
Abstract
Cognitive deficits are prevalent in individuals with psychosis and are associated with neurobiological changes, potentially serving as an endophenotype for psychosis. Using the HCP Early Psychosis dataset (n=226), we aimed to replicate cognitive subtypes (deficit, intermediate, spared) through data-driven clustering on affective and non-affective psychosis patients and controls. We explored differences between the clusters in symptom manifestation, cognition, medication, and grey matter volume, comparing patients to controls. Fuzzy K-Means clustering on PCA-selected features revealed three cognitive subgroups significantly varying in clinical symptoms and cognitive impair-ment, and importantly also in medication and grey matter volume in fronto-parietal and subcortical networks. The spared cluster (86% controls, 37% affective psychosis, 17% non-affective psychosis) exhibited unimpaired cognition, lowest symptoms/medication, and grey matter comparable to controls. The deficit cluster (4% controls, 10% affec-tive psychosis, 47% non-affective psychosis) had impairments across domains, highest symptoms/medication, and pronounced grey matter alterations. The intermediate clus-ter (11% controls, 54% affective psychosis, 36% non-affective psychosis) showed fewer deficits than the second cluster, but similar symptoms/medication/grey matter to the first. Controlling for medication, cognitive scores correlated with grey matter changes and negative symptoms across all patients. Our findings generally emphasize the inter-play between cognition, brain structure, symptoms, and medication, and specifically suggest a possible mediating role of cognition linking alterations in brain structure and symptoms, which highlights the potential of screening cognitive changes to aid in tailoring treatments and interventions.
1 Introduction
Cognitive alterations are core symptoms of psychosis [1–4], which have been described in areas of working memory [5, 6], attention [7, 8], reasoning [9, 10], decision making [11–13], salience processing [14, 15], learning (e.g., lower learning rate or increased forgetting, [16–18]) and problem solving [19, 20] and across all stages of the disease [21–25]. Cognitive deficits furthermore precede the clinical onset of psychosis [26], and predict functional out-come in later stages of the disease [27, 28], impacting employment status, independent living and social functioning [28, 29]. Although cognitive impairments are present in about 80% of patients suffering from psychotic disorders [30–32], therapeutic interventions are limited. A meta-analysis including 93 studies using different agents targeting mainly glutamatergic and cholinergic neurotransmitter systems, but also serotonin, dopamine, GABA and nora-drenaline agents [33] reported a significant, although very small (g=0.10) improvement of cognition in general. However, this meta-analysis failed to find significant improvement for cognitive subdomains [33]. Cognitive training, also called cognitive remediation therapy, has produced more promising effects [34, 35]. A recent meta-analysis found that cognitive reme-diation showed significant small-to-moderate cognitive improvements in all domains studied (g=.19–.33) and a small improvement in function (g=.21). Furthermore, research has shown that fewer cognitive deficits and higher cognitive reserve during prodromal and first episode psychosis are generally, diagnosis-independently, associated with better functioning and re-covery [36, 37]. Indicating that maintaining and improving cognitive functioning is crucial in the interventional and therapeutic processes.
Cognitive deficits in psychosis in general have been linked to alterations in the cortico-cerebellar-thalamic-cortical circuits [38]. Here, dysfunctional GABA (gamma-amino-butyric acid) inter-neurons, the main inhibitory neurons of the central nervous system, may disrupt the balance between excitatory and inhibitory processes in the cortex [39]. A recent review [25] summarizes the association between functional brain alterations and cognitive deficits in individuals at-risk for psychosis, early onset psychosis, and chronic schizophrenia. They report a clear association between altered cortical (e.g., prefrontal cortex, anterior cingulate cortex, insula) and subcortical (e.g., thalamus, striatum, hippocampus, cerebellum) brain signalling and aberrant cognition across the different stages. Further support is provided by imaging studies showing reduced gray matter volume and altered network organization which correlates with cognitive deficits, at illness onset [40, 41], early psychosis [42] and chronic schizophrenia [43].
