
ABSTRACT
Background The overall objective of this rapid overview of reviews (overview hereafter) was to identify evidence from systematic reviews (SRs) for infection control and prevention practices for adults aged 60 years and older in long-term care settings.
Methods Comprehensive searches in MEDLINE, EMBASE, the Cochrane Library, biorxiv.org/medrxiv.org, clinicaltrials.gov and the Global Infectious Disease Epidemiology Network (GIDEON) were carried out in early March 2020. Title/abstract and full-text screening, data abstraction, and quality appraisal (AMSTAR 2) were carried out by single reviewers.
Results A total of 6 SRs published between 1999 and 2018 were identified and included in the overview. The SRs included between 1 and 37 primary studies representing between 140 to 908 patients. All of the primary studies included in the SRs were carried out in long-term care facilities (LTCF) and examined pharmacological, non-pharmacological, or combined interventions. One high quality SR found mixed results for the effectiveness of hand hygiene to prevent infection (2 studies statistically significant positive results, 1 study non-statistically significant results). One moderate quality SR with meta-analysis found a moderate non-statistically significant effect for personal protective equipment (PPE) in preventing infection and found no statistically significant results for the effectiveness of social isolation. One moderate quality SR reported statically significant evidence for the effectiveness of amantadine and amantadine + PPE to prevent infection with respiratory illness in LTCF.
Conclusion The current evidence suggests that with antiviral chemoprophylaxis with adamantine is effective in managing respiratory illness in residents of long-term care facilities. The rest of the strategies can be used in long-term care facilities, yet have limited evidence supporting their use from systematic reviews.
INTRODUCTION
Purpose and Research Questions
The Infection Prevention & Control of the World Health Organization (WHO) Health Emergency Programme presented a query on preventing and managing COVID-19 in older adults aged 60 years and above living in long-term care facilities including privately paid for and publicly paid for settings with a 5-business day timeline. According to the WHO, "long-term care covers those activities undertaken by others to ensure that people with, or at risk of, a significant ongoing loss of intrinsic capacity can maintain a level of functional ability consistent with their basic rights, fundamental freedoms and human dignity” (https://www.who.int/ageing/long-term-care/WHO-LTC-series-subsaharan-africa.pdf?ua=1). Examples of long-term care include nursing homes, charitable homes, municipal homes, long-term care hospitals, long-term care facilities, skilled nursing facilities, convalescent homes, and assisted living facilities (https://www.canada.ca/en/health-canada/services/home-continuing-care/long-term-facilities-based-care.html).
The overall objective of this rapid overview of reviews (overview hereafter) was to identify evidence on infection protection and control measures for adults aged 60 years and older in long-term care settings from systematic reviews. In order to focus the research question to increase feasibility, we proposed the following key research questions:
What are the infection prevention and control practices/measures for preventing or reducing respiratory viruses (including coronavirus and influenza) in older adults aged 60 years and above living in long-term care?
How do infection prevention and control practices differ for adults aged 60 years and above living in long-term care with respiratory illness and severe comorbidities or frailty differ than those without such severe comorbidities/frailty?
How do infection prevention and control practices differ for adults aged 60 years and above living in long-term care with respiratory illness from low- and middle-income economy countries (LMIC) differ than those living in high-income economy countries and do differences exist across different cultural contexts?
METHODS
The rapid overview was guided by the Cochrane Handbook for Systematic Reviews of Interventions1 along with the Rapid Review Guide for Health Policy and Systems Research2. The team used an integrated knowledge translation approach, with consultation from the knowledge users from the WHO at the following stages: question development, interpretation of results, and draft report. We used the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement3 to guide the reporting of our rapid overview results; a PRISMA extension for rapid reviews and a reporting guideline on overviews are currently under development. This rapid overview was completed in conjunction with a rapid review of clinical practice guidelines published in a separate report titled: Guidelines for preventing respiratory illness in older adults aged 60 years and above living in long-term care: A rapid review of clinical practice guidelines.
Protocol
We prepared a brief protocol for this query that is available in Appendix 1. If publication in a peer-reviewed journal is planned in the future, we will register this rapid review with the Open Science Framework (https://osf.io/).
Literature search
Comprehensive literature searches addressing all research questions were developed by an experienced librarian for MEDLINE, EMBASE, the Cochrane Library, and biorxiv.org/medrxiv.org databases. Grey (i.e., difficult to locate or unpublished) literature was located using keyword searches of relevant terms (e.g. respiratory illness, MERS, coronavirus, SARS, long-term care facilities) in clinicaltrials.gov and GIDEON (Global Infectious Diseases and Epidemiology Network). The full MEDLINE search strategy can be found in Appendix 2. Due to the rapid timelines for this overview, a peer review of the literature search was not conducted.
Eligibility criteria
The Eligibility criteria followed the PICOST framework and consisted of:
Population: Individuals aged 60 years and above residing in long-term care facilities. The age cut-off for an older adult might be 50 years and above in different LMIC and/or cultural settings. As such, we included these in level 1 screening of titles and abstracts and presented potentially relevant studies in an appendix.
Intervention: Any form of infection control and prevention, such as hand hygiene, respiratory hygiene/etiquette, personal protective equipment (for patients and health care providers), triage (on arrival), source control, isolation, daily monitoring/surveillance for signs and symptoms of respiratory illness (e.g., COVID-19) in residence, environmental cleaning, cleaning of linen and medical equipment used by patients, restrictions on resident movement and transportation, restrictions on visitors, restrictions on travel for health care providers and other long-term care facility staff, waste management, dead body management. Only those measures used to prevent and control respiratory illnesses, including influenza and coronavirus (e.g., COVID-19, MERS, SARS) were included. Interventions focused on preventing bacterial respiratory outbreaks (e.g., strep, pneumonia, klebsiella) or aspiration pneumonia were excluded. Interventions specifically focused on vaccination were excluded, as a vaccine for the coronavirus currently does not exist.
Comparator: One of the interventions listed above or no intervention
Outcomes: Lab-confirmed respiratory illness due to the virus (e.g., SARS, MERS, COVID-19, influenza) [primary outcome], secondary bacterial infection, symptoms, secondary transmission (e.g., other patients, healthcare workers, visitors), goal concordant care, hospitalization, intensive-care unit (ICU) admission, and mortality.
Study designs: We limited inclusion to systematic reviews using the Cochrane definition of a systematic review (https://www.cochrane.org/news/what-are-systematic-reviews).
Time periods: All periods of time and duration of follow-up were eligible.
Other: No other restrictions were imposed.
Study selection
For both level 1 (title/abstract) and level 2 (full-text) screening, a screening form was prepared based on the eligibility criteria and pilot-tested by the review team using 25 citations prior to level 1 screening and 5 full text articles prior to level 2 screening. Agreement between reviewers was sufficiently high (>75%) in both cases so no further pilot-testing was required. Full screening was completed by a single reviewer for both level 1 and level 2 using Synthesi.SR, the team’s proprietary online software (https://breakthroughkt.ca/login.php).
Data items and data abstraction
Items for data abstraction included characteristics (e.g., duration of follow-up, study design, country of conduct, multi-center vs. single site, long-term care setting characteristics, such as availability of medical support, characteristics of care staff, family/community engagement, accommodation characteristics, collective practices), patient characteristics (e.g., mean age, age range, co-morbidities), intervention details (e.g., type of intervention, duration and frequency of intervention, timing of intervention), comparator details (e.g., comparator intervention, duration and frequency of intervention, timing of intervention), and outcome results (e.g., lab-confirmed viral respiratory infection, symptoms, secondary transmission, hospitalization, ICU admission, mortality) at the longest duration of follow-up. A standardized data abstraction form was developed. Prior to data abstraction, a calibration exercise was completed to test the form amongst the entire review team using two randomly selected full-text systematic reviews. Following successful completion of the calibration exercise, included reviews were abstracted by single reviewers.
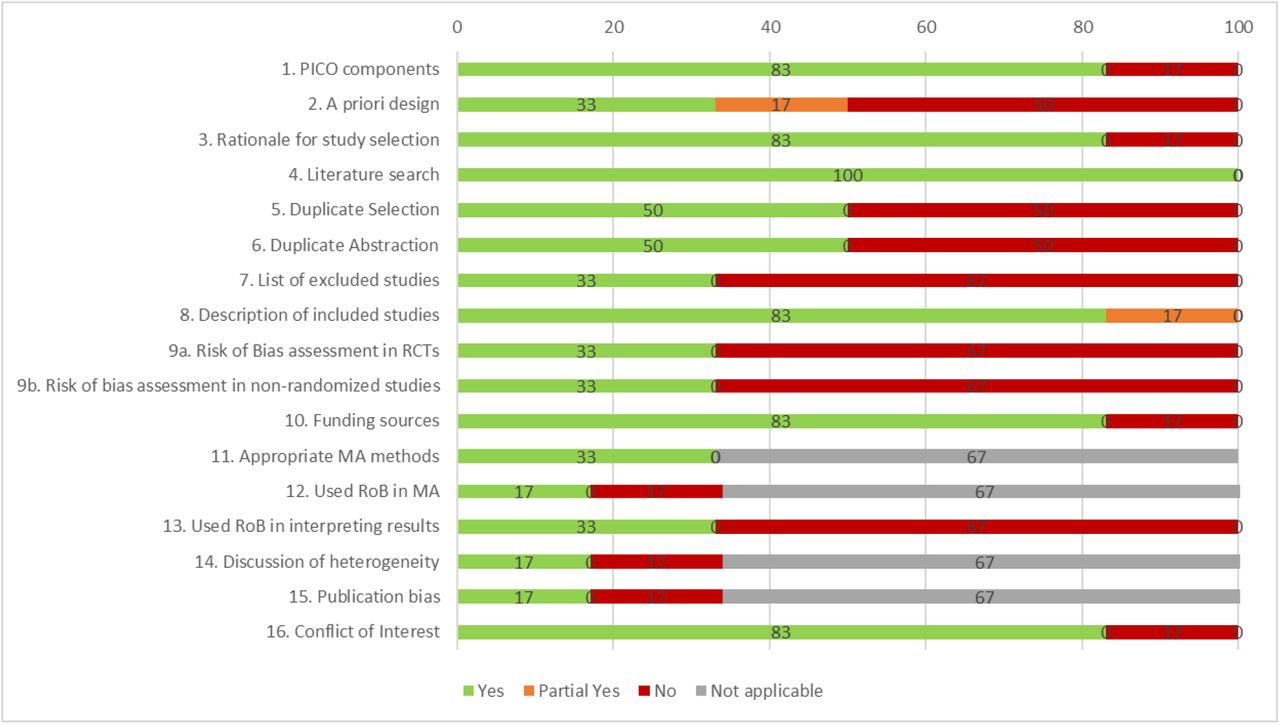
Risk of bias appraisal
Risk of bias appraisal was carried out by single reviewers using the AMSTAR-2 tool (https://amstar.ca/Amstar-2.php). The AMSTAR-2 tool includes 16 items, plus an overall risk of bias rating that ranges from low risk of bias to high risk of bias, with moderate risk of bias in between. The items focus on methods related to the research question, protocol, literature search, study selection, risk of bias appraisal, data abstraction, meta-analysis, and conflicts of interest.
Synthesis
Included studies were synthesized descriptively including summary statistics and detailed tables of study characteristics and results. Tables of study results are organized according to study design and where available, information on relevant subgroups were highlighted.
RESULTS
Literature Search
The database search returned a total of 3,309 citations, while the grey literature searches returned 42 citations for level 1 screening. A total of 3,225 citations were excluded after level 1 screening. Of the 126 articles screened at level 2, 6 systematic reviews were included (Figure 1).

Characteristics of included systematic reviews
The six systematic reviews were published between 1999 and 2018 (Appendix 3). The number of studies included in the systematic reviews ranged from 1 to 37 (not reported in one systematic review). Only two systematic reviews reported the number of included patients, which ranged from 140 to 908. The systematic reviews included studies that were conducted in long-term care facilities and the interventions were pharmacological (e.g., antiviral chemoprophylaxis), non-pharmacological (e.g., increasing hand hygiene, personal protective equipment, social distancing), and a combination of pharmacological and non-pharmacological.
Quality Appraisal Results
The six systematic reviews varied in their quality according to the AMSTAR-2 tool, with two being assessed as having a high risk of bias, one with a moderate risk of bias, and three with a low risk of bias (Figure 2, Appendix 4).
{kind=link}
{kind=link}
Effectiveness Results
Preventing respiratory illness in long-term care facilities
One high quality SR found mixed results for the effectiveness of hand hygiene to prevent infection with 2 studies reporting statistically significant positive results in favour of hand hygiene and 1 study reporting non-statistically significant results. One moderate quality SR with meta-analysis found a moderate non-statistically significant effect in favour of personal protective equipment (PPE) in preventing infection. The same SR and meta-analysis also examined the effectiveness of social isolation to prevent infection and found no statistically significant results. One moderate quality SR reported statically significant evidence for the effectiveness of amantadine and amantadine + PPE to prevent the spread of viral respiratory infections in long-term care facilities.
Managing respiratory illness in long-term care facilities
Statistically significant results were found from one moderate and one high quality systematic review for the use of amantadine as antiviral chemoprophylaxis for individuals diagnosed with lab-confirmed influenza (Table 1). In addition, statistically significant results were found from one high quality systematic review for the use of amantadine plus personal protective equipment to prevent spread of infection from individuals diagnosed with lab-confirmed influenza. Statistically significant results were not observed in one moderate and one high quality systematic review regarding rimantadine or neuraminidase inhibitors as antiviral chemoprophylaxis. However, statistically significant results were observed in one low quality systematic review for rimantadine as antiviral chemoprophylaxis. Mixed evidence was identified from two low quality systematic reviews for zanamivir as antiviral chemoprophylaxis that reported non-statistically significant reductions in viral respiratory infection rates. The full systematic review results are available in Appendix 5.
DISCUSSION
The WHO commissioned a rapid overview to address the urgent question of the infection prevention and control practices/measures for respiratory viruses in long-term care facilities that could be applied to COVID-19. A comprehensive literature search of both electronic databases and grey literature sources resulted in six included systematic reviews, none of which specifically focused on issues related to residents with respiratory illness and severe comorbidities or frailty. Furthermore, none focused on issues in LMIC or different cultural contexts.
Overall, the results of the included systematic reviews suggest that high quality evidence supports treating residents with antiviral chemoprophylaxis with adamantine, as well as adamantine in combination with personal protective equipment. For the rest of the strategies, there was either no evidence of effectiveness (e.g., social isolation) or mixed evidence of effectiveness (e.g., rimantadine, zanamivir, hand hygiene, personal protective equipment). The mixed evidence on hand hygiene and use of personal protective equipment does not imply these should not be used in outbreaks.
There are several limitations to the overview methods employed here, single screening and abstraction for example, however they were selected to thoughtfully tailor our methods according to our knowledge user needs and the urgent nature of the request to provide timely results.
CONCLUSIONS
The current evidence suggests that with antiviral chemoprophylaxis with adamantine is effective in managing respiratory illness in residents of long-term care facilities. The rest of the strategies can be used in long-term care facilities, yet have limited evidence supporting their use.
Data Availability
All datasets supporting the conclusions of this article are included within the article
Copyright claims/Disclaimers
The intellectual property rights in data and results generated from the work reported in this document are held in joint ownership between the Knowledge Translation Program team and the named Contributors.
Users are permitted to disseminate the data and results presented in this report provided that the dissemination (i) does not misrepresent the data, results, analyses or conclusions, and (ii) is consistent with academic practice, the rights of any third party publisher, and applicable laws. Any dissemination of the data and results from this document shall properly acknowledge the Knowledge Translation Program team and named Contributors.
Funding Statement
This systematic review was commissioned and paid for by the World Health Organization and conducted through the Strategy for Patient Oriented-Research (SPOR) Evidence Alliance. The authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the World Health Organization.
Acknowledgements
Jessie McGowan (literature search), Krystle Amog (report preparation), Chantal Williams (report preparation), Naveeta Ramkissoon (report preparation)
APPENDIX 1 – PROTOCOL
Team name: Knowledge Translation Program of St. Michael’s Hospital, Unity Health Toronto (Drs. Tricco and Straus, contact andrea.tricco{at}unityhealth.to)
Query: Preventing the transmission of coronavirus (COVID-19) in older adults aged 60 years and above living in long-term care
Query Submitter: Infection Prevention & Control, World Health Organization (WHO) Health Emergency (WHE) Programme
Objective and research questions:
The Infection Prevention & Control of the WHO WHE Programme has presented a query on the transmission of COVID-19 in older adults aged 60 years and above living in long-term care including privately paid for and publicly paid for settings with a 5-business day timeline. According to the World Health Organization, “long-term care covers those activities undertaken by others to ensure that people with, or at risk of, a significant ongoing loss of intrinsic capacity can maintain a level of functional ability consistent with their basic rights, fundamental freedoms and human dignity” (https://www.who.int/ageing/long-term-care/WHO-LTC-series-subsaharan-africa.pdf?ua=1) Examples of long-term care will include nursing homes, charitable homes, municipal homes, long-term care hospitals, long-term care facilities, skilled nursing facilities, convalescent homes, and assisted living facilities (https://www.canada.ca/en/health-canada/services/home-continuing-care/long-term-facilities-based-care.html).
The proposed research questions are:
What are the infection prevention and control practices/measures for preventing or reducing respiratory viruses (including coronavirus and influenza) in older adults aged 60 years and above living in long-term care?
How do infection prevention and control practices differ for adults aged 60 years and above living in long-term care with respiratory illness and severe comorbidities or frailty differ than those without such severe comorbidities/frailty?
How do infection prevention and control practices differ for adults aged 60 years and above living in long-term care with respiratory illness from low- and middle-income economy countries (LMIC) differ than those living in high-income economy countries and do differences exist across different cultural contexts?
Research approach
The research question will be addressed through a rapid review informed by the methods proposed by the WHO Guide to rapid reviews (https://www.who.int/alliance-hpsr/resources/publications/rapid-review-guide/en/).
Protocol
Due to the urgent nature of the request and limited time frame to complete the work, this document will serve as the protocol for this query. If publication in a peer-reviewed journal is planned in the future, we will register this rapid review with the Open Science Framework (https://osf.io/).
Literature search
Comprehensive literature searches will be developed by an experienced librarian for MEDLINE, EMBASE, the Cochrane Library, biorxiv.org/medrxiv.org, and GIDEON (Global Infectious Diseases and Epidemiology Network). Grey (i.e., difficult to locate or unpublished) literature will be searched via clinicaltrials.gov. Due to the rapid timelines for this review a peer review of the literature search will not be conducted.
Eligibility criteria
The Eligibility criteria will follow the PICOST framework and will consist of:
Population: Individuals aged 60 years and above residing in long-term care facilities. The age cut-off for an older adult might be 50 years and above in some LMIC and/or cultural settings. As such, we will include these in level 1 screening of titles and abstracts and include anything deemed relevant at level 2 screening of full-text articles in an appendix.
Interventions: Any form of infection control and prevention, such as hand hygiene, respiratory hygiene/etiquette, personal protective equipment (for patients and health care providers), triage (on arrival), source control, isolation, daily monitoring/surveillance for signs and symptoms of respiratory illness (e.g., COVID-19) in residence, environmental cleaning, cleaning of linen and medical equipment used by patients, restrictions on resident movement and transportation, restrictions on visitors, restrictions on travel for health care providers and other long-term care facility staff, waste management, dead body management. Only those measures used to prevent and control respiratory illnesses, including influenza and coronavirus (e.g., COVID-19, MERS, SARS) will be included. Interventions focused on preventing bacterial respiratory outbreaks (e.g., strep, pneumonia, klebsiella) will be excluded.
Comparator: One of the interventions listed above or no intervention
Outcomes: Lab-confirmed respiratory illness due to the virus (e.g., SARS, MERS, COVID-19, influenza) [primary outcome], secondary bacterial infection, symptoms, secondary transmission (e.g., other patients, healthcare workers, visitors), goal concordant care, hospitalization, intensive-care unit (ICU) admission, mortality
Study designs: Due to the rapid nature of this request, we will limit inclusion to clinical practice guidelines and systematic reviews, using the Cochrane definition of a systematic review. If there is scant evidence from these study designs, we will expand inclusion to include the following study designs:
Randomized controlled trials (RCTs)
NRCTs (e.g., such as quasi-RCTs, non-randomized trials, interrupted time series, controlled before after),
Observational studies (e.g., cohort, case control, cross-sectional)
Case studies, case reports, and case series, including outbreak reports
Time periods: All periods of time and duration of follow-up will be included.
Other limitations: No other limitations will be imposed. If possible, we will translate studies written in languages other than English (e.g., Mandarin, Cantonese) that are deemed relevant.
Study selection process
In order to meet the requested timeline of 5 working days a streamlined approach to study selection will be employed. A screening form based on the eligibility criteria will be prepared and a brief calibration exercise will be conducted prior to citation and full-text screening. Screening will be completed by single reviewers using Synthesi.SR, the team’s proprietary online software (https://breakthroughkt.ca/login.php).
Data items and data abstraction process
Items for data abstraction will include study characteristics (e.g., duration of follow-up, study design, country of conduct, multi-center vs. single site, long-term care setting characteristics, such as availability of medical support, characteristics of care staff, family/community engagement, accommodation characteristics, collective practices), patient characteristics (e.g., mean age, age range, co-morbidities), intervention details (e.g., type of intervention, duration and frequency of intervention, timing of intervention), comparator details (e.g., comparator intervention, duration and frequency of intervention, timing of intervention), and outcome results (e.g., lab-confirmed viral respiratory infection, symptoms, secondary transmission, hospitalization, ICU admission, mortality) at the longest duration of follow-up. For the clinical practice guidelines, we will abstract the recommendations and level of evidence for reach recommendation.
Prior to data abstraction, we will complete a calibration exercise of the form amongst all reviewers using a random sample of 2 included articles. Following calibration, included studies will be abstracted by single reviewers.
Risk of bias appraisal
Risk of bias appraisal will be carried out by single reviewers using the AMSTAR-2 tool (https://amstar.ca/Amstar-2.php) for systematic reviews and the AGREE-2 tool (https://www.agreetrust.org/resource-centre/agree-reporting-checklist/) for clinical practice guidelines.
Synthesis
The synthesis will involve providing a descriptive summary of included studies with summary tables and detailed tables of study results. Tables of study results will be organized according to interventions of interest and reported outcomes and where available, information on relevant subgroups will be presented separately.
Preliminary knowledge translation plan
The summary of results will be sent to the WHO and other relevant policy-makers as a brief summary report (1-5 pages) and 1-page policy brief (see http://www.cihr-irsc.gc.ca/e/documents/dsen-abstract-en.pdf for an example). We will work with the WHO team to consider submitting this paper to an open-access, peer-reviewed journal for publication (e.g. British Medical Journal).
Timeline (from the point of official approval)
Five business days (March 16, 2020)
Updates provided to the WHO
Daily emails will be sent to the WHO
Funding
Funding will be obtained from the WHO and the Canadian Institutes of Health Research Strategy for Patient Oriented Research Evidence Alliance (https://sporevidencealliance.ca/).
APPENDIX 2 – MEDLINE SEARCH STRATEGY
respiratory tract infections/ or exp bronchitis/ or exp common cold/ or exp influenza, human/ or laryngitis/ or exp pharyngitis/ or exp pleurisy/ or exp pneumonia/ or exp rhinitis/ or exp rhinoscleroma/ or exp severe acute respiratory syndrome/ or exp sinusitis/ or exp supraglottitis/ or exp tracheitis/ or exp whooping cough/
coronaviridae infections/ or coronavirus infections/ or SARS Virus/
(coronavirus* or “corona virus*” or mers or “middle east respiratory syndrome*” or “Severe Acute Respiratory Syndrome*” or SARS or CoV or SARS-CoV or MERS-CoV or 2019-nCoV or COVID-19 or “2019 novel coronavirus disease” or “2019 ncov disease” or “2019 ncov infection” or “coronavirus disease 19” or “severe acute respiratory syndrome coronavirus 2” or “severe acute respiratory syndrome coronavirus 2” or “wuhan” or “sars cov 2”).tw,kf.
(flu or influenza or “respiratory tract infection*” or “respiratory infection*” or bronchitis or “common cold” or laryngitis or pharyngitis or pneumonia or rhinitis or rhinoscleroma or sinusitis or supraglottitis or tracheitis or “whooping cough”).tw,kf.
or/1-4
pc.fs.
exp Infection Control/ or secondary prevention/
exp hand hygiene/ or hygiene/
(prevent* or “respiratory hygiene” or “respiratory etiquette “ or “cough etiquette” or “Hand Hygiene” or “hand wash*” or “handwash*” or “patient isolation” or “quarant*” or “infection control” or “blood safety” or steril* or disinfect* or “contract tracing” or “disease notification” or fumigat* or “personal protective equipment” or triage or “source control” or isolation or “daily monitoring” or surveillance or “waste management” or cadaver or body or corpse or “face mask*” or facemask* or “social distanc*” or housekeeping). tw,kw.
(clean* adj3 (linen or equipment or environment)).tw,kf.
(restrict* adj3 (resident* or patient* or visit* or family or travel* or staff or provider* or employee*)).tw,kf.
personal protective equipment/
Housekeeping, Hospital/
Waste Management/
patient isolation/
triage/
Cadaver/
or/6-17
5 and 18
Long-Term Care/ or exp Nursing Homes/ or Homes for the Aged/ or Assisted Living Facilities/
(“long-term care” or “long term care” or “senior* home*” or “senior* residence*” or “nursing home*” or “old age home*” or “old age residence*” or “home* for the aged”).tw,kf. (48416)
20 or 21
19 and 22
APPENDIX 3 – SYSTEMATIC REVIEW CHARACTERISTICS
APPENDIX 4 – QUALITY APPRAISAL RESULTS FOR SYSTEMATIC REVIEWS AND CLINICAL PRACTICE GUIDELINES
APPENDIX 5 – SYSTEMATIC REVIEW RESULTS



