
Abstract
Spatial neglect is a common and severe cognitive consequence of stroke, yet there is currently no effective rehabilitation tool. Virtual Reality (VR) telerehabilitation tools have the potential to provide multisensory and enjoyable neuropsychological therapies and remotely monitor adherence without the presence of a therapist at all times. In order to inform the development of these tools researchers and industry need to better understand end-user perspectives about these technologies to ensure these are acceptable and user-friendly to ultimately optimize adherence and efficacy. Therefore, this study explored end-user perspectives on the use of self-administered VR telerehabilitation for spatial neglect. We used a mixed-method design including focus groups, self-administered questionnaires and individual interviews with stroke survivors (N = 7), their carers (N = 3) and stroke clinicians (N = 6). End-user perspectives identified clarity of instructions, equipment (cost, available resources) and for some, level of experience with technology as barriers of use. Perceived facilitators of use were performance feedback, engagement and enjoyment, and psychological benefits associated by self-administered VR telerehabilitation. Overall, end-users were positive and interested in using VR telerehabilitation for spatial neglect. These perspectives enabled us to produce practical recommendations to inform future development, enhance engagement and uptake of self-administered VR telerehabilitation.
1. Introduction
Around 20-40% of the 1.2 million stroke survivors currently living in the UK (Stroke Association, 2018) are estimated to have spatial neglect (Ringman et al., 2004; Rowe et al., 2019; Puig-Pijoan et al., 2018). Spatial neglect is a severe neuropsychological syndrome generally defined as a failure to respond to stimuli on the side of the space opposite to the side of the brain lesion. The clinical impact of spatial neglect is substantial with 40% of people showing neglect symptoms even more than a year post-stroke (Nijboer, Kollen & Kwakkel, 2013) and its presence being a major predictor of disability (e.g., Gillen, Tennen & McKee, 2005). Unfortunately, there is no specific recommended rehabilitation for the condition (Azouvi, Jacquin-Courtois & Luauté, 2017; Bowen et al., 2013). Yet, previous research has found that stroke survivors, carers and clinicians identified visual problems as one of the top 10 priorities in stroke research (Pollock et al., 2014).
The fast advancement of affordable, user-friendly and portable virtual reality (VR) technology means that it can be more easily applied in clinical settings (Castelvecchi, 2016). In fact, several VR interventions have been recently introduced for cognitive and/or physical impairments for various conditions, such as Parkinson’s disease (Dockx et al., 2016), Traumatic Brain Injury (TBI; Maggio et al., 2019) and stroke (Laver et al., 2017; Warland et al., 2019). VR enables a user to interact with a virtual environment, using either immersive (e.g. wearing VR headsets) or non-immersive technology (e.g. presents a virtual/computerized environment without being immersed within it). VR presents many advantages when compared to traditional rehabilitation including the ability to create rich sensory environments and replicate real-world situations within safe conditions (e.g. city; Cipresso et al., 2014; Ogourtsova et al., 2017), the ability to boost enjoyment, confidence and enthusiasm levels (Thornton et al., 2005; Pietrzak, Pullman & McGuire, 2014) and facilitate self-administration of rehabilitation (‘telerehabilitation’) while objectively monitoring therapy adherence remotely (Burdea, 2003; Threapleton, Drummond & Standen, 2016). Moreover, telerehabilitation can benefit patients living in remote locations and can be cost-effective when compared to one-to-one rehabilitation (Peretti et al., 2017).
The development of VR rehabilitation for spatial neglect is still in its infancy. To date, studies in spatial neglect have explored both immersive and non-immersive VR including real-world tasks such as navigation and cooking (Ogourtsova et al., 2018; Tobler-Ammann et al., 2017) and visual search tasks (Yasuda et al., 2017; Cipresso et al., 2014). Even though several VR therapies have been introduced for neurorehabilitation, not much is known about the views of stroke survivors, their carers or clinicians regarding their usability and acceptability (e.g., Threapelton, Drummond & Standen, 2016). The aim of this study was to explore the perspectives of end-users about non-immersive, self-administered VR telerehabilitation for spatial neglect. To the best of our knowledge, only one study has explored perspectives of using VR in spatial neglect but only investigated VR use for assessing neglect and only collected data from clinicians (Ogourtsova, Archambault & Lamontagne, 2019). Ogourtsova and colleagues used focus groups and interviews with clinicians and identified a series of barriers and facilitators including equipment (e.g., cost), client suitability (age), personal and institutional factors (e.g. familiarity with VR).
In the present mixed-methods study, we gathered perspectives on the use of self-administered VR telerehabilitation for spatial neglect from clinicians but also, importantly, from stroke survivors and their carers. Working directly with end-users our aims were to 1) identify any facilitators or barriers of use and 2) produce recommendations that may improve future development (Threapleton, Drummond & Standen, 2016) and, ultimately, enhance adherence, efficacy and implementation into clinical practise (Brouns et al., 2018).
2.1 Participants
In line with similar studies (e.g. Ogourtsova, Archambault & Lamontagne, 2019; Lane et al., 2019; Niraji, Wright & Powell, 2018), our sample comprised of 16 participants: seven stroke survivors (mean age = 67.1, SD = 6.8 years old, one female), three partners or carers of stroke survivors (mean age = 51, SD = 30.1 years old, one male) and six stroke clinicians (one male, mean age = 44.7, SD = 12.1 years old). Demographic and clinical data of all participants are presented in Tables 1 and 2.
Demographic and clinical data for stroke survivors.
Carer and clinician demographic data.
All stroke survivors and carers were recruited face-to-face or by email/telephone from local community-led stroke support groups and social media. Two of the carers were partners of stroke survivors who also took part in the study. Six stroke survivors self-reported experiencing spatial neglect in the past or present (e.g., could not see one-half of the television). None of the stroke survivors received any form of spatial neglect rehabilitation at the time of this study. Prior to focus groups, spatial neglect was formally assessed in a separate session at the participant’s home, using paper-and-pencil tests including Behavioural Inattention Test (BIT; Wilson, Cockburn & Halligan, 1987), line bisection task (Rossit et al., 2019) and the paper version of the Broken hearts test (Oxford Cognitive Screening; Demeyere et al., 2015). Five stroke survivors were classified as having neglect as they were impaired in one of the spatial neglect tests (N+). One stroke survivor had recovered from spatial neglect (Nrec) and the other did not show any symptoms (N-; see Table 1 for neuropsychological test scores). The study was approved by the University of East Anglia Psychology ethics committee and all participants provided informed consent.
Six stroke clinicians (mean age = 44.7, SD = 12.1) were recruited from local networks and took part in either individual interviews (N = 3) or a small focus group (N = 3). Experience working in brain injury ranged from 3 to 39 years (mean = 11.2, SD =13.9).
2.2 Procedure
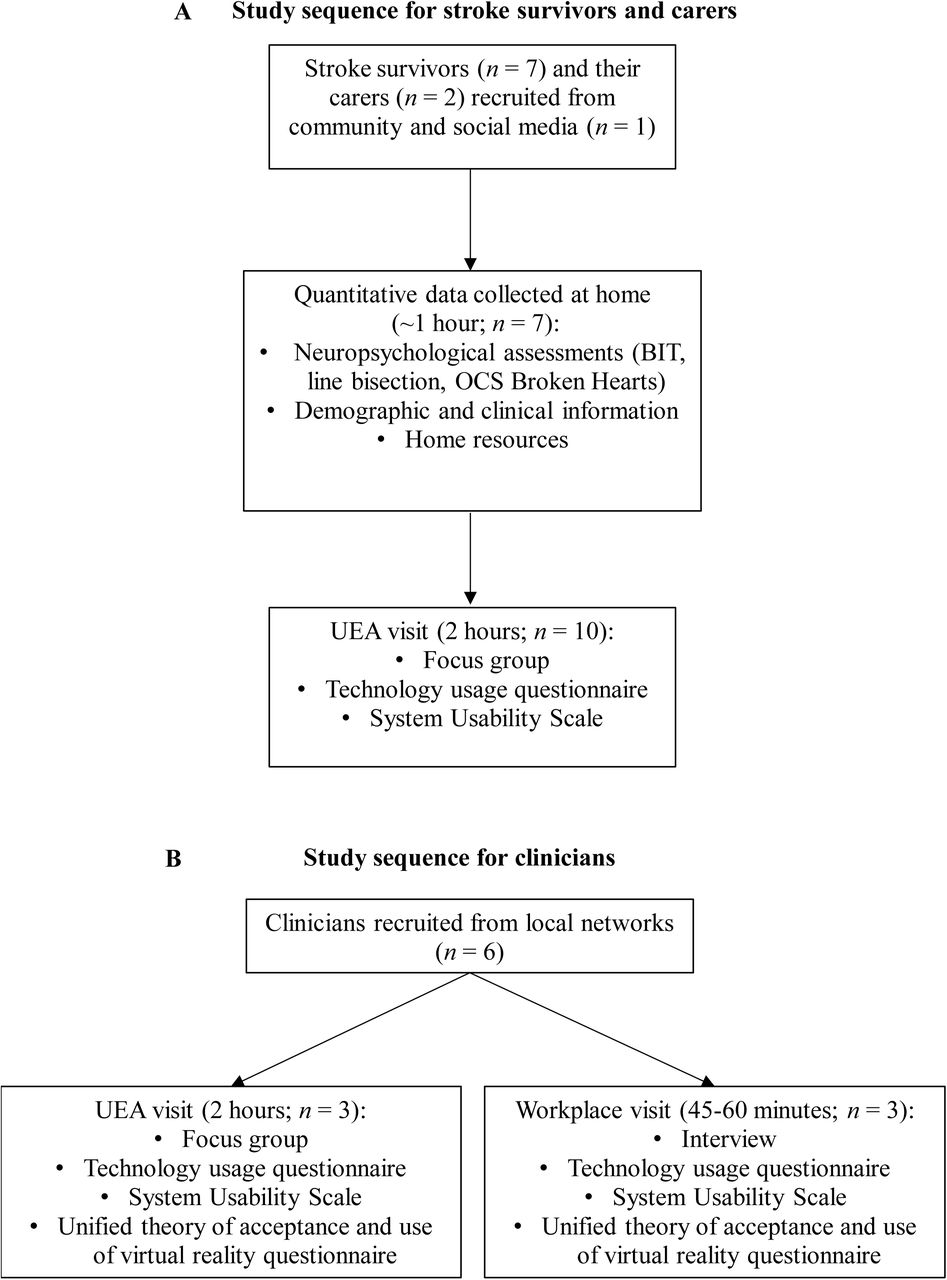
We carried out a mixed methods study using focus groups and semi-structured interviews combined with neuropsychological assessments and questionnaires (see flowchart in Figure 2). Before beginning focus group discussions, the moderator delivered a short presentation about the focus group guidelines (Vaugh, Schumm & Sinagub, 1996), study rationale and VR. Lead author and research associate working on the project (BSc, MSc) with experience of running a previous pilot focus group, conducted all focus groups and interviews. Following this, participants tried (for the first time) non-immersive forms of VR telerehabilitation (see section 2.3) and were encouraged to comment on this. The focus group discussions followed 10 semi-structured questions and unscripted follow-up questions to further explore certain perspectives. Example of questions included: What did you find enjoyable in the virtual reality games? How did you find the feedback you received during the virtual reality games? What do you think about using this equipment and games at home or in clinic? (see supplementary materials for all questions). Individual interviews were carried out with three clinicians who could not attend the clinician focus group following the same procedure as the focus groups. Both focus groups and interviews were audio recorded and transcribed by the lead author.

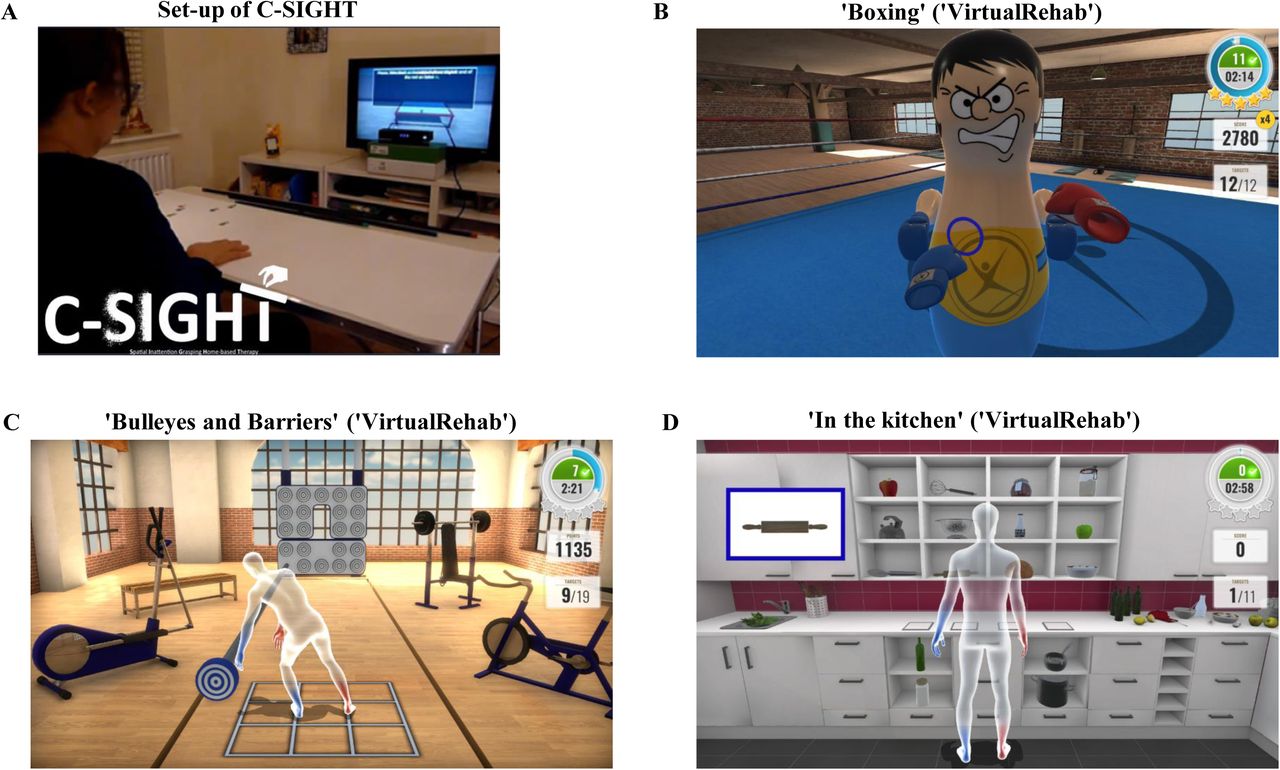
(A) Set-up of C-SIGHT in a home setting, (B) display when using ‘Boxing’, (C) ‘Bulleyes and Barriers’, and (D)‘In the kitchen’ in ‘VirtualRehab’ (by Evolv Technologies).
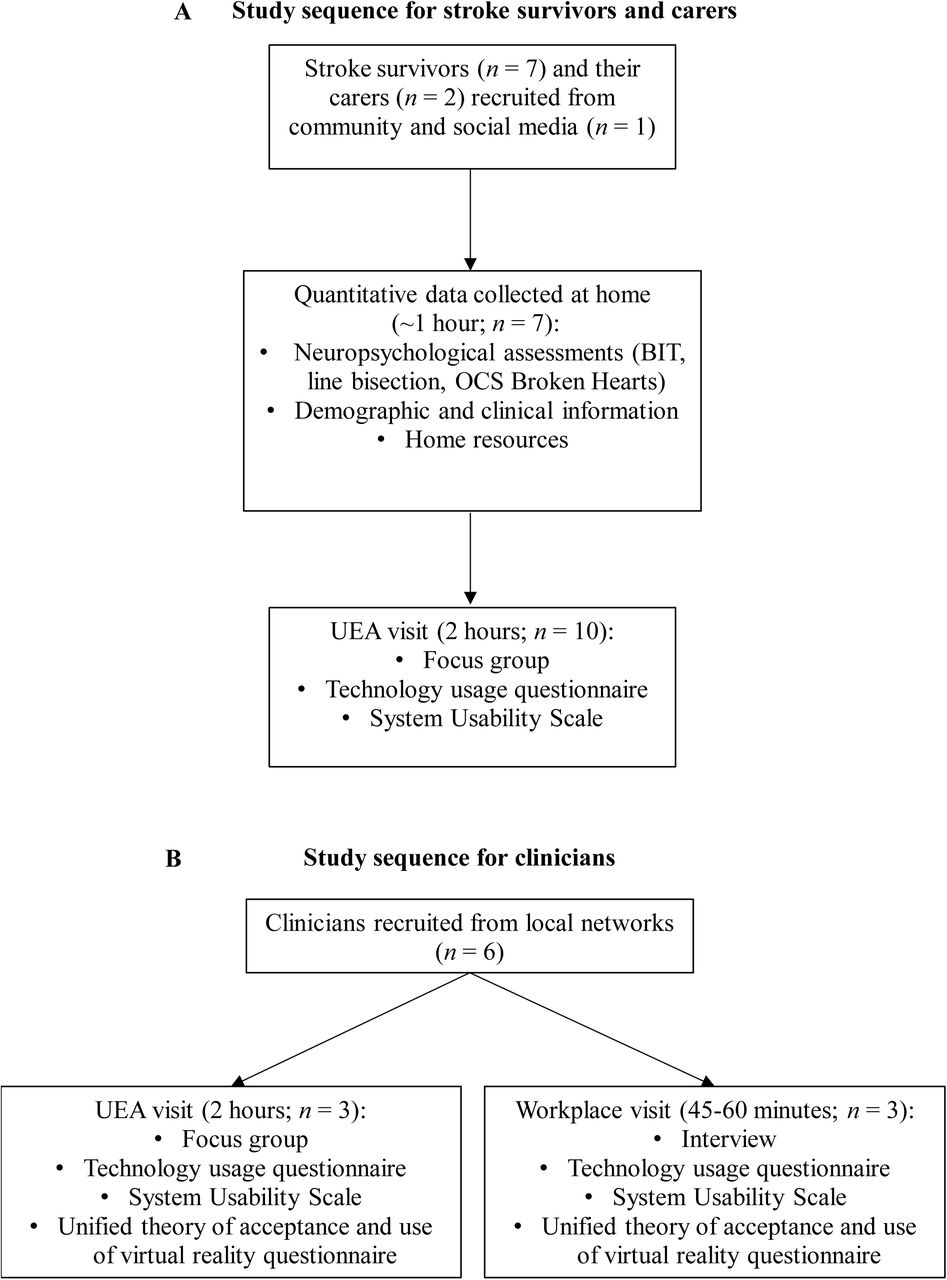
Flowchart of study for stroke survivors and carers (A) and clinicians (B).
Following the focus group/interviews, to measure the usability of the VR telerehabilitation shown, all participants completed the System Usability Scale (which included questions such as ‘I thought the system was easy to use’; Brooke, 1996; Meldrum et al., 2012; Pei, Chen, Wong & Tseng, 2017). Moreover, participants also completed the ‘technology usage questionnaire’ (adapted from Vekiri & Chronaky, 2008) to investigate the frequency and variation of technology used by participants, including previous experience with VR. In addition, to explore the acceptance of using VR in their workplace (Ogourtsova et al., 2019), the clinician group completed the ‘Unified theory of acceptance and use of virtual reality questionnaire’ (Venkatesh, Davis & Davis, 2003). Finally, during the home visit for stroke survivors we collected information about home resources (WiFi, room size, TV size, TV model, table size).
2.3 Self-administered VR telerehabilitation
All participants trialled a novel VR version of our home-based therapy for spatial neglect (Rossit et al., 2019) - computerized spatial inattention grasping home-based therapy (C-SIGHT – Figure 1A). During the focus group, the stroke survivors and carers also trialled three VirtualRehab ‘exergames’ (videogame-like exercise activities developed by Evolv Rehabilitation Technologies) including: ‘Boxing’ (sparring with a virtual boxing partner; Figure 1B), ‘Bullseyes and Barriers’ (hitting or avoiding targets; Figure 1C) and ‘In the Kitchen’ (search task in realistic kitchen layout; Figure 1D). The non-immersive VR was presented on a Samsung MD40B monitor (40-inch) attached to a laptop (HP 15.6 Omen) and used a low-cost and portable motion-tracking sensor (Microsoft Kinect) to measure body movements.
2.4 Data analysis
Focus group and interview data was transcribed using Nvivo (QSR International’s NVivo version 12) by the first author (H.M). The data was analysed using a deductive thematic analysis with a semantic approach (Clarke & Braun, 2014). NVivo software was used to facilitate coding the data. Meaningful themes emerged from the data and were transposed to a coding grid to capture the facilitators and barriers to engagement with the VR telerehabilitation. Codes and themes were discussed by the research team to achieve consensus as to their meaning and/or overlap. A final round of analysis was then performed by author H.M until data saturation occurred across themes. Descriptive statistics were used to summarize quantitative data (e.g. frequency counts). All participants completed all required parts of the study and there were no drop-outs.
3 Results
3.1 Qualitative data
Data collected from focus groups and interviews revealed three major barriers and four major facilitators of using self-administered VR telerehabilitation for spatial neglect. Themes are described below and details of participant perspectives are shown in Table 3.
Qualitative data. Details of stroke survivors (SS), carer (C) and clinician (Clin) perspectives for each theme.
Clarity of instructions (barrier)
All participants identified the length and format of instructions as important barriers of use in VR telerehabilitation. Lengthy instructions could be problematic for stroke survivors who experienced fatigue or cognitive impairments (“My concern would be people with attentional deficits” Clin4; Table 3). Instead of text alone, one clinician and stroke survivor suggested providing an option for users to have pictorial or video instructions.
Level of experience with technology (barrier)
Lack of experience or confidence with technology emerged as a potential barrier for two stroke survivors and one clinician. This was a particular concern as users might experience a technical problem which would worry them (“different generations aren’t used to using motion sensitive software” SS9). Similarly, two clinicians felt VR would be particularly desirable for younger clients, but one clinician noted that if implemented into clinical practise this technology would become more familiar and acceptable with older clients.
Equipment (barrier)
Some stroke survivors (3 out of 7) were concerned that the motion-tracking camera positioned above their television might pose a security risk and be an “intrusion” (SS9). In addition, one stroke survivor, carer and clinician felt that VR telerehabilitation would be less accepted and user-friendly if it was difficult to set-up (“if it becomes difficult to set up all the other benefits {…} disappear” SS5). Furthermore, four stroke survivors identified expensive equipment as a barrier of use, since not everyone would own or could purchase a laptop or television. Community and acute stroke clinicians (3 out of 6) were concerned that stroke survivors may not have adequate resources in their homes to accommodate the VR equipment (e.g. a television, space, Wi-Fi). Nevertheless, when asked directly about the equipment they trialled, all stroke survivors said they would be happy having the equipment in their homes.
Performance feedback (facilitator)
All participants believed that using VR telerehabilitation for spatial neglect would provide more feedback than conventional therapies. Stroke survivors and carers believed clear progress feedback (visual or auditory) would motivate the user and make rehabilitation more engaging. For example, SS3 found auditory prompts (e.g., cheers, claps) engaging by reassuring he was completing the therapy correctly (“I like being cheered”). However, one stroke survivor preferred discrete auditory prompts and feedback. Additionally, one carer thought it would be interesting to monitor their partner’s progress using the feedback from VR.
Engagement and enjoyment (facilitator)
One stroke survivor felt that ‘gamification’ of a therapy would increase their engagement, enjoyment and “increase the amount of time I spend on rehabilitation” (SS3). Two stroke survivors and one carer believed that adding a competition element to rehabilitation (either against the software, carer or other users) would increase their enjoyment.
Psychological benefits (facilitator)
Four stroke survivors shared the negative feelings they felt after their stroke (e.g. “I was dependent on somebody, I had lost everything” SS5, “a lot of things in your life, your world have been taken away from you” SS9). C10 thought self-administering rehabilitation would enable stroke survivors to go at their own pace. As a result, one stroke survivor, carer and clinician thought the user might feel more competence and “ownership” (Clin5) over their rehabilitation since they could carry it out independently. Moreover, two stroke survivors and one carer thought this would increase positive feelings, such as confidence and independence (e.g. “made me feel a lot better about myself” SS5).
Meeting an unmet need (facilitator)
When asked their opinion on using VR for rehabilitation, two stroke survivors thought it was an “excellent idea” (SS3, SS4) and “very good idea” (SS5). Stroke survivors (2 out of 7) and carers (2 out of 3) believed a self-administered VR telerehabilitation for spatial neglect would be more convenient and accessible. One stroke survivor noted that home-based VR telerehabilitation would be especially beneficial for those who had mobility issues. Moreover, all clinicians recognised the unmet need for spatial neglect rehabilitation. In addition, they also recognized the benefits of developing a self-administered VR telerehabilitation for spatial neglect with the capabilities of objectively measuring adherence remotely.
3.2 Quantitative data
3.2.1 System Usability Scale (SUS)
All participants gave an adequate SUS score regarding the VR telerehabilitation tools for spatial neglect: stroke survivors (62; ok), carers (74.2; good) and clinicians (67.5; ok). This indicates that the self-administered VR telerehabilitation was acceptable for all participants (Bangor, Kortum, & Miller, 2008; Bangor, Kortum & Miller, 2009).
3.2.2 Technology-usage questionnaire
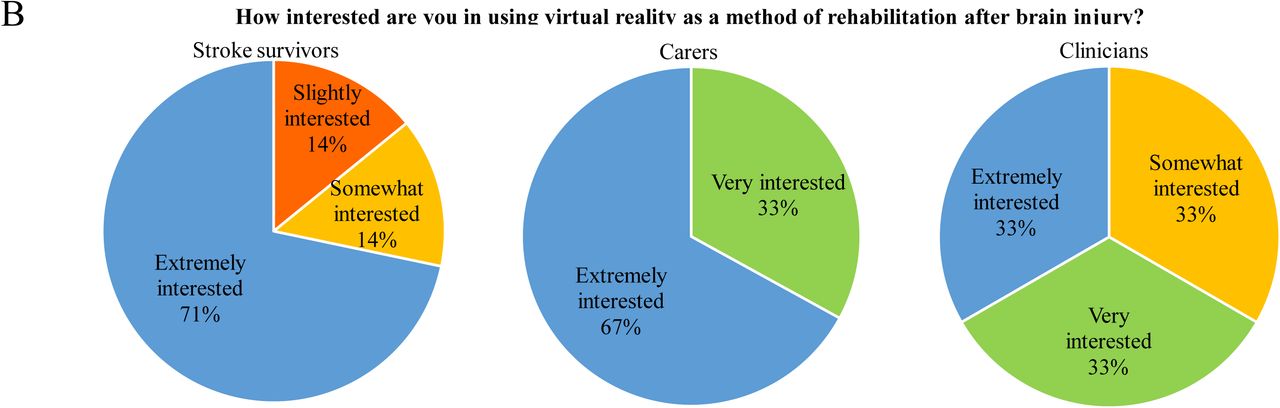
All but two stroke survivors (SS7, due to severe neglect symptoms) reported owning a mobile phone or smartphone. Clinicians and carers reported using a laptop/computer daily or 2-4 times a week, whereas stroke survivors’ computer usage varied from daily to rarely. Only one stroke survivor played computer games daily. All stroke survivors and the majority of clinicians had never tried VR before the present study (see Figure 3A). More than 67% of stroke survivors and carers were extremely interested in using VR in their rehabilitation and 66% of clinicians were very interested (see Figure 3B). All participants were mostly confident that they could use VR for rehabilitation (see Figure 3C).
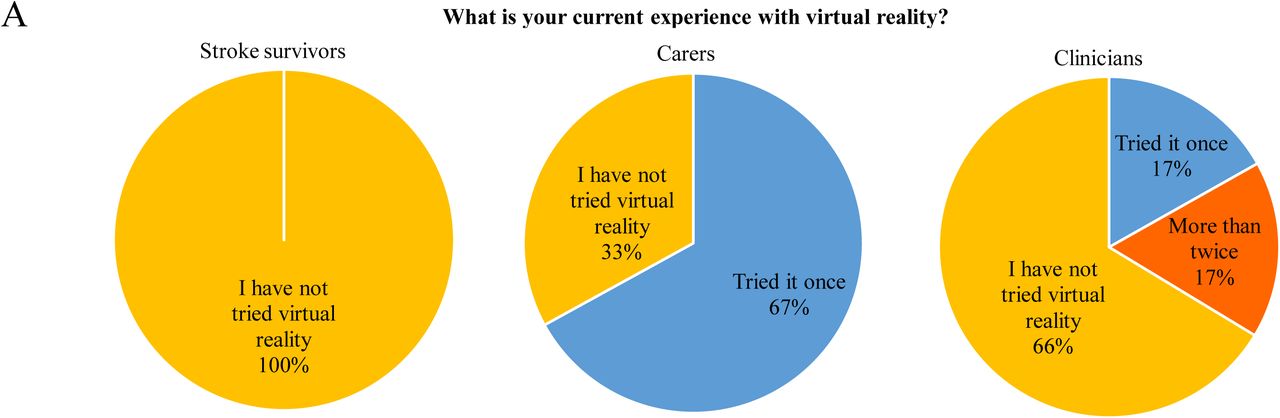
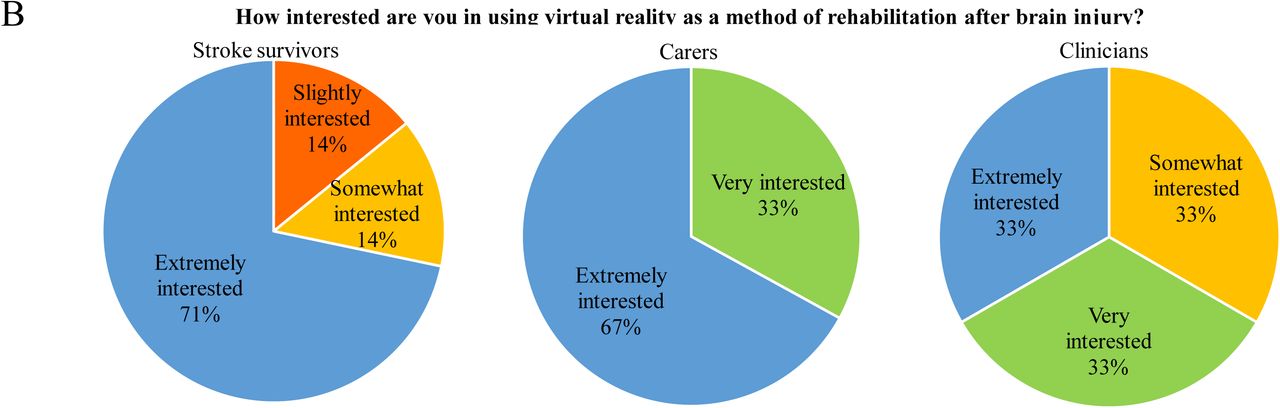
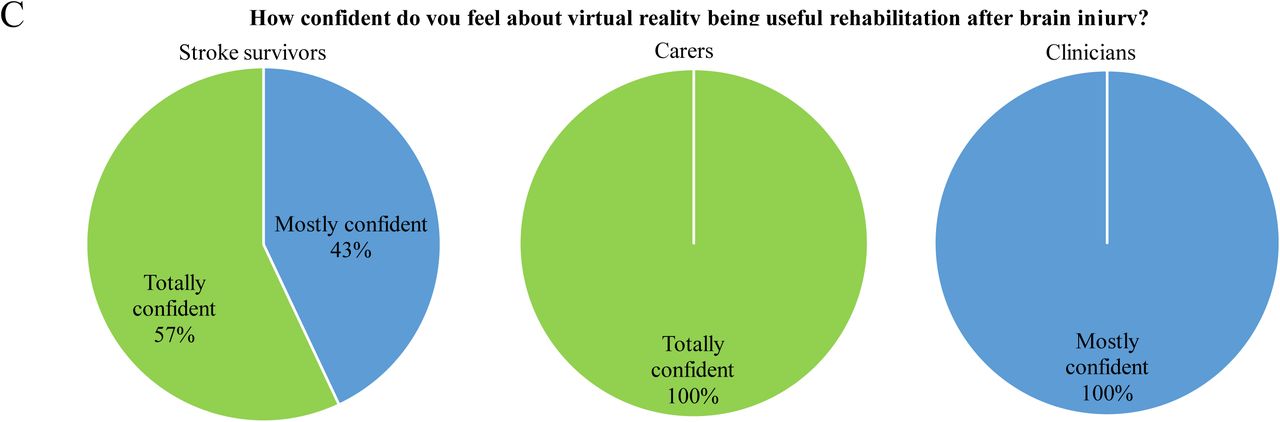
(A) What is your current experience with Virtual Reality?, (B) How interested are you in using virtual reality as a method of rehabilitation?, (C) How confident do you feel about virtual reality being a useful rehabilitation after brain injury?
3.2.3 ‘Unified theory of acceptance and use of virtual reality’ for spatial neglect questionnaire
All clinicians (except one) agreed that VR rehabilitation could improve their work performance and effort (see Q1-5 in Fig.4). Clinician’s reported mixed views on whether members of their organization would support the use of VR rehabilitation (see Q6-9 in Fig.4). The majority of clinicians (80%) reported having adequate resources and knowledge to use VR rehabilitation in clinical practice (see Q10-16 in Fig.4). Finally, most clinicians (67%) agreed that they intend to use VR rehabilitation if available in the next year (see Q17 in Fig.4). Notably, one clinician noted on questionnaire that they would plan to use VR rehabilitation in the next 12 months “if I had the support from management and time to use”.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
‘Unified theory of acceptance and use of virtual reality’ for spatial neglect clinician questionnaire’
Home resources
All stroke survivors had a television larger than 32 inches and Wi-Fi which would enable them to run VR telerehabilitation from their homes. Moreover, all stroke survivors had an average of 5.3ft in front of their television which would allow them to use the motion tracking sensor to record body movements.
3. Discussion
To the best of our knowledge, this is the first study to explore perspectives on self-administered VR telerehabilitation for spatial neglect with stroke survivors, carers and clinicians. We identified three barriers and four facilitators of using self-administered VR rehabilitation for spatial neglect which should be considered in future studies to increase its acceptability and usability. Importantly, this mixed-methods design revealed that end-users were accepting and willing to use self-administered VR telerehabilitation for spatial neglect.
Focus groups and interviews identified the need for short instructions and use of multiple formats (e.g. pictures, large font; similar to Wentink et al., 2019). This is important since those using self-administered VR telerehabilitation for spatial neglect (e.g. C-SIGHT) may experience difficulty with functional reading (associated with increased neglect severity; Galletta et al., 2014). Additionally, considering around 30% of stroke survivors are affected by aphasia (impaired language and communication function; Dickey et al., 2010) the provision of pictorial and/or auditory instructions would mean these stroke survivors would not be excluded from using self-administered VR telerehabilitation for spatial neglect.
Interestingly, it seemed two clinicians and two stroke survivors had an expectation that those with little experience with technology or of older age are not interested in using VR (e.g. Farrow & Reid, 2004; Ogourtsova et al., 2019; Wentink et al., 2019). Indeed, one stroke survivor with less technological experience did express a concern that VR telerehabilitation would not be accepted if it was difficult to set-up. However, most of the sample (many reporting little technological experience) did not acknowledge this as a barrier. For example, one stroke survivor (SS3) and carer (C2) felt confident about setting up the equipment since they had previous experience (i.e, they used a Wii Fit). In fact, more than half of the sample were very interested and felt confident in using VR telerehabilitation and rated its usability as acceptable, regardless of their technology usage/experience.
Participants valued the features facilitated by VR equipment (e.g. remote monitoring of adherence, feedback) and would be willing to use it in their homes. However, some stroke survivors believed user acceptance could be affected by the risk of security breaches and the presence of the motion-tracking camera in their home (e.g. aesthetics; Threapleton, Drummond & Standen, 2016). In this study, our sample had resources in their homes to support self-administered VR, nevertheless it is important to consider this since the other users’ homes may not have these resources due to cost (e.g. large TV). Therefore, changes may have to be made (e.g. move furniture/items) to accommodate the equipment, which may not be acceptable or feasible to the user (e.g. if they use assistive equipment; Threapleton, Drummond & Standen, 2016; Mountain, Wilson & Eccleston, 2010).
Previous findings have found that clinicians report that the feedback from VR is beneficial in motor learning principles and increasing therapy usage (Schmid, Glassel & Schuster-Amft, 2016; Finley and Combs, 2013). Similarly, our study found feedback provided by self-administered VR telerehabilitation (e.g. auditory prompts, visual progress) was seen as a major facilitator of use (e.g. Burdea, 2003). One stroke survivor felt feedback offered by self-administered VR telerehabilitation would increase the enjoyment and engagement while carrying out “ordinarily boring” (SS3) exercises/tasks. Among feelings of engagement and motivation, participants believed users might feel an increase in competence, confidence, independence and ownership from using self-administered VR telerehabilitation. Farrow and Reid (2004) found similar results with stroke survivors who felt VR enabled them to engage in activities they could no longer do, increasing feelings of competence, control, and positive feeling of self (Farrow & Reid, 2004; Pallesen et al., 2018). Considering one-third of stroke survivors report experiencing symptoms of post-stroke depression (Stroke Association, 2018; Hackett et al., 2014), this is an important perceived benefit of using VR telerehabilitation.
Stroke clinicians recognised that there was a need for a rehabilitation for spatial neglect, especially one with remote monitoring/accessibility to user performance facilitated by VR (Burdea, 2003; Ogourtsova et al., 2019). In line with this, stroke survivors and carers believed that the self-administered aspect of VR telerehabilitation would increase the accessibility of rehabilitation for spatial neglect. Stroke survivors in this study believed offering self-administered VR telerehabilitation to stroke survivors after discharge could help those with decreased mobility and increase their psychological wellbeing. This is an important perceived benefit since around 45% of stroke survivors report feeling abandoned after discharge (Stroke Association, 2018). Reflecting on one carer’s comments on convenience, offering self-administered VR telerehabilitation for spatial neglect at home could reduce the cost and time for carers (Tindall & Huebner, 2009).
We collected perspectives from a multidisciplinary group of stroke clinicians (occupational therapists, healthcare assistant, physiotherapist and clinical psychologist). Previous research has suggested the use of a VR rehabilitation is influenced by the clinician’s current technology experience (Burdea, 2003). Although our clinicians reported a low to moderate technology usage, they were open and positive about using VR telerehabilitation and believed it could improve their performance during clinical practice in line with previous studies (Ogoutsova et al., 2019). While most clinicians had adequate resources to support VR telerehabilitation usage, clinicians working in an acute setting (e.g. hospital) anticipated more difficulty since there were limited resources to facilitate VR use (e.g. lack of working computers, space, television screens). Facilitating conditions such as these are a powerful predictor of a clinician’s intention to use a new technology (Liu et al., 2015) and therefore are an important factor to consider when planning implementation of VR telerehabilitation into clinical practice. Perspectives collected from our multidisciplinary group are promising indications that stroke clinicians within different settings would be willing to implement self-administered VR telerehabilitation for spatial neglect with their patients.
Some studies have explored clinician perspectives on VR rehabilitation for upper limb training (Schmid, Glassel & Schuster-Amft, 2016), exergames (Nguyen et al., 2019) and immersive games (Farrow & Reid, 2004). However, few (e.g. Pallesen et al., 2018) benefit from exploring perspectives from both clinicians and stroke survivors. Moreover, despite the emergence of using VR rehabilitation interventions for spatial neglect (e.g. Ogourtsova et al., 2018; Tobler-Ammann et al., 2017; Yasuda et al., 2017; Cipresso et al., 2014) few studies qualitatively explore perspectives end-users. The current study used a mix-methods which offered a holistic approach (Klinke et al., 2016) to explore stroke survivor, carer and clinician’s perspectives, whilst objectively measuring factors (e.g. neglect, stroke severity, technology usage, resources) which might influence perspectives.
However, the current study has limitations. Due to time constraints only one focus group was held with clinicians. This could be considered a limitation since one large focus group with all six clinicians may have facilitated deeper exploration of ideas and opinions with others (Folch-Lyon & Trost, 1981). Despite our relatively small sample size (albeit in line with sample sizes of similar studies; Lane et al., 2019; Ogourtsova et al., 2019; Pallesen et al., 2018; Niraji, Wright & Powell, 2018), we were able to collect the personal perspectives of various end-users (stroke survivors with and without spatial neglect, carers of different ages and multidisciplinary stroke clinicians). Moreover, our findings are both original (e.g. first to explore perspectives on self-administered VR telerehabilitation for spatial neglect) and consistent with previous studies (e.g. Ogourtsova et al., 2019).
Future studies should carry out a usability study to test the equipment and set-up of self-administered VR telerehabilitation for spatial neglect in stroke survivor’s homes (e.g. Warland et al., 2019). This would produce both ecologically valid and constructive feedback on the feasibility and acceptability of using self-administered VR telerehabilitation in user’s homes. Additionally, there is a need for more qualitative and mixed methods studies exploring stroke survivor, carer and clinician perspectives on both non-VR and VR rehabilitation techniques for spatial neglect. Identifying factors which motivate and engage stroke survivors with spatial neglect provides us with a better understanding on how to increase therapy adherence and enjoyment.
Based on the perspectives from end-users in this study, we have produced some practical recommendations for future development of self-administered VR telerehabilitation for spatial neglect. To address concerns regarding user instructions we recommend using short text presented gradually and providing a choice of format for users (e.g. pictorial, written and/or auditory). Secondly, all efforts should be made to reduce the volume, complexity of equipment used (such as, using existing equipment in participant’s homes; e.g. television). Concerns could be reduced by labelling equipment (including cables), providing a clear, comprehensive demonstration of set-up and video or step-by-step instructions (with pictures). Embedding built in support (e.g. ‘help’ button, contact number) and online forum for users to ask each other questions are also possible steps to take. Thirdly, security concerns can be reduced by ensuring transparency of the use of each piece of equipment and recommending users switch off motion sensor cameras when not in use. Finally, the user should be provided with a choice to personalise their telerehabilitation when possible, such as providing a choice of visual or auditory feedback and music.
3.1 Conclusion
This mixed methods study identified that the acceptability of self-administered telerehabilitation was determined by the length and format of instructions. Additional barriers were the potential lack and cost of available resources for stroke survivors and acute setting stroke clinicians, which would facilitate usage of self-administered VR telerehabilitation for spatial neglect. Overall, stroke survivors, carers and clinicians were accepting, interested and confident about using self-administered VR telerehabilitation regardless of their level of technology experience. Potential psychological benefits were identified, such as an increase in independence and confidence, which were associated with motivating and engaging feedback provided by VR.
Future research on VR rehabilitation for spatial neglect should incorporate end-user perspectives to improve the acceptability and engagement of interventions. Perspectives collected using this mixed-methods design with three groups of end-users has enabled us to produce practical recommendations for future development of VR telerehabilitation post-stroke. It is hoped these recommendations may improve future development (Threapleton, Drummond & Standen, 2016) and increase user enjoyment and engagement with VR telerehabilitation.
Data Availability
N/A
Declaration of interest statement
The authors report no declaration of interest.
Acknowledgements
We would like to thank all the stroke survivors, carers and clinicians for their useful comments and kind cooperation during this study. This work was supported by the University of East Anglia Innovation Proof-of-Concept Fund 2017-2018.
References



