programmes.
We conducted a rapid systematic review and meta-analysis of large nationally representative study samples to address the current lack of consensus on; i) the proportion of the population willing to be vaccinated against COVID-19 when a vaccine become available and how this differs across countries, ii) whether vaccination intentions have declined as the pandemic has progressed, iii) socio-demographic inequalities in intended vaccine uptake.
Method
To inform mass COVID-19 vaccination programmes, we used rapid systematic review methodology16. Rapid reviews provide timely evidence synthesises whilst maintaining the rigour of traditional systematic reviews17 using expedited review processes 17,18, such as limiting databases searched or number of reviewers (e.g. cross-checking of a proportion of extraction as opposed to independent extraction by a second author).
Eligibility criteria
We included studies that measured intentions to be vaccinated against coronavirus in nationally representative samples of the general public. Published journal articles and pre-prints were eligible for inclusion. News articles reporting on opinion polls (with no corresponding scientific report including methodology used) were not eligible. The review is registered on PROSPERO (CRD42020223132).
Populations and study design
To be eligible studies were required to have used a sampling approach designed to be nationally representative on key population demographics of the country (e.g. gender, education level), such as quota sampling or random probability sampling. Sampling error is problematic when examining prevalence estimates in small sample sizes19. Because sampling error tends to be minimal at sample sizes of ≥100019, as is considered common practice for nationally representative surveys20, we limited eligibility to studies with a sample of n≥1000 from the same country. Studies that collected non-general public samples (e.g. healthcare professionals, parents, students) were not eligible. Studies that used non-representative sampling (e.g. convenience sampling, snowball sampling) were not eligible and studies that lacked sufficient methodological information to determine sampling used were ineligible.
Interest (measure)
To be eligible studies were required to include a question that measured intentions/willingness to use a vaccine for COVID-19 when one becomes available (e.g. ‘I would use a vaccine for COVID-19 when it becomes available’). Studies that exposed participants to information designed to alter vaccine intentions (e.g. experiments comparing how public health messages may improve vaccine intentions) were not eligible. Studies that compared willingness to take different types of vaccine (e.g. varying hypothetical effectiveness/price) were ineligible, unless they also included a questionnaire item measuring general willingness to take a COVID-19 vaccine.
Outcome
Studies were required to report the proportion of participants responding to the different response options for the vaccine intention question (e.g. Yes vs. No, Willing vs. Unsure Vs. Unwilling, Likely vs. Undecided vs. Unlikely).
Article identification strategy
During November 2020, we searched PUBMED and Scopus (2020 onwards) for published articles in peer reviewed journals. We used the following search terms: (COVID OR coronavirus OR SARS-COV-2) AND (Vaccine OR Vaccination) AND (Inten* OR willing* OR attitud* OR hypothetical). We also searched three pre-print servers; Open Science Framework (which includes 30 other preprint archives, including PsychArxiv), MedrXiv and the Social Science Research Network (SSRN). One author conducted the initial title and abstract screening to exclude unrelated articles and a second author checked 25% of this (there were no discrepancies). A single author conducted full-text screening to determine eligibility and a second author cross-checked all eligibility decisions. For all eligible articles identified through searches, we used forward citation tracking (Google Scholar) and our knowledge of existing research to identify any further articles.
Data extraction
For each study one author extracted information, all extraction was cross-checked by a second author and disagreements were resolved through discussion. We extracted the following information; bibliographic information, country, sampling procedure (e.g. quota vs. probability), sample size, month of survey, measure of vaccination intentions and results. We extracted results based on response options, resulting in % choosing response options indicative of definitely or probably yes, % definitive or probable no, % unsure (if measure allowed for the latter). If studies had multiple waves of data collection, we extracted results from the most recent wave. We also extracted information on whether studies reported results of analyses examining demographic predictors of vaccination intentions that were commonly examined (i.e. at least 5 studies) in studies. To be eligible for extraction, demographic predictors were required to be examined adjusting for other demographics (i.e. zero-order correlations were not eligible) in order to be confident of independent effects. We prioritised extraction of results of analyses that examined vaccine intentions (i.e. reference of category of yes vs. other (unsure/no combined). If this analysis was not available, in order of priority we favoured extracting demographic results for analyses examining yes vs. no, then yes vs. unsure.
