
Abstract
Importance Traditional observational epidemiological studies have consistently found an association between tobacco use, cannabis use and subsequent mental ill-health. However, the extent to which this association reflects an increased risk of new-onset mental ill-health is unclear and may be biased by unmeasured confounding.
Objective To examine the association between cannabis use, tobacco use and risk of incident mood, anxiety, and psychotic disorders, and explore risk of bias.
Data Sources CINAHL, Embase, MEDLINE, PsycINFO and ProQuest Dissertation and Theses were searched from inception until November 2022, in addition to supplementary searches.
Study Selection Longitudinal studies assessing tobacco use and cannabis use and their association with incident mood, anxiety or psychotic disorders were included. Studies conducted in populations selected on health status (e.g., pregnancy) or other highly-selected characteristics (e.g., incarcerated persons) were excluded.
Data Extraction and Synthesis A modified Newcastle Ottawa Scale was used to assess study quality. The confounder matrix and E-Values were used to assess potential bias due to unmeasured confounding. Summary risk ratios (RR) were calculated in random-effects meta-analyses using the generic inverse variance method.
Main Outcome(s) and Measure(s) Exposures were measured via self-report and defined through status (e.g., current use) or heaviness of use (e.g., cigarettes per day). Outcomes were measured through symptom-based scales, interviews, registry codes and self-reported diagnosis or treatment. Effect estimates extracted were risk of incident disorders by exposure status.
Results Seventy-five out of 27789 records were included. Random effects meta-analysis demonstrated a positive association between tobacco use and mood disorder (RR:1.39, 95%CI:1.30–1.47) and psychotic disorder (RR:3.45, 95%CI:2.63-4.53), but not anxiety disorder (RR:1.21, 95%CI:0.87–1.68). Cannabis use was positively associated with psychotic disorders (RR:3.19, 95%CI:2.07-4.90), but not mood disorders (RR:1.31, 95%CI:0.92-1.86) or anxiety disorders (RR:1.10, 95%CI:0.99-1.22). Confounder matrix and E-value assessment indicated estimates were moderately biased by unmeasured confounding.
Conclusions and Relevance This systematic review and meta-analysis presents evidence for a longitudinal, positive association between both substances and incident psychotic disorders and tobacco use and mood disorders. There was no evidence to support an association between cannabis use and common mental health conditions. Existing evidence across all outcomes was limited by inadequate adjustment for potential confounders. Future research should prioritise methods allowing for stronger causal inference, such as Mendelian randomization and evidence triangulation.
Introduction
Tobacco and cannabis are two of the most commonly used recreational drugs worldwide. In 2019, approximately 1.14 billion adults globally had smoked tobacco regularly and an estimated 200 million people used cannabis in the last year.1 Existing observational evidence demonstrates prospective associations between cannabis use, tobacco use and mental ill-health; including depression,2–12 anxiety,7–10, 12–16 and psychosis.10, 17–26 However, it remains unclear if the associations in question are causal or if they result from observational data biases (e.g., confounding, reverse causality).27 Numerous reviews of these substances and mental ill-health highlight confounding as a key limitation when interpreting results.3–5, 9, 18, 19 However, no comprehensive assessment of the strength of potential confounding bias has been conducted. For example, confounding can be reduced if appropriate controls are implemented (e.g., multivariable regression), but in-practice it is difficult to measure all confounders and without error.28
A further difficulty for tobacco and cannabis research is that co-use of these substances is highly common.29–31 Cannabis-tobacco co-use comprises both ‘concurrent use’ (i.e., use of both products in a pre-defined time period) and ‘co-administration’ (i.e., simultaneous use within the same delivery method).31 Considering the high co-occurrence and associations with mental ill-health, there has been debate as to which, if any, has a more important role to play in the development of subsequent mental illness.32, 33 To our knowledge, few reviews examining links with psychological outcomes have considered evidence for both substances independently,8 or jointly.34–36 These reviews have a range of limitations such as synthesising predominantly cross-sectional studies,34, 35 focusing on specific geographic regions or clinical populations,8, 36 lack of quality and confounding assessment.34, 36
As such, we aimed to synthesise longitudinal studies examining the association of cannabis and tobacco use with incident mental ill-health, with a focus on critically assessing biases that limit causal interpretation.
