
Abstract
Background Coronavirus disease 2019 (COVID-19) has spread rapidly worldwide and seriously threatens human health since December 2019. However, information about acute kidney injury (AKI) during COVID-19 infection is limited. Some studies thought that presence of AKI is very common and cannot be ignored, while some studies pointed that AKI only is a rare incident during COVID-19 infection. This meta-analysis aimed to find out the truth of COVID-19 related AKI and to provide stronger evidence.
Methods Two authors independently performed a literature search using PubMed, Web of Science, Embase, and Cochrane Library fulfilled the pre-specified criteria until April 25, 2020 to include studies reported the necessary clinic characteristics, then the incidence of AKI, incidence of required RRT, the mortality with AKI and the death risk with AKI during COVID-19 infection were pooled for statistical analysis by Open Meta-Analyst software to get conclusions.
Findings It was found that the incidence of AKI in hospitalized patients with COVID-19 infection is low, only about 3.8%; the in-hospital mortality with AKI in COVID-19 infected patients is reach up to 32.6%; the death risk with AKI in COVID-19 infected patients is about 16.1 times higher than those without AKI.
Conclusions This meta-analysis indicated AKI during COVID-19 infection should be pay more attention, it maybe a strong red flag to death risk. It is still need additional studies to support the conclusions and to explore the AKI mechanism during COVID-19 infection.
1. introduction
Starting in December 2019, coronavirus disease 2019 (COVID-19) caused by the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) with unbelievable spread speed and high mortality worldwide. 1 According to the WHO, SARS-CoV-2 infection outside of China is keep increasing rapidly by April 20, 2020, with 231,4621 laboratory-confirmed cases and 157847 deaths due to COVID-19 in > 150 different countries. 2 There are still no specific treatments or vaccines for COVID-19 at present.
The SARS-CoV-2 was found as a positive-sense single-stranded RNA virus belonging to the β-coronavirus cluster, mainly cause community-acquired pneumonia in humans. 1 Fever and cough were the most common symptoms during infection. 3 Epidemiological data about COVID-19 are still limited available so far, early studies focused on describing the clinical characteristics and severe cases. Rencently, the evidence growing that there was a common presence of acute kidney injury (AKI) in COVID-19 patients even related to death,4,5,6 while other studies1,7 thought that AKI is only a rare incident during COVID-19 infection. More powerful evidences are lack and urgently needed to resolve clinical problems and disputes. In addition, the effects of COVID-19 infection on renal function still remain unclear and should to explore. This meta-analysis aimed to investigate the authentic incidence of AKI during COVID-19 infection and to confirm whether COVID-19 related AKI would impact on mortality or not, by pooling the available data from publications.
2. Materials and Methods
2.1. Search Strategy
The protocol for this meta-analysis was registered with the International Prospective Register of Systematic Reviews (PROSPERO ID. CRD42020181188). A systematic literature search was performed using PubMed, Web of Science, Embase, and Cochrane Library through April 25, 2020 to summarize the data of AKI on COVID-19 infected patients. The systematic literature search was not executed on any preprints databases to ensure the reliability of final statistical results. Two authors (ZX.M. and X.Z.) independently carried out systematic literature search employing terms “acute kidney” OR “acute renal” AND “coronavirus 2019” OR “COVID-19” OR “2019-nCoV” OR “SARS-CoV-2” OR “severe acute respiratory syndrome coronavirus 2” OR “novel coronavirus” OR “SARS-CoV-2” OR “nCoV disease” OR “SARS2” OR “COVID19” OR “2019nCoV” OR “coronavirus disease-19” OR “coronavirus disease 2019” OR “2019 novel coronavirus”. Each study was evaluated for inclusion or exclusion for this analysis. No language restriction was applied. Publication dates restriction was applied from January 2020. A manual search for references cited in the articles found was performed as well. The meta-analysis was conducted and handled according to the guidelines of the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). (http://www.prismastatement.org/).
2.2. Inclusion/ Exclusion Criteria
For the meta-analysis presented and AKI definition, eligible studies reporting the AKI or AKI related indicators of patients infected with COVID-19 were considered. Studies met the Population, Interventions, Comparison and Outcomes (PICO) criteria were included in the meta-analysis.
All the studies selected fulfilled the following criteria: original cohort studies provided the necessary clinical characteristic data during COVID-19 infection; concerning AKI required/not required renal replacement therapy (RRT) among COVID-19 infected patients; reported the specific AKI related indicators (hematuria, proteinuria, or serum creatinine) of COVID-19 infected patients; potentially eligible studies regardless AKI or RRT definition; all COVID-19 infected patients enrolled in this study were identified and confirmed with nucleic acid detection by laboratory.
