
ABSTRACT
Background The transition to air-breathing at birth is a seminal, but poorly understood, respiratory event common to all humans. The objectives of this prospective, observational study were to describe the spatiotemporal gas flow, aeration and ventilation patterns occurring within the lung in neonates during successful respiratory transition.
Methods Electrical impedance tomography was used to image intrathoracic volume patterns for every breath until six minutes from birth in term infants not needing resuscitation. Breaths were classified by video data, and measures of lung aeration, tidal flow conditions and intrathoracic volume distribution calculated for each inflation.
Findings 1401 breaths (n=17 neonates) met eligibility and data analysis criteria. Stable functional residual capacity was obtained by median (IQR) 43 (21, 77) breaths. Breathing patterns changed from predominantly crying (80.9% first minute) to tidal breathing (65.3% sixth minute). Tidal ventilation was inhomogeneous at birth, favouring the right and non-dependent lung; p<0.001 versus left and dependent lung (mixed effects model). Initial crying created a unique pattern with delayed mid-expiratory gas flow associated with intrathoracic volume redistribution (pendelluft flow) within the lung. This preserved functional residual capacity (70.8% cries), especially within the dorsal and right lung.
Interpretation The commencement of air-breathing at birth generates unique flow and volume states associated with marked spatiotemporal ventilation inhomogeneity not seen elsewhere in respiratory physiology. At birth neonates innately brake expiratory flow to defend functional residual capacity gains and redistribute gas to less aerated regions.
Funding National Health and Medical Research Council (Australia).
Evidence before this study Birth requires the rapid transition from a fluid-filled to aerated lung. Despite being a seminal event for all humans, very little is understood about the physiological processes supporting the transition to air-breathing. Radiological and interventional studies from more than 40 years ago suggest that respiratory success at birth requires high intrathoracic pressure and flow states. Imaging studies in animals indicate that braking expiratory flow aids generating functional residual capacity.
Added value of this study In term neonates during successful respiratory transition, breath-by-breath imaging of the intrathoracic gas flow and volume patterns within the lungs was possible with electrical impedance tomography. We found that aeration and ventilation were not uniform, with highly inhomogeneous, spatiotemporal volume patterns during attainment of functional residual capacity. Crying at birth created a unique expiratory pattern that allowed intrathoracic volume redistribution (pendelluft flow) within the lung, and preserved functional residual capacity. We hypothesise that newborns defend aeration from intrathoracic lung-fluid shifts by innately braking flow using the glottis and diaphragm.
Implications of all the available evidence Real-time imaging of intrathoracic volume patterns in humans is practical and may offer measures that identify neonates needing resuscitation. Whilst inspiration generated aeration, expiration is equally important to the respiratory transition. Expiratory braking is essential as a mechanism of defending aeration; suggesting that positive end-expiratory pressure is likely to be the most important method of supporting the failing human lung at birth.
INTRODUCTION
The rapid adaptation to air-breathing at birth (aeration) is one of the most important, but least understood, physiological events in humans. Much of our understanding is inferred from preclinical studies 1-4 or invasive observational studies.5-7 These studies suggest that creating a functional residual capacity (FRC) during the initial process of lung aeration requires first clearing the airways of fetal lung liquid using high intra-thoracic pressure gradients.1,2,5 Subsequent tidal ventilation must prevent influx of fluid back into the alveoli during expiration.1 Animal studies have demonstrated that these processes exhibit a high degree of spatiotemporal variability within the lung.2,8 For most newborns, fluid clearance and the transition from placenta to lung as the organ of gas exchange is achieved through the spontaneous onset of breathing. When this process fails, especially in preterm infants, death or significant morbidity may result. Due to an inability to define the process of aeration and ventilation at birth, effective evidence-based interventions to support breathing after birth are lacking.9
The development of effective interventions in the delivery room first requires an understanding of the physiological processes defining success or failure of aeration at birth. Adapting physiological concepts from preclinical studies have limited utility as instrumentation restricts the ability to emulate respiratory mechanics and the neurological state of the breathing human infant.1-3,10 The delivery room further creates a challenging research environment, the time critical and dynamic nature of birth itself hampers physiological measurements.11 Lung volume changes at birth have been intermittently imaged using chest radiography12 and ultrasound13, and pressure and flow patterns measured invasively within the pharynx or by imposing a face-mask.5,14 These studies identified unique breath types associated with high intra-thoracic driving pressure gradients during successful respiratory transition in term infants, specifically crying and grunting.5,15,16 Importantly, these studies failed to directly define the fundamental dynamic spatiotemporal processes of aeration and subsequent ventilation within the lung.
To address this gap in knowledge, we used electrical impedance tomography (EIT), an emerging radiation-free imaging modality in critical care medicine.17 EIT uses the differential electrical properties of aerated and fluid-containing tissue to measure the tidal and end-expiratory volume changes in lung regions within a transverse chest slice.17 We adapted our EIT techniques for measuring the respiratory transition in preclinical studies.2-4,10 This allowed non-invasive, and non-hazardous, direct imaging of the dynamic breath-to-breath regional process of aeration at birth in human infants without interfering with normal physiology or clinical care. The objective of this study was to describe the spatiotemporal respiratory patterns associated with the successful transition to air-breathing after birth in term infants. The specific aims were to 1) characterise the inspiratory and expiratory time and flow characteristics within the lung at birth, and 2) describe the resultant spatiotemporal ventilation and volume patterns by breath type and time.
METHODS
A detailed methodology can be found in the online supplement. This prospective observational study was conducted at the Royal Women’s Hospital, Melbourne, Australia.
