
Abstract
England has experienced a heavy burden of COVID-19, with high infection levels observed throughout the summer months of 2021. Alongside the emergence of evidence suggesting that COVID-19 vaccine protection wanes over time, booster vaccinations began for individuals aged 50 and above in September 2021. Using a model fitted to 18 months of epidemiological data, we project potential dynamics of SARS-CoV-2 transmission in England to September 2022. We consider key uncertainties including behavioural change, waning vaccine protection, strategies for vaccination, and the reintroduction of public health and social measures. We project the current wave of transmission will peak in Autumn 2021, with low levels of transmission in early 2022. The extent to which SARS-CoV-2 transmission resurges in 2022 depends largely on assumptions around waning vaccine protection and booster vaccinations. Widespread booster vaccinations or the reimposition of mild public health and social measures such as work-from-home policies could largely mitigate the wave of COVID-19 transmission projected to occur in England in Spring/Summer 2022.
Main
Eighteen months into the COVID-19 pandemic, 250 million confirmed cases and 5 million deaths have been attributed to severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) worldwide1. In England as of 17th November 2021, cumulative confirmed COVID-19 cases exceed 8 million, with more than 500,000 hospitalisations and 120,000 deaths within 28 days of a positive test being recorded, respectively2. Different variants of SARS-CoV-2 have emerged, with four (Alpha, Beta, Gamma and Delta) currently designated as variants of concern (VOC) associated with either increased transmissibility, severity, or changes in immunity by the World Health Organisation3. England saw the emergence and takeover of the Alpha B.1.1.7 variant in late 2020, which was subsequently overtaken by the Delta B.1.617.2 variant in Spring 2021. Various public health and social measures (PHSMs) have been implemented to suppress COVID-19 transmission in England, including national lockdowns, staged relaxations of lockdowns and tiered regional restrictions4, but all legal restrictions were completely lifted on 19th July 2021.
Safe and effective COVID-19 vaccines have been developed at unprecedented speed, with four currently approved for use by the UK’s Medicines and Healthcare products Regulatory Agency (MHRA). The COVID-19 vaccine rollout in England began on the 8th of December 2020 and to date more than 42 million people have received at least their first COVID-19 vaccine dose2. The initial rollout of vaccines followed guidance issued by the UK’s Joint Committee on Vaccination and Immunisation (JCVI)5, with vaccine supply being targeted to health and social care workers and those in the highest risk categories first. Vaccines were then offered to sequentially younger age groups of adults (18 years and above). In August 2021, children aged 16 and 17 years old and clinically vulnerable children aged 12-15 were offered COVID-19 vaccines6. In September 2021, healthy 12-15-year-olds in England were offered their first COVID-19 vaccination, but to date, no such recommendation has been made for the second dose follow up7.
A COVID-19 booster vaccination programme began on 24th September 2021, initially targeting the same priority groups that were first vaccinated. A full dose of the Pfizer/BioNTech or a half dose of the Moderna vaccine are recommended as a booster dose, regardless of what vaccine was received previously, to those at least 6 months after their primary course of vaccination. On 15th November 2021, the JCVI issued advice recommending that the widespread COVID-19 booster vaccination programme be extended to individuals aged 40-49 years8. In addition to a widespread booster vaccination programme, the JCVI have recommended that severely immunocompromised individuals over 12 years of age should be offered a third COVID-19 vaccination dose as part of their primary COVID-19 vaccination schedule9. With rising COVID-19 incidence and concerns about hospital bed pressures over the coming months, stakeholders including the British Medical Association have also called for the introduction of PHSMs in place in several other European countries, including face covering mandates, vaccine certification and encouragement to work from home where possible10. In addition to this, evidence continues to emerge about waning vaccine protection over time11, 12.
Using an age-structured deterministic compartmental model of SARS-CoV-2 community transmission, we project the consequences of behavioural changes, waning vaccine protection and of different vaccination and PHSMs on COVID-19 cases, hospitalisations and deaths into 2022. We fit the model to region-specific data on COVID-19 deaths, hospitalisations, and hospital bed occupancy, as well as PCR prevalence, seroprevalence, and the emergence of the Alpha B.1.1.7 and Delta B.1.617.2 VOCs, as well as integrating data on the number of vaccinations delivered at the level of NHS England regions and by age group. We consider the effects of fully vaccinating different age groups of adolescents and children in the future, different levels of uptake for these age groups, as well as the consequences of implementing mass COVID-19 booster vaccination campaigns in different age ranges in the population, seasonality, and the implementation of PHSMs to suppress projected rises in transmission. Considering different assumptions on vaccine rollout going forwards, we explore the projected dynamics of SARS-CoV-2 transmission over the winter months and until September 2022.
Results
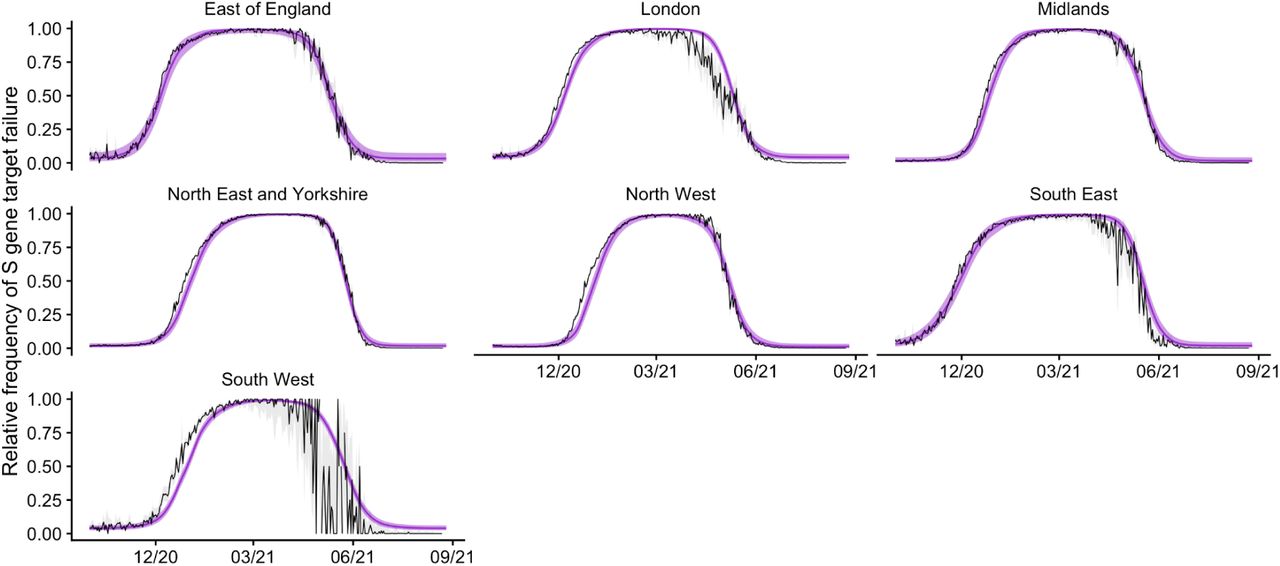
Our compartmental model fits the observed dynamics of SARS-CoV-2 community transmission during the first, second and third waves of the COVID-19 epidemic in England between mid-February 2020 and October 2021 (Figs. 1 and S1), reproducing NHS England region-specific observed deaths, hospitalisations, hospital and ICU bed occupancy, PCR prevalence, and seropositivity. The model also captures the emergence and spread of the Alpha B.1.1.7 and Delta B.1.617.2 variants of concern in late 2020 and early 2021, fitting to the prevalence of S gene target failure (Fig. S2) and to the proportion of Delta sequenced cases (Fig. S3). Model estimates for increased transmissibility of Alpha relative to previously circulating SARS-CoV-2 variants and of Delta relative to Alpha are given in Table S1.

Black lines show reported data, with vertical black lines showing 95% confidence intervals for PCR prevalence. Coloured lines and shaded areas show medians and 90% interquantile ranges from the fitted model. The original model fitting is done independently for each NHS England region, with the aggregated model output for the whole of England shown here. COVID-19 deaths data was provided by the UK Health Security Agency (UKHSA) and hospital admissions, hospital and ICU bed occupancy data was provided by NHS England. These data sources are unpublished and not publicly available, but are closely aligned with the UK Government’s COVID-19 dashboard. PCR prevalence data was obtained from the Office for National Statistics’ COVID-19 Infection Survey (ONS-CIS)13. ICU = intensive care unit. NHS = National Health Service.