Risk of bias indicators
We considered quota-based samples as being higher in risk of bias than probability-based sampling, as the latter tends to be a more accurate/representative sampling approach21,22. We also reasoned that studies not having yet undergone formal peer review (pre-prints) may increase risk of bias and coded for this. We reasoned that studies that did not use an ‘unsure’ or ‘undecided’ response option (e.g. responses grouped into yes vs. no, as opposed to yes vs. unsure vs. no) may affect vaccine acceptance and rejection estimates, so we examined if pooled estimates of intended vaccination and intended refusal differed between these two types of study. For studies examining demographic predictors, we considered relatively smaller sample sizes (n<2500) as higher in risk of bias due to concerns over small numbers of cases in analyses when examining sub-groups. For example, with n ≥ 2500, for minority sub-groups (e.g. ∼2% of the population, such as Black people in the UK) there would be expected to be a minimum of 50 cases in analyses, as opposed to only 20 cases with n=1000. Studies of demographic predictors that adjusted for attitudinal predictors (e.g. attitudes towards vaccination) of vaccine intentions were considered higher in risk of bias, as inclusion may mask associations between demographics and vaccination intentions.
Synthesis of evidence
We meta-analysed proportions of the samples ((Total sample N / 100) * % reporting) reporting: i) intending to vaccinate, ii) unsure, and iii) not intending to vaccinate. Analysis was performed using the ‘metafor’ package in R. We used a logit transformation on raw proportions in random effects, generic inverse variance meta-analyses with a restricted maximum-likelihood estimator. Transformations were conducted using the ‘escalc’ function in the metafor package. Back-transformed (inverse) logit values are presented in the text, whilst raw proportion data is presented in forest and funnel plots to aid interpretation. Heterogeneity was assessed with the I2 statistic. We conducted meta-regressions to examine the relationship between outcomes and month of study data collection (treating month as a continuous variable, e.g. March = 1, April = 2). We conducted leave-one-out analysis to examine the stability of the pooled estimates and identify any influential samples in the main analyses and meta-regressions. We conducted sub-group analyses to examine whether results differed between studies using quota vs. probability sampling and pre-prints vs. journal articles. We limited these analyses to studies which collected data early in the pandemic (March-May) to account for the majority of probability samples (3/4) and journal article sample (12/12) studies being conducted in this period. Sub-group analysis compared studies that did vs. did not allow for an ‘unsure’ response option. We also examined potential publication bias and small study effects (see online supplementary materials). Demographic predictors were measured and/or analysed differently across studies, so for each demographic we reported the proportion of studies finding evidence vs. no evidence of significant (p < .05) relationships with vaccination intentions, and whether results were similar when limited to studies that had larger sample sizes and did not adjust for attitudinal predictors in analyses.
Results
Study selection
A total of 792 unique articles were found through database searches and other sources. Of the 145 articles full-text screened, 20 articles reporting on 28 samples were eligible for inclusion. See Figure 1. For bibliographic information of all included articles, see online supplementary material.
Overview