Infants were eligible for enrolment if they were delivered by elective caesarean section for non-fetal reasons at ≥36+0 weeks post-menstrual age, and written prospective parental consent obtained. Infants were not included if placement of an EIT belt would interfere with clinical care,18,19 or the fetus was known to have a congenital condition that could alter EIT interpretability Infants who received resuscitative interventions were excluded from analysis.
Measurements
Heart rate and peripheral oxygen saturation (SpO2) were measured with a Radical 7 pulse oximeter (Massimo Corporation, Irvine CA). Regional lung volume changes were imaged at 48 frames per second with the Pioneer EIT system using an ultrasound gel coated 33 cm NeoSensor Belt (Sentec AG, Landquart, Switzerland).2,10,18-20 Audio and video were recorded at 30 frames per second with a high-definition webcam (Logitech, Lausanne, Switzerland).
Delivery room protocol
As the infant was being placed supine on the resuscitaire the NeoSensor Belt was secured (Velcro tab) around the chest at nipple level (Supplementary Video 1). The pulse oximetry sensor was applied to the right hand. There was no other interference with routine clinical care. Infants were managed in a supine position in accordance with local guidelines, including timing of umbilical cord clamping. Data were only recorded during care on the resuscitaire.
Data acquisition and analysis
EIT, video, audio and pulse oximetry data were continuously recorded digitally during resuscitaire management, and timing of critical events from birth documented. SpO2 and heart rate data were reviewed for loss of signal or movement artefact. EIT data were recorded in a custom-built infant imaging package,21 and images reconstructed post hoc17,22 using the vendor-provided human model chest atlas, with non-lung regions excluded.19 Each potential tidal volume (VT) change due to breathing was identified from the global lung signal. Analysis of the EIT change associated with a breath was only performed if there was 1) video confirmation of a breath; and 2) no movement interference on the video. All included breaths were classified by the presence of a cry, grunt or no breathing noise (tidal breath) in the audio. If audio classification was not possible the breath was excluded (Supplementary Figure 1).
For included breaths, the pre and post-breath FRC, inspiratory time (Ti), expiratory time (Te), time constant of the respiratory cycle (τ) and relative peak inspiratory (PIF) and expiratory flow (PEF) were calculated for the global signal and right, left, ventral and dorsal lung regions.17 The shape of the impedance change during each breath was classified by an investigator (DGT) unaware of the breath type or time from birth. The centre of ventilation along the ventrodorsal (CoVVD) and right-left (CoVRL) planes were calculated to determine spatiotemporal distribution of VT within the chest slice.17,23 The percentage of the global VT signal was calculated for the most dependent, central and non-dependent thirds of the right and left lung, and the percentage and location of lung regions without any VT signal.17,20
Sample size and statistical analysis
Based on a previous study of respiratory parameters at birth 14, a convenience sample of thirty infants was estimated to provide data for breath-by-breath classification. and analysis of 100-150 breaths/infant per 5-6 minute period in 15-20 infants. Continuous data were analysed with a mixed-effects linear regression model, with robust standard error and cluster analysis to adjust for multiple breaths from each infant. A p value <0.05 was considered statistically significant.
RESULTS
A visual abstract of the main study findings is available in Supplementary Video 2.
Study population
Thirty-three families were approached on the day of the delivery, with three declining to participate. Two studied infants received resuscitative support after birth and were excluded. Of the remaining 28 infants, EIT data were obtained in 27 infants (EIT belt incorrectly placed). Complete audio or video data were not acquired in ten infants (technical failure in delivery room, staff obstructing camera, excessive background noise or inability to delineate any audio/video breaths). The characteristics of the final 17 infants with matched EIT, video and audio data are described in Supplemental Table 1. All were singleton pregnancies and no mother received antenatal corticosteroids.
Pulse oximetry
A pulse oximetry signal could be acquired in 15 infants, with a median (range) of 17 (3, 198)s to apply the probe and acquire a signal. The first SpO2 signal was acquired at 52 (12, 97)s, but then lost for >10s at least once in ten infants. SpO2 increased with time from 53 (48, 72)% at 60s to 78 (60, 96)% by 360s (p=0.029; mixed-effects model, Supplementary Figure 2). Heart rate was stable throughout the study period (p=0.25).
Time to image acquisition
The median (range) time from birth to first EIT image was 36 (20, 62)s, with the longest periods being in the two infants born with delayed cord clamping (60 and 62s). The time between cutting of umbilical cord and first EIT image was 31 (20, 48)s. In all infants the time between applying the EIT belt and first images was <12 s, with no subsequent signal loss.
Breathing patterns
A total of 1401 inflations met the inclusion criteria (Table 1). Only 14 breaths (1%) had audible grunting (all during periods of crying), and were included with the crying breaths (787 breaths). Crying was more prominent early in the respiratory transition, representing 80.9% of all inflations within the first minute, then decreasing to 34.7% by the sixth minute (p<0.0001; chi-squared test for trend). Breaths could be classified as following two distinct EIT volume patterns; 1) linear inspiratory and expiratory volume change consistent with tidal ventilation of already-aerated lungs, or 2) an expiratory phase with a distinct bifid expiratory wave and a transient increase or preservation in lung volume (Figure 1 and Supplementary Video 2). During these bifid waves there was a subtle redistribution of ventilation seen on fEIT images. 70.8% of all crying breaths had a bifid wave, but only 2.5% of tidal breaths.