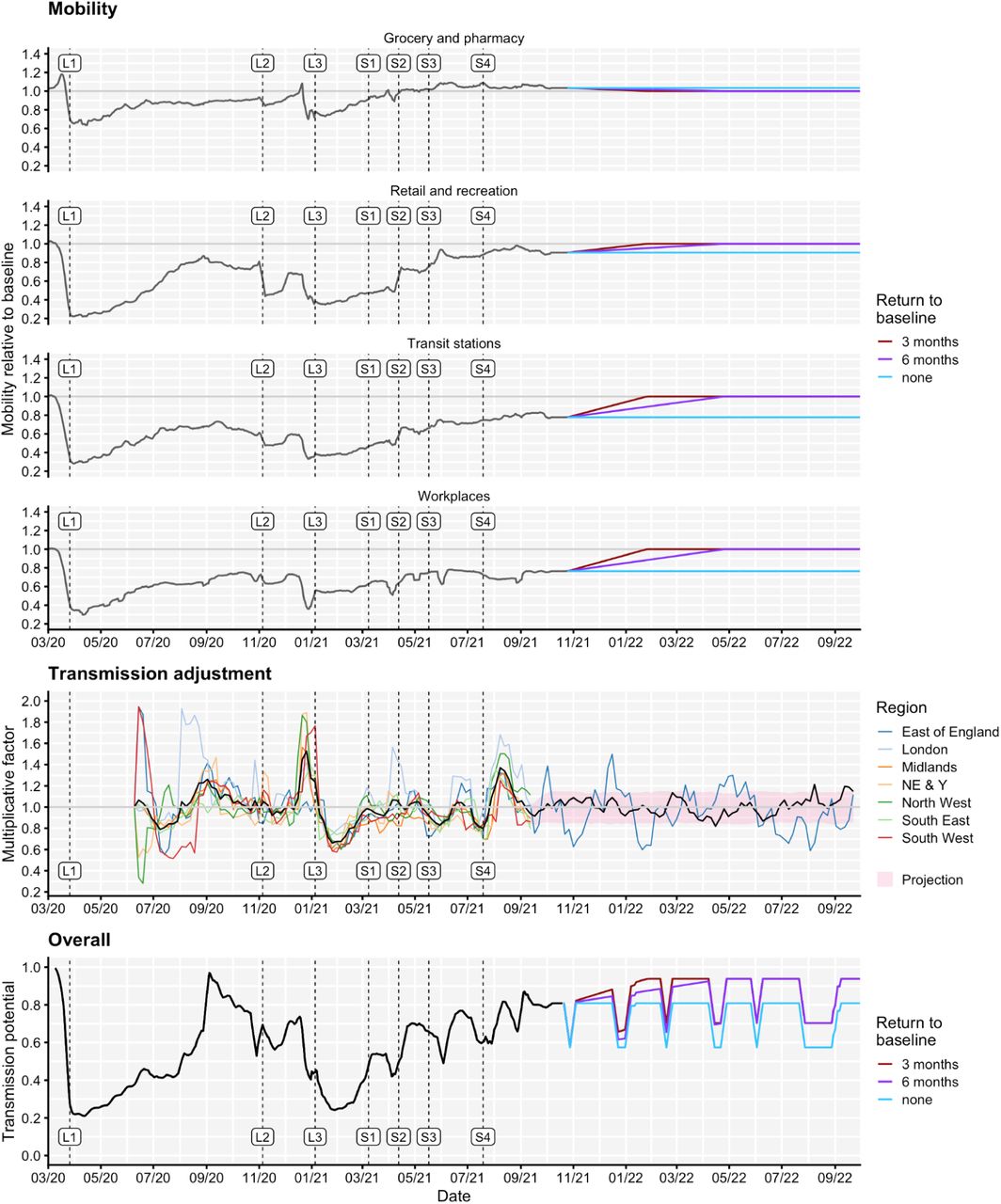
To capture historic behavioural changes, the model uses Google Community Mobility indices over time to derive contact rates for each NHS England region modelled, based upon a measured relationship between Google Mobility indices and age-specific contact rates as measured by the CoMix study, and in combination with school attendance data and assumptions about school schedules (Fig. 2). The model also fits a time-varying “transmission adjustment” component for each NHS England region in order to capture additional variability in transmission that is not explained by the mobility data (see Methods). The fitted transmission adjustment can be seen in the middle row of Fig. 2; there are notable sharp peaks around Christmas 2020 and towards the end of Summer 2021, as well as a deep trough around the lockdown in early 2021. To project behavioural changes forwards from October 2021 to September 2022, we combine various assumptions on future mobility changes (Fig. 2) with simulated trajectories for future transmission adjustments based on the historic fitted transmission adjustment (full details are given in the Methods section).
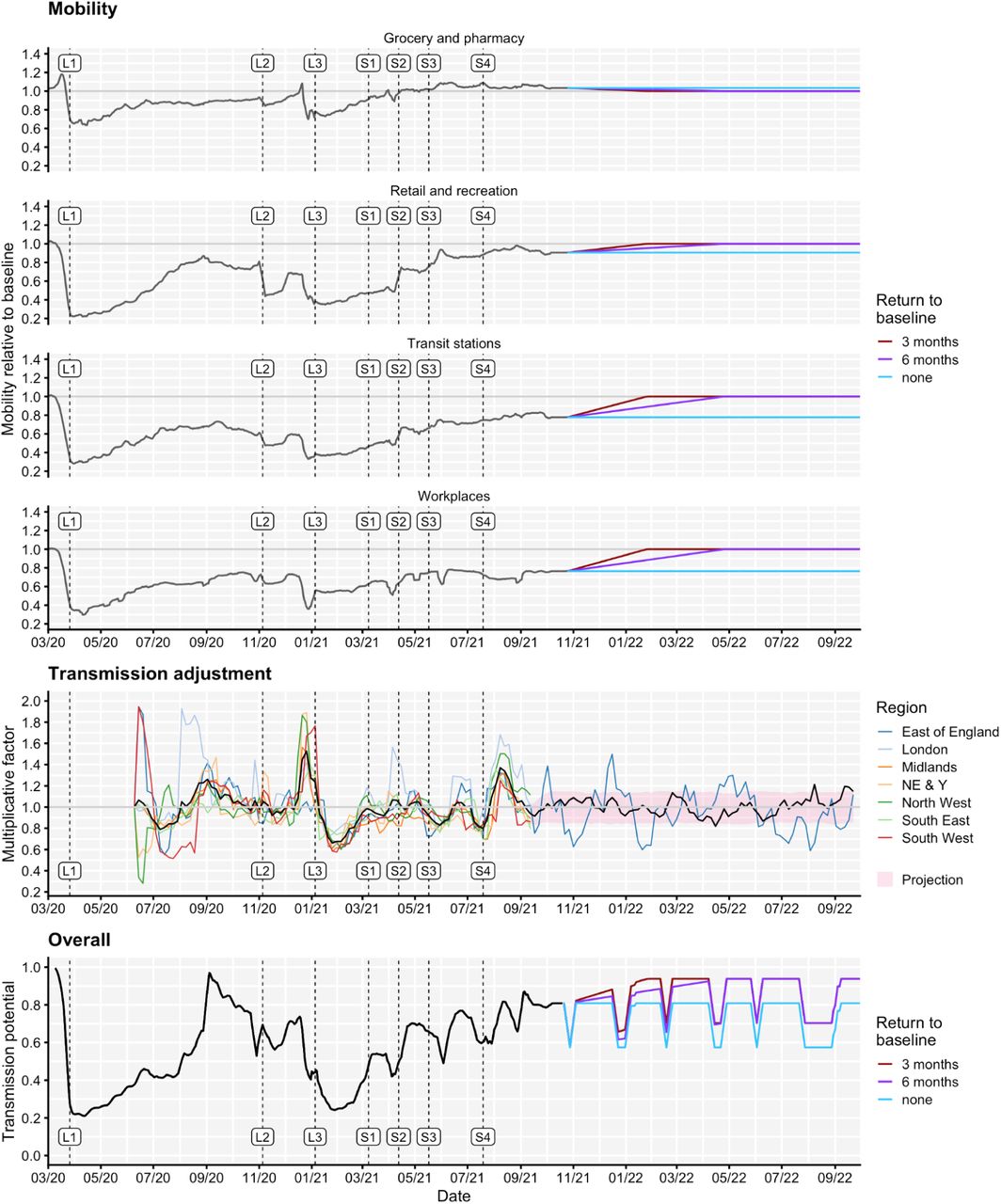
Top: Historic Google Community Mobility data (grey) and assumed future mobility in England for no change (blue), a 3-month return to pre-pandemic baseline levels (red) and a 6-month return to pre-pandemic baseline levels (purple) scenarios used for model projections. Mobility indices are measured relative to baseline mobility levels recorded during early 2020, prior to the COVID-19 pandemic. The beginning of each lockdown and each roadmap Step is marked with a vertical dashed line and ‘L’ and ‘S’ labels, respectively. Middle: Fitted transmission adjustments by NHS England region and the average across regions (black), example projection for East of England (blue) and mean (black line) + interquartile range (red shaded) for projected transmission adjustments. Bottom: The “transmission potential” captures the overall impact of mobility and transmission adjustments on the time-varying potential for effective transmission, ignoring the impact of immunity and novel variants, though including the impact of school vacation periods. NE & Y = North East & Yorkshire. NHS = National Health Service.
We present the majority of results here by plotting the median and interquantile ranges of a number of simulated future trajectories of SARS-CoV-2 transmission in England, but it is important to note that individual epidemic trajectories can fall outside of the model’s projection intervals (Fig. 3A). Some individual epidemic trajectories are projected to result in rapid exponential rises in transmission with large peaks that may require PHSMs to be implemented in response. A comparison of the projected cumulative number of SARS-CoV-2 infections, hospital admissions and deaths between October 2021 and September 2022 across all the scenarios considered here is shown in Fig. 4, along with detailed results related to each type of uncertainty in the Supplementary material (Figs. S4-S9). Although this work investigates the consequences of behavioural change, booster vaccination policies and waning vaccine protection, it is important to note that PHSMs also have the ability to suppress projected rises in transmission (Figs. 3B, 4, S4). A complete list of scenarios considered and key assumptions for each scenario is given in the Supplementary material (Table S6).
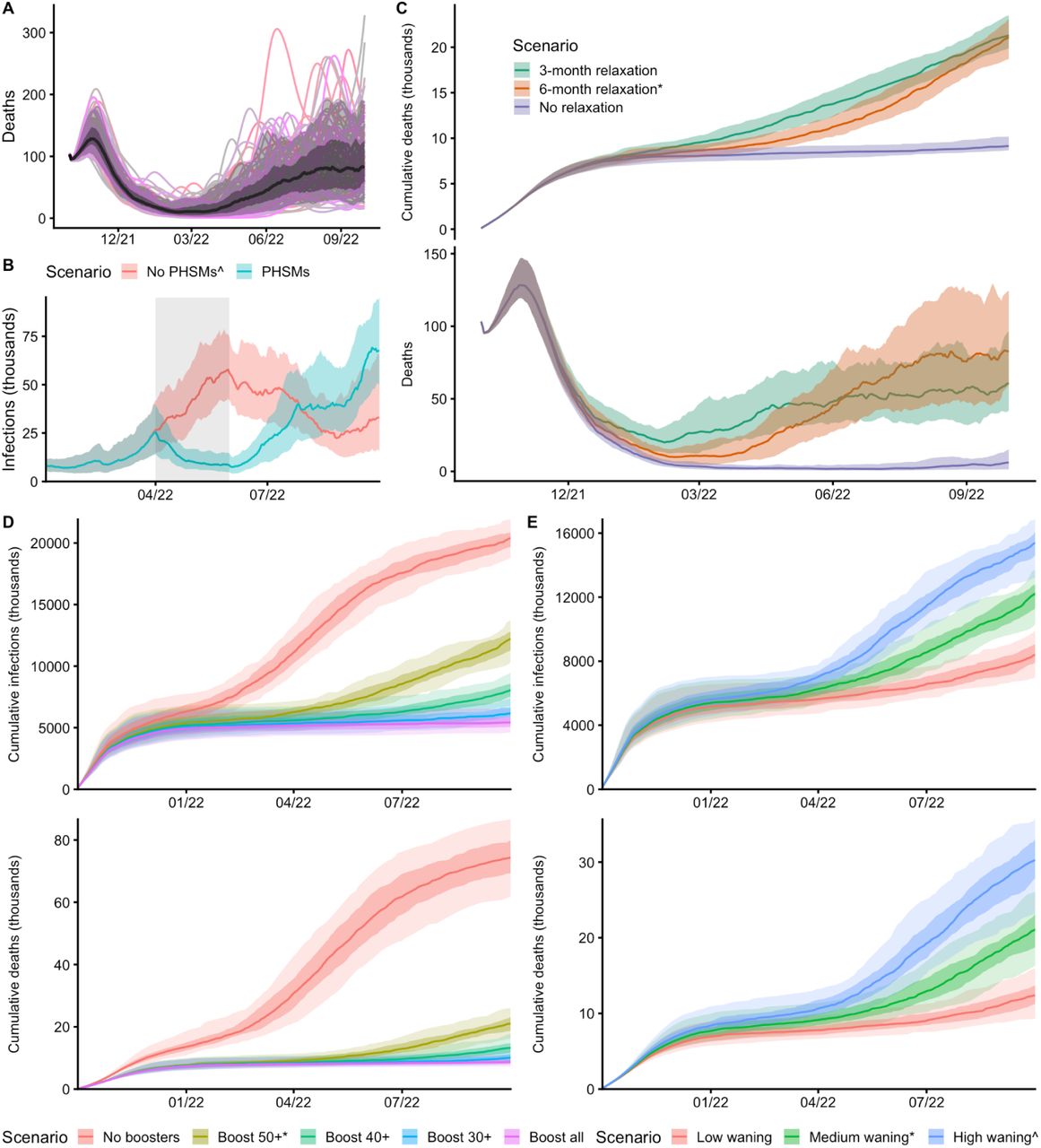
The central scenario is shown here which assumes a 6-month return to baseline mobility levels, medium waning of vaccine protection (Table S3), 90% of vaccinated individuals aged 50 and above receiving booster vaccinations and 20% seasonality from 1st April 2021. The black line shows the median trajectory of COVID-19 deaths over time, with the shaded areas showing the 50% and 90% interquantile ranges. Individual model trajectories are plotted in coloured lines. B: The effect of PHSMs on projected SARS-CoV-2 infections over time are shown with two scenarios. Both scenarios assume a 6-month return to baseline mobility levels, high waning of vaccine protection (Table S3), 90% of vaccinated individuals aged 50 and above receiving booster vaccinations and 20% seasonality from 1st April 2021. The PHSMs scenario implements a combination of three PHSMs (Figures 4, S7) between 1st April and 31st May 2022. C: The effect of behaviour on COVID-19 deaths and cumulative deaths over time is shown with three scenarios for future mobility: a 3-month and a 6-month return to baseline levels, and a no change scenario. All three scenarios assume medium waning (Table S3), 90% of vaccinated individuals aged 50 and above receiving booster vaccinations and 20% seasonality from 1st April 2021. D: The effect of booster vaccination policy on cumulative infections and deaths over time is shown with five scenarios for booster policies. All five scenarios assume a 6-month return to baseline mobility, medium waning (Table S3) and 20% seasonality from 1st April 2021. E: The effect of waning vaccine protection on cumulative infections and deaths over time is shown with three scenarios for waning (Table S3). All three scenarios assume a 6-month return to baseline mobility, 90% of vaccinated individuals aged 50 and above receiving booster vaccinations and 20% seasonality from 1st April 2021. Scenarios marked with an asterisk (*) are equivalent, and scenarios marked with a caret (^) are equivalent.

Each box plot shows the projected median, 5th, 25th, 75th and 95th percentile values across all simulations for the relevant scenario. Scenarios are coloured according to the result type (behaviour, booster vaccination policy, waning vaccine protection (Table S3), public health and social measures (PHSMs), seasonality, and vaccination policy for children). Behavioural scenarios assume medium waning vaccine protection (Table S3), 90% of vaccinated individuals aged 50 and above receiving booster vaccinations and 20% seasonality from 1st April 2021. Booster vaccination policy scenarios assume a 6-month return to baseline mobility levels, medium waning (Table S3), and 20% seasonality from 1st April 2021. Waning vaccine protection scenarios assume a 6-month return to baseline mobility levels, 90% of vaccinated individuals aged 50 and above receiving booster vaccinations and 20% seasonality from 1st April 2021. PHSM scenarios assume a 6-month return to baseline mobility levels, high waning vaccine protection (Table S3), and 20% seasonality from 1st April 2021. Seasonality scenarios assume a 6-month return to baseline mobility levels, medium waning vaccine protection (Table S3), and 90% of vaccinated individuals aged 50 and above receiving booster vaccinations. Vaccination of children scenarios assume a 6-month return to baseline mobility levels, medium waning vaccine protection (Table S3), 90% of individuals aged 50 and above receiving booster vaccinations and 20% seasonality from 1st April 2021. A full list of scenarios and assumptions is given in the supplementary material (Table S6). Scenarios marked with an asterisk (*) are equivalent, and scenarios marked with a caret (^) are equivalent.
A key uncertainty is future behaviour and assumptions about future levels of mobility greatly influence the projected dynamics of SARS-CoV-2 transmission into 2022 (Figs. 3C, 4, S4). We consider three scenarios for future mobility (no change, a 3-month and a 6-month return to pre-pandemic baseline levels, shown in Fig. 2) to capture this uncertainty. All behavioural change scenarios considered project a peak in SARS-CoV-2 transmission in late 2021 followed by a decline to very low levels of transmission in early 2022 (Fig. S4). This is due to depletion of susceptible individuals due to a high force of infection in England during Autumn 2021. The scenario assuming no change in mobility projects that transmission remains at low levels through most of 2022, with early increases being projected by September 2022. The largest difference in projected outcomes lies between the no change and return to baseline scenarios (Figs. 3C, 4, S4). However, the timing and speed of the return to baseline levels of mobility is important; a 3-month return to baseline mobility results in transmission rising sooner in 2022 and remaining flatter through the projected time horizon, whereas a 6-month return to baseline mobility levels leads to a later rise in transmission but a higher peaking epidemic (Figs. 3C, S4). Over shorter timescales, a more gradual return to baseline mobility decreases the total number of infections, hospital admissions, and deaths, but over long timescales there is less of a difference between different rates of returning to baseline (Fig. S4 tables). Both of the return to baseline mobility scenarios result in very similar cumulative numbers of SARS-CoV-2 infections, hospital admissions and deaths by the end of September 2022 (Figs. 3C, 4, S4). These differences can be explained by interactions between waning, seasonality, and mobility rates.
Other influential factors considered here are future policies on COVID-19 booster vaccinations and the rate at which vaccine protection wanes over time (Figs. 3D, 3E). Assuming a medium rate at which vaccine protection wanes, rolling out COVID-19 booster vaccinations has the largest overall effect in suppressing transmission of SARS-CoV-2 of all the scenarios considered (Fig. 4). Targeting booster vaccinations to individuals aged 50 years and above is estimated to have prevented around 50,000 deaths by September 2022, when compared with a counterfactual scenario where booster vaccinations were not implemented (Fig. 3D, S5). Scenarios where booster vaccinations are offered to sequentially younger age groups provide additional benefits in suppressing COVID-19 transmission into 2022, but with larger effects in reducing SARS-CoV-2 infections compared to reducing hospital admissions and deaths (Figs. 3D, 4, S5). Administering booster vaccinations to 90% of all individuals who receive two COVID-19 vaccinations is projected to suppress transmission of SARS-CoV-2 to low levels throughout the time horizon considered (Fig. S5), with 2.5 million less SARS-CoV-2 infections projected by September 2022, compared with the scenario offering booster vaccinations to individuals aged 40 and above, which is closest in line with the latest JCVI guidance8.
The extent to which vaccine protection wanes over time is a key uncertainty and different assumptions result in dramatically different projected transmission dynamics until September 2022 (Figs. 3E, 4, S6). We consider three waning vaccine protection scenarios for individuals who do not receive a third booster vaccination after their second COVID-19 vaccination: low, medium and high waning (Table S3). All three of these scenarios assume that 90% of vaccinated individuals aged 50 and above receive a booster vaccination. Low waning vaccine protection delays and reduces the projected resurgence in transmission, with 12,500 deaths projected to occur between October 2021 and September 2022 (Fig. S6 Table). The most extreme waning scenario considered results in a significant wave of transmission during the summer of 2022, with 30,300 deaths projected to occur within the same timescale, with the potential for more than 1000 hospitalisations and 200 deaths to occur per day in England at the peak of transmission (Fig. S6).
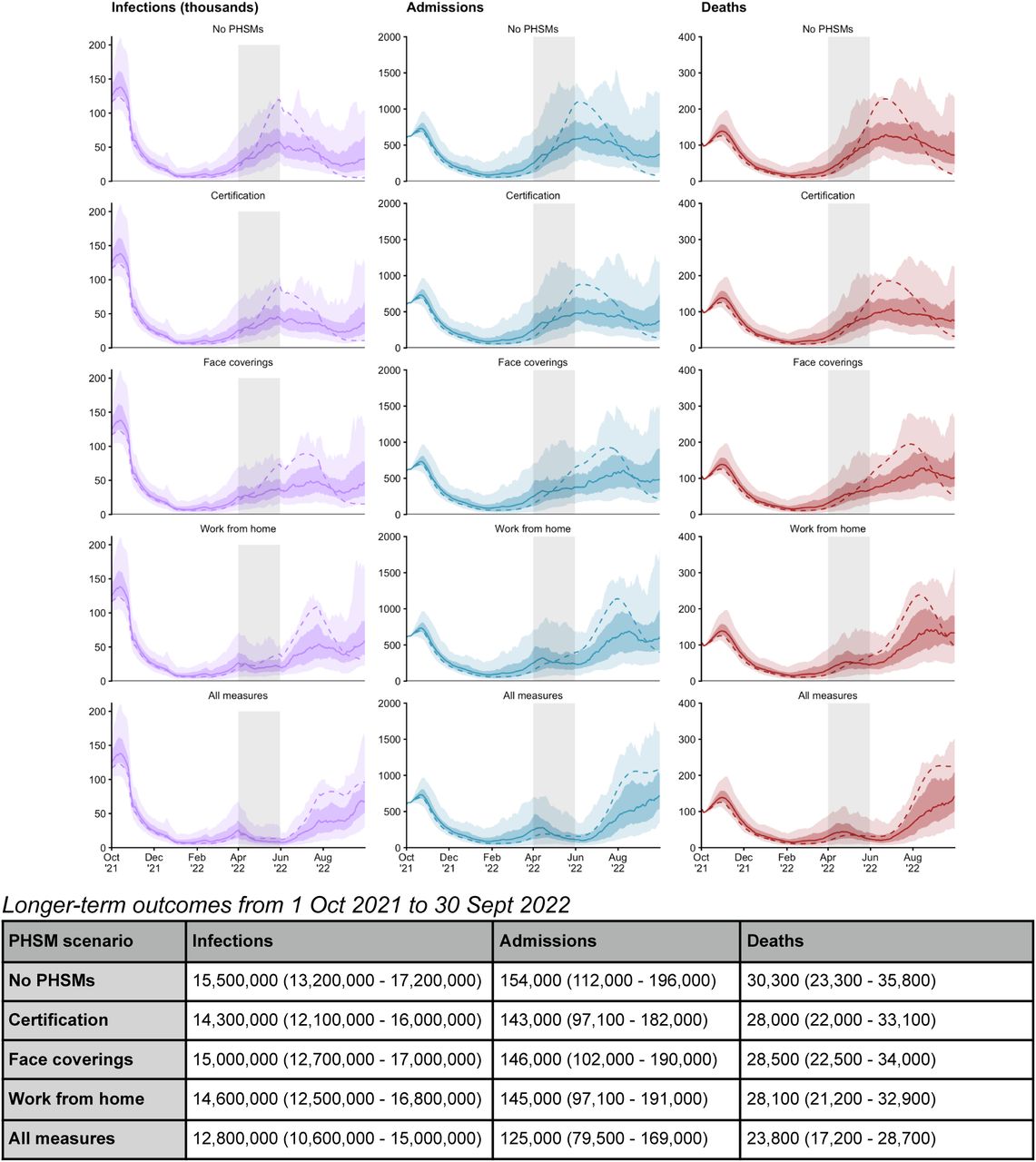
The majority of scenarios considered project rises in SARS-CoV-2 transmission to occur towards the spring and summer months of 2022, with more pessimistic assumptions related to behaviour change, booster vaccination policy and waning vaccine protection leading to more significant and/or earlier resurgences (Figs. S4-6). For the most extreme waning scenario, we consider the additional introduction of temporary public health and social measures between 1st April and 31st May 2022 (Fig. S7). Of the three PHSMs considered, a vaccine certification policy, modelled as leading to increased vaccine uptake in individuals aged 18-29, had the smallest impact on projected transmission to September 2022. Introducing a work-from-home policy, modelled by returning work-related mobility to the same levels that were recorded during the week beginning 15th of March 2021, had the strongest effect in suppressing transmission during the intervention period. A combination of vaccine certification, increased mask wearing and work-from-home policies is sufficient to bring the reproduction number below 1 for the duration of the intervention period and is projected to result in 6,500 fewer deaths between October 2021 and September 2022 than the equivalent scenario without the introduction of PHSMs (Fig. S7). However, the introduction of PHSMs is modelled as a temporary measure, and transmission is projected to resurge again following their removal, eventually increasing above the levels projected to occur without any PHSMs being introduced (Figs. 3B, S7).
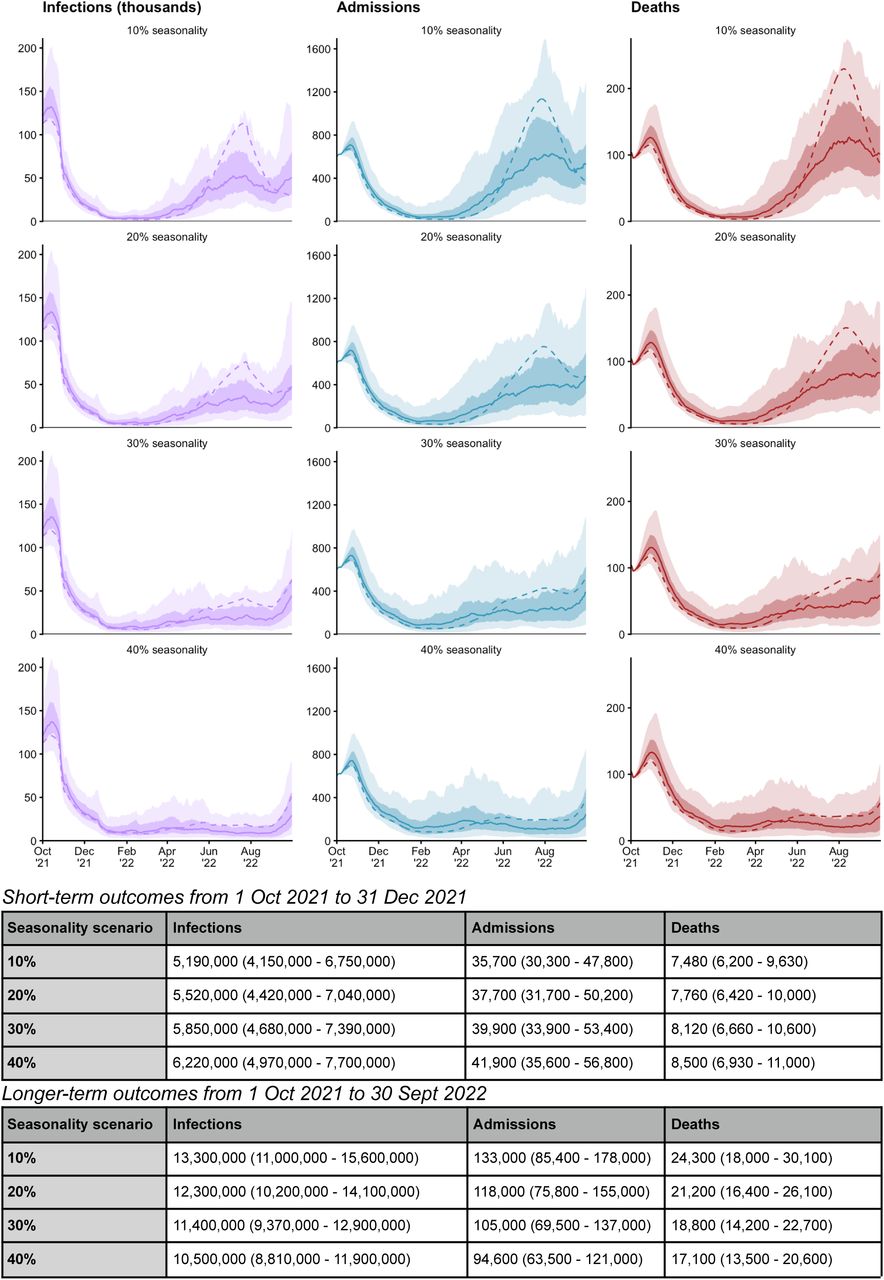
Different assumptions related to the extent of seasonality also influence the projected dynamics of SARS-CoV-2 transmission to September 2022 (Figs. 4, S8). Scenarios assuming more extreme seasonal effects result in smaller cumulative burdens between October 2021 and September 2022 (Fig. 4). However, scenarios assuming the most extreme seasonal effects appear to be resurging in September 2022 and may result in significant waves of transmission during the winter months of 2022-2023, far beyond the time horizons considered in this study. This effect can be observed by comparing short-term and longer-term outcomes; scenarios with greater seasonal effects are projected to result in more infections, hospitalisations and deaths between October and December 2021 but in less infections, hospitalisations and deaths between October 2021 and September 2022 (Fig. S8 Tables).
Finally, we consider a number of scenarios related to the vaccination of children aged 12 years and above and children aged 5 years and above (Figs. 4, S9). Of all the uncertainties considered here, using different assumptions related to the vaccination of children had the smallest overall effect in projected SARS-CoV-2 transmission until September 2022 (Fig. 4). Between October and December 2021, different vaccination policies resulted in minor differences in the projected number of hospital admissions only (Fig. S9 Table). Between October 2021 and September 2022, different vaccination policies were projected to result in small differences across infections, hospital admissions and deaths (Fig. S9 Table). Scenarios assuming both higher uptake of COVID-19 vaccinations in children aged 12 and above and aged 5 and above or vaccinating wider age ranges of children are projected to result in marginal reductions in infections, hospital admissions and deaths between October 2021 and September 2022 (Fig. S9 Table), but not to significantly alter projected transmission dynamics (Fig. S9). This is due to high levels of infection in the model in these age groups during the autumn of 2021 (Fig. S10).
Discussion
We have fitted a deterministic compartmental model of SARS-CoV-2 transmission to data on COVID-19 deaths, hospital admissions, hospital bed and ICU bed occupancy, PCR prevalence, sero-prevalence, and the emergence and spread of the Alpha B.1.1.7 and Delta B.1.617.2 variants, incorporating additional data on vaccination coverage and behaviour over time. Projecting forwards to September 2022, we have considered a number of uncertainties around behaviour, booster vaccination policy, waning levels of vaccine protection over time, seasonality, and different policy options for vaccination of children. We have also considered the temporary reintroduction of PHSMs to suppress future projected rises in SARS-CoV-2 transmission.
Modelled levels of immunity in England (both from natural infection and induced by COVID-19 vaccinations) suggest that SARS-CoV-2 transmission will fall in the Autumn of 2021, but there remains significant uncertainty around the extent and the timescale to which immunity wanes. In addition, the projected winter dynamics depend on the current wave of transmission being large enough to deplete most susceptible individuals. Our model has estimated the number of daily infections in October 2021 to be up to 3 times larger than the number of daily reported cases on the COVID-19 dashboard2. We also assume that all individuals being administered their first COVID-19 vaccinations go on to receive a second dose. Currently 12-15 year olds in England are being recommended the first COVID-19 vaccine dose only7.
The majority of scenarios considered project resurgences in transmission occurring later in 2022. However, none of these resurgences are expected to reach the levels of hospital admissions and deaths seen in 2020 and 2021, largely due to high levels of vaccine and natural protection in the population (Fig. S10). Large reductions in the levels of protection conferred by COVID-19 vaccines over time have the potential to lead to substantial resurgences in transmission, particularly if no measures are implemented in response. Administering booster vaccinations to all individuals who have received first and second COVID-19 vaccinations provides a medium- to long-term solution towards mitigating future resurgences of SARS-CoV-2 community transmission. The re-introduction of PHSMs such as work-from-home policies can suppress projected resurgences, but are only considered as temporary measures here. Once PHSMs are relaxed, SARS-CoV-2 transmission is projected to resurge again. However, delaying a resurgence can give time to introduce further measures, to increase vaccine uptake and to allow advances in treatment of COVID-19 to occur.
The World Health Organization has stated that “administration of booster doses will exacerbate inequities by driving up demand and consuming scarce supply while priority populations in some countries, or subnational settings, have not yet received a primary vaccination series”14. Given that England has largely relaxed PHSMs against COVID-19 since July 2021, and given current vaccine supply constraints globally, it may be more equitable to implement PHSMs in England to suppress SARS-CoV-2 transmission in the short-term whilst sharing vaccine doses with countries that have not yet vaccinated their most vulnerable populations with a primary dose.
There are a number of limitations in this work which are important to consider. The extent to which immunity from natural infection and from vaccination wanes is uncertain. Individuals may retain very long-term protection against severe outcomes, but have faster rates of waning against less severe outcomes such as mild or asymptomatic infection. We model waning vaccine protection in a way that initially allows protection against different outcomes to be reduced to different extents. Individuals can then return to being entirely susceptible from the vaccinated-and-waned state or from the naturally infected and recovered state (see assumed rates of waning in Table S4). We have parameterised waning rates in relation to measured reductions in protection against severe outcomes, but our assumption that individuals return to being completely naive to infection may still be overly pessimistic. We have not attempted to explore the dynamics of waning immunity from natural infection here in detail. Throughout, we assume identical levels of protection are conferred from natural infection and from vaccination across individuals of all ages. It is likely that protection will differ from person to person and that more clinically vulnerable individuals may have lower levels of protection or faster reductions in protection. Further, we do not consider any differences in vaccine coverage by risk group.
This work assumes that no new variants of SARS-CoV-2 possessing any kind of transmission advantage emerge in the future. As we have seen with the Alpha B.1.1.7 and Delta B.1.617.2 VOCs in England (Figs. S2, S3), novel VOCs with transmission advantages can spread to dominance very quickly, and this could have substantial implications for the future dynamics of COVID-19. In addition to future emergence of VOCs, it is impossible to predict future policy or behavioural changes with any certainty. It remains unclear whether mobility and behaviour will return to the same levels seen prior to the COVID-19 pandemic. We have considered one scenario where behaviour remains largely unchanged, and two scenarios in which mobility increases to pre-pandemic levels in either 3 months or 6 months to capture this uncertainty. In addition to longer-term changes, we are not able to forecast shorter-term behavioural changes that have been observed in the historic data, e.g. around Christmas of 2021 and during the Euro 2020 football tournament in the summer of 2021 (Fig. 2). Behavioural changes can also occur in response to awareness of a growing or declining epidemic15, 16, which is something that we do not capture in any forward projections.
It is clear that the extent to which immunity, both derived from natural infection and from COVID-19 vaccination, wanes will become extremely important in the medium- to long-term. It is crucial to improve our current understanding of the dynamics of SARS-CoV-2 immunity and to consider the consequences of this on community transmission in the context of varying levels of PHSMs and vaccination coverage, both in England and worldwide.
Methods
Epidemiological model
We use an age-structured and region-specific deterministic compartmental model of SARS-CoV-2 transmission, building on previous work17–19. Geographic structure is by NHS England region and age groups are divided into 5-year age bands from 0–4 to 70–74 years, with an additional age group comprising individuals aged 75 years and over. The model tracks three variants of SARS-CoV-2 to capture wild-type, Alpha B.1.1.7 and Delta B.1.617.2 variants separately. We model vaccination against SARS-CoV-2 with separate compartments for two vaccine products, for each of the viral vector and mRNA-based COVID-19 vaccines in use in England. The model also captures the administration of booster vaccinations, and waning immunity derived from natural infection and vaccination. A full description of assumptions related to vaccine protection against different outcomes and waning immunity is provided in the Supplementary Material and in Tables S2 - S4.
Hospital admissions and occupancy data were provided by NHS England and deaths, immunisations and variant data were provided by the UK Health Security Agency (UKHSA). These data sources are unpublished and not public, but are closely aligned with healthcare, deaths and vaccinations data on the UK Government COVID-19 Dashboard2. Seroprevalence data were obtained from the UK Biobank20 and the REACT-2 study21, and seroprevalence and PCR positivity data were obtained from the the Office for National Statistics COVID-19 Infection Survey (ONS-CIS)13, 22.
The age-specific probability of clinical symptoms is adopted from a study using data from 6 countries23. The age-specific probability of hospital admission, ICU admission, and death given infection are fitted to data from England, with the relative rates by age group based on data collected by a large meta-analysis of the COVID-19 infection fatality rate24 and based on data collected by ISARIC (the CO-CIN study) for England17, then adjusted to better match observed hospitalisations and deaths in England (see Model fitting). Each of these age-specific probabilities of severe outcomes is allowed to vary over the course of the epidemic in England and vary between pre-existing variants and Alpha B.1.1.7. For the third variant Delta B.1.617.2, we assume that the probability of severe outcomes is twice that of Alpha B.1.1.7, in line with estimates from Public Health Scotland and UKHSA25. A full description of fitted and assumed parameters is provided in Tables S5A and S5B.
The model uses Google Community Mobility data26 to capture mobility in various settings: workplaces, retail & recreation venues, transit stations, and grocery & pharmacy locations. In turn, the relationship between mobility data and social contact rates is derived from the historical relationship between Google Community Mobility indices and social contact rates as measured by the CoMix study in 202017. School openings and closings are accounted for in contacts among school-aged children, university-aged young adults and school/university staff. We assume that schools in England follow their traditional schedules (i.e. are closed during holiday periods), and we combine these assumptions with school attendance data in England up to July 202127. To reflect the introduction of mass testing within educational facilities in the Spring of 2021, we have assumed an additional 30% reduction in transmission related to educational settings between the reopening of schools on 8th March 2021 and school closures in July 2021. This reduction in transmission is reflected in the model with a 30% reduction in school-related contacts. Seasonality is modelled as a sinusoidally-varying multiplier on transmission with the peak occurring on January 1st and the trough on July 1st of each year. By default, we assume the amplitude of the seasonal component is 20% from trough to peak.
Model fitting
The model is fitted using a two-stage process. In the first stage, the model parameters are fitted by Bayesian inference using Markov chain Monte Carlo (MCMC) to reported regional data on hospital admissions, hospital and intensive care unit (ICU) bed occupancy, seroprevalence, PCR positivity, and deaths within 28 days of a patient’s first positive SARS-CoV-2 test, as well as to data tracking the emergence and spread of the Alpha B.1.1.7 variant (the frequency of S-gene target failure in PCR tests) in late 2020 and of the Delta B.1.617.2 variant (the frequency of Delta in genomic sequencing data) in 2021. We use the DE-MCMC algorithm28 implemented in C++ (see analysis code). The introduction time and relative transmissibility of both the Alpha and Delta variants are fitted for each geographic region in the model. We use data recording the number of first COVID-19 vaccine doses delivered by age, geography and vaccine product from 8th December 2020 to 3rd October 2021 to inform the fraction of first-dose vaccinated individuals in each age group, NHS England region and by vaccine type over time. Additionally, in this initial stage, 14 additional parameters are fitted to define a “transmission multiplier” function, with each of the 14 parameters defining a stepwise change in transmission at fixed six-week intervals from 12th April 2020 to 10th October 2021. This transmission multiplier function allows the modelled epidemic trajectory to better capture changes in SARS-CoV-2 transmission over time, and reflects residual changes in transmission that are not captured by mobility data alone, e.g. as resulting from changes in personal protective behaviours such as mask-wearing or from changes in social behaviour such as during holidays.
In the second stage of model fitting, a particle filtering algorithm29 is used to refine the “rough” transmission multiplier function, while holding other fitted model parameters constant, to achieve a more fine-scaled function with stepwise changes to the transmission multiplier every 5 days, instead of the cruder 6-week increment used in the initial stage of fitting. In the second stage, the transmission multiplier is fitted as a random walk on a logarithmic scale, that is, multiplicative increments to the transmission multiplier are proposed rather than absolute levels.
The same likelihood is used for Bayesian inference in both stages of the model fitting process. In particular, the likelihood allows the infection fatality rate (IFR), infection hospitalisation rate (IHR), and infection critical-illness rate (ICR) to vary over the course of the epidemic, to reflect changes in treatment success, admissions criteria, and availability of hospital resources over time. To achieve this, the model’s initial output of deaths and hospital burdens, which are based upon a fixed IFR, IHR, and ICR (except as modified by variant-specific characteristics and by vaccine protection), are treated as the prior expectation for deaths and hospital burdens on each day. This expectation is used as the mean of a gamma distribution, with standard deviation set to 0.3 times the mean, which, in turn, is taken as the prior distribution for the mean of a Poisson distribution from which the observed burden for a given day is assumed to be drawn. This process allows the IFR/IHR/ICR to change over time, while not straying too far from the expected burden based upon the underlying fixed IFR/IHR/ICR.
Model assumptions
Vaccine effectiveness
We base our vaccine effectiveness assumptions on the latest available evidence (Tables S2, S7, S8). These may be subject to change in future work, as new evidence emerges. We currently treat individuals who have been and will be vaccinated with Moderna vaccines the same as individuals receiving Pfizer vaccines. We model individuals who have received different vaccine products (e.g. AstraZeneca and Pfizer/Moderna) and one or two vaccine doses separately, assuming separate efficacy estimates for each category. We additionally consider individuals who have received two vaccine doses but no booster dose as having reduced levels of protection, with various scenarios considered in relation to vaccine protection (Table S3).
We model vaccine protection against five separate outcomes: infection, disease (i.e. symptomatic infection), hospitalisation, mortality and onward transmission following a breakthrough infection (i.e. when an individual who has vaccine protection becomes infected). We assume the same vaccine effectiveness for the first two SARS-CoV-2 variants considered in the model (pre-Alpha B.1.1.7 and Alpha B.1.1.7), and separate specific vaccine effectiveness estimates for the Delta B.1.617.2 variant, shown in Table S2. Tables S7 and S8 show summaries of the relevant evidence we have used to guide our assumptions on vaccine effectiveness against the Alpha B.1.1.7 and pre-existing variants of SARS-CoV-2 and against the Delta B.1.617.2 variant, respectively.
Our assumptions about the levels of vaccine protection for individuals who have received two vaccine doses but no booster dose, and their protection has waned, are shown in Table S3. To parametrise these reductions in vaccine protection, we have referred to Andrews et al.12, using the measured percentage change in protection for ages 16+ against symptomatic disease and hospitalisation between week 1 and 20+ weeks and against death between week 1 and 15-19 weeks. We have used the vaccine product specific percentage changes in protection against symptomatic disease to scale our estimates against infection and disease, and the percentage changes in protection against hospitalisation and death to scale our estimates against hospitalisation and death, respectively. We have calculated the mean percentage change across these three values for each vaccine product and used this change to scale our estimates for vaccine protection against onward transmission. Since we model an individual’s average duration in second dose protection as 29.3 weeks, before they are either boosted and remain at two-dose levels of protection or are not boosted and wane, we consider these baseline assumptions for the levels of protection in the waned state as being optimistic, and we refer to this as the ‘less waning’ scenario. Therefore, we also consider an additional two scenarios for two-dose vaccinated-and-waned individuals, where we assume 25% (moderate waning) and 50% (more waning) reductions to the waned estimates shown in Table S2.
Waning immunity
We model waning protection from SARS-CoV-2 infection developed from natural infection and vaccination. For waning protection from natural infection, we assume identical rates of waning for all three virus variants and for all age groups (Table S4). Once individuals who have recovered from natural infection wane, they return to a susceptible disease state; thus we model waning of natural immunity against different endpoints (infection, disease, hospitalisation, deaths and onward transmission) at the same rate. In contrast to previous reports, we no longer model individuals waning from second vaccination protection directly back to being susceptible. To account for booster vaccinations, upon leaving the second dose state, individuals either receive a booster vaccine and return to second dose levels of protection, or move into a third state with reduced levels of vaccine protection across different outcomes (see Table S3). This third state corresponds to individuals who have received two vaccine doses followed by waning of their vaccine protection. Once individuals have moved into this waned state with reduced levels of vaccine protection, they are also allowed to wane back to being susceptible, with different rates considered for each vaccine product (Table S4). The assumed percentage loss in reduction here is based on measured percentage changes in vaccine protection against hospitalisation for each vaccine product in Andrews et al.12
Vaccination, waning and intervention scenarios
To produce forward projections, the model requires information about future contact rates and vaccination rates. We base our assumptions on how social contact rates might be expected to change by referring to historical mobility data26 and making assumptions about future mobility until September 2022 (Fig. 2). Mobility levels have been gradually increasing since March 2022 but have still not returned to pre-pandemic levels. Hence we consider three scenarios: we project current levels of mobility forwards (i.e. no change), and we consider a return to pre-pandemic baseline levels of mobility within a period of 3 months and a period of 6 months. Where we consider the introduction of PHSMs such as increases in mask-wearing and advice to work from home, we introduce changes to either all contacts or work-related contacts.
The time-varying transmission multiplier also needs to be projected forwards for model projections. This is done by using the R package forecast30 to fit an ARIMA model to the fitted transmission multiplier function (using the function auto.arima), then using random forecasts of the resulting ARIMA model for each new projection. This process of using different realisations of the projected transmission multiplier is what produces most of the variability among different runs of each scenario (Fig. 3A).
For future first-dose vaccinations, we generate vaccine schedules according to assumed future vaccine supply (i.e. number of doses available) and uptake limits per 5-year age group. We assume that first-dose vaccination uptake limits in individuals aged 20 years and above have already been reached, so no future first doses are delivered to these age groups. Our basecase scenarios assume that uptake is limited at 70% for individuals aged 12-19, delivering future first doses first to the 15-19 age group up to the uptake limit, followed by 12-14 year olds. Future first doses per day are distributed into the seven NHS England regions in proportion to population size. The allocated number of first doses per day, per region and per age group are divided into specified proportions of vaccine products relevant to each age group. Any doses remaining after this process are carried over to the next age group down (up to the relevant uptake limit), the next NHS England region, or the next day, or are left unallocated in the schedule and recorded as leftover doses.
Individuals remain in first- and second-dose vaccine states for durations drawn from pre-specified waiting time distributions. The distribution for the time spent in the first-dose vaccine state is based on measured delays between first and second doses in the UKHSA vaccination data, separated into two periods (before and after the JCVI issued guidance on widening the dosing gap from 3 weeks to a maximum of 12 weeks). Upon leaving the first-dose vaccine state, individuals transition into the second-dose vaccine state with increased levels of protection (Table S2). The distribution governing the duration that individuals have second-dose levels of vaccine protection is chosen to match the time between the start of the COVID-19 vaccination rollout (8th December 2020) and the start of the COVID-19 booster dose rollout (24th September 2021) less the assumed average duration of first-dose protection. Upon leaving the second-dose vaccine state, individuals either move into a vaccinated-and-waned state with reduced levels of protection specific to the vaccine they received (Table S3), or receive a booster vaccination and return to second-dose levels of protection assumed for the mRNA vaccines (Table S2). This assumption reflects the fact that all booster vaccinations in England are either the Pfizer/BioNTech or Moderna mRNA vaccines and evidence finding higher immunogenicity for individuals receiving Pfizer/BioNTech following Oxford-AstraZeneca, compared with individuals receiving both Oxford-AstraZeneca vaccine doses31.
For modelling potential PHSMs, we use the high waning scenario from Figure 3 in the main text (see also Table S3) as a baseline to represent a larger wave of infection. We assume that the measures announced are temporary, and are in force between 1st April and 31st May 2022.
We consider three potential contingency measures. “Certification” represents the introduction of vaccination or testing requirements for nightclub attendance. We model the impact of the certification policy by assuming that it will lead to an increase in vaccination rates among young people, as has been observed in some other European countries32. Certification policy in France was associated with a 2.5% increase in uptake across the entire population, particularly in ages 12-29. We assume that a similar policy in England could also increase vaccine uptake by 2.5%, specifically in individuals aged 18-29, and that this increase in uptake would occur between 14 days before and 7 days after the start of the contingency period.
“Face coverings” represents the reintroduction of mask-wearing. Since late August 2021, mask wearing in England has decreased by approximately 30%33. We assume that this decrease could be completely reversed by the face covering measure, and that this would result in a 7.5% reduction in R over the contingency period, comparable to the effect size measured in a regression analysis across 92 regions34 and a cluster randomized trial in Bangladesh35.
Finally, “Work from home” represents the reimposition of work from home guidance over the contingency period. We model this by returning work mobility indices to their value the week of March 15th 2021, after Step 1 of the roadmap.