Interestingly, psychosis patients with different diagnoses, e.g., affective vs non-affective psychosis, show varying cognitive deficits [44–46]. In a review, Barch and Sheffield [46] summarized that while the severity of cognitive impairment is stronger in non-affective com-pared to affective psychosis, the relative impairments across different cognitive domains are very similar. Other studies however do not differentiate between affective vs non-affective psychosis when investigating cognitive deficits [47]. Despite these differences in cognitive alterations with regard to specific diagnoses, cognitive deficits in psychosis have been de-scribed and investigated as intermediate phenotypes [48]. In a recent study, Shafee et al.[49] pointed out that cognitive phenotypes may vary grossly depending on specific types of psy-chosis (e.g. affective vs non-affective), suggesting that certain domains of cognition (e.g., working memory vs face processing) may be more etiologically linked to psychosis than oth-ers. Using a K-means clustering approach in a cross-diagnostic sample, Lewandowski et al. [50] identified four cognitive subgroups combining different psychosis groups. Importantly, they identified one cognitively intact cluster including healthy controls and patients with different diagnoses, while the other three clusters were dominated by different cognitive im-pairment profiles [50]. A recent systematic review of data-driven identification of cognitive subtypes [51] highlighted that despite the heterogeneity of clustering methods used and cog-nitive domains studied, there is some commonality in the identification of a severe cognitive deficit phenotype showing deficits across multiple domains and a spared cognitive deficit phenotype with similar performances to controls. It is, however, unclear how these cogni-tive subtypes vary or are linked to differences in symptom expression, medication status and brain structure (i.e., grey matter volume). These open questions are however crucial in order to understand whether cognitive subtypes are clinically relevant, and could increase our mechanistic understanding of the disorder.
In the current study, we, therefore, aimed at exploring these important open ques-tions. First, we wished to replicate three cognitive subtypes using the HCP Early Psy-chosis dataset (https://www.humanconnectome.org/study/human-connectome-project-for-early-psychosis, [52]) using data-driven clustering on standardized cognitive, perceptual and emotional task and score data, but no clinical data. Second, we explored whether the pa-tients in the three clusters differed in symptom expression, cognition, medication and grey matter volume. And, third, depending on results for the first two questions, we wished to understand if symptoms, alterations in cognition and brain morphometry were associated when controlling for medication within and across the clusters.
2 Methods
2.1 Participants
We analyzed data collected by the “Human Connectome Project for Early Psychosis” (HCP-EP, [53], [54]). The HCP-EP 1.1 release (August 2021 HCP-EP Release 1.1 on NDA) contains 251 subjects consisting of 68 healthy control individuals, 57 patients with affective and 126 patients with non-affective psychosis, both patient groups were within the first three years of the onset of psychotic symptoms. The Structured Clinical Interview for DSM-5: Research Version (SCID-5-RV) ([55]) was used to confirm diagnoses of non-affective (i.e., schizophrenia, schizophreniform, schizoaffective, psychosis not otherwise specified, delu-sional disorder, brief psychotic disorder) or affective psychosis (i.e., major depression with psychosis or bipolar disorder with psychosis). Clinical symptoms were assessed using the Positive and Negative Syndrome Scale (PANSS, [56]). Disease onset for all patients was within the last five years prior to study enrollment. For a comprehensive cognitive, percep-tual and emotional assessment, the NIH toolbox ([57], [58]; i.e., cognition (Picture Sequence test, Dimensional Change test, Flanker test, Picture Vocabulary test, Pattern Completion test, List Scoring test, and Oral Reading test), emotion (Self-report emotion), perception (Words in Noise, Odor Identification, and Dynamic Visual Acuity), sensory-motor functions (9-Hole Pegboard, and Grip Strength), the HCP Lifespan Measures ([59]; i.e., Delay Dis-counting and Penn Emotion Recognition), the WASI-II ([60]) and the Seidman Auditory Continuous Performance Test ([61]) was used. Structural brain imaging data was available for 183 of the 251 subjects. After ensuring that there were sufficient data for both, features and subjects (see description of analysis below), the analysis was performed on 226 subjects (i.e., 56 healthy controls, 52 affective psychosis group, 118 non-affective psychosis group). Demographics and clinical scores for the three groups are presented in Tab. 1. Detailed analysis of PANSS items are presented in Suppl. Fig. 1.
2.2 Variable Selection and Preprocessing
Initially, all cognitive, perceptual and social/emotional functioning scores available in the HCP-EP data-set were selected, resulting in 70 variables as potentially relevant to our analysis (Suppl. Tab. 1). As covariates, we chose age, gender, socio-economic status and mother’s level of education. Variables containing information of primary diagnosis for affective and non-affective psychosis, such as the Positive and Negative Symptom Score or the Clinical Assessment Interview for Negative Symptoms, as well as variables describing medication dosage, usage or equivalent doses, were not included in the clustering analysis, but only used for subsequent analyses.