Cases with history of chronic kidney diseases pre-COVID-19 infection while can not identified after infected in the original report were excluded; case/case series reports containing < 10 patients were excluded; duplicate articles were excluded; reports from the National Health Commission were excluded to avoid repeated data.
2.3. Data Extraction and Study Quality
A data collecting spreadsheet (Microsoft Corporation, Redmond, WA) was established to extract the following data from each included study: the first author, data collection period, region/hospital, number of patients, number of AKI/RRT patients, AKI related indicators, AKI related death. No attemps were made for specific or missing data from the authors. To prevent data overlapping, the duration and hospital were specified due to some reports come from the same hospital.
All included studies considered were assessed regarding their quality using the Newcastle-Ottawa Quality Assessment Scale (NOS) containing 3 aspects (selection, comparability and outcomes) and 8 items. 8 It ranges from 0 to 9 scores, studies with a score ≧ 6 were considered to meet adequate methodological quality.
2.4. AKI and RRT definitions
RIFLE (the Risk of renal failure, Injury to the kidney, Failure of kidney function, Loss of kidney function and End stage kidney disease), AKIN (the Acute Kidney Injury Network), and KDIGO (the Kidney Disease Improving Global Outcomes) were the three major criteria to define AKI.9,10 In this meta-analysis, AKI were accepted as the original studies believed AKI incident occurred no matter have defined according to one of the above guidelines or not; required RRT were accepted as the original studies have record RRT used regardless modality.
2.5. Statistical Analysis
Open Meta-Analyst software (for Windows 10 version; Brown University, Providence, USA) was applied for the statistical analysis. In this analysis, random effects models and DerSimonian-Laird method were applied to analyze the incidence of AKI, the incidence of required RRT, the mortality with AKI (ratio variables), and the death risk with AKI (dichotomous variables) during COVID-19 infection; the pooled odds ratio (ORs) was used to analyze the death risk with AKI; all the corresponding 95% confidence intervals (CI) were evaluated; I2 test was used to assess heterogeneity due to probability variance among observational studies; the graphically plotted using forest plots. Statistically significant heterogeneity among studies was defined as χ2P value< 0.05 or I2 test > 50%; P value < 0.05 was considered statistically significant.
3. Results
3.1 Literature Search and study characteristics
The flowchart of the systematic review with selection process and reasons for exclusion was demonstrated in detail in Figure 1. A total of 58 records were identified from 4 databases (PubMed, n= 24; Web of Science, n= 7; Embase, n= 27; Cochrane Library, n= 0). After duplicates were excluded (32 records), 26 articles were screened through titles and abstracts manually for eligibility. Then in-vitro studies, animal studies, case reports, review articles, letters, comments, and erratums were excluded. 15 remaining articles were full-text reviewed for eligibility. The cited reference of the remaining articles were also screened through titles. The studies contained< 10 patients or insufficient clinical data were also excluded. Finally 11 cohort studies involving 5336 patients fulfilled the pre-specified criteria were included for the meta-analysis (Table 1). Four studies (36.4%) with a score ≧ 6 were considered with high quality according to the NOS criteria (Table 2) (follow-up outcomes data were not available).

The flowchart for the systematic review.
Study characteristics
Newcastle-Ottawa Scale for assessing the quality of cohort studies
3.2 Included Studies characteristics
The data collection period of included studies was between December 2019 and April 2020. Six studies (54.5%) reported the outcomes with clearly defined AKI according to KDIGO. Eight (72.7%) studies reported RRT required during COVID-19 infection and almost used continuous renal replacement therapy (CRRT). Four studies (36.4%) reported the outcomes with clearly numbers of AKI related death while one study gave the hazard ratios (HR) between AKI and in-hospital death.