Of the 28 samples included, the majority were from the UK and North America (7=US, 2=Canada, 7=UK) as well as samples from France (n=3), Australia, China, Denmark, Germany, Italy, Ireland Netherlands, Poland and Portugal. Full study information is reported in Table 1. Sample sizes ranged from 1,000 to 7,547 (median = 1198). Samples were collected in the early phases of the pandemic (March-May, n = 18) and later (June onwards, n = 10). Twenty-four samples used quota-based sampling and four used probability sampling, 12 articles were in peer-reviewed journals and 16 were pre-prints (at the time of identification).
Study and sample information of eligible articles included in review
Intentions to vaccinate (Figures S1-S3)
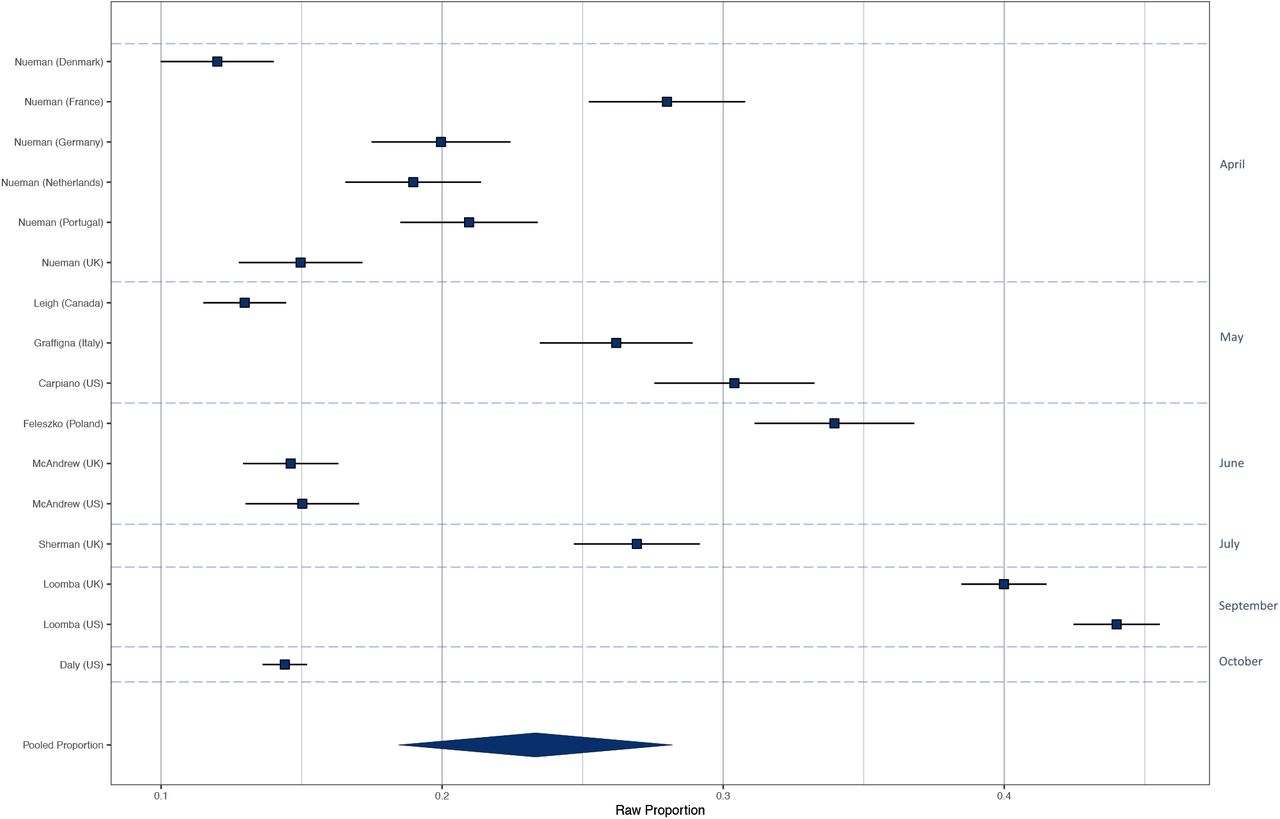
Including all 28 samples collected from March-October, the pooled proportion reporting intending to vaccinate was .729 [n = 28, 95% CI: .666 to .784: I2 = 99.6%], the proportion reporting they would refuse a vaccine was .143 [n = 28 95% CI: .114 to .178: I2 = 99.3%] and the proportion reporting being unsure was .221 [n = 16, 95% CI: .178 to .271: I2 = 99.0%]. Values do not equal 100 as not all studies included an unsure response option. See supplementary materials document for results in full and Figure 2 for proportion of populations intending to vaccinate by country and month.

Presence vs. absence of ‘unsure’ response option in survey
There was a significant difference in the proportion intending to vaccinate when an ‘unsure’ response option was used vs. when there was no ‘unsure’ response option (X2(1) = 16.82, p < .001). When there was no unsure response option the proportion was .828 [95% CI: .759 to .880: I2 = 99.4%], and when unsure was a response option the proportion was .635 [95% CI: .569 to .670: I2 = 99.2%]. There was not a significant difference in the proportion intending to refuse a vaccine between samples with [.124, 95% CI: .092 to .163: I2 = 99.0%] vs. without [.172 [95% CI: .120 to .240: I2 = 99.4%] ‘unsure’ response options (X2(1) = 2.12, p = .146).
Time trends
See Figures 2-4. There was a significant association between proportion of individuals intending to vaccinate and month study was conducted (coefficient = -.24 [95% CI: - .37 to .11], z = 3.55, p < .001) and also a significant association between intentions not to vaccinate and month of study (coefficient = .15 [95% CI: .03 to .28], z = 2.36, p = .018). Over time intentions to vaccinate decreased, and intentions not to vaccinate increased. For example, in studies (n = 18) that collected data during the early phase of the pandemic (March-May), the proportion intending to vaccinate was 79% and not intending to was 12%, compared with 60% and 20% June-October studies (n = 10). There was no association between proportion of individuals being unsure about vaccination and when the study was conducted (coefficient = .10 [95% CI: -.03 to .24], z = 1.54, p =.124]. Because samples varied by country, to confirm time trend findings were not explained by different countries being sampled earlier vs. later in the pandemic, we replicated the meta-regressions for the two countries with multiple samples collected during different months. Among UK samples (n = 7, coefficient = -.39 [95% CI: -.57 to -.21], z = 4.34, p < .001) and US samples (n = 7, coefficient = -.22 [95% CI: -.38 to -.05], z = 2.53, p = .014)] the same negative associations were observed as in the main analyses.
There was minimal evidence of publication bias and leave out one analyses indicated limited variation in estimates (online supplementary materials document). We found no evidence that results differed between samples reported in journal articles vs. pre-prints. There was minimal evidence of differences in findings between studies using probability vs. quota sampling, with the exception of ‘unsure’ responses being lower in quota samples (see online supplementary materials).
Demographic predictors
Fourteen studies examined demographic predictors. See Table 2. In 12/14 studies older adults were significantly more likely to report intending to vaccinate than younger, one study found no effect of age and in one study young adults (<25 years) were more likely than middle aged adults, but not older adults. In 9/14 studies males were more likely to intend to vaccinate than females (no significant association in five studies). Higher education level was associated with intending to vaccinate in 7/14 studies (no association in seven). White ethnic groups were more likely to vaccinate in 7/11 studies (no association in four). Higher income was associated with intending to vaccinate in 8/9 studies and in one study there was no association. Presence of a health condition was examined in five studies and was non-significant in n=4 and not having a health condition was associated with intending to be vaccinated in one study. When analyses were limited to the five higher quality studies the role of demographic factors was more consistent; 5/5 studies found that older adults, males and higher education levels were associated with increased likelihood of intending to vaccinate. Similarly, 3/4 studies found that being white and 4/4 found that those on higher income were more likely to intend to vaccinate. Presence of a health condition was non-significant in n=2.
Discussion
Results of this systematic review and meta-analysis of 58,656 participants drawn from 28 large nationally representative study samples across 13 countries indicates that the percentage of the population intending to be vaccinated when a COVID-19 vaccine becomes available has declined markedly across countries as the pandemic has progressed. Numbers reporting that they will refuse a vaccine have increased over time and a substantial proportion of adults now intend to refuse a vaccine, when available (June-October estimate = 20%). There is also consistent socio-demographic patterning of vaccination intentions; being female, younger, of lower income or education level and belonging to an ethnic minority group are associated with a reduced likelihood of intending to be vaccinated when a vaccine become available.
Emerging evidence suggests that both exposure to misinformation about COVID-19 10,23 and public concerns over the safety of vaccines24 may be contributing to the observed declines in intentions to be vaccinated, and this highlights the need for measures to address public acceptability, trust and concern over the safety and benefit of approved vaccines. As well as observing declines in intentions to vaccinate over time in our main analyses, we also note intentions differed markedly by country. When sampled during a similar period early on in the pandemic (March-April), 91% of adults in China reported intending to be vaccinated, compared to 76% of adults in France. However, the most recent estimate (September-October) in France is now 52% and similar to the US (54%).
Across studies there was very consistent socioeconomic patterning of vaccination intentions: lower income or education and ethnic minorities were less likely to intend to vaccinate. There was no evidence in any studies reviewed that presence of a chronic health condition was associated with increased vaccination intentions, even though these groups are at increased risk of dying from COVID-1925. Measures are required to maximise vaccine uptake in vulnerable and disadvantaged groups who have already been disproportionately affected by the pandemic, such as those from lower income and ethnic minority groups25,26. Strengths of the present research are that we limited evidence synthesis to study designs that allow for accurate estimates of population level intentions with minimal sampling error, as small studies of non-representative samples are likely to provide biased estimates. We found no evidence that the type of sampling method used had a meaningful impact on estimates and that studies reported in pre-prints produced similar effect estimates as peer-reviewed journals. Analyses also accounted for studies using different response formats and findings were similar.
We found evidence of declining vaccination intentions when data was analysed using meta-regression (continuous month-of-year variable), when comparing study estimates from early in the pandemic (March-May) to later (June-October) and when examining time trends within countries (UK, US). Two included individual studies (US, France) also reported vaccination intentions over time in the same population and results were consistent24,27. As included studies examined nationally representative samples we do not know whether a similar pattern of results would be expected among other population groups (e.g. healthcare workers) and research is required to address these questions28,29. Findings of the present research are limited to studies that met eligibility criteria for having used large and nationally representative sampling and this tended to be developed western countries.
Conclusions
Intentions to vaccinate when a COVID-19 vaccine becomes available have been declining globally and there is an urgent need to address social inequalities in vaccine hesitancy and promote widespread uptake of vaccines as they become available.
Data sharing
Study data files and analysis code are openly available on the Open Science Framework; https://osf.io/hj4ds/
Data Availability
Study data files and analysis code are openly available on the Open Science Framework; https://osf.io/hj4ds/
Contributors
The study was designed by ER. Data was collected by ER, AJ, IL and MD. AJ and ER analysed the data. The first draft was written by ER. All authors critically revised the manuscript and agree to be accountable for all aspects of the work.
Role of the funding source
There was no funding source for this study.
Declaration of interests
All authors report no conflicts of interest. ER has previously received funding from the American Beverage Association and Unilever for projects unrelated to the present research.
Figure headings



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Acknowledgments
ER’s time was part-funded by the European Research Council and their support is gratefully acknowledged.
References