Methods
We pre-registered our protocol on PROPSERO (CRD42021243903) and the Open Science Framework (https://osf.io/5t2pu/). Protocol changes have been reported in eSupplement, and we have followed MOOSE reporting guidelines (eSupplement).37
Search and Selection
We searched CINAHL, Embase, MEDLINE, PsycINFO and ProQuest Dissertation and Theses from inception to November 2022. Searches were conducted using MeSH headings and text words relating to exposures, outcomes, and study design (eSupplement). CB and AB/RL/KS independently assessed title/abstracts and full texts. Discrepancies were resolved through discussion amongst the reviewers, or a third reviewer where necessary (GT).
Eligibility Criteria
We included prospective longitudinal studies that (1) measured cannabis, tobacco, or co-use as an exposure, (2) used a ‘non-exposed’ comparator group, (3) reported a relevant effect estimate (e.g., risk ratio, odds ratio) and its variance, or necessary raw data. There were no restrictions on publication status, article language or publication date. To minimise risk of bias from reverse causation, we only included studies where participants with the outcome of interest were excluded at baseline (i.e., ‘incidence’). Studies were also excluded if participants were selected on a specific health status (e.g., pregnancy), or other highly selected characteristics (e.g., incarcerated persons). Full details in eSupplement.
Data Extraction
Standardised forms were used to extract study information by two independent reviewers (CB and JL). A modified Newcastle Ottawa Scale (NOS) was used to evaluate study quality (eSupplement).38 The NOS evaluates studies across selection, comparability, and outcome assessment. A standardised assessment sheet was used (CB) and calibrated with a second-rater (JL) for ∼20% of the included studies. Disagreements were raised with an independent third reviewer (GT).
To explore the impact of bias due to unmeasured confounding across the included studies we used a combination of approaches. The E-value represents the minimum strength of association, on a risk ratio (RR) scale, an unmeasured confounder would need to have to fully explain a specific exposure–outcome association [i.e., fully reducing a RR to 1].39 What constitutes a small or large E-value is context dependent, relative to the exposure, outcome and measured covariates.40 To support interpretation of the E-values, we used a ‘confounder matrix’ assessment and a directed acyclic graph (DAG).41 The confounder matrix provides improved assessment and visualization of confounding control in reviews of observational studies. Based on our DAG (eSupplement), studies in the primary meta-analyses were assessed on adjustment for six constructs: other substance use; psychiatric comorbidity; socioeconomic status; sociodemographic factors; psychological factors; and other lifestyle factors (eSupplement).
Statistical Analysis
We used RR and corresponding 95% confidence intervals (95%CIs), as the summary estimate. Included studies presented varied effect estimates and approach for conversion to RR is described in eSupplement. Adjusted and unadjusted, or minimally adjusted (i.e., age and sex), effect estimates were pooled separately. Random-effects meta-analysis using generic inverse variance approach was conducted. Between-study heterogeneity was explored through visual inspection of forest plots and tau-squared (τ2), and statistical inconsistency quantified using the I2 statistic.42 Prediction Intervals (PI) were additionally calculated i.e., 95% range of true effect estimates to be expected in exchangeable studies.43 Small-study effects were examined using Doi plots and asymmetry was quantified using the Luis Furuya-Kanamori (LFK) index.44 Where ≥10 studies were available, sources of heterogeneity in the primary analyses were explored through pre-planned subgroup analyses and meta-regressions.42 Additional exploratory sensitivity analyses were conducted for outliers and confounder matrix assessment. Meta-analyses were conducted in R, using the ‘meta’ package.45 Data and R scripts are available on GitHub (https://github.com/chloeeburke/tobcanmeta). The ‘E-Value’ online calculator (https://www.evalue-calculator.com/) and ‘metaconfoundr’46 package were used for sensitivity analyses.