3.3 Incidence of AKI during COVID-19 infection
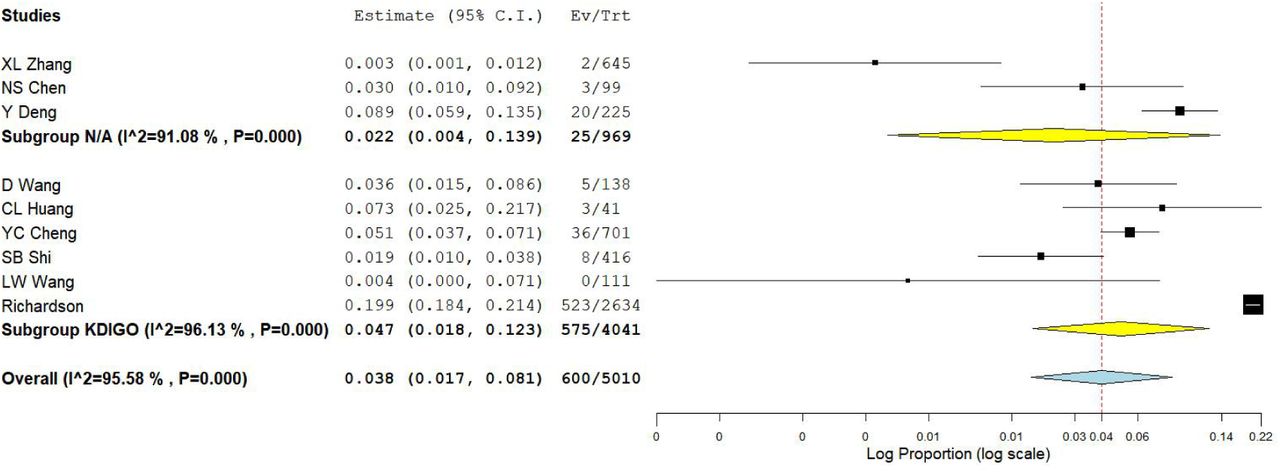
Overall, 600 patients developed AKI during COVID-19 infection, the pooled estimated incidence of AKI during COVID-19 infection was 3.8% (95%CI: 1.7%-8.1%, P < 0.001, Figure 2), and significant heterogeneity (I2= 95.58%, χ2P < 0.001) was observed. Subgroup analysis was performed according to different AKI defined criterion. The pooled estimated AKI incidence in KDIGO subgroup analysis and none-defined (N/A) subgroup analysis were 4.7% (95%CI: 1.8%-12.3%, I2=96.13%, χ2P< 0.001, P< 0.001, Figure 2) and 2.2% (95%CI: 0.4%-13.9%, I2= 91.08%, χ 2P< 0.001, P< 0.001, Figure 2) respectively. There were still significant heterogeneity existed after subgroup analysis. (Data come from NS Chen 12 and XB Yang 13 was not calculated 2 times)
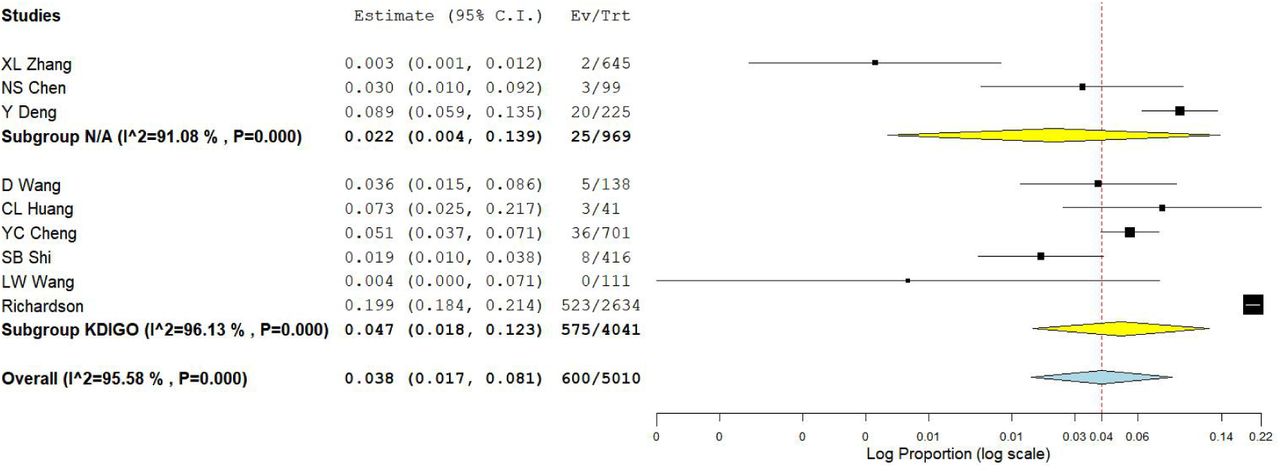
Incidence of AKI during COVID-19 infection.
3.4 Incidence of Required RRT during COVID-19 infection
The following meta-analysis showed that 100 patients required RRT during COVID-19 infection, the pooled estimated incidence of required RRT during COVID-19 infection was 2.2% (95%CI: 1.0%-4.6%, P< 0.001, Figure 3), and significant heterogeneity (I2= 81.28%, χ2P< 0.001) was also observed among the eligible studies. (Data come from T Chen 3 and YC Cheng 6 was not calculated 2 times).

Incidence of Required RRT during COVID-19 infection.
3.5 Mortality with AKI and the death risk with AKI during COVID-19 infection
The last series meta-analysis showed that 407 patients death with AKI during COVID-19 infection, the pooled estimated mortality with AKI in COVID-19 infected patients was 32.6% (95%CI: 16.8%-63.2%, P< 0.001, Figure 4a), and significant heterogeneity (I2= 95.64%, χ2P< 0.001) was also observed among the eligible studies. The death risk with AKI in COVID-19 infected patients with AKI was estimated 16.1 times higher (OR, 16.1; 95%CI: 5.9–46.14, P< 0.001, I2= 56.88%, χ2P= 0.073) than those patients without AKI (Figure 4b).

Mortality with AKI and the death risk with AKI during COVID-19 infection
4. DISCUSSION
This population-based meta-analysis provided evidence that the incidence of AKI in hospitalized patients with COVID-19 infection is low, only about 3.8%. However, the appearance AKI during COVID-19 infection should be recognized a strong warning signal: the in-hospital mortality with AKI in COVID-19 infected patients is greater, reach up to 32.6%; the death risk with AKI in COVID-19 infected patients is extremely high, about 16.1 times higher than those without AKI.
The spike protein of SARS-CoV-2 binds to angiotensin converting enzyme 2 (ACE2), would be activated and cleaved by cellular transmembrane serine proteases (TMPRSSs), leading to release of fusion peptides and fuse to host cells membrane. 19 Thus, the co-expression of ACE2 and TMPRSSs are key factors to determine the entrance of SARS-CoV-2 into host cells. One study based on analysis of normal kidney cells indicated that ACE2 and TMPRSS genes were high co-expression in podocytes and proximal straight tubule cells, which play critical roles in urine filtration, reabsorption and excretion. 20According to the European Centre for Disease Prevention and Control (ECdC), about 80% of COVID-19 infection cases is mild, while 14% patients experience severe infection and 6% patients develop to critically ill. 21 As the SARS-CoV-2 mainly first induced respiratory tract infection, the duration and accumulation of SARS-CoV-2 in the circulation, maybe key courses to attack extra-pulmonary organs include kidney. Once extra-pulmonary organs dysfunction such as kidney occurrence, which means a large number of viruses had been replicated in patients, multiple organs would be attacked simultaneously, plus a pathologic dysregulated host response with a hyper inflammatory cytokine storm, 22 together cause critical illness patients to death. These perhaps explanations of different AKI incidence and mortality among studies observed during COVID-19 infection. A time dependant anti-viral treatment approach perhaps need to be focused, while this is beyond the scope of the meta-analysis and not investigated. However, renal function and the urine of COVID-19 patients should be frequently monitored any way.
Rencently, some studies proposed a mechanism named “organ crosstalk”, it describes that the impaired function of one organ is communicated to the dysfunction of other organs and mediated each other via complex mechanisms in critical illness,23,24 AKI is one of typical examples involving multiple organ interactions.23,24 Acute respiratory distress syndrome (ARDS) associated AKI as a kind of lung-kidney interactions has been identified. AKI may act as an initiated incident or an aggravated factor via multiple mechanisms, including blood gas disturbances, renal congestion due to pulmonary hypertension, and hormone dysregulation. 25 In addition, mechanical ventilation induced haemodynamics alternation and lung injury may amplify the conditions and exacerbate end-organ injury already existed. 25
As mentioned above, no vaccine or specific anti-viral drugs for covid-19 has yet been shown to be effective. At present, supportive treatment to ease the symptoms and to prevent multi-organ dysfunction in severe COVID-19 infected patients were often prescribed, which means some executed interventions with the inevitable sacrifice of renal function (such as chloroquine phosphate). AKI might be considered an inevitable clinical syndrome in these patients like other critical ill patients, as over 50% of those would develop stage 1 AKI at some point during their ICU course. 26
The study has several limitations. Firstly, there are still limited original studies (< 10) to evaluate the death risk with AKI during COVID-19 infection. However, considering this research potentially with important clinical guidance and the serious situation of COVID-19 spread, we decided to report. Second, there is statistical significant heterogeneity in the meta-analysis for AKI incidence. Potential origins for significant heterogeneity may come from different COVID-19 infection stage. As performed subgroup analysis of AKI definition, the heterogeneity still showed significant. Lastly, since the clinic data collection based on publications was limited availability, extra sub-analysis could not but should performed (infection period, drugs used, COVID-19 infection stages separation et al). Nevertheless, AKI with COVID-19 infection should be pay more attention. Furthermore studies are still need to support the conclusion and explore the AKI mechanism during COVID-19 infection.
Data Availability
All data generated or analyzed during this study are included in this article.
Footnotes
Funding: This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.





{kind=link}
{kind=link}
{kind=link}
{kind=link}