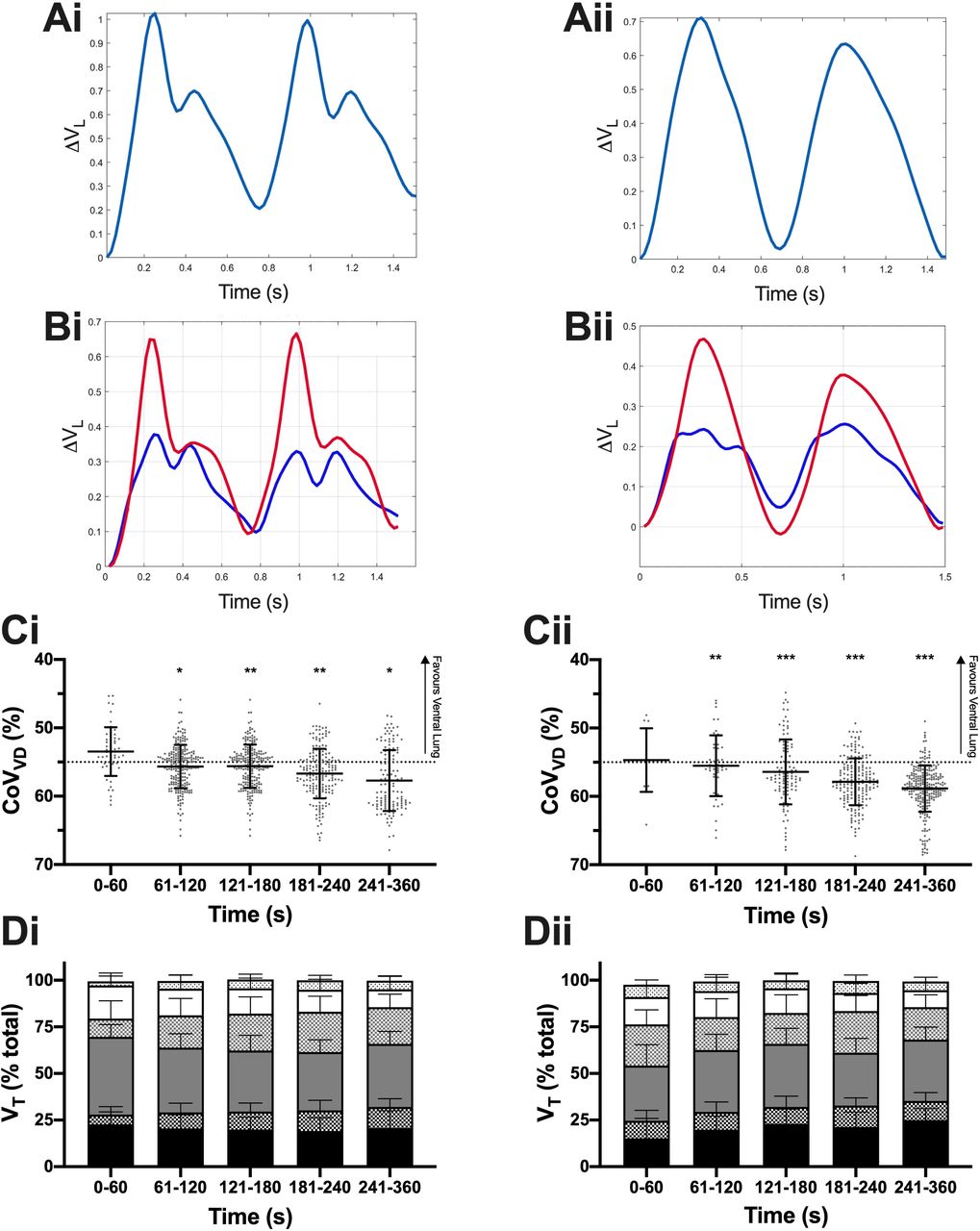
A. Relative Volume change (ΔVL) over time within the whole lung during the two representative breaths for crying (i; 25 s) and tidal breaths (ii; 5 min). B. ΔVL during the same breaths within the ventral (blue) and dorsal (red) hemithoraces. C. Ventrodorsal centre of ventilation (CoVVD) by minute after birth for crying and tidal breaths. CoVVD of 55% represents uniform ventilation, with values <55% indicating relatively greater ventilation in the ventral lung and >55% the dorsal lung. Grey dots represent individual breath data, and black line and bars mean±SD. C. Relative distribution of ventilation (% total VT) along the gravity dependent plane for crying and tidal breaths in the most gravity dependent third of the lung (black bars), central third (grey bars) and non-gravity dependent third (white bars), with solid bars being right lung region and dotted bars left lung. All data mean+SD. *p<0.05, **p<0.01, ***p<0.0001 against first 60s (mixed-effects model).
Ti increased over the first minutes of life for both breath types; p<0.0001, mixed-effects model (Figure 2A). Ti was quicker during crying than tidal breaths in the first 60s, being a mean (95% CI) 101 (56, 147) ms shorter, and then also from 180s (p<0.0001). In contrast, Te and τ were longer during crying than tidal breaths (both p<0.0001). Te and τ did not change significantly with time for crying or tidal breaths, but Te was longer during crying between 61 and 180s (maximum difference 169 (112, 227) ms, and τ longer, and more variable during crying after 240s, difference 99 (46, 152) ms (Figure 2B and C).

Ti (A), Te (B), respiratory system time constant (τ; C), PIF (D) and PEF (E). Black circles indicate crying breaths and white diamonds tidal breaths. All data mean±SD. *p<0.05, **p<0.01, ***p<0.0001 cry vs tidal inflation; †p<0.01 within breath type (all mixed-effects model).