Many of the selected variables contained missing data. We therefore excluded variables when more than 10% of the entries were missing, and we excluded subjects with more than 20% missing variables (Suppl. Tab. 1). As a result, 33 of initially 70 variables remained in the data set and 226 subjects. The distribution of the remaining subjects reflected the distribution of the original data with regard to diagnosis type. For an overview of the selected variables, and group comparison, see Suppl. Tab. 2. In the final dataset used for analysis, subjects were missing a maximum of seven variables (Suppl. Tab. 4). Missing data were imputed using the mean for continuous and mode for categorical variables (e.g. demographic control variables). Since the ratio of patients and controls was not balanced, mean or mode for data imputation were calculated separately for patients and controls. Both patient groups were combined in order to minimize the bias of classical group membership (Suppl. Tab. 3).
Prior to our analysis, all continuous features and covariates were normalized using z-score normalization. Ordinal covariates such as socio-economic status and mother’s education were scaled between 0 and 1, and treated gender binary.
The HCP-EP brain imaging data contain structural magnetic resonance imaging (MRI) data. We used T1-weighted structural images recorded at a 3T SIEMENS MAGNETOM Prisma scanner using a MPRAGE sequence (TR=2400ms, TE=2.22ms, FoV read=256mm, FoV phase=93.8%, flip angle=8 deg, slices per slap=208, slice thickness=0.8mm). In order to receive individual gray matter volume for structural covariance networks generated across all subjects (Suppl. Tab. 2), the structural brain data was preprocessed as described in the supplement section supplementary material 1.4 and elsewhere [62]. The structural covariance networks were used for analyses following the clustering.
2.3 Correlation and Homogeneity
To investigate correlation between all features, we performed a Pearson’s correlation be-tween all subjects’ non-standardized variables. Differences between correlations between the groups were evaluated with a T-test for means of two independent samples. We then tested homogeneity between groups, using a Levene’s test for equal variances between groups. Bonferroni corrections were applied.
2.4 Feature Selection
To reduce the dimensionality of our data set and at the same time keeping its maximal variance, we used a principal component analysis (PCA), which is suitable for our data type [63], and was applied to all variables and covariates. Significant principal components were identified using a permutation test (5000 random permutations of each feature across subjects). Components which survived permutation testing were considered significant.
2.5 Fuzzy Clustering
Instead of a hard clustering approach that assumes well separated clusters and assigns each data point to only one cluster (e.g. K-Means), we used a soft clustering approach. This approach accounts for fuzzy boundaries between subgroups, and is thus better suited for overlapping subgroups [64], as would be expected for clinical groups. We, therefore, used Fuzzy K-Means clustering as described in [65]. As input to our clustering analysis, we used the dimensionality-reduced data which included demographic control variables for all three groups (i.e., controls, affective and non-affective patients). We specified the number of clusters prior to our analysis. We used a priori knowledge about the number of cognitive clusters (i.e., three different cognitive cluster were reported in the literature [51]). As a control analysis, we also used three clusters on patient data only. This analysis was used to determine influence of control subjects on the clustering, and is presented in the supplements.
Performance of the clustering analysis was determined by the ratio of the subjects of one group (healthy controls, affective psychosis group and non-affective psychosis group) in each cluster. The ratio of subjects in cluster j for group i in {controls, affective and non-affective}

2.6 Cluster exploration
After the identification of the three clusters, we explored differences in the patients dis-tributed over those three clusters and controls in cognitive scores, clinical scores, medication and grey matter volume. We want to point out that the control subjects were removed from each of the clusters and combined in one healthy group. Thus, a group comparison across four groups was computed. For comparing groups, we used SciPy’s Kruskal-Wallis test with Dunn’s test for post-hoc analyses, a Chi-square test of independence or ranked analysis of variance with Bonferroni corrected post-hoc tests. As a control analysis, we performed par-tial Pearson’s correlations between cognitive scores, clinical scores, and grey matter volume controlled for medication across all patients, with multiple comparison corrections.
2.7 Statistical implementation
Preprocessing and data analysis was performed in Python 3.9.7. We used scikit-learn 1.0.2, SciPy 1.7.2 for all analyses and the fuzzy clustering implementation of [66]. Partial correlations were performed using the ppcor 1.1 [67]. For clustering analyses, brain data was corrected for total intacranial volume (TIV), age and sex, using the R stats package, version 4.0.5 R [68].
3 Results
3.1 Homogeneity of data across groups
Correlations of all cognitive, perceptual and emotional functioning data revealed, that correlations were highest within controls compared to affective (T-test: t5838=16.34, p<0.001) and non-affective (T-test: t17058=26.03, p<0.001) patients. For non-affective patients, corre-lations within subjects were lowest (non-affective vs. affective patients: T-test: t16626=8.47, p<0.001), indicating greatest variability. Confirming these results, highest heterogeneity was found in non-affective patients compared to controls (Levene’s test for equal variance: F1,174=187.3, p<0.001) and affective (Levene’s: F1,168=70.39, p<0.001). Controls were the most homogeneous (Levene’s: F1,106=22.34, p<0.001) (Fig. 1a).
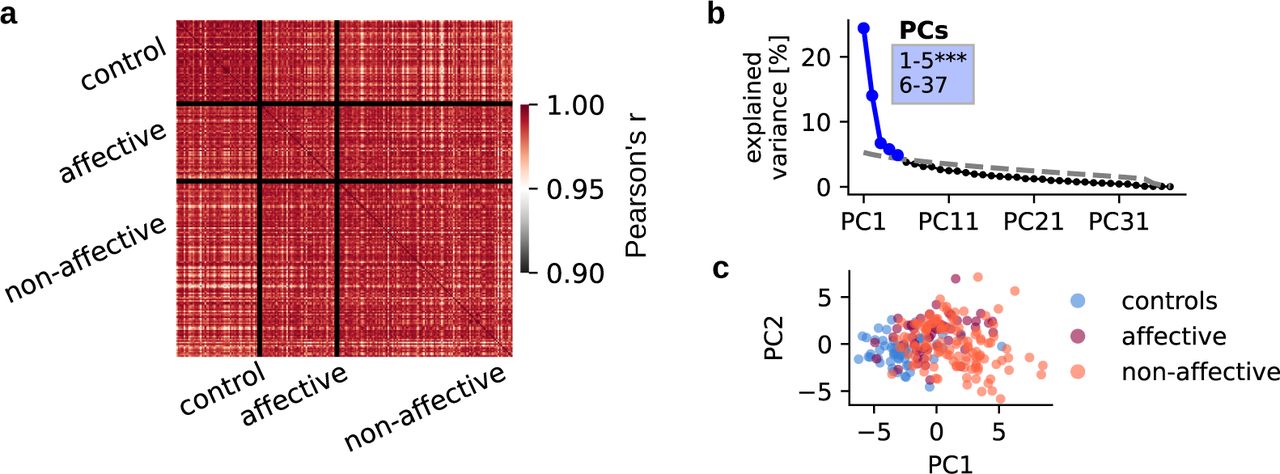
(a) All variables (i.e., cognitive, emotional, perceptual data) correlated across subjects using Pearson correlation. Correlations within groups are displayed in squares on the diagonal, and correlations between groups are displayed in off-diagonal squares. (b) Variance ex-plained by each of the PCs in % of a PCA performed on all variables and covariates across 226 subjects. The first five PCs (blue) survived permutation testing (p<0.05, 5000 permu-tations). Significant components captured 55.8 % of all variance. (c) Individual data points represent relevant variables for each subject, displayed on the first two principal components and colored according to subject group affiliation.
3.2 Feature selection using principal component analysis
During the data dimensionality reduction, we identified five significant PCs, using all data from all groups, that captured 55.8 % of total variance (Fig. 1b). Explained variance of PCAs was consistent with other symptom-reduction studies [69]. Fig. 1c illustrates the data reduction using the first two principal components. The two patient groups and the control group are predominantly distributed across the dimension of P1. However, no clear boundaries between groups could be detected. The features that explained most variance were Fluid Intelligence and Crystallized Intelligence, Total IQ, the Picture Vocabulary Test Picture vocabulary test, Oral reading recognition, Auditory attention, Working memory, WASI -Verbal comprehension, WASI -Matrix reasoning as well as DCCS -Executive functioning (Suppl. Fig. 3). To check the influence of combining patient and control data, the same analysis was performed on patients only data, which also resulted in five significant components that captured 53.7 % of all variance (p<0.05, 5000 permutations) (Suppl. Fig. 4a, b). The top ten features contributing to the explained variance were the same across both analysis -with and without controls. Those feature were taken for subsequent statistical analyses.
3.3 Group representation in the three clusters
We performed clustering on the selected features, including controls and both patient groups, with three clusters. Fig. 2a and b present the results. One cluster (cluster 0) contained 86% (48/56) of all controls and 37% (19/52) of all affective subjects. Non-affective subjects were represented only in small proportion of 17% (20/118). A mixed, second cluster (cluster 1) consisted of mostly patients, with the majority of affective individuals: 54% (28/52) of non-affective and 36% (42/118) of affective patients and only 11% (6/56) control. Most non-affective subjects were contained in the third cluster (cluster 2) with 47% (56/118) of the non-affective, and only 10% of affective patients (5/52) and 4% (2/56) of controls. (Fig. 2b).