Results
Literature Search
Of the 27789 records screened, 486 studies were retained for full-text screening (eSupplement). We identified 75 studies for inclusion,13, 47–120 of which 59 were included in the primary meta-analyses.13, 47, 49, 50, 52, 53, 55–68, 71–73, 75–78, 80–82, 84, 85, 87–89, 91, 92, 94–96, 100, 102–118, 120 A list of studies excluded at full text stage is available in eSupplement). Studies included in the primary meta-analyses consisted of 1733679 participants at risk of incident outcomes. Follow-up length ranged from 6-months to 63-years. Exposures were measured according to heaviness (e.g., cigarettes per day; k=28) or status of use (e.g., current use; k=31). Outcomes were assessed using symptom-based scales (k=21), interviews (k=18), registry codes (k=14), self-reported treatment/diagnosis (k=2) and composites (k=4). Study characteristics are presented in eSupplement.
Meta-Analyses
Tobacco
Tobacco use was associated with incident mood disorders (K= 43; RR:1.39, 95%CI:1.30–1.47; I2=61.2%; τ2=0.014; PI: 1.08–1.77; Figure 1)13, 47, 49, 50, 52, 53, 55–64, 68, 71–73, 75–78, 80, 81, 85, 87, 88, 91, 92, 100, 102, 103, 105–110, 114, 115, 118. Exclusion of outliers,49, 68, 73 produced similar results (K=40; RR:1.38, 95%CI:1.31–1.45, I2=28.5%). Pooled unadjusted results yielded a larger point estimate (K=41; RR:1.47, 95%CI:1.34–1.60; I2=68.6%; τ2=0.06; PI: 0.92–2.33; eSupplement).47, 48, 50–56, 58, 68–74, 77, 80, 81, 83, 85, 86, 88, 90, 92, 93, 97, 98, 102, 103, 105–108, 110, 114, 115, 118, 119

Meta-analysis of the association of tobacco use and mood disorders
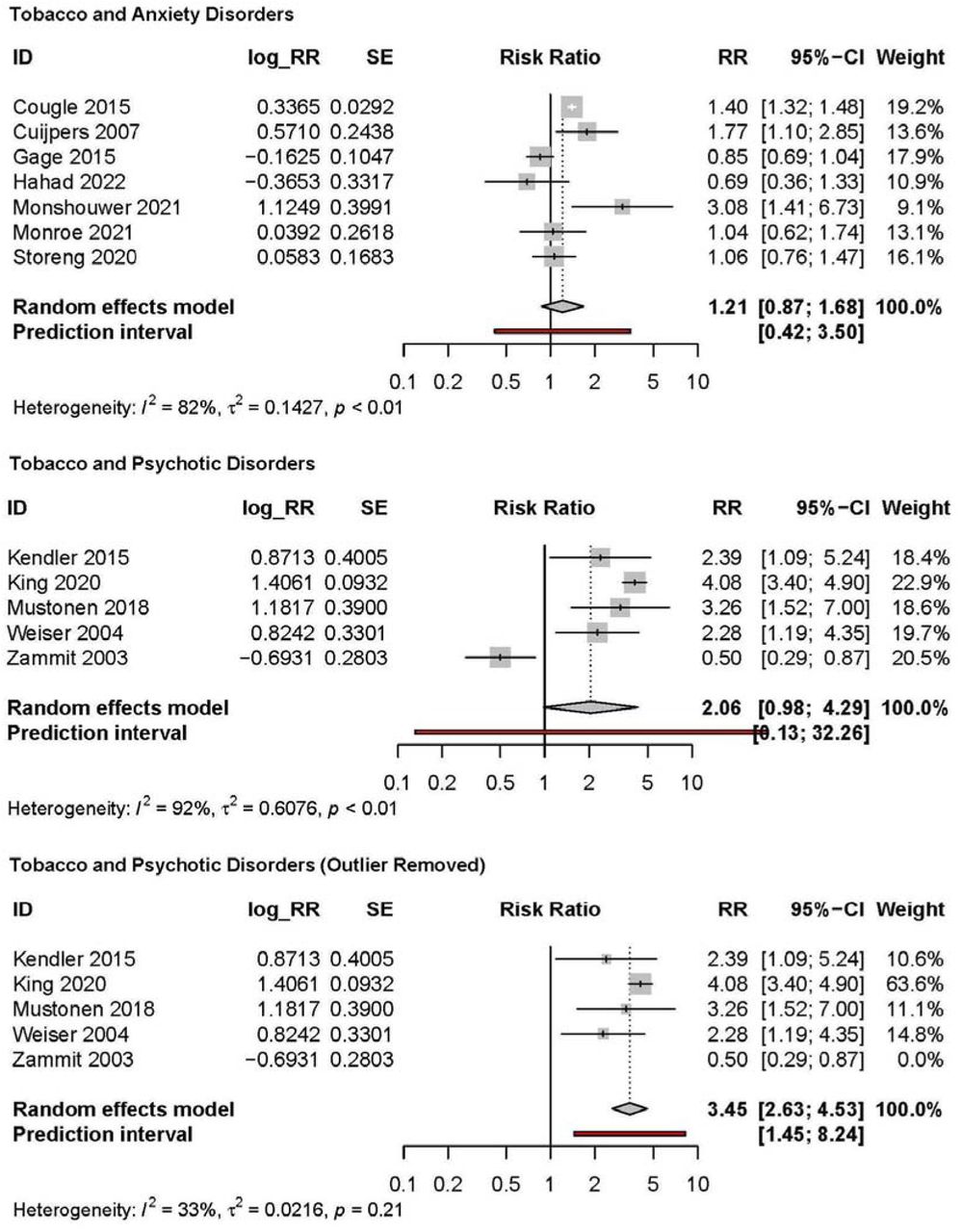
Tobacco use was not associated with incident anxiety disorders (K=7; RR:1.21, 95%CI:0.87-1.68; I2=82.2%; τ2=0.143; PI: 0.42–3.50; Figure 2).63, 64, 71, 76, 91, 92, 107 Pooled unadjusted studies yielded a larger point estimate (K=8; RR:1.60, 95%CI:1.10–2.32; I2=71.7%; τ2=0.204; PI: 0.48–5.30; eSupplement).53, 71, 79, 91, 92, 96, 107, 120

Meta-analyses of adjusted associations of tobacco use and anxiety and psychotic disorders
Tobacco use was not associated with incident psychotic disorders (K=5; RR:2.06, 95%CI:0.98-4.29; I2=92.3%; τ2=0.608; PI=0.13–32.26).82, 84, 94, 113, 117 Exclusion of one outlier,117 yielded a larger pooled estimate (RR:3.45, 95%CI:2.63–4.53, I2=32.9). As outlier identification was exploratory, pooled results with and without the outlier excluded are presented (Figure 2). Pooled unadjusted studies yielded a larger estimate (K=5; RR:3.12, 95%CI:1.67–5.81; I2=83%; eSupplement).82, 84, 99, 113, 117
Cannabis
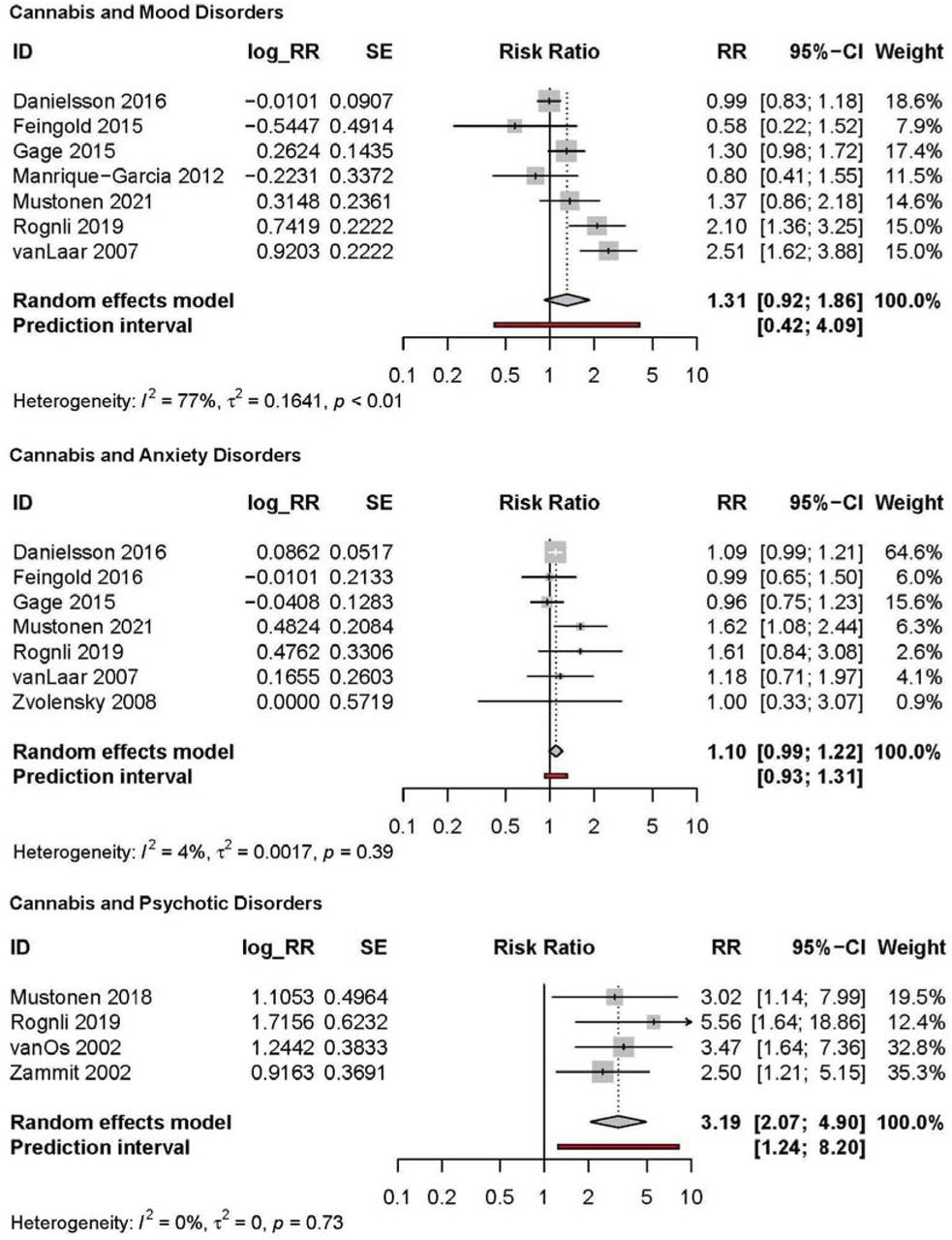
Cannabis use was not associated with incident mood disorders (K=7; RR:1.31, 95%CI:0.92-1.86; I2=77.0%; τ2=0.164; PI: 0.42-4.09; Figure 3).65, 66, 71, 89, 96, 104, 111 Pooled unadjusted studies yielded a larger estimate (K=7; RR:1.47 95%CI:1.19–1.81; I2=72.4%; eSupplement).65, 66, 71, 89, 96, 101, 111
{kind=link}
{kind=link}
{kind=link}
Meta-analyses of adjusted associations of cannabis use and mood, anxiety and psychotic disorders
Cannabis use was not associated with incident anxiety disorders (K=7; RR:1.10, 95%CI:0.99-1.22; I2=4.4%; τ2=0.002; PI: 0.93–1.31; Figure 3).65, 67, 71, 96, 104, 111, 120 Pooled unadjusted studies yielded a larger estimate (K=6; RR:1.51 95%CI:1.20–1.89; I2=74.3%; eSupplement).65, 67, 71, 96, 111, 120
Cannabis use was associated with incident psychotic disorders (K=4; RR:3.19, 95%CI:2.07–4.90; I2=0%; τ2=0.00; PI: 1.24–8.20; Figure 3).95, 104, 112, 116 Pooled unadjusted studies yielded a larger estimate (K=3; RR:4.68 95%CI:3.30–6.64; I2=0.0%; eSupplement).95, 112, 117
Quality Assessment and Meta-Biases
Across studies included in the primary meta-analyses, roughly one quarter of studies (27%) were judged as ‘high’ quality (i.e., lower risk of bias) in the quality assessment (eSupplement), with an overall mean score of 7.35 (SD 1.01). The proportion of high quality studies differed by analysis (eSupplement). Many studies (58%) were marked down due to high attrition or insufficient information about loss to follow-up (e.g., differential attrition), and 41% of studies were marked down for ‘comparability’ (i.e., confounding bias). Using the confounder matrix, most studies had multiple confounding constructs rated as inadequately adjusted for (eSupplement), particularly other psychological factors (e.g., loneliness) and psychiatric comorbidity. Median E-values for study effect estimates and CIs have been presented in Table 1.
E-value and confounder matrix summary
Evidence for small-study effects was present in all analyses, except cannabis and mood disorders, with Doi plots and LFK indices suggesting minor or major asymmetry (eSupplement).
Subgroup and Sensitivity Analyses
Subgroup and sensitivity analyses were only performed for tobacco use and mood disorders due to low study numbers (K <10) in other meta-analyses. Results were examined across different age groups, follow-up length, sample size, study quality, confounding adjustment and exposure/outcome types. No analyses supported evidence of subgroup effects (eSupplement).
Discussion
To our knowledge, this is the first systematic review and meta-analysis on the association of tobacco use, cannabis use and incident mental ill-health that has undertaken a comprehensive assessment of the influence of confounding bias, employing novel methods (i.e., confounder matrix, E-values) to support this assessment. We found evidence for positive associations of tobacco and incident mood and psychotic disorders, and of cannabis and incident psychotic disorders. Our review includes the first meta-analysis of the longitudinal association between tobacco use and anxiety disorders, and addresses limitations of previous reviews which have considered evidence for both substances in relation to psychological outcomes.
Accurately understanding the causal pathways between substance use and subsequent mental illness is crucial for informing the implementation of effective evidence-based public health policies.121 Results from this review are based on observational evidence and cannot in isolation be considered proof of causality. However, current tobacco policy and clinical implications regarding the association and between smoking and various physical conditions (e.g., lung cancer) is considered strong evidence of causality due to consistency in direction and strength of the effect estimate in combination with other criteria (e.g. dose-response). This study adds to a wider, growing body of evidence that these substances have a causal role in development of psychotic disorders, and tobacco use in mood disorders.122, 123 As such, policy makers should consider the level of evidence as adequate to inform public health campaigns (e.g. warning labels) about the potential harms of smoking for mental health.76 Nonetheless, there are still essential areas for future research to inform, including accurately identifying size of causal effects and possible biological mechanisms.123
While there was evidence for an association between tobacco and both mood and psychotic disorders, we did not find compelling evidence to suggest tobacco use is associated with incident anxiety disorders. Previous narrative syntheses found mixed evidence regarding the association between tobacco use and later anxiety.7,12 The effect size observed in the analysis of tobacco use and subsequent mood disorders is consistent with previous meta-analyses.2, 3, 6, 8 Although there was considerable methodological heterogeneity present across these studies, subgroup analyses of studies using different exposure and outcome definitions demonstrated similar associations. Importantly, lack of evidence for differences between subgroups does not automatically imply the effect is equivalent across subgroups, and specific subgroup analyses may have been affected by other sources of heterogeneity.
Comparatively fewer studies examined the relationship between cannabis use and incident mood disorders. Our analyses of cannabis use for subsequent mood and anxiety disorders did not support evidence of an increased risk in the cannabis use versus non-use groups. Several previous meta-analyses have reported mixed evidence regarding the association between cannabis use and elevated anxiety symptoms or disorder,124 and there are multiple meta-analyses of prospective studies which report a modest association between cannabis use and depressive symptoms or disorder.124 Three previous meta-analyses of prospective studies adjusting for baseline depression, found modest associations (OR range: 1.17-1.37)4, 5, 8 between cannabis use and subsequent depression. It’s possible that focusing on incident outcomes (vs. statistical adjustment) could explain the discrepancy in findings but may also relate to other differences in review criteria and content (e.g., adolescents only, number of studies). Recent reviews focusing on studies of cannabis frequency and potency suggest that more frequent use,24 and use of more potent forms,125 poses greater risk. However, due to limited study numbers and measurements, it was not feasible to investigate these potential moderators.
In line with other meta-analyses, this review reported evidence of a strong association between tobacco use, cannabis use and psychotic disorders.10, 18, 19, 21, 22, 24 Considerable uncertainty regarding the size of the association was indicated by confidence and prediction intervals. ‘Noisy’ effect estimates are common in the case of rare outcomes, due to lower statistical power. Pooling such effects in a meta-analysis can help yield a more precise estimate of the association of substance use with psychotic disorder, but this review included few studies. This is likely related to our exclusion of traditional case-control designs, which are well suited to the study of rare outcomes but are at increased risk of bias from retrospective recall and reverse causality.126 Lack of prospective research in this area has been previously highlighted.127, 128
We did not identify any eligible studies of cannabis-tobacco co-use. Assuming causality, dual use may place consumers at a higher risk of developing a mental health disorder than the independent use of either substance. There is a selection of cross-sectional research which indicates people who co-use have a higher prevalence of mental health disorders,129, 130 and levels of psychological distress.131 Some longitudinal evidence suggests co-use is associated with greater mental health symptoms,132 but prospective evidence in general population samples is lacking.
Analyses of small-study effects suggested possible risk of publication bias, with evidence of asymmetry for most meta-analyses. As such, pooled estimates may misrepresent the ‘true’ association. However, asymmetry can be driven by multiple factors (e.g., methodological heterogeneity) and may not represent publication bias.133 Furthermore, in the case of small study numbers (K<10), Doi plots and LFK index have advantages over traditional funnel plots in detecting asymmetry but may still misrepresent asymmetry.44
E-value and confounder matrix assessment suggested that many of the studies are at risk of confounding bias. Studies often inadequately adjusted for key confounding variables (e.g., ACEs). Previous reviews of these exposures have demonstrated moderate-strong associations with risk of substance use and various mental health outcomes (e.g., ACEs: ORSmoking 2.82, ORDepression, 4.40).134 Notably, subgroup analyses stratified by study quality and confounding adjustment suggested minimal impact on the tobacco and mood disorders pooled estimate. Combined with our focus on incidence, this implies stronger evidence of a causal effect of tobacco smoking for mood disorders. However, none of the extracted effect estimates adjusted for genetic vulnerability (e.g., polygenic risk) which alternative study designs (e.g., familial-based designs) suggest may play a substantial role in the observed associations.135–137 E-values must be interpreted considering some assumptions and limitations.40, 138 Importantly, adjustment for some covariates (e.g., SES) likely reduces bias from some unmeasured confounding (e.g., ACEs) due to the associations between these constructs. Nonetheless, the smaller E-values observed for some significant associations (i.e., tobacco/mood) would suggest that pooled estimates likely overestimate the size of effect. Furthermore, many studies were limited by inadequate description of attrition and few studies reported on individual-level missing data or used methods to account for this (e.g., multiple imputation). This directly contradicts recommendations by relevant reporting guidelines (e.g., STROBE)139 and hinders assessment of selection bias. It’s critical that future studies aiming to explore causal associations, provide more detailed descriptions of participant attrition and missing data and apply appropriate methods to reduce bias.140 Finally, although we focused on incidence, this does not exclude risk of bias from reverse causation as both psychotic and non-psychotic mental disorders do not have discrete onsets and subthreshold or prodromal symptoms at baseline may remain unaccounted for.141 As such, to support the identification of the size of causal effects, there is the need for further research focusing on addressing and exploring the biases that arise in traditional observational epidemiological studies.
Mendelian randomisation (MR) is one such method. MR uses genetic variation as an instrumental variable for an exposure to estimate causal effects that are more robust to reverse causality and confounding bias.142 A systematic review of MR studies investigating the causal relationships between substance use and mental health found evidence to support a bi-directional, increasing relationship between smoking and symptoms of depression, bipolar disorder and schizophrenia.143 Evidence regarding cannabis use and mental health was less conclusive, which may relate to lack of available frequency instruments.143, 144 Still, MR is “far from a silver bullet”145 and there are important limitations to be addressed through more advanced methods (e.g., multivariable MR), additional sensitivity tests (e.g., residual population stratification) and incorporation into planned triangulation frameworks,27 including triangulation with carefully planned longitudinal cohort analyses.27, 143 Widespread adoption of DAGs when selecting secondary data sources may yield useful insights as to whether research questions are feasibly explored within certain datasets.40 In combination with the need for well-controlled prospective longitudinal studies, more evidence using alternative study designs is required, as meta-analysis of the same study design may serve to amplify inherent biases.
Limitations
Several important limitations need to be considered. All studies used self-report to define exposure status. This is not unusual in cohort studies but will result in measurement error that can bias effect estimates in the case of both differential and non-differential misclassification. Similarly, we included studies which used symptom-based scales, self-reported diagnosis and resource access (e.g., medication) which will introduce further measurement error. Most studies were based in high-income countries, and we restricted the review to include studies conducted in a broadly general population samples which reduces generalisability. The number of studies included in most meta-analyses was small and also prevented planned explorations of heterogeneity, which is highly recommended for syntheses of non-randomised studies.146 Finally, through analysing overarching diagnostic groups (e.g., mood disorders), relevant differences for individual disorders may be overlooked (e.g., bipolar disorder), which will be important to consider in exploring possible causal mechanisms (e.g., neuroadaptations in nicotinic pathways).123
Conclusions
This systematic review and meta-analysis presents evidence for a longitudinal, positive association between both substances and incident psychotic disorders and tobacco use and mood disorders. In contrast to previous meta-analyses, there was no evidence to support an association between cannabis use and common mental health disorders. Existing evidence across all outcomes was limited by inadequate adjustment for potential confounders. Future research should prioritise methods allowing for stronger causal inference, such as Mendelian randomization and evidence triangulation.
Acknowledgements
Author Contributions: (1) Concept and design: CB, TF, HS, RW, GT; (2) Acquisition, analysis, or interpretation of data: CB, AB, JL, KS, RL, TF, HS, RW, GT; (3) Drafting of the manuscript: CB, AB, JL, KS, RL, TF, HS, RW, GT; (4) Statistical analysis: CB, GT, TF, HS, RW; (5) Obtained funding: CB; (6) Administrative, technical, or material support: CB, AB, JL, KS, RL; (7) Supervision: TF, HS, RW, GT
Conflict of Interest Disclosures: GT has previously received funding from Grand (Pfizer) for work not related to this project. CB, HS and RW have done paid consultancy work for Action on Smoking and Health (ASH) for work related to this project. The remaining authors have no conflicts of interest to declare.
Funding/Support: This study was supported by a Society for the Study of Addiction (SSA) PhD studentship awarded to CB.
Role of Funder/Sponsor: The funding organization had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.↵
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.
- 12.↵
- 13.↵
- 14.
- 15.
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.
- 21.↵
- 22.↵
- 23.
- 24.↵
- 25.
- 26.↵
- 27.↵
- 28.↵
- 29.↵
- 30.
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.↵
- 45.↵
- 46.↵
- 47.↵
- 48.↵
- 49.↵
- 50.↵
- 51.
- 52.↵
- 53.↵
- 54.
- 55.
- 56.↵
- 57.
- 58.↵
- 59.
- 60.
- 61.
- 62.
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.
- 70.
- 71.↵
- 72.
- 73.↵
- 74.↵
- 75.
- 76.↵
- 77.↵
- 78.↵
- 79.↵
- 80.↵
- 81.↵
- 82.↵
- 83.↵
- 84.↵
- 85.↵
- 86.↵
- 87.↵
- 88.↵
- 89.↵
- 90.↵
- 91.↵
- 92.↵
- 93.↵
- 94.↵
- 95.↵
- 96.↵
- 97.↵
- 98.↵
- 99.↵
- 100.↵
- 101.↵
- 102.↵
- 103.↵
- 104.↵
- 105.
- 106.
- 107.↵
- 108.↵
- 109.
- 110.↵
- 111.↵
- 112.↵
- 113.↵
- 114.↵
- 115.↵
- 116.↵
- 117.↵
- 118.↵
- 119.↵
- 120.↵
- 121.↵
- 122.↵
- 123.↵
- 124.↵
- 125.↵
- 126.↵
- 127.↵
- 128.↵
- 129.↵
- 130.↵
- 131.↵
- 132.↵
- 133.↵
- 134.↵
- 135.↵
- 136.
- 137.↵
- 138.↵
- 139.↵
- 140.↵
- 141.↵
- 142.↵
- 143.↵
- 144.↵
- 145.↵
- 146.↵




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos