
Abstract
Background Limited health information and education about female genital mutilation (FGM) risks in at-risk children, especially in prevalent societies in Tanzania, hinder breaking the cycle, highlighting the need for targeted interventions. This year-long study analyzed the impact of educational interventions on raising awareness of FGM among young adults aged 15 to 19, promoting community discussions, and intergenerational abandonment, in the Chamwino district, Dodoma region, Tanzania.
Methods A mixed-methods community-based cross-sectional explanatory sequential design was conducted from April 2023 to March 2024. A completed follow-up sample of 452 participants from hospitals and schools evaluated the impact of educational interventions. Content analysis of 10 interviews triangulated findings. SPSS v25 provided descriptive and inferential statistics. Paired t-test, chi-square, prevalence ratios, and logistic regression (p < 0.05, 95% CI) assessed variable significance accordingly.
Results 7.3% self-reported FGM, 16.6% observed in labor wards. Adequate awareness increased from 1.3% to 14.6%, p < .001. 96.7% knew FGM was harmful, 95.8% desired its abandonment. Content analysis yielded three themes: the hidden system, blood and lies, and intergenerational revolt.
Conclusion FGM persists in Chamwino, shifting to early childhood to avoid legal consequences. The study raised awareness, changed attitudes, and encouraged community discussion. However, whether these changes will reduce FGM over generations remains uncertain, necessitating ongoing sensitization and evaluation.
Introduction
Young adults can analyze, decide, and hold attitudes toward societal events [1]. Tanzania sees children as the nation of tomorrow, inheriting traditions like FGM that can undermine social dignity [2–4]. Cultures restrict their self-defense and decision-making against FGM [5], which has affected over 230 million girls and women in 31 countries for 2,000 years, mainly in Africa [6]. FGM is common in Tanzania, varying by society. Its prevalence among reproductive-age women is 8% [7], ranking it 23rd in the world [8]. Education and laws have reduced FGM, but it remains prevalent in rural areas, now shifting to early childhood [8,9].
In mainly affected societies like Dodoma, interventions are limited and mainly target adults, neglecting at-risk children who could abandon FGM if educated early. These children are less attached to traditions, and conflicting ideas about FGM in childhood can oppose participation in adulthood. Little is known about children’s awareness and attitudes toward abandoning FGM, leading to fewer targeted interventions and the need for focused research. Understanding their views can guide global and Tanzanian policies, supporting SDG 3. Educating children about FGM’s harms can empower resistance and shift community attitudes. A year-long study in Chamwino assessed the impact of an education campaign on 15-19-year-olds, influencing both individual and community perspectives on abandoning FGM.
Methods
Study design
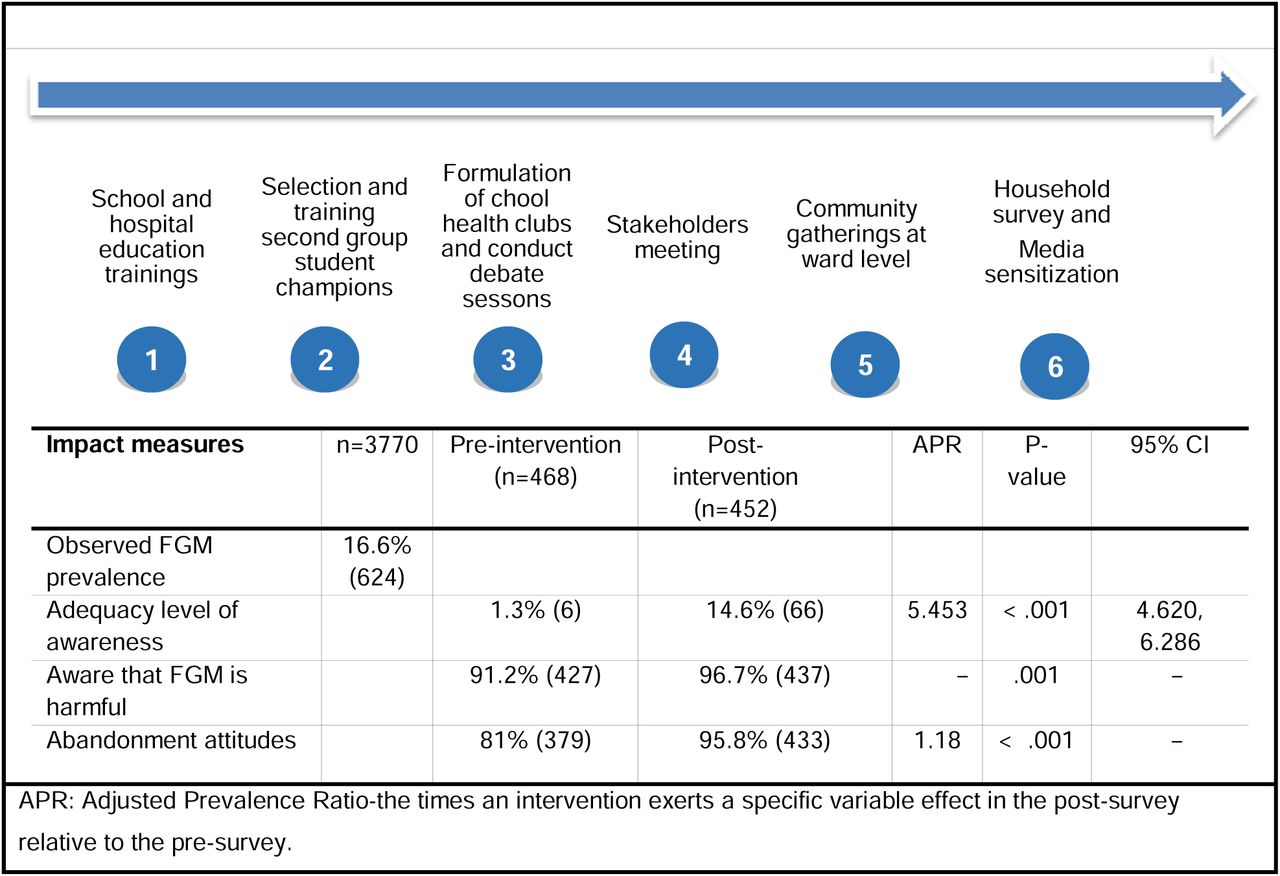
This study used a community-based interventional design with mixed methods to evaluate an educational program increasing FGM awareness among young adults (15-19) in Dodoma, Tanzania, from April 2023 to March 2024. The mixed-methods, explanatory sequential approach consisted of two phases: a cross-sectional, pre-post evaluation quantitative survey in schools and hospitals, measuring awareness, attitudes, and intentions to abandon FGM, and a qualitative phase involving interviews to explore the findings. The intervention featured a multi-component educational campaign, including community teaching sessions. Focused on young adults as future decision-makers, the study aimed to influence community attitudes against FGM, with broader community engagement also targeted. Study phases are outlined in Table 1.
Setting and Context
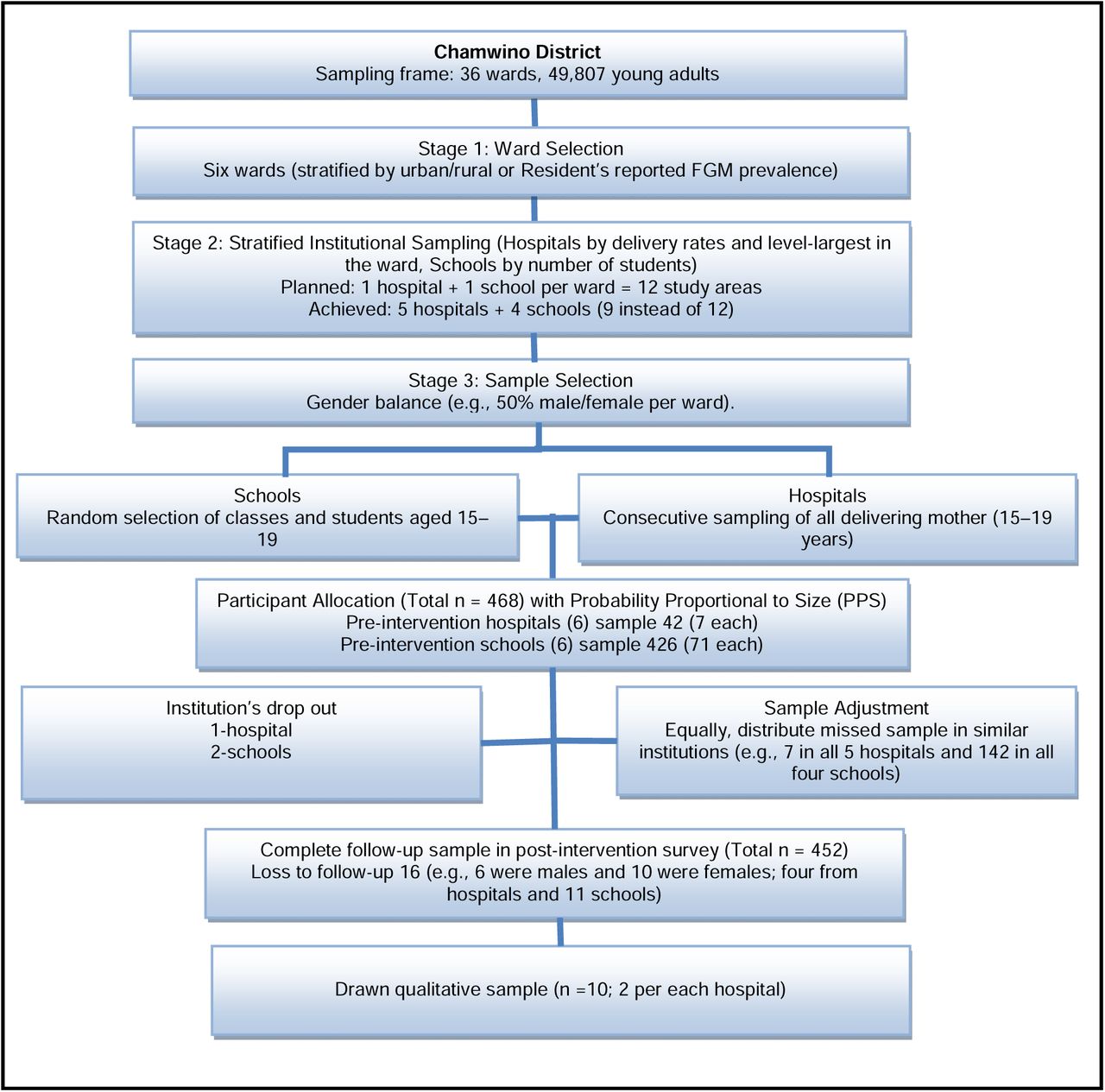
Tanzania’s 2022 population was 61.7 million, with Dodoma at 5%, or 3,085,625 people, including 486,176 in the Chamwino district [10]. Dodoma has the second-highest FGM rate (47%), and 18% of women of reproductive age [7]. Indigenous and migrant tribes like the Gogo, Sandawe, Burunge, Rangi, and Maasai practice FGM. Though FGM shows a decrease in Dodoma [7], it remains secretly widespread, requiring ongoing efforts. Chamwino, with 36 wards, 107 villages, and 820 hamlets, is primarily inhabited by the Gogo, the region’s dominant tribe and the third-largest in Tanzania, who are also the leading FGM practitioners, yet with limited abandonment information [11,12]. We selected six wards stratified by urban/rural and on-the-ground FGM prevalence, based on budget, time, accessibility, and proximity to hospitals and schools, aligning with the scattered nature of the wards. Each ward aimed to have one hospital and one secondary school, but some lacked either, resulting in a total of five hospitals and four schools being studied (Table 2).
Interventions
Literature related to FGM prevalence, interventions, perception, barriers, and gender roles [13–20], framed this study’s activities. The evaluation team validated the study activities and the training manual. The interventions used a health-risk education approach, involving champions and engaging the community through social gatherings, stakeholder meetings, school, household and hospital training, students’ clubs, debates, and media campaign. The first group facilitators, 15 ‘champions’ from seven social groups—health workers, teachers, local leaders, religious leaders, elders, traditional birth attendants, and community health workers—organized meetings, helped with data collection, and led training in their areas. An 11-member evaluation team, including the two first authors, one from each champion group, a student, and a police officer, designed, validated, supervised, and sustained the activities.
All interventions were ward-based due to Chamwino’s dispersed geography. Initially, school training stratified 737 students by gender for discussion. Later, 35 students became second group champions, working with teachers to form health clubs and prepare debates. These clubs in one school met monthly for 3 months on FGM, with health workers, traditional birth attendants, police, and gender desk reps discussing health risks, birth issues, laws, and reporting. Each club had 35 students, totaling 210 attendances. Debate sessions occurred three times at one school. Over 900 students received FGM education across four schools. Hospitals held thirteen training sessions for 246 mothers in labor wards and clinics.
Student champions led the social gatherings and household surveys under teacher and researcher supervision, promoting ownership, changing agent role, and message assimilation. In Tanzania, with an average household size of 5 [7], we targeted 20 households for 100 people, based on a feasibility-driven estimate of available resources and logistics, rather than statistical power in one month. A team of 15—2 researchers, three teachers, and 10 students in 5 groups—planned visits, each lasting 1 hour per household and area. Each group aimed to visit at least four households in Chamwino ward to reach 100 participants, accompanied by a local government representative. During each visit, all present family members, including adults and children, participated in a standardized educational session on health consequences and benefits of abandonment. Language was adjusted to facilitate dialogue and ease discomfort. Informed consent was obtained from the household head or senior adult, and orally from other members. Forty-six houses were surveyed, teaching 104 residents (41 adults and 63 children). Children counted were at least 12 and able to understand.
Two gatherings in Chamwino and Mlowa attracted over 500 people. To reduce bias, participants privately indicated ownership: 77.9% (household survey) and 83.6% (423/506 respondents) at gatherings said yes. Including an evaluation (92.5%), an average of 84.7% felt ownership. The campaign reached over 1,700 people. A local radio program covered the project’s purpose and FGM plans. The team assessed impacts and set sustainable goals. Fig 1 shows study activities and impact measures.

Training manual
The manual, based on literature [7,19–22] and validated by the evaluation team, trained study assistants, champions, and participants on FGM’s meaning, evolution, prevalence, types, causes, health risks, and abandonment strategies. Nurse-midwives were trained to categorize FGM types, and each champion received a copy for reference.
Sampling and recruitment of participants
The study used multi-stage cluster sampling with stratified institutional recruitment. The initial sample was 466, increased to 468 for equal ward representation (78 each). It aimed to recruit 426 from schools and 42 from hospitals, with equal gender balance (Table 2). The 468 sample represented 49,807 young adults in Chamwino district [10]. The health centre (HC) in Itiso ward exhibited low delivery rates for young adults (< 7 per month) and was excluded. Schools in Mlowa and Mpwayungu were excluded because no samples were collected during holidays. Missed samples were evenly distributed and adjusted during analysis. After the intervention, 452 follow-ups were completed, with 16 (3.4%) losses. Ten purposive in-depth interviews, aligned with a sample of 5-25 participants in a phenomenological design of lived experiences [23]. Interviews stopped at the 10th interview after reaching saturation at the phenomenon level, guided by Saunders et al [24]. Participants from various ward-hospitals shared a common experience but offered diverse data. Interviews were conducted once. Four eligible participants refused due to fear. Fig 2 illustrates the multistage cluster sampling and recruitment process.

Study variables
Primary dependent variables are FGM prevalence, awareness levels, awareness of health risks, and desire to abandon. Predictor variables include participant demographics, such as age, sex, ward, interview location, education, years in the community, and tribe.
Eligibility of hospitals, schools, and participants
The initial hypothesis was that schools had about 10 times more eligible young adults than hospitals. Probability Proportional to Size ensured larger populations like schools contributed proportionally more (10 times), with all settings and participants having an equal probability, resulting in no under- or overrepresentation. Hospital inclusion required young adult delivery rates of ≥7/month, while schools, ≥71 students aged 15-19. Quantitative criteria included living in the district for at least a year and not graduating during the study. Qualitative: only young mothers in hospitals with positive FGM status, willing to share experiences and had reported awareness of FGM continuation, were interviewed. Interviews prioritized depth over breadth, aiming to understand the inner world of the experience itself from those who lived it. We focused on their physical, psychological, and social impacts, believing these individuals could provide rich, firsthand insights into the practice and its community effects.
Data collection, instruments, and techniques
Literature on FGM prevalence, health risks, and abandonment [4,7,19,21,22,25], guided the data collection instruments, all in Swahili for participants’ comfort. The evaluation team initially validated them. The quantitative tool was pre-tested at 10% (47) in one school. We conducted two hospital interviews to validate the qualitative tool. All pre-testing findings refined the tools and were excluded from the main study. Two quantitative tools were developed—the first evaluated intervention impacts, pre- and post, with a 10-month gap. To reduce conformity, social desirability bias, and response tampering, while boosting privacy, comfort, and focus during sensitive discussions, students were spaced 1 meter apart in open areas to complete questionnaires. Data collection used interviewer- and self-administered questionnaires at participants’ convenience, with accuracy verified before departure. The second tool assessed FGM prevalence and types among all delivering mothers. The qualitative tool explored experiences and life with FGM among positive young adult mothers. The first two authors conducted separate face-to-face interviews in private hospital wards. They were recorded using audio, field notes, and participant verification.
Data analysis
SPSS v25 generated univariate and multivariate statistics. All comparisons excluded loss to follow-up. Paired t-tests assessed changes in awareness levels. Prediction of binary and multinomial outcomes used adjusted logistic regression (p < 0.05; 95% CI). McNemar assessed changes in paired binary outcomes (e.g., pre- and post-survey). Chi-square tested associations of independent outcomes. Adjusted PR (Modified Poisson regression) measured intervention impacts. Twenty-three FGM questions evaluated awareness; scores as <50 inadequate, 50-75 moderate, 76-100 adequate [26]. The first two authors familiarized, transcribed verbatim, and manually coded five interviews each in the research field daily, following the six-step inductive thematic analysis [27]. The two then refined the themes together. The data sets and analyses were discussed and validated by all authors. The manuscript was drafted following the COREQ standards for transparency [28].
Results
The results include data from pre- and post-surveys, hospital FGM statistics, and key informant (KI) interviews. FGM remains prevalent in the Chamwino community, often done secretly. Discussing its existence is taboo, hindering reporting. The study raised awareness about FGM risks, engaged social groups, and encouraged open discussion. Participants showed positive attitudes toward abandoning FGM, but behavioral change couldn’t be measured in a year. Many expressed fear and lack of power as main barriers, despite wanting to break the cycle.
Post-survey participants’ characteristics
Table 2 details the three characteristics (sex, ward, and ward type), while Table 3 covers others. Most participants came from Chamwino ward (25.4%, 115). Two wards were semi-urban (27.2%, 123) and four remote (72.8%, 329). Out of 452 complete follow-up samples, 50.4% (228) were males, 49.6% (224) females. Most (93.1%, 421) had secondary education, and students (91.6%, 414). Of the 38 in hospitals, 28 were FGM positive. Median age was 17 (range 15-19), and median years in the community were 16 (range 1-19). Of 33 tribes, the majority were Gogo (57.5%, 260) (Table 3).
FGM prevalence
About (7.3%, 17) of females self-reported FGM in pre-survey, while (16.6%, 624) were observed in 9 months. Young adults contributed (27.1%, 510) of all deliveries and (25.3%, 158) of FGM prevalence. FGM prevalence in young adults was (31%, 158). Most FGM cases were from Haneti HC (43.3%, 270). Only types II and I were practiced, with type II being predominant at 97.4 % (608). The Gogo tribe constituted most of the FGM prevalence (73.6%, 459) (Table 4).
FGM awareness level
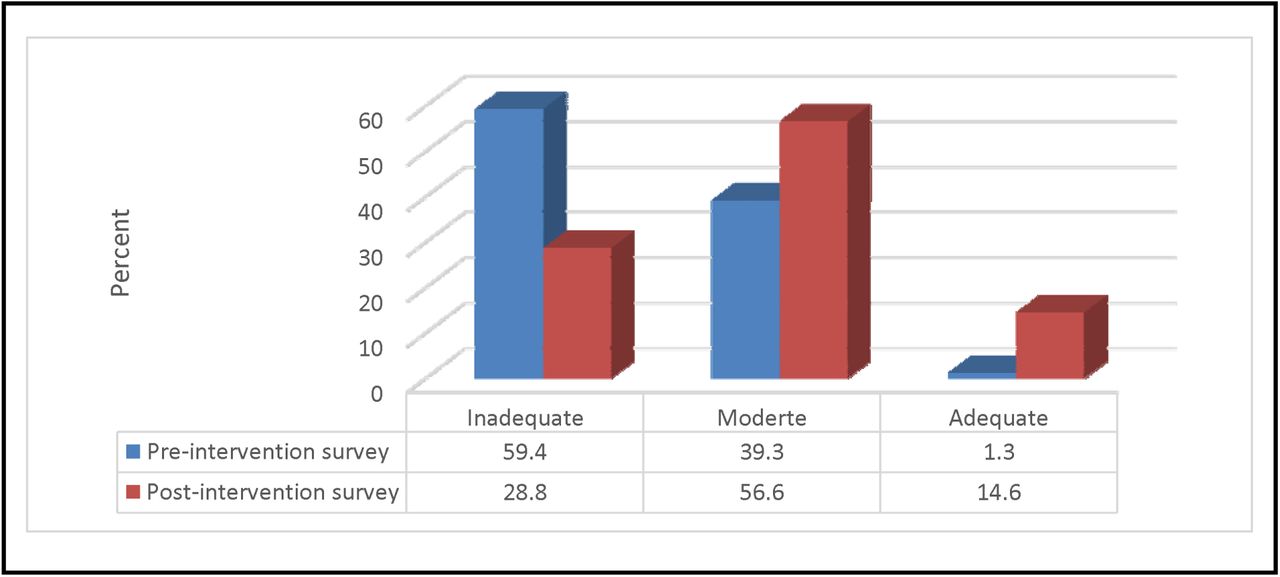
Adequate awareness increased from 1.3% to 14.6%. Adjusted PR of participants’ characteristics (PR = 5.453, 95%CI [4.620, 6.286], p < .001). Paired t-test revealed significant increase: pre-score M=44.08 (SD=15.853), post-score M=59.12 (SD=16.854), mean difference, 15.044, 95%CI [12.903, 17.184], t (13.813) = 451, p < .001. Adjusted multinomial logistic regression revealed, semi-urban residents had 3.295 times higher odds of moderate awareness (aOR = 3.295, 95% CI [1.020, 10.662], p = .046) and 9.258 adequate awareness (aOR = 9.258, 95% CI [2.304, 37.196], p = .002), compared to remote wards. See Fig 3 for detailed changes in awareness level.

FGM health risk awareness
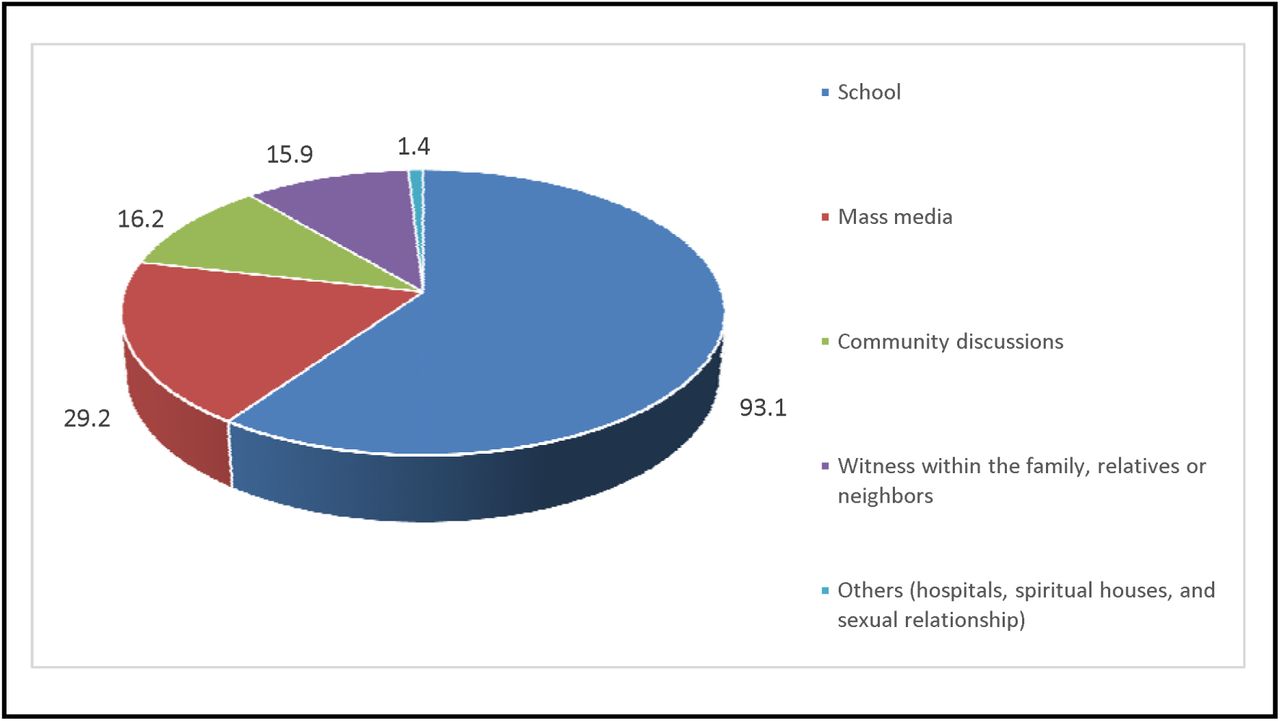
Awareness of FGM harm rose from 91.2% to 96.7%, McNemar (X²=10.473, p=.001), net improvement 25 (40 new gained awareness and 15 regressed). Participant characteristics were not predictors. Awareness was high among those familiar with FGM in their community (X² (1) =5.836, p=.016, φ=.114). The most recognized side effect was excessive bleeding (91.5%). About 92.7% knew FGM lacks medical justification, up from 52.6%, and 97.6% recognized it violates girls and women, up from 85%, with child and early marriage (61.7%) being the most identified violation. 93.1% knew FGM through school, 29.2% mass media, and 16.2% community discussions (multiple responses allowed). However, none of them had prior participation in anti-FGM activities. Fig 4 details participants’ sources of awareness regarding FGM.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Awareness of FGM continuation and reasons
About (50.9%, 230) knew FGM was still occurring, up from 39.7%, McNemar’s Test: X² = 9.653, p =.002, net improvement 51 (155 changed from ‘No’ to ‘Yes’ and 104 regressed). Binary logistic regression showed males had 135% higher odds of admitting FGM occurrence than females (aOR = 2.350, 95% CI [1.441, 3.833], p = .001), while additional years of community residency decreased 6.2% in odds (aOR = 0.938, 95% CI [0.892, 0.986], p = .012). About 60.9% (140/230) could not identify reasons for FGM, while preserving norms and honoring ancestors was commonly cited by 17.4% (40). All reasons are detailed in Table 5.
Attitudes and strategies for abandoning FGM
About (95.8%, 433) desired FGM abandonment, up from 81%, McNemar’s Test: X² = 40.625, p < 001, net improvement 66 (85 changed from ‘No’ to ‘Yes’ and 19 regressed). Binary logistic regression showed no association with participants’ characteristics. About (96.7%, 437) knew FGM is criminal, up from 87.3%. (95.8%, 433) knew the International Day for FGM, up from 42.3% (Table).
KI Interviews
Ten interviews included two participants from every five hospitals. Tribes: seven were Gogo, with Maasai, Burunge, and Rangi each contributing one. Participants aged 15-19, with three at 17 and 18, two at 19, and the others at 15 and 16. Half were married or not. Six had secondary, four primary educations. The thematic analysis yielded three main themes: The Hidden System, Blood and Lies, and Intergenerational Revolt, supported by six categories, and 27 illustrative codes (Table 7). Theme-specific findings are presented with participants’ quotes.
Theme 1: The Hidden System
The theme included three categories and ten codes, showing how FGM persists as a ‘deep-hidden root system’ through gender dynamics, with male and female roles enforcing it. Anti-FGM laws prompted secret ritual adaptations in early childhood, not abandonment. Most admitted to ongoing FGM, mainly postnatal, changing ceremonies. Three KIs added:
Unlike the past, when FGM was conducted on adults, the practice has shifted. Now babies are cut very young, even before they are out. …Knowing how much, currently, is hard, since even ceremonies are no longer held, but many babies are still cut discreetly. …Even those who perform it no longer reveal themselves; many disguise themselves as traditional healers or birth attendants, and their identity is kept classified among a few elders to avoid the hand of law… (KI6, 8 and 10)
Most (7/10) could not recall their cutting experience, saying it happened when they were too young to comprehend self-awareness. Parents hid information and restricted naked interactions with girls of unknown status, claiming their bodies were clean and had to be kept secret until marriage, a common tactic to delay noticing of physical differences. Three reported being cut at ages 6-8. Three reported physical normality, while seven noticed abnormalities. The three believed FGM made them complete women. For some, abnormalities were noticed at least age 10, influenced by sexual activity and peer exposure. Three KIs described:
I noticed differences accidentally while showering with uncut girls because our mother forbade us from bathing or changing clothes with some girls. She kept saying, “Your bodies are clean, keep it secret, meant only for husbands”. …I never knew if I was different since all the girls at home looked similar until I entered into a sexual relationship. …Nobody talks about it; they keep it secret. They know if we knew early, we might disclose, cause trouble, or avoid it (KI9, 6 and 1)
Witnesses of their siblings’ cutting described strategies parents used to keep children unaware of the act. These included sending the young ones away for weeks, then returning after it was done and possibly healed. This aimed to prevent frightening memories and the spreading of news. If they returned before healing, measures like hiding her nakedness were taken. One KI said if the home were unsuitable, a pretence of illness would be made to take her out for some time, claiming she was going to the traditional healer.
Upon returning, we could not see the baby naked, bathe, or change her; services were in the room, and only adults were allowed. Mother said it was from the doctor for children to avoid contact until she recovered. After over 3 months, we were allowed, but then realized she had a healed scar. …if they suspect discovery, they might take her out pretending she is sick and going for medicine…” (KI4 and 5)
Fathers hiding behind the curtain and treating FGM as a women’s issue, letting mothers and grandmothers lead, contributed to its persistence in this patriarchal society. Nevertheless, they fear opposing their mothers’ decisions or punishing them, even if they are against it.
Fathers often avoid direct involvement, leaving elder women in charge. While they are aware of home matters, they see FGM as a woman’s role. …Saying fathers do not participate is misleading; resistance would strip women of power. …Even when informed, fathers dare not punish wives or elders out of respect for tradition, and they have already faded the mindset of marrying cut women (KI 3, 8 and 9)
Theme 2: Blood and Lies
The theme carried three codes. The three KIs who were cut at the age of self-awareness described their experience as ‘violence disguised as care’ and ‘inhumane process,’ involving force, restraint, and bonding pain. Deception lies in making them complete women. However, painful memories fueled their desire to break the generational trauma cycle. One KI shared her experience at age six.
When I was around six, my mother took me to visit my grandmother in the village. My two aunts were also there when we arrived. I did not know what was behind the curtain. My grandmother woke me up the next morning and told me to bathe. A while ago, an older woman arrived with a handbag, and they boiled medicine. They went inside and talked for a while, then called me. When I entered, they closed the door, took off my clothes, and covered my face with a black cloth. Grandmother said, ‘We are making you a clean and complete woman; you will be cut, do not worry.’ I was scared, I cried a lot, and tried to run, but was grabbed. That older woman was spitting medicine on my body while saying things that I did not understand. Despite the high screaming and begging for help, no one came to my aid. One aunt grabbed my mouth and laid me down, while the others tightened my legs and hands down. That older woman forcibly cut my genitalia. It was hurtful; I fainted for an unknown time. When I woke up, they caressed me, saying, ‘You are now a complete woman, the pain will be short, be strong,’ but that elderly woman was gone. I spent over a month inside; at some interval, they washed my perineum with warm water and applied local herbs. I was in much pain, especially when urinating; added to the many scars I had from the forceful cutting. The pain I went through was not of this world and is indescribable. I hate everyone every time I think about it, even though I cannot do them anything. The frequent complaint of my husband’s sexual dissatisfaction and bullying is also killing me. I feel like I came to this world to suffer. At times, I feel miserable and detest my body. What can I do? The cup I should drink for the rest of my life, but honestly, I would not want my child to go through the same cup (moment of sorrow and tears) (KI2)
Theme 3: Intergenerational Revolt
The theme encompassed three categories and 14 codes focused on the power struggle and generational hurdles associated with abandonment of FGM, along with recommendations for effective intervention. Young adults expressed contradictions between education and tradition. While some acknowledged the cruelty of FGM, most were hesitant to abandon it for their children because of a lack of power and desire to maintain societal norms. Those who underwent cutting during ages of non-self-awareness were more likely to adhere to FGM for their children, due to a fear of contradicting their parents, combined with an uncertainty of what occurred to them. A KI in child marriage identified that young fathers often feel powerless in opposing the will of their parents, owing to societal perceptions of their relative immaturity and financial dependence. The fear of being thrown out or punished socially with segregation increases the difficulty of moving away from parental intentions. Delaying child marriage, being economically empowered, and developing awareness of methods can increase their objection power.
Although it sounds scary, I cannot stop the elders, even if I want to—I do not remember what happened, so if it involves following traditions, I am unable to stop them. …My young husband may struggle to oppose his parents’ intentions. Even if he objects, they treat him like a child. He has nothing and fears rejection or isolation. Maybe, if they marry later and become financially independent, they can gain strength (KI2 and 3).
The paradigm shift complicates challenges, requiring refined abandonment strategies. Lack of community-tailored anti-FGM programs hampers across generational efforts. None of the KIs had participated in similar programs before. Although individual awareness of FGM health risks increased, many reported negligence at the community level, and no universal perspective change.
I never participated in programs like this before, such as people visiting our homes or villages to educate us. I learned it at school, noticed the difference after self-checking and comparison, and a little on the radio. Nurses also at the hospital teach us, but such information is not publicly available, as many do not discuss it openly. Though individuals are gaining education, at the community level, many still ignore it and lack readiness to change (KI7)
A key societal challenge was the lack of education on FGM health risks, which allowed its continuation. Many noted education programs were mainly targeted at adults and overlooked the younger generation. Severely, in labor wards, husbands are often absent, leaving mothers or grandmothers, foremost FGM advocates, who might hear and neglect it there. Partner presence can promote universal understanding and resistance power. Therefore, interventions should improve perinatal attendance, couple and family education, and add community conferences by age. Two KIs added:
Changing elders’ attitudes may be more complex than children’s. To end FGM, prioritizing education for uneducated village children is key. Children may still not be deeply immersed in rituals, so even minor efforts can significantly alter their perspectives. …While education is provided here, it is more effective when combined with partner or family involvement and extended through age-based community conferences (KI7 and 10)
Law enforcement and leaders’ commitment are vital for change, but weak enforcement hinders FGM efforts. Leaders may be aware of the issue but conceal the perpetuators. Strong laws and child surveillance could identify current practices and catch offenders. Two KIs added.
Leaders know who performs FGM but hide it. Abandonment is possible with readiness; a strategy focused on law enforcement and investigating all children. …The government could enforce a policy to track all children from now on, with the option to sue offenders even after 20 years. This also helps determine current prevalence (KI3 and 8)
Lastly, ‘The International Day of Zero Tolerance for FGM’ celebrations should shift from the national level to community levels, especially in high-prevalence areas, to boost awareness. Some have heard of it before but could not understand its purpose, which is concerning for action.
I just heard about World FGM Day but never knew what it exactly meant… (KI1).
Discussion
This yearlong study evaluated education interventions against FGM, significantly raising awareness of its harm, changing attitudes, and facilitating community discussions. The discussion triangulates mixed-method findings to generate a comprehensive picture of FGM in the Chamwino community, highlighting its prevalence, awareness, shifts in attitude, challenges to abandonment, and practical strategies.
FGM Prevalence
Over 80% of FGM cases occur in Africa [6]. It is prevalent in Tanzania, and Dodoma ranks second [9]. A self-reported prevalence (7.3%) was below the previous 12% [29] and 69.2% [14] in Tanzania, reflecting inhibited disclosure across societies raised by KIs [16], opposite to the observed 16.6%. While this prevalence was below 47%, previously reported in Dodoma [9], it remains above the national average of 10% [7], indicating more efforts. One-third of the young adults were FGM positive, comprising a quarter of all cases, reflecting ongoing practices [14], supported by KIs. However, fear of arrest reduced public ceremonies, yet mimicked current prevalence, highlighting gaps in policy and commitment.
FGM runs deeply in ethnicity, rural residence, and so do types [8,30,31]. In Chamwino, the Gogos represented 73.6% of FGM prevalence, mirroring ethnic ties [7,14,32,33]. Haneti, a remote ward, had the highest FGM rate at 43.3%. Rural areas favor FGM due to factors like lack of education, limited anti-FGM efforts, limited healthcare, environmental suitability, strong customs, practitioners’ availability, and economic opportunities [14,20,21,31]. High rural prevalence may be attributed to uneducated urban dwellers who use it as their practice site [14,18]. Anti-FGM efforts should be universal, focusing more on rural areas, and scrutinizing methods practitioners use to evade laws [15].
Although types of FGM vary globally owing to cultural beliefs, reporting, and regional differences, this study’s 97.4% and 89% [33] show that type II is most common in Tanzania, and worldwide [21]. FGM types are rooted in history, including the extent of controlling women’s sexuality, non-medical cosmetics, age at practice, and cutting difficulties [34]. The more the genital is modified, the more the risk of complications [21,30]. Sadly, practitioners only focus on immediate effects like pain and bleeding but ignore the lasting impacts on the victim, such as depression, low self-esteem, and family violence—things that were hurting many of the KIs.
The intervention and impact
The achieved 14.6% FGM adequate awareness in this study may not predict community change or FGM abandonment over a year [14,19]. It was lower than 30% in Arusha [14] and 25.7% in Beni-Suef [35]. However, all communities demonstrated low awareness, underscoring the need for ongoing efforts. Participants and studies [14–17,19,29,33] described low awareness about FGM health risks due to cultural rigidity, poor education, informational barriers, limited efforts, and neglect of the young, hindering attitude shifts. Cultural pressures, information access, legal commitment, community dynamics, individual perceptions, and alternative rites influence awareness differences [21,36–38].
Most participants (96.7%) knew FGM is harmful, higher than 70.9% in Ethiopia [38], 68.3% in Saudi Arabia [39], and 30% in Arusha [14]. Awareness, which is crucial to abandoning FGM, is often hidden by a societal system. Nearly half concealed its occurrence, and over 60% could not mention its causes. The longer individuals spend in the community, the higher the likelihood of concealing it, conforming to the powerful effect of social norms discouraging disclosure [40]. Educating children less embedded in the social system and norms can promote openness and perspective change, especially when combined with advocacy, tailored interventions, and stakeholder engagement [14,15,19,29,41]; as implemented in this study.
Experience influences awareness and attitude change [35]. This study and [21,42,43] identify excessive bleeding and severe pain as common FGM side effects. Even though these are irreparable, complications may vary due to FGM type, practitioner’s skill, tools, resistance, healing, and aseptic conditions [42,43]. Training in this study helped broaden the mind of consequences. While [35] highlighted personal experiences as the common source of information regarding FGM, this study found, school education. Personal experiences helped KIs understand health risks. Those who experienced FGM at an age of self-awareness described it as inhumane, with endless bonding pain, echoing [35]. The pain fueled a desire to break FGM’s generational cycle, but fear of penalties caused uncertainty, explaining why even abused women perpetuate cycles.
Most believed FGM violates girls’ and women’s rights, is illegal, and lacks medical basis, aligning with [21,38]. Those cut early in childhood were less aware of consequences and displayed hesitation to abandonment, viewing it as a cultural requirement. In this study, 96.1% of boys and 95.5% girls desired abandonment, higher than 64% and 53% in Sudan [44], reflecting the fruitfulness of our interventions. Even if they wished to stop, a lack of power stifles determination. Campaigns should raise power, promote reporting mechanisms, and alternative rites [14]. This study and [33,38,45] found women centring FGM perpetuation, while fathers assume the passive role. KIs recommend that fathers in patriarchal societies be central to all anti-FGM programs for sustainable change. Additional knowledge on fathers’ misconceptions about FGM and marriageability (e.g., adding women’s value during marriages) can help debunk it as a pre-marital requirement. Father-centred programs yield a two times faster decline in FGM prevalence in Sudan and Somalia [46].
Reasons for FGM follow similar patterns across societies. The reasons in this study, like controlling women’s sexuality, avoiding stigma, rites to womanhood, and limited decision-making power, are common in communities where FGM persists [14,17,21,29]. FGM has shifted to early childhood to evade laws, with public discussion being rare [14,15,33,47]. Only 39.7% acknowledged its occurrence in the pre-survey, rising to 50.9% after education. Increased awareness and discussion in Chamwino, like 98% in Ikungi [29], are boosted by education and alternative rites [13–15,19,48]. Community-tailored programs, coupled with the International Day of Zero Tolerance for FGM, can promote open talks [15,19,22,39,48]. 95.8% of the Chamwino community, (88%) of Mukulat [14], and two-thirds worldwide wish to abandon FGM [49], with education correlating [17,20,31,33,37,38]. Participants noted that ongoing FGM is due to ineffective strategies and law enforcement failures. Despite a strong desire to abandon FGM, challenges in implementation remain, indicating that desire alone cannot beat the strong cultural intent without a solid plan and universal commitment.
Implications for policy and practice
This study’s findings, grounded in participant advocacy, translate into actionable recommendations in three key areas: strengthening legal and leadership frameworks, transforming educational and community engagement, and refocusing on child-centered and gender-inclusive strategies.
Strengthen legal enforcement and leadership accountability, addressing the gap between good policy and poor outcomes. Participants stressed that FGM abandonment depends on consistent government enforcement and community leaders scrutinizing perpetrators, not defending them. This involves moving beyond laws to establish locally actionable accountability mechanisms.
Transform educational and community engagement approaches: participants called for a fundamental shift in awareness efforts:
From one-sided to universal education: programs should target all social groups, extending beyond traditional methods. This involves enhancing FGM integration into perinatal care to promote couple and family discussions, breaking one-sided information flow.
From general to tailored campaigns: interventions should be highly community-tailored, using a network of champions, open dialogues, local media, and survivor testimonies.
Beyond awareness to economic solutions: effective rites of passage must tackle economic factors. This involves giving boys financial literacy and income skills to lessen dependencies that drive practices like early marriage, often connected to FGM.
Implement proactive, child-centered protection strategies: participants highlight that adults, though aware of risks, are immersed in the social system sustaining FGM. Lasting change lies in the next generation. They recommend:
Prioritize early childhood education on FGM risks before social norms are fully internalized through universal programs. Children growing up with this knowledge are more likely to abandon the practice.
Establishing robust, ethical mechanisms for child surveillance to identify current practices, protect at-risk girls, and apprehend perpetrators retroactively.
Strengths and Limitations
This study provided new insights into FGM awareness, experiences, engagement, and attitudes among young adults in the unresearched Chamwino community using mixed methods. It faced limitations: it could not quantify long-term relationships between FGM prevalence and interventions in one year, requiring multifaceted evaluations. Participants suggested involving couples or families in FGM discussions, which we could not achieve, creating opportunities for targeted interventions. A <5% loss to follow-up (3.4%, 16) introduces slight bias [50]. Of the 10 lost females, four had FGM. Their loss, and that of others, may have limited some insights.
Due to ward scattering in Chamwino, time, and institutional constraints, some lacked hospital or school representation. Distributing missed samples equally ensured balanced ward representation, though this may affect findings. The scattered locations led to ward and institutional training of champions, using measures like a WhatsApp group to connect them. While WhatsApp couldn’t include student champions, it was a practical, low-cost solution for adult champions, enabling remote supervision, feedback, sharing materials, and engagement. Efforts were made to include student champions in final ward meetings to introduce them, gather views, acknowledge contributions, and plan jointly. Interviews primarily explore the lived experience of women who underwent FGM, excluding perspectives of uncircumcised women, elders, and practitioners. While this limit understanding of broader community dynamics, it provides detailed insights into personal impacts. Future research should incorporate these perspectives for a more comprehensive understanding.
Conclusion
FGM is still prevalent in Chamwino at an underground, indeterminate rate. This study increased community awareness, shifted attitudes, encouraged community engagement, established a champion’s network, and promoted sustainable abandonment approaches.
Authors’ information
Declarations
Ethical consideration
Kilimanjaro Christian Medical University College (KCMUCo-CREC) approved the study [Cert. No. 2625], and local government granted permissions. Participants signed consent after the researcher explained the study; teachers added a second signature for minors (<18 years). Labor ward interviewees were considered adults and required no extra signature. Quantitative participants were coded P1-P466 for follow-up and analysis, while KI1-KI10 anonymized interviewees. All data were securely stored in a coded file, accessible only for research.
Consent for publication
Not applicable
Author contributions
LBK and MNI: Investigation, Data Curation, Formal Analysis, and Writing – Original Draft. BZT and ACM: Validation of Analysis and Writing – Review & Editing. BTM: Supervision, Funding Acquisition, and Critical Appraisal of Draft. However, all authors conceptualized and approved the final draft.
Funding
This project was funded by GAIA Grant (Project 21-S22F).
Competing interests
The authors declare no competing interests.
Data availability statement
All quantitative data generated during this study are included in this published article and its supplementary files. The data supporting the qualitative findings are available from the corresponding author upon reasonable request.
Acknowledgements
We thank all members of the Chamwino community for their personal support and involvement in the study.
Abbreviations
- HC
- Health Center
- FGM
- Female Genital Mutilation
- KI
- Key Informant
References