(a) Result of clustering. Cluster affiliation of each subject is displayed on the first two PCs. Colors correspond to cluster 0, 1 or 2. (b) Percentage of subjects of each group in each cluster. E.g. 47 % (56/118) of all non-affective subjects are in cluster 2.
3.4 Exploring cognition, symptoms, medication and gray matter volume in the clusters
To identify possible cognitive subgroups represented in the clusters, we explored cognitive scores and symptom expression for patients assigned to the clusters (see comprehensive display of statistical differences between all clusters and cognitive items in Suppl. Tab. 5). We compared cognitive scores across patients in respective clusters. Scores of control subjects were used for comparison. Patients in cluster 2 (mainly non-affective patients) showed a significant decrease in all cognitive features compared to patients assigned to other clusters, as well as controls. Patients in cluster 1, which contains 28 affective and 42 non-affective patients, showed significant decrease of Fluid Cognition, Auditory attention (%correct) and DCCS -Executive functioning compared to controls. Patients (19 affective and 20 non-affective) in cluster 0 showed most similar scores compared to control subjects, with Auditory attention (%correct) being the only score that is significantly lower compared to controls (Fig. 3c) and group comparisons are presented in Tab. 5.

(a) Clinical scores of affective and non-affective patient within each cluster are displayed in boxplots. Individual boxplots show data minimum, first quartile, median, third quartile, and data maximum. Individual subjects are overlaid as dots. Outliers are indicated outside the minimum or maximum. (b) Medication dosage and status of affective and non-affective patients within each cluster. (c) Cognitive score of affective and non-affective patient within each cluster are displayed and compared to all control subjects (c, light blue). The plots display the ten features contributing most to explained variance of the PCs. (d) Differences in three grey matter volume comparing affective and non-affective patient within each cluster are displayed and compared to all control subjects (c, light blue). NW 18 comprises the putamen and the amygdala; NW 29 comprises the paracingulate gyrus, the juxtapositional lobule, the supe-rior parietal lobule, and the precentral gyrus;1a1nd the NW 30 comprises the superior fornatl gyrus, the frontal pole, the putamen, the postcentral gyrus and the cerebellum crus. The plots display the ten features contributing most to explained variance of the PCs. Signifi-cance is indicated as p ≥ 0.05 (*), p ≥ 0.01 (**) and p ≥ 0.001 (***).
Patients in cluster 2, who showed the strongest cognitive deficits and who were mainly diagnosed with non-affective psychosis, were significantly increased in PANSS total com-pared to patients in both, cluster 0 and 1. They were also significantly increased in PANSS positive, PANSS negative and general psychopathology compared to patients in cluster 0. Even tough patients in cluster 0 and cluster 1 did not show as a strong difference in cognitive scores, patients in cluster 1 were significantly increased in PANSS total, PANSS positive and general psychopathology compared to patients in cluster 0 (Fig. 3a) and group comparisons are presented in Tab. 5.
Further, we explored the medication status of patients within the clusters. We found that patients assigned to cluster 2 had a significantly higher Chlorpromazine equivalence dose in general and at the scanning date compared to patients in both cluster 0 and 1, and a significant increase in lifetime antipsychotic drug exposure compared to patients in cluster 1 (Fig. 3b) and group comparisons are presented in Tab. 5.
Furthermore, we explored differences in grey matter networks across the patients in the clusters and the controls. The ranked analysis of variance revealed a highly significant inter-action effect (F(87)=2.564, p=1.79e-13) between the patients in the three clusters and the controls (four groups) and the grey matter volume in each network (30 networks). Bonferroni corrected post-hoc analyses revealed significant differences in network 18 (F(3,48.64)=9.32, p=0.00027), network 29 (F(3,45.13)=7.8, p=6e-05) and network 30 (F(3,45)=10.95, p=2e-05) (Fig. 3d) and group comparisons are presented in Tab. 5.
Finally, we investigated partial Pearson correlations between the ten cognitive features, the three significant grey matter volume networks, and the clinical scores, controlling for Chlorpromazine equivalent dose within each cluster and across all patients. Not with in the clusters, but across all patients we found several significant, multiple-comparison-corrected associations, see Fig. 4 and Suppl. Tab. 6.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Correcting for the equivalent dose of medication, we used Partial Pearson correlations to investigate the interaction between cognitive scores (i.e., Fluid Intelligence and Crystallized Intelligence, Total IQ, the Picture Vocabulary Test Picture vocabulary test, Oral reading recognition, Auditory attention, Working memory, WASI -Verbal comprehension, WASI -Matrix reasoning as well as DCCS -Executive functioning), brain networks (i.e., NW18, NW29, NW30), and clinical scores (i.e., PANSS total, PANSS positive, PANSS negative, General psychopathology score) across all patients independent of cluster.