Vaccine schedules
First-dose vaccine schedules are generated by combining PHE/UKHSA data on vaccines delivered up to the 3rd of October 2021 in England with future schedules based on a number of assumptions related to vaccine product distribution, vaccine supply and vaccine uptake. The number of future first doses supplied for each day in the schedule are distributed into the seven NHS England regions according to the population size of each region. Existing first-dose vaccination uptake for ages 20+ are used as uptake limits such that no future first doses are delivered to these age groups. For central scenarios considered here, we assume uptake is limited at 70% for individuals aged 12-19, delivering future first doses first to the 15-19 age group up to the uptake limit followed by 12-14 year olds. The allocated number of first doses per day, per region and per age group are divided into specified proportions of vaccine products relevant to each age group (see ‘Vaccine mix’ section). If doses are remaining after this process, leftover doses are carried over to either the next age group down up to the relevant uptake limit, the next NHS England region, the next day, or are not allocated in the schedule and are recorded as leftover doses.
First-dose vaccinated individuals transition into second dose protection according to a distribution controlling the duration of vaccinated individuals remaining at first-dose levels of protection. This distribution is chosen according to measured delays between first and second doses in the PHE/UKHSA vaccination data, separated into two periods (before and after the JCVI issued guidance on widening the dosing gap from 3 weeks to a maximum of 12 weeks). The duration that individuals have second-dose levels of protection is chosen to match the time between the start of the COVID-19 vaccination rollout (8th December 2020) and the start of the COVID-19 booster dose rollout (24th September 2021), less the time duration already assumed at first dose levels of protection. At the end of their second dose protection, individuals either receive booster doses and retain second-dose levels of protection, or move into a waned state with reduced levels of vaccine protection.
For projecting vaccination forwards, future first-dose vaccine supply is assumed to be 150,000 doses per week for England. The following proportions of each vaccine product are used in the vaccine schedules projected forwards: 75% Pfizer and 25% Moderna for <40 year olds, and 60% AstraZeneca, 30% Pfizer and 10% Moderna for 40+ year olds.
Contributions
RCB and NGD accessed and verified the data and conducted the analyses. All authors contributed to study design and drafting of the manuscript.
Declaration of interests
RCB, NGD, MJ and WJE are participants of the UK’s Scientific Pandemic Influenza Group on Modelling. WJE attends the UK’s Scientific Advisory Group for Emergencies. All authors declare no competing interests.
See supplementary material for working group authors and acknowledgments.
Statement on data availability
Analysis code and data will be made available upon publication at: https://github.com/rosannaclairebarnard/newcovid3
Funding statement
The following funding sources are acknowledged as providing funding for the named authors. This project has received funding from the European Union’s Horizon 2020 research and innovation programme - project EpiPose (101003688: RCB, MJ, WJE) and the UK Medical Research Council (MC_PC_19065: NGD, WJE). It was also partly funded by the Bill & Melinda Gates Foundation (INV-003174 and INV-016832: MJ) and the National Institute for Health Research (NIHR) (Health Protection Research Unit for Immunisation NIHR200929: NGD, MJ; Health Protection Research Unit in Modelling and Health Economics NIHR200908: MJ, WJE; PR-OD-1017-20002: WJE).
Ethics
Ethical approval for this research was given by the London School of Hygiene & Tropical Medicine Ethics Committee, project ID: 22828.
Supplementary material

Black lines show reported data, with vertical black lines showing 95% confidence intervals for PCR prevalence and seroprevalence estimates. Coloured lines and shaded areas show medians and 90% interquantile ranges from the fitted model. COVID-19 deaths data was provided by the UK Health Security Agency (UKHSA) and hospital admissions, hospital and ICU bed occupancy data was provided by NHS England. These data sources are unpublished and not publicly available, but are closely aligned with the UK Government’s COVID-19 dashboard2. PCR prevalence data was obtained from the Office for National Statistics’ COVID-19 Infection Survey (ONS-CIS)13. Seroprevalence data was obtained from the UK Biobank36, REACT-2 study37 and from the ONS-CIS13, 22. ICU = intensive care unit. NHS = National Health Service.

Black lines show reported data, with grey shaded regions showing 95% confidence intervals for the relative frequency of S-gene target failure in Pillar 2 PCR confirmed cases. Coloured lines and shaded areas show medians and 95% interquantile ranges from the fitted model. S-gene target failure data was provided by the UK Health Security Agency (UKHSA). This data source is unpublished and not publicly available. NHS = National Health Service.

Black lines show reported data, with grey shaded regions showing 95% confidence intervals for the relative frequency of Delta B.1.617.2 variant of concern in sequenced Pillar 2 PCR confirmed cases. Coloured lines and shaded areas show medians and 95% interquantile ranges from the fitted model. Sequencing data was provided by the UK Health Security Agency (UKHSA). This data source is unpublished and not publicly available. NHS = National Health Service.

Top: Possible trajectories for infections, admissions, and deaths are simulated for different rates of return to pre-pandemic baseline levels. The shaded areas and solid lines show the 90% interquantile range, the 50% interquantile range, and the median for each time point, while the dashed line shows one sample trajectory. All scenarios assume moderate waning of vaccine protection (see Table S3), 90% of individuals aged 50 and above who are vaccinated against COVID-19 receive additional booster vaccines, and 20% seasonality introduced from 1st April 2021. Tables: the total number of infections, admissions, and deaths, over the shorter term (October to December 2021) and the longer term (October 2021 to September 2022), shown to 3 significant figures.

Top: Possible trajectories for SARS-CoV-2 infections, hospital admissions and deaths are simulated until September 2022, with different assumptions used for age groups receiving COVID-19 booster vaccinations. The shaded areas and solid lines show the 90% interquantile range, the 50% interquantile range, and the median for each time point, while the dashed line shows a single sample trajectory. All scenarios assume that mobility returns to pre-pandemic baseline levels over a 6-month period, a medium rate of waning protection conferred by vaccines (Table S3), and seasonality of 20% is introduced from 1st April 2021. The ‘boosters for all’ scenario is modelled as 90% of all individuals who receive initial COVID-19 vaccination being offered a booster vaccine at least 6 months following their second dose. Tables: the total number of infections, admissions, and deaths, over the shorter term (October to December 2021) and the longer term (October 2021 to September 2022), shown to 3 significant figures.

Top: Possible trajectories for SARS-CoV-2 infections, hospital admissions and deaths are simulated until September 2022, with different assumptions used for the rate that vaccine protection wanes for individuals who do not receive a booster vaccination. The shaded areas and solid lines show the 90% interquantile range, the 50% interquantile range, and the median for each time point, while the dashed line shows a single sample trajectory. Assumptions for the low, medium and high waning scenarios are shown in Table S3. All scenarios assume that mobility returns to pre-pandemic baseline levels over a 6-month period, 90% of vaccinated individuals aged 50 and above receive a booster vaccination, and seasonality of 20% is introduced from 1st April 2021. Tables: the total number of infections, admissions, and deaths, over the shorter term (October to December 2021) and the longer term (October 2021 to September 2022), shown to 3 significant figures.
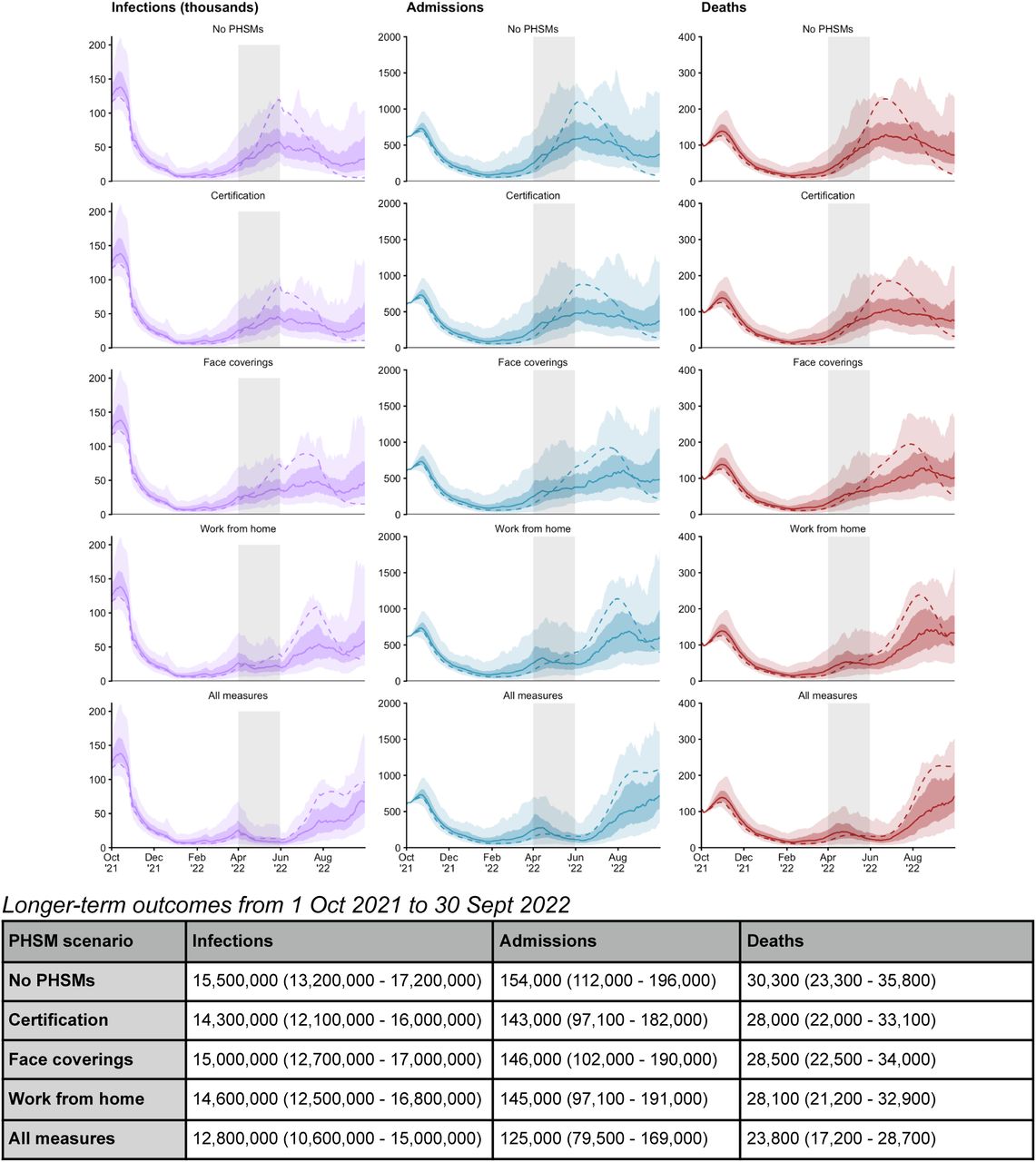
Top: Possible trajectories for SARS-CoV-2 infections, hospital admissions and deaths are simulated until September 2022, with different public health and social measures introduced between 1st April and 31st May 2022 (grey shaded rectangle) to suppress projected rises in transmission. The shaded areas and solid lines show the 90% interquantile range, the 50% interquantile range, and the median for each time point, while the dashed line shows a single sample trajectory. All scenarios shown assume mobility returns to pre-pandemic baseline levels over a 6-month period, a high rate of waning vaccine protection for individuals who don’t receive a booster vaccination (Table S3), 90% of vaccinated individuals aged 50 and above receive a booster vaccination, and seasonality of 20% is introduced from 1st April 2021. Table: the total number of infections, admissions, and deaths between October 2021 and September 2022, shown to 3 significant figures.

Top: Possible trajectories for SARS-CoV-2 infections, hospital admissions and deaths are simulated until September 2022, with different assumptions made for the extent of seasonality in transmission. From top to bottom: 10%, 20%, 30% and 40% seasonality is introduced from 1st April 2021. The shaded areas and solid lines show the 90% interquantile range, the 50% interquantile range, and the median for each time point, while the dashed line shows a single sample trajectory. All scenarios shown assume mobility returns to pre-pandemic baseline levels over a 6-month period, a medium rate of waning vaccine protection for individuals who don’t receive a booster vaccination (Table S3), and 90% of vaccinated individuals aged 50 and above receive a booster vaccination. Tables: the total number of infections, admissions, and deaths, over the shorter term (October to December 2021) and the longer term (October 2021 to September 2022), shown to 3 significant figures.

Top: Possible trajectories for SARS-CoV-2 infections, hospital admissions and deaths are simulated until September 2022, with different assumptions made for vaccination strategies of adolescents and children and with different levels of vaccination coverage in those age groups. From top to bottom: vaccinating children aged 12-15 at 70% uptake and at 50% uptake, and vaccinating children aged 5 and above at 70% uptake and at 50% uptake. The shaded areas and solid lines show the 90% interquantile range, the 50% interquantile range, and the median for each time point, while the dashed line shows a single sample trajectory. All scenarios shown assume mobility returns to pre-pandemic baseline levels over a 6-month period, a medium rate of waning vaccine protection for individuals who don’t receive a booster vaccination (Table S3), 90% of vaccinated individuals aged 50 and above receive a booster vaccination, and seasonality of 20% is introduced from 1st April 2021. Tables: the total number of infections, admissions, and deaths, over the shorter term (October to December 2021) and the longer term (October 2021 to September 2022), shown to 3 significant figures.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Each panel shows the proportion of individuals in each age group who are: currently susceptible, currently infectious, naturally protected (including individuals who have been both vaccinated and have natural protection due to infection prior to or after vaccination), vaccine protected with 1 dose, vaccine protected with 2 doses, and partially vaccine protected with waned vaccine protection six months after the second dose. Note that, due to waning of both natural and vaccine protection back to the fully-susceptible state, the susceptible proportion does not represent the fraction of each age group that has never been infected or vaccinated, as it includes some people who have been infected or vaccinated but have completely lost their protection. The “base case” scenario (3-month return to baseline, 90% booster uptake among over-50s who have received their second dose, medium vaccine waning, 70% vaccine uptake in 12–15-year-olds) is shown up to December 31, 2021.
Scenarios are listed in the same order as Figure 4. Scenarios marked with an asterisk (*) and a caret (^) are equivalent. For the public health and social measures (PHSMs) scenarios, details related to each specific measure or combination of measures considered are given in the online Methods section. For the vaccine scenarios considering vaccination of children of different age ranges and coverage levels, a unique vaccine schedule was generated for each scenario, according to the specified age range and coverage levels, as described in the online Methods section.
Working group authors and acknowledgements
CMMID COVID-19 Working Group
The following authors were part of the Centre for Mathematical Modelling of Infectious Disease COVID-19 working group. Each contributed in processing, cleaning and interpretation of data, interpreted findings, contributed to the manuscript, and approved the work for publication: James D Munday, Rachel Lowe, Gwenan M Knight, Quentin J Leclerc, Damien C Tully, David Hodgson, Rachael Pung, Joel Hellewell, Mihaly Koltai, David Simons, Kaja Abbas, Adam J Kucharski, Simon R Procter, Frank G Sandmann, Carl A B Pearson, Kiesha Prem, Alicia Showering, Sophie R Meakin, Kathleen O’Reilly, Ciara V McCarthy, Matthew Quaife, Kerry LM Wong, Yalda Jafari, Arminder K Deol, Rein M G J Houben, Charlie Diamond, Thibaut Jombart, C Julian Villabona-Arenas, William Waites, Rosalind M Eggo, Akira Endo, Hamish P Gibbs, Petra Klepac, Jack Williams, Billy J Quilty, Oliver Brady, Jon C Emery, Katherine E Atkins, Lloyd A C Chapman, Katharine Sherratt, Sam Abbott, Nikos I Bosse, Paul Mee, Sebastian Funk, Jiayao Lei, Yang Liu, Stefan Flasche, James W Rudge, Fiona Yueqian Sun, Graham Medley, Timothy W Russell, Amy Gimma, Stéphane Hué, Christopher I Jarvis, Emilie Finch and Samuel Clifford.
CMMID COVID-19 Working Group funding statements
PK (Royal Society: RP\EA\180004, European Commission: 101003688), TJ (Global Challenges Research Fund: ES/P010873/1, UK Public Health Rapid Support Team, NIHR: Health Protection Research Unit for Modelling Methodology HPRU-2012-10096, UK MRC: MC_PC_19065), AG (European Commission: 101003688), SFlasche (Wellcome Trust: 208812/Z/17/Z), RL (Royal Society: Dorothy Hodgkin Fellowship), DH (NIHR: 1R01AI141534-01A1), AJK (Wellcome Trust: 206250/Z/17/Z, NIHR: NIHR200908), HPG (EDCTP2: RIA2020EF-2983-CSIGN, UK DHSC/UK Aid/NIHR: PR-OD-1017-20001), SFunk (Wellcome Trust: 210758/Z/18/Z), GMK (UK MRC: MR/P014658/1), WW (MRC: MR/V027956/1), RME (HDR UK: MR/S003975/1, UK MRC: MC_PC_19065, NIHR: NIHR200908), MK (Wellcome Trust: 221303/Z/20/Z), LACC (NIHR: NIHR200908), YL (B&MGF: INV-003174, NIHR: 16/137/109, European Commission: 101003688, UK MRC: MC_PC_19065), KA (BMGF: INV-016832; OPP1157270), KO’R (B&MGF: OPP1191821), KEA (ERC: SG 757688), FYS (NIHR: 16/137/109), FGS (NIHR: NIHR200929), RP (Singapore Ministry of Health), PM CADDE (MR/S0195/1 & FAPESP 18/14389-0), SC (Wellcome Trust: 208812/Z/17/Z, UK MRC: MC_PC_19065), SA (Wellcome Trust: 210758/Z/18/Z), CIJ (Global Challenges Research Fund: ES/P010873/1), CVM (NIHR: NIHR200929), NIB (HPRU: NIHR200908), SRP (B&MGF: INV-016832), KLM (European Commission: 101003688), JH (Wellcome Trust: 210758/Z/18/Z), YJ (UKRI: MR/V028456/1), MQ (ERC Starting Grant: #757699, B&MGF: INV-001754), OJB (Wellcome Trust: 206471/Z/17/Z), JDM (Wellcome Trust: 210758/Z/18/Z), TWR (Wellcome Trust: 206250/Z/17/Z), KP (B&MGF: INV-003174, European Commission: 101003688), BJQ (NIHR: 16/137/109, NIHR: 16/136/46, B&MGF: OPP1139859), SRM (Wellcome Trust: 210758/Z/18/Z), GFM (B&MGF: NTD Modelling Consortium OPP1184344), EF (MRC: MR/N013638/1), CJVA (ERC: SG 757688), CABP (B&MGF: NTD Modelling Consortium OPP1184344, FCDO/Wellcome Trust: Epidemic Preparedness Coronavirus research programme 221303/Z/20/Z), AE (Nakajima Foundation), JCE (ERC Starting Grant: #757699), QJL (UK MRC: LID DTP MR/N013638/1), RMGJH (ERC Starting Grant: #757699), CD (NIHR: 16/137/109), JYL (B&MGF: INV-003174), KS (Wellcome Trust: 210758/Z/18/Z), DS (BBSRC LIDP: BB/M009513/1), JWR (DTRA: HDTRA1-18-1-0051).
Footnotes
↵† See end material for working group authors
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
1
Blogs/Media
Author Videos