
Abstract
Background In December 2020, two mRNA-based COVID-19 vaccines were authorized for use in the United States. Vaccine safety was monitored using the Vaccine Adverse Event Reporting System (VAERS), a passive surveillance system, and v-safe, an active surveillance system.
Methods VAERS and v-safe data during December 14, 2020—June 14, 2021 were analyzed. VAERS reports were categorized as non-serious, serious, or death; reporting rates were calculated. Rates of reported deaths were compared to expected mortality rates by age. Proportions of v-safe participants reporting local and systemic reactions or health impacts the week following doses 1 and 2 were determined.
Findings During the analytic period, 298,792,852 doses of mRNA vaccines were administered in the United States. VAERS processed 340,522 reports; 92·1% were non-serious; 6·6%, serious, non-death; and 1·3%, death. Over half of 7,914,583 v-safe participants self-reported local and systemic reactogenicity, more frequently after dose 2. Injection-site pain, fatigue, and headache were commonly reported during days 0–7 following vaccination. Reactogenicity was reported most frequently one day after vaccination; most reactions were mild. More reports of being unable to work or do normal activities occurred after dose 2 (32·1%) than dose 1 (11·9%); <1% of participants reported seeking medical care after vaccination. Rates of deaths reported to VAERS were lower than expected background rates by age group.
Interpretation Safety data from >298 million doses of mRNA COVID-19 vaccine administered in the first 6 months of the U.S. vaccination program show the majority of reported adverse events were mild and short in duration.
Introduction
In December 2020, two mRNA coronavirus disease 2019 (COVID-19) vaccines (BNT162b2; Pfizer-BioNTech and mRNA-1273; Moderna) were granted Emergency Use Authorization (EUA) by the U.S. Food and Drug Administration (FDA) as 2-dose series and recommended for use by the Advisory Committee on Immunization Practices (ACIP).1,2 In clinical trials, both mRNA COVID-19 vaccines showed acceptable safety profiles;3,4 the most frequently reported local and systemic symptoms were injection site pain, fatigue, and headache. Reactogenicity was more frequently reported following dose 2, and more common among participants aged <65 years.3-5
Post-authorization safety monitoring better characterizes the safety profiles of mRNA-based COVID-19 vaccines in larger and more heterogeneous populations.6 Phased administration of COVID-19 vaccines in the United States began with healthcare workers and long-term care facility residents and expanded to the general population by Spring 2021; however, implementation plans varied by state.7 The major sources of initial U.S. safety data were the Vaccine Adverse Event Reporting System (VAERS), a spontaneous, passive reporting system,8 and v-safe,9 a new active monitoring system. Reports from these systems have been issued through websites, publications, and presentations to advisory committees.10-14 We review VAERS and v-safe data during the first 6 months of the U.S. vaccination program, when >298 million doses of mRNA COVID-19 vaccines were administered.
Methods
VAERS
VAERS is a national spontaneous reporting system for detecting potential adverse events (AEs) for authorized or licensed U.S. vaccines8 co-administered by the Centers for Disease Control and Prevention (CDC) and FDA. VAERS accepts reports from healthcare providers, manufacturers, and the public. Reports include information about the vaccinated person, type of vaccine administered, and AEs experienced. We included all VAERS reports for mRNA vaccines submitted and processed from December 14, 2020 through June 14, 2021, inclusive of any interval from vaccination to event report.15 Processed reports were those quality checked and coded using the Medical Dictionary for Regulatory Activities (MedDRA) terminology.8 Each VAERS report may be assigned more than one MedDRA Preferred Term (PT); PTs do not necessarily indicate a medically confirmed diagnosis, and include signs and symptoms of illness and results of diagnostic tests.
Based on the Code of Federal Regulations,16 VAERS reports were classified as ‘serious’ if any of the following were documented: hospitalization, prolongation of hospitalization, permanent disability, life-threatening illness, congenital anomaly or birth defect, or death. Adverse events of special interest were selected for enhanced COVID-19 vaccine safety monitoring based on biologic plausibility, previous vaccine safety experience, and theoretical concerns related to COVID-19.17 Death certificates and autopsy reports were requested for death reports. CDC physicians reviewed VAERS reports and available death certificates for each decedent to form an impression about cause of death. Impressions were assigned to one of the following categories: one of the 15 most common International Classification of Disease, Tenth Revision (ICD-10) diagnostic categories reported on U.S. death certificates18; COVID-19-related; other (i.e., impression was not included in a pre-specified categories); or unknown/unclear if a likely cause could not be determined.
V-safe
V-safe is a voluntary smartphone-based system that uses text messaging and secure web-based surveys to actively monitor COVID-19 vaccine safety for common local injection site and systemic reactions.9 V-safe participants receive text messages that link to web-based health check-in surveys following vaccination, initially daily (days 0–7), then at longer intervals post vaccination. The system resets to the initial survey frequency after entry of another dose. We analyzed survey reports from days 0–7 for reactogenicity, severity9 (mild, moderate, severe), and health impact (i.e., unable to perform normal daily activities, unable to work, and/or received care from a medical professional). Participants who reported receiving medical care were contacted and VAERS reports were completed, if clinically indicated.
Data analyses
We conducted descriptive analyses of available VAERS and v-safe data from December 14, 2020 through June 14, 2021 following dose 1 and dose 2 of BNT162b2 and mRNA-1273 vaccines among individuals aged ≥16 years. For VAERS, bivariate analyses included sex, age groups, race/ethnicity, serious AEs, and vaccine type/manufacturer administered and for death reports, time from vaccination to reported death (i.e., onset interval) and cause of death. Reporting rates to VAERS were calculated for AEs using the total number of doses of mRNA vaccine administered during the 6-month period. COVID-19 vaccine administration data were provided through CDC’s COVID-19 Data Tracker.19 Reporting rates for deaths within 7 days following vaccination and 42 days following vaccination were calculated per vaccinated persons using persons who received at least one dose as the estimation of persons vaccinated and compared to expected background mortality rates.20
Empirical Bayesian (EB) data mining was used to detect disproportional reporting of post-vaccine outcomes by vaccine among all VAERS serious and non-serious reports received by June 14, 2021.21 This statistical method calculates observed to expected MedDRA PT pairings by comparing a specific vaccine-MedDRA PT pair to all vaccine-PT pairs in VAERS, adjusting for age, sex, and year received.22 These ratios are ranked by the lower 5% bound of the EB geometric mean confidence interval (EB05) and a standard alert threshold of EB05 >2 was used. An EB05 >2 represents a high degree of confidence that a vaccine-PT pair was reported at least twice as frequently as expected.
V-safe participants who responded to at least one health check-in survey during day 0–7 after vaccination were included in analyses. Descriptive statistics were calculated for participants’ characteristics (sex, age, race/ethnicity), reaction (type and severity) and health impact by manufacturer, dose number, and number of days following vaccination.
SAS software, version 9.4 (SAS Institute; Cary, NC, USA) was used for analyses. Both VAERS and v-safe conduct surveillance as a public health function and are exempt from institutional review board review. Activities were reviewed by the CDC and conducted in accordance with applicable federal law and CDC policy (See: 45 C.F.R. part 46.102(l)(2), 21 C.F.R. part 56; 42 U.S.C. §241(d); 5 U.S.C. §552a; 44 U.S.C. §3501 et seq.).
Results
During December 14, 2020–June 14, 2021, a total of 298,792,852 doses of mRNA COVID-19 vaccines were administered in the United States: 167,177,332 were BNT162b2 and 131,639,515 were mRNA-1273 (Supplemental Table 1). A greater proportion of vaccines were administered to females (53·2%) compared with males (45·8%). The median age at vaccination was 50 years (inter-quartile range [IQR]: 33–65) for BNT162b2 and 56 years (IQR: 39–68) for mRNA-1273, respectively. Non-Hispanic White persons accounted for 38·4% of vaccine recipients; however, race/ethnicity was unknown for 34·9% of all vaccine recipients.
VAERS
During the analytic period, VAERS received and processed a total of 340,522 reports: 164,669 following BNT162b2 and 175,816 following mRNA-1273 vaccination (Table 1). Of these reports, 92·1% were classified as non-serious, 6·6% were serious, not resulting in a death (non-death), and 1·3% were deaths. Seventy-two percent of reports were among females, and 45·3% of reports were among those aged 18–49 years; median age was 50 years (IQR: 36–64). Fifty percent of those reporting race/ethnicity identified as non-Hispanic White; for 22·1%, race/ethnicity was unknown. The most common MedDRA PTs among non-serious reports were headache (20·4%), fatigue (16·6%), pyrexia (16·3%), chills (15·7%), and pain (15·2%). The most common MedDRA PTs among serious reports were dyspnea (15·4%), death (14·1%), pyrexia (11·0%), fatigue (9·7%), and headache (9·5%). The reporting rate to VAERS was 1,049 non-serious reports per million doses, and 90 serious reports per million doses (Table 2). Among the pre-specified AESIs, reporting rates ranged from 0·1 narcolepsy reports per million doses administered to 32 COVID-19 disease reports per million doses administered.
There were 4,496 reports of death to VAERS (Table 3). After review, 24 reports were excluded because of miscoding of death or duplicate reporting. Of the 4,472 reports of deaths analyzed, 2,087 (46·7%) were reported following BNT162b2 and 2,385 (53·3%) following mRNA-1273. Females accounted for 42·6% of reported deaths; the median age was 76 years (IQR: 66–86). More than 80% of deaths were reported among individuals aged 60 years or older (deaths reported per million doses administered by age group: 60–69 years, 14·4; 70–79 years, 28·5; 80–89 years, 75·4; ≥90 years, 2·1). 18·3% of decedents were identified as long-term care facility residents. Time interval to death following vaccination was available for 4,119 reports (92·1%); median time interval was 10·0 days (range: 0—161 days). The greatest number of death reports occurred on day 1 (10·5%) and day 2 (7·0%) following vaccination (Supplemental Figure 1). Compared to expected background rates of death from all causes per million vaccinated persons20, deaths reported to VAERS following mRNA vaccination were consistently 