Comparison between patients in all clusters and control subjects for cognitive features that contributed most to variance, as well as medication and PANSS comparison between patients in different clusters. For the group comparison, a Kruskal-Wallis was used with a Dunn’s test for pairwise comparisons (statistics and p-value displayed or ns -non significant).
4 Discussion
The aim of this study was (1) to investigate cognitive subtypes using the HCP Early Psychosis dataset and data-driven clustering on standardized cognitive, perceptual and emo-tional task and score data, but no clinical data; to explore (2) differences in and (3) associ-ations between cognition, symptom expression, medication and grey matter volume. Using a data driven parameter selection and clustering approach, we were able to identify three clusters that significantly differed in across cognitive deficits forming a cognitively intact cluster, an intermediately affected cluster and an cognitively affected cluster, and poten-tially characterise subgroups previously described in the literature [36, 50, 70–75]. Impor-tantly, our results extend those findings, showing that patients within those clusters also differ in medication dosage, in specific grey matter brain networks and in clinical symptoms. Interestingly, across all patients but not within clusters we found that decreased grey mat-ter volume in frontal, parietal and subcortical regions was linked to higher cognitive scores including crystallized cognition, verbal comprehension or matrix reasoning, when control-ling for medication, and that decreased cognitive scores were linked to increased negative symptoms, when controlling for medication.
Using a three cluster solution on all participants (i.e., controls, affective and non-affective psychosis), allowed the identification of cognitive subtypes, which significantly varied in clinical and cognitive impairment. Patients of cluster 2, consisting of nearly 50% of the non-affective psychosis individuals, expressed the highest symptom scores across PANSS total, PANSS negative and positive and general psychopathology and impaired cognition in all domains compared to cluster 0 containing 17% of the non-affective and 37% of the affective individuals, and partially also compared to cluster 1 which consists of the majority of affective individuals and 36% of non-affective individuals. Patients in cluster 0 had the lowest symptom scores and globally spared cognitive abilities, which were similar to those of controls. Cluster 1 was intermediate, with cognitive impairments in several but not all domains and slightly increased symptoms compared to the cognitively spared cluster. This finding confirms results from Lewandowski and colleagues [50] who found a four-cluster solu-tion to provide the best fit to their data containing three diagnostic patient groups, with one globally impaired cluster, for which cognitive deficits were associated with symptom severity and poorer functioning, one cognitively spared cluster and two intermediate clusters [50]. The overall structure of cognitive clusters identified in the present study supports findings discussed in a recent meta-analysis of data-driven identification of cognitive phenotypes in schizophrenia [51]. Green and colleagues [51] describe that what is characteristic to all cluster solutions is the presence of a cognitively spared, one or multiple intermediate and a deficit subgroup [51]. Importantly, the current study replicates three cognitive clusters us-ing standard cognitive, perceptual and emotional assessments, selected for general cognitive screening purposes but not necessarily to detected the largest or most consistent cognitive deficits in early stages of psychosis, suggesting generalisability among these clusters.