PIF increased with time for tidal breaths (p<0.0001, mixed-effects model; Figure 2D). However, during crying PIF was only different after 240s, being a mean (95% CI) 1.6 (0.7, 2.4) AU/s lower compared to 181-240s. PIF was greater at all time epochs during crying compared to tidal breaths (all p<0.0001). PEF increased with time during tidal breaths (p<0.0001; Figure 2E), being 1.3 (0.8, 1.8) AU/s faster after 240s compared to the first 60s. There was no change in PEF over time during crying. PEF was greater during crying for the first 180s compared to tidal breaths (all p<0.0001), with the greatest difference in the first 60s (1.4 (0.9, 1.8) AU/s).
The detailed spatiotemporal behaviour of Ti, Te, τ, PIF and PEF in the right, left, ventral and dorsal lungs are provided in the supplemental results (Supplemental Figures 3-7). Overall, Ti, Te and τ were similar within all lung regions for both breath types. Crying resulted in faster PIF and PEF in the dorsal and right lung compared to ventral and left respectively. Tidal breaths resulted in less right-left and ventral-dorsal differences in PIF and PEF than crying.
Functional residual capacity
Overall relative FRC increased with each breath from birth (Figure 3 and Supplemental Figure 8). FRC was quickly established after birth, with the maximum recorded FRC value for each infant occurring at a median (IQR) 43 (21, 77) of included breaths after birth. Maximal FRC occured at 67.8 (51.9, 94.5)% of the analysed sequential breaths for each infant, being the last recorded breath in only two infants. During an infant’s first 100 breaths (or total if <100), 48% of FRC change occurred within the first 5 breaths.

A. Change (Δ) in FRC from first measured inflation for all breaths (A) and for the first 100 inflations (maximum)(B). ΔFRC normalised to the FRC before the first breath (0%) and maximum FRC (100%) for each infant. A. Blue line represents line of best fit (dashed lines 95% CI) using a one-phase exponential association; y=yplateau.[1-ex.τ-1]; plateau (95% CI) 56.2 (54.0, 58.6)%, τ 8.0 (6.0, 10.5) inflations (R2 0.14, RSME 24.5%, replicates test discrepancy (F) 0.82 [p=0.96]). Grey dashed lines demonstrate ΔFRC at 50% of FRCmax and 50 inflations. B. Black circles represent the mean ΔFRC every 5 inflations for each infant, and dashed lines 95% CI.
Regional ventilation patterns
Ventilation redistributed towards the dorsal lung with time for both crying and tidal breaths (Figure 1); CoVVD p=0.045 and p<0.0001 respectively (mixed-effects model). Overall, CoVVD favoured the ventral lung during crying compared to tidal breaths by a mean (95% CI) 1.6 (0.3, 2.9)%, although the differences were not significant within each minute. The redistribution of VT towards the dorsal lung was predominantly due to increased VT within the central lung regions during crying, and the dorsal region during tidal breaths (p=0.0004), both at the expense of ventral lung VT.
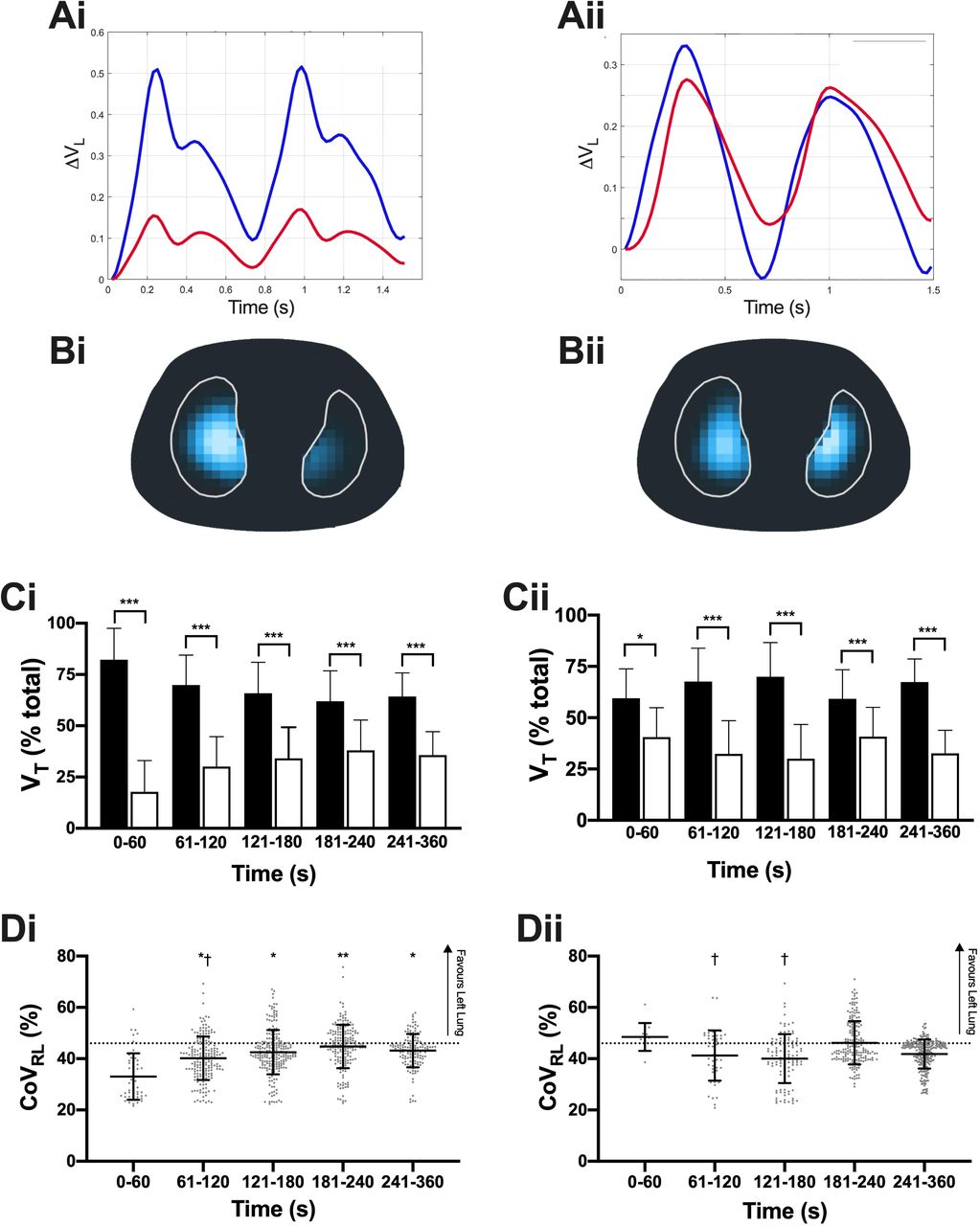
Both breath types resulted in greater ventilation in the right lung (Figure 4). In the first 60s a mean (SD) 82.2 (15.3)% of total VT occurring in the right lung during crying, with a resultant CoVRL of 33.0 (9.1)% (ideal 46%). Ventilation increased in the left lung with time (p=0.011, mixed effects model); with 64.3 (11.4)% of VT in the right lung, and CoVRL 43.1 (6.5)% from 240s. Right-left lung VT did not change over time for tidal breaths (p=0.10). In the first minute 59.5 (14.3)% of VT was in the right lung, and CoVRL 46.4 (9.3)%. Crying resulted in greater right-left lung inhomogeneity, with CoVRL being a mean (95% CI) 2.0 (0.5, 3.5)% less overall than tidal breaths, and greatest in the first minute (difference 13.4 (6.7, 20.1)%).
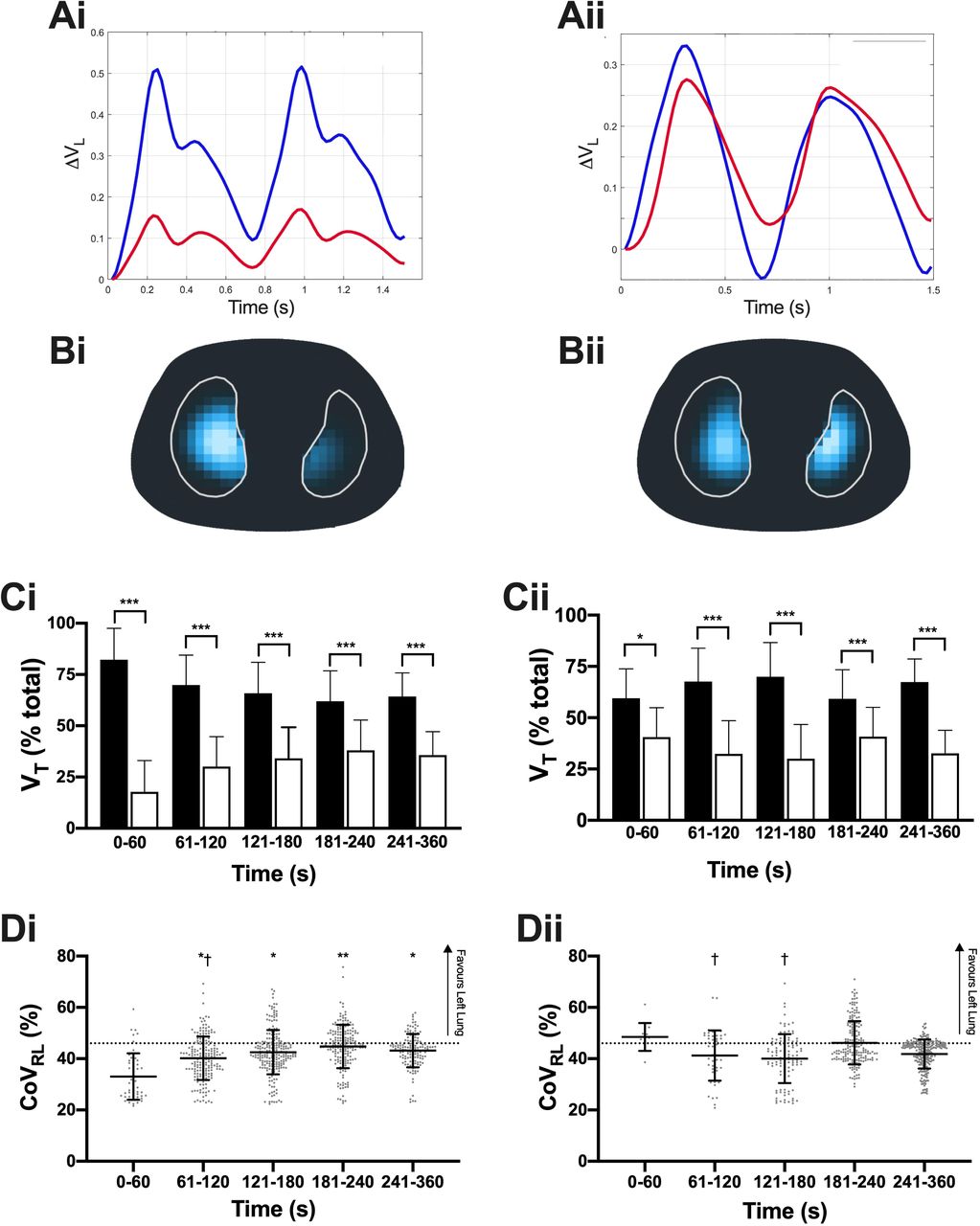
A. Relative Volume change (ΔVL) over time within the right (blue) and left (red) lung during the two representative breaths for crying (i; 25 s) and tidal breaths (ii; 5 min). B. Functional EIT images of volume change within the lungs for the same breaths using the colour scale defined in Supplementary Video 2. C. Relative distribution of ventilation (% total VT) in the right (black bars) and left (white bars) lung for crying and tidal breaths. D. Centre of ventilation (CoVRL) along the right-left plane for all inflations by minute after birth for crying and tidal breaths. CoVRL of 46% represents uniform ventilation, with values <46% indicating relatively greater ventilation in the right lung, and >46% greater ventilation in the left lung. All data mean±SD, and dots individual breath data. Panel A and C; *p<0.05, ***p<0.0001 (mixed-effects model). Panel B and D; *p<0.05, **p<0.01 against first 60s. † p<0.05 against 181-240s.
Approximately 10% of predefined lung regions were unventilated for both tidal and crying breaths, with not difference in the ventrodorsal pattern of unventilated regions (Supplementary Figure 9). After 240s there was less unventilated lung regions, especially during tidal breathing, suggesting increasing aeration resulted in greater engagement of the distal lung in ventilation.
DISCUSSION
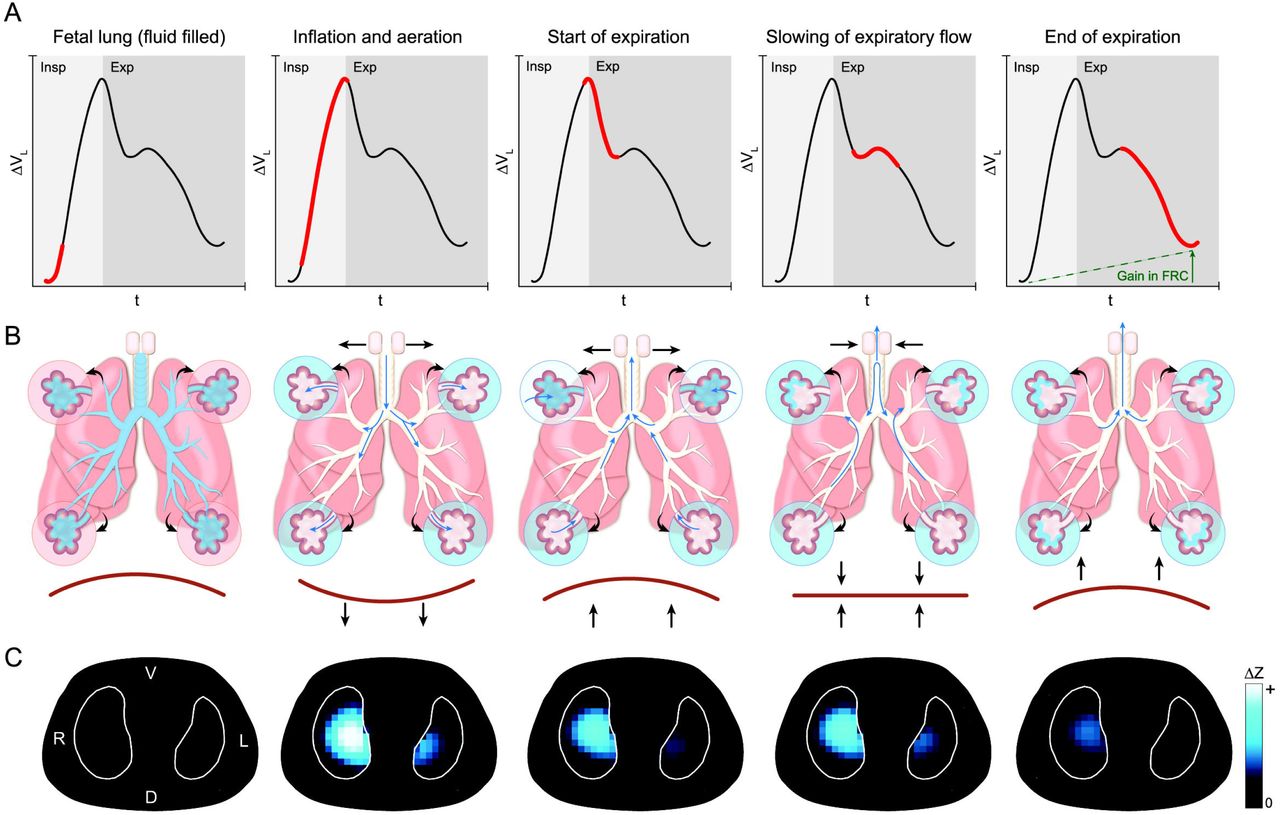
The transition to air-breathing at birth is a seminal physiological event essential to life in all humans. In our observational study we provide the first detailed description of the volumetric processes within the lung during this process. We found that the transition to air-breathing is characterised by complex spatiotemporal patterns of aeration and ventilation initially mediated by high PIF rates and prolonged expiration. Overall this results in rapid lung aeration that moves from the central to distal lung, with the right lung engaging in ventilation earlier than the left. Crying is the dominant breathing pattern at birth, creating greater PIF and complex expiratory volume patterns more suited to both rapid aeration and maintenance of FRC than tidal breathing at a time the lung is still likely to be partially fluid-filled. That these findings occurred in healthy term infants without instrumentation or active intervention is important, providing the first human evidence that successful aeration at birth is dependent on actively engaging in expiratory mechanisms to protect FRC (Figure 5).

Representative global lung volume change during a single cry at 14 s after birth (Infant 6; Panel A) demonstrating the dynamic volume change during inspiration and expiration, and resultant increase in end-expiratory FRC. The breath has been divided into five phases related to the mechanistic events identified during the respiratory transition from a fluid-filled to aerated lung (Panel B), and the respective fEIT images for each shown in Panel C. At the start of the inflation the airways and alveoli are fluid filled (#1). A cry initiates a rapid and large contraction of the diaphragm with a resultant rapid inspiratory flow (slope of the time-volume curve) and high inflating (driving) pressure within the lung generating aeration by moving fluid from the proximal airways to the alveoli (enlarged) and then the lung interstitium (#2). Expiration begins with rapid contraction of the diaphragm (#3). The fall in intra-thoracic pressure during expiration lowers intra-alveolar pressure, and in some lung units this fall allows fetal fluid to influx back into the alveoli spaces. To counteract this effect the neonate slows (brakes) diaphragmatic contraction and partially closes the glottis, thus transiently re-pressurising the lung and allowing pendulluft gas flow between aerated to poorly aerated lung units (#4). When expiration continues it does so against a partially closed glottis which mediates slower expiratory gas flow and allows some gas to remain in the lungs, thus generating a greater end-expiration FRC (#5) and more favourable lung conditions at the start of the next inflation.
Clearing the respiratory system of fetal lung liquid, and establishing aeration is essential to physiological success at birth. The first few inflations at birth rapidly achieved the majority of lung aeration, similar to chest radiography studies during the first seconds after birth in term infants.6,7 Unlike these studies we were able to continuously follow the process of aeration beyond these first inflations. Although there was considerable inter-subject variability, aeration conformed with an exponential pattern reported in preclinical studies,3,4 and during lung recruitment in the already-aerated lung.24 Aeration was also associated with a temporal increase in distal lung ventilation. Our study is the first in humans to confirm the sequential central-distal movement of the air-fluid interface during aeration from the major airways to the distal alveoli reported in animal studies is ongoing beyond the first few breaths.1,8 Due to the markedly different electrical properties of air and fluid, EIT is ideally suited to mapping the air-fluid interface and tracking lung aeration clinically.
The patterns of ventilation indicate that spatiotemporal aeration after birth is more complex than a central-distal process. The preferential ventilation of the right lung was unexpected but biologically plausible. At birth the lung is fluid filled, and airways (and tissue) have a high resistance.25 The left main bronchus exits the carina acutely, and is encumbered by the heart. This may create preferential flow states towards the right lung, especially during the higher inspiratory flows of crying. Resistance falls in those areas of the lung that aerate first, further potentiating ventilation compared to unaerated regions. Our data also suggests that ventilation initially follows a gravity-dependent pattern, similar to that seen in parenchymal lung diseases.26 Once aerated the lung rapidly develops the anatomical ventrodorsal pattern of ventilation reported in healthy older infants, favouring the dorsal lung with its increased lung mass and greater diaphragmatic tidal movement.17,27 These changing spatiotemporal patterns across multiple planes make applying respiratory support without risking lung injury particularly challenging.
As expected in healthy infants, during the first two minutes 80% of breaths were cries. In a similar population of 13 infants, 77% of all breaths (n=749) in the first 90 seconds after birth were classified as cries or grunts, but breath classification was performed post hoc from face mask flow measurements without auditory or visual confirmation, limiting interpretability.14 Our study is the first to classify volume changes with flow and breathing behaviour. Crying created different flow characteristics than tidal breathing, quickly inflating the lung with faster Ti and PIF. This is advantageous within the highly resistive fluid-filled lung at birth,25 but once aerated provides little mechanical or gas exchange benefit. We postulate that crying has a de novo physiological purpose, and not simply due to the noxious stress response of birth. Once aerated the high PIF conditions of crying increase unventilated lung tissue, with infants switching to the more advantageous tidal breaths.
Crying is also an expiratory phenomenon, being associated with slow expiratory flows, longer Te and τ. Volume loss during expiration followed a unique bifid pattern, occurring in 71% of all cries and rarely in tidal inflations. This pattern of volume change represents transient periods of minimal airway flow despite the chest wall being in a state of expiratory recoil. In this state reducing expiratory flow could only be achieved via active means, such as glottic closure or diaphragmatic hold; both seen in radiological imaging at birth.7 The lung is in a state of flux in early ex-utero life; the alveoli maybe air-filled but fetal lung fluid remains in the interstitium, and fluid can influx back into alveoli if the intrathoracic pressure gradient falls, compromising FRC.4,8,25 It has been proposed that ‘expiratory braking’ is essential during this period,1,5-7,15,16 and flow patterns measured at the airway opening support this, but have not been correlated to temporal FRC change.14 Our study provides the first evidence that expiratory braking does more than just prevent egress of gas from the lungs. It also facilitates the volumetric conditions needed to preserve FRC, and importantly redistributes gas within the lungs (pendelluft flow). This provides a simple visual indicator of an infant’s independent ability to support respiratory transition. Further studies involving at risk and preterm infants are warranted.
Reports of the cardiorespiratory processes at birth are sparse, mainly due to challenges in measurement. Following chest radiology studies in the 1960s,6,7 instrumentation within the mouth, initially with bulky equipment,5,15,16 and more recently, face masks14,28 have been used to measure airway opening flow, VT, expired CO2 and/or pressure changes, and infer intrathoracic conditions. The usefulness of face mask measurements during spontaneous breathing is questionable. Face masks are frequently applied with a leak,29 application interferes with normal breathing efforts,30 and cannot identify important spatiotemporal events. Ideally measurements should be obtained from the thorax without interfering with respiratory effort. Recently respiratory inductive plethysmography28 and lung ultrasound13 have been used in the delivery room. Inductive plethysmography requires applying two belts and determines lung volume from measuring the cross-sectional areas of the chest and abdomen, which may not change between fluid- and air-filled states.24 Lung ultrasound is ideal for imaging the air-fluid interface, is simple to use, but lacks regional resolution, and continuous imaging has not been possible.13 In this context, EIT is attractive. EIT is an established and validated method of measuring multiple spatiotemporal respiratory parameters.17 EIT is radiation-free and available with a simple non-invasive belt 18 that could be applied as quickly, and more reliably, than pulse oximetry. EIT also confirmed the physiological patterns seen in humans and preclinical studies using these other measurement tools.2,8 We contend that EIT is currently the best method of monitoring the respiratory system at birth.
Limitations
EIT is not without limitations, which have been extensively detailed.17 EIT primarily measures relative changes, being more suited to monitoring intra-subject temporal changes. Like all other imaging tools used to describe the respiratory transition, EIT is limited to imaging a single slice of the lung. However, single slice EIT has been shown to represent whole lung patterns in infants.17 EIT cannot measure intrathoracic pressure. To do so would require invasive instrumentation, but is unnecessary as flow patterns reflect intrathoracic pressure states. Our study of 1401 inflations from 17 infants is one of the largest to date, but, like previous studies,14,15 exclusions were high. In part this was intentional; our methodology was designed to minimise the potential of artefact and ensure correct breath classification lacking in previous studies. It is possible that respiratory drive occurred with an occluded airway. This would not result in a volume change on EIT but is an important physiological finding that should be seen on video.
Conclusions
This study provides the first detailed description of the respiratory behaviour of the healthy human lung during the transition to air-breathing after birth. The respiratory transition requires rapid aeration of the lung, and is achieved predominately via crying. Crying creates unique flow and volume states not seen elsewhere in respiratory physiology, and is characterised by high peak inspiratory flow and expiratory braking to preserve attained FRC and allow volume redistribution. The right lung ventilates before the left lung after birth, and the lung quickly develops an anatomical pattern of ventrodorsal ventilation once aerated. Understanding how the human lung successfully commences breathing at birth is the first step in developing tools to identifying when intervention is required.
Data Availability
Individual participant data collected during the study, after de-identification, and study protocols and statistical analysis code are available beginning 3 months and ending 23 years following article publication to researchers who provide a methodological sound proposal, with approval by an independent review committee (learned intermediatry) identified for purpose. Data is available for analysis to achieve aims in the approved proposal. Proposals should be directed to david.tingay@mcri.edu.au; to gain access, data requestors will need to sign a data access or material transfer agreement approved by the Murdoch Childrens Research Institute.
Author Contributions
DGT developed the concept and designed the experiment. DGT, OF, JT, EJP, CR enrolled and studied all infants. AW, IF, AA, DGT developed the image reconstruction and analysis methods used in the study. DGT, OF, JT, PP-F were involved in data analysis. DGT, PGD, IF, AA interpreted the data. DGT wrote the first draft of the manuscript and all authors contributed to redrafting the manuscript.
Financial Support
This study is supported by the Victorian Government Operational Infrastructure Support Program (Melbourne, Australia) and a grant from a National Health and Medical Research Council Centre of Research Excellence (Grant ID 1057514). DGT is supported by a National Health and Medical Research Council Clinical Career Development Fellowship (Grant ID 1053889). PGD is supported by a National Health and Medical Research Council Program Grant (Grant ID 606789). PGD is supported by a National Health and Medical Research Council Practitioner Fellowship (Grant ID 556600).
Competing Interests
AW was an employee of Swisstom AG (Landquart, Switzerland), who initially developed the EIT hardware and software systems (Swisstom was acquired by Sentec AG after the study was completed). Swisstom was not involved in study design, implementation, analysis, interpretation or reporting. IF and AW were investigators in an European Union Horizon 2020 Research and Innovation program grant to develop an infant EIT chest imaging system (CRADL project, Grant ID 668259). IF also reports funding from another European Union Horizon 2020 project (WELMO, Grant ID 825572) and reimbursement of speaking fees, congress and travel costs by Dräger Medical (a company that produces a commercial EIT unit). No author received an honorarium, grant, or other form of payment to produce the manuscript. The study was not commissioned and no commercial agencies were involved in any aspect of this study. The authors have no other competing interests to declare.
Ethics Approval
The Royal Women’s Hospital Human Research and Ethics Committee (#16-33), and registered with the Australian New Zealand Clinical Trials Registry (ACTRN12618000128291).
Data Sharing
Individual participant data collected during the study, after de-identification, and study protocols and statistical analysis code are available beginning 3 months and ending 23 years following article publication to researchers who provide a methodological sound proposal, with approval by an independent review committee (“learned intermediatry”) identified for purpose. Data is available for analysis to achieve aims in the approved proposal. Proposals should be directed to david.tingay@mcri.edu.au; to gain access, data requestors will need to sign a data access or material transfer agreement approved by the Murdoch Children’s Research Institute.
Acknowledgements
The authors wish to thank the families, infants and Royal Women’s Hospital staff involved in the study. The authors acknowledge Dr Kate Patterson of Medipics and Prose for assistance with figures and videos. The authors also acknowledge the assistance of Dr Louise Owen and Dr C. Omar Kamlin at the Royal Women’s Hospital for advice on study implementation in the delivery room.
ABBREVIATIONS
- AU
- Arbitrary Units
- CoV
- Centre of Ventilation
- EIT
- Electrical Impedance Tomography
- FRC
- Functional Residual Capacity
- PEF
- Peak Expiratory Flow
- PIF
- Peak Inspiratory Flow
- SpO2
- Peripheral oxygen saturation
- τ
- Time constant (tau)
- Ti
- Inspiratory time
- Te
- Expiratory time
- VT
- Tidal Volume





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}