In addition to the differences across many cognitive domains between the patients of the clusters, we also found differences with regard to amount of medication using Chlorpro-mazin equivalent doses and grey matter volume in frontal, parietal and subcortical brain areas. This emphasizes the complexity of the inter-relationships of cognitive deficits, brain alteration, medication usage and symptom expression, especially when considering that the clustering is based on task and questionnaire data only, and still, differences across all do-mains -cognition, brain scores, medication and symptoms -have been identified. Several studies indicate an association between higher doses of medication and stronger cognitive deficits [76–78]. In a birth cohort study, for example, Husa and colleagues [76] showed that a higher lifetime dose of anti-psychotics was associated with lower cognitive performance in schizophrenia patients at the age of 43. Interestingly, a longitudinal study [77] investigating the effect of anti-psychotic treatment discontinuation showed that those individuals who did not remain on their medication after a 3.5 year follow up had improved significantly more than those who stayed on their medication even when controlling for symptom severity and cognitive scores at baseline. General non-adherence of medication use, however, does not have the same positive effect on cognition [79]. Especially, anticholinergic medication has been associated with a high cognitive burden [78], which is being supported by our results. Changes in gray matter volume have been associated with an increased risk for psychosis and disease development [80–82], and provided the basis for good classification in a recent multicohort-study [83], as well as in earlier studies [84, 85], although classification results are inconsistent [86]. Our results show that the cluster with the strongest cognitive deficits has increased grey matter volume in three brain networks spanning fronto-parietal and sub-cortical areas. Across all participants and when correcting for medication we also found a negative correlation between grey matter volume and cognitive performance in several cognitive tests, including general cognition, verbal cognition and reasoning. Interestingly, grey matter volume alterations, especially reductions have been reported in association with schizophrenia [41, 87–89]. Results however depend on the specific region [90], illness stage and medication [91, 92]. Interactions between grey matter alterations and various cognitive scores have not been studied extensively. Most studies investigated cognitive alterations in specific domains (e.g., working memory) and often reported positive correlations [93–95]. Very few studies report negative correlations -increased grey matter volume being linked to reduced cognitive scores. Zhang and colleagues [96] for example showed, comparable with our results, that the performance in the Stroop Color-Word Test’s Card C was negatively correlated with grey matter volumes of frontal and middle frontal brain areas. In a cohort of at-risk mental state for psychosis individuals, Koutsouleris and colleagues [97] found positive and negative correlations between grey matter volume and performance in the trail-making test, with negative correlation reported for cerebellar regions, which is comparable to what we report in the current study. We suspect that the structural covariance networks anal-ysis, which specifically aims at finding similarity networks between participants, and then analyses grey matter volume differences within these similar networks might contribute to the difference in directionality of the correlations. Our results however clearly demonstrate differences in the cluster containing the most strongly affected patients -clinically and cog-nitively. These differences reported in the literature may suggest that grey matter changes are not generally linked to cognitive changes, but rather play a mediating role. This argu-ment would be in the same line of thought as put forward by Palaniyappan [98], stating that grey matter changes in multimodal brain regions which have a supervisory function on sensory, emotional and language processing, may link to symptom expression when occur-ring with functional impairments. Future studies should therefore aim at the combination of additional structural imaging data, such as structural or white matter connectivity, to com-plement their analysis and potentially identify underlying neuropathological mechanisms.
Our data furthermore reveals a strong link between negative symptoms and cognitive impairments. Investigating PANSS total, we found a step-wise increase in symptom severity from cluster 0 to cluster 2, with the cognitive deficit cluster 2 to show highest symptom scores. We found, also, that cluster 0, the cognitively spared cluster, showed significantly lower positive symptoms compared to cluster 1 and 2. Furthermore, the globally impaired cluster (cluster 2) revealed increased negative symptoms compared to both other clusters, and increased global psychopathology compared to the cognitively spared cluster (cluster 0), indicating that the cognitive deficits occur in those subjects with strong negative symptoms and a higher severity of general psychopathology [99]. This is in congruence with Oomen and colleagues [100] who reported three clusters based on only cognitive data with one severely cognitively impaired cluster, which showed general functioning being significantly lower compared to the patients in the other clusters. Interestingly, patients of the severely impaired cluster also showed lower general functioning scores at a trend at 6- and 12-month follow-up. Similar results were reported by Haining and colleagues [74]. Tan and colleagues [75] on the other hand did not find associations between the three cognitive clusters and symptom expression, but found that the cognitively impaired subgroup already showed worse academic performance at the level of childhood, early and late adolescence. These findings confirm the critical relevance of cognitive deficits for early detection and functional prediction [26–28, 74]. This often replicated distribution of a severely impaired cluster, indicating that early interventions based on such cluster analysis would be suitable too.
Finally, as our results confirm that patients with non-affective psychosis show stronger cognitive deficits compared to patients with affective psychosis, it is not surprising that non-affective patients are more likely to be in the intermediate and impaired subgroups. Still both patient groups are present in all clusters, with the cognitively intact subgroup consisting of 19/52 and 20/118 patients with affective and non-affective psychosis, respectively, the intermediate group with 28/52 affective and 42/118 non-affective psychosis patients, and the cognitively impaired group with 5/52 affective and 56/118 non-affective psychosis patients. Our results indicate that clustering extends classical patient classification and diagnosis solely based on International Statistical Classification of Diseases (ICD)/Diagnostic and Statistical Manual of Mental Disorders (DSM) [101, 102] and may provide an additional characterisation of patients which may emphasise additional targets of interventions and treatment, such as cognitive remediation, especially for those individuals in the intermediate and in the deficit cluster.
This study has several limitations: Generally, K-Means [103] is a commonly used cluster-ing algorithm that performed well on our behavioral, such as cognitive, data. Nevertheless, there are some drawbacks of this method: First, the algorithm requires a predefined number of clusters. Based on the diagnosis, data contained at least three groups. We used this prior information as basis for the specification of the number of clusters in our analysis. Based on the literature, where a spared, an impaired and an intermediate cluster are regularly de-tected [51] we predefined three clusters for the identification of subgroups. Identification of four or more clusters require large sample sizes in order to produce reliable and interpretable results. Our sample size does not allow this, because of the restricted number of subjects. Second, K-Means clustering does not work well with non-spherical cluster or clusters with different sizes [104]. We, therefore, also performed fuzzy K-means clustering approach which accounts for fuzzy boundaries between subgroups, and is suited for potentially overlapping subgroups [64]. The age difference between the groups might constitute another limitation of the study. However, since age was added as a covariate to all analyses, we believe that this aspect did not affect the results to a significant degree. Third, the basis of our clus-tering provided cognitive, perceptual and emotional test scores, which were taken from the standardised NIH toolbox ([57], [58]). Further improvement of clustering and identification of cognitive subgroups may be achieved through the selection of specific behavioral tasks and cognitive domains. Moreover, advanced analysis strategies, e.g., computational mod-elling may improve clustering [16, 17, 105], as it provides the opportunity to identify and mathematically differentiate behavioral parameters, which were found to be reliable and unique across individuals [106].
In conclusion, our results provide evidence for the presence of three cognitive subgroups -one cognitively intact, one intermediate and one deficit group -replicating previous find-ings. This study however extends those results showing that patients within those three clusters also differ with respect to current medication dosage and grey matter volume in fronto-parietal and subcortical regions. Our results therefore emphasize the complex inter-relations between cognition, symptoms, brain structure and medication, drawing attention to the pivotal role alterations in cognition as a factor for the selection of treatments and interventions.
Acknowledgement
Research using Human Connectome Project for Early Psychosis (HCP-EP) data reported in this publication was supported by the National Institute of Mental Health of the National Institutes of Health under Award Number U01MH109977. The HCP-EP 1.1 Release data used in this report came from DOI: 10.15154/1522899.
Footnotes
Conflict of Interest: None of the authors declares a conflict of interest.
Author contributions: FK, KB, AW conceptualisation; KK preprocessing of structural brain data; FK and KB formal analysis of cognitive data and clustering analysis; FK and KB writing of first draft; FK, KB, AW and KK editing and revising of manuscript.
We defined our clusters on data only containing cognitive, emotional and perceptual task and questionnaire data, while before we included structural brain data. We the analysed the clusters with regard to alterations in cognition, medication, symptoms and structural brain data. This we had not done before.
References
- [1].↵
- [2].
- [3].
- [4].↵
- [5].↵
- [6].↵
- [7].↵
- [8].↵
- [9].↵
- [10.].↵
- [11].↵
- [12].
- [13].↵
- [14].↵
- [15].↵
- [16].↵
- [17].↵
- [18.].↵
- [19].↵
- [20].↵
- [21].↵
- [22].
- [23].
- [24].
- [25].↵
- [26].↵
- [27].↵
- [28].↵
- [29].↵
- [30].↵
- [31].
- [32].↵
- [33].↵
- [34].↵
- [35].↵
- [36].↵
- [37].↵
- [38].↵
- [39].↵
- [40].↵
- [41].↵
- [42].↵
- [43].↵
- [44].↵
- [45].
- [46].↵
- [47].↵
- [48].↵
- [49].↵
- [50].↵
- [51].↵
- [52].↵
- [53].↵
- [54].↵
- [55.].↵
- [56].↵
- [57].↵
- [58].↵
- [59].↵
- [60.].↵
- [61].↵
- [62].↵
- [63.].↵
- [64].↵
- [65].↵
- [66].↵
- [67].↵
- [68].↵
- [69].↵
- [70].↵
- [71].
- [72].
- [73].
- [74].↵
- [75].↵
- [76].↵
- [77].↵
- [78].↵
- [79].↵
- [80].↵
- [81].
- [82].↵
- [83].↵
- [84].↵
- [85].↵
- [86].↵
- [87].↵
- [88].
- [89].↵
- [90].↵
- [91].↵
- [92].↵
- [93].↵
- [94].
- [95].↵
- [96].↵
- [97].↵
- [98].↵
- [99].↵
- [100].↵
- [101].↵
- [102].↵
- [103].↵
- [104].↵
- [105].↵
- [106].↵
- [107].
- [108].
- [109].
- [110].
- [111].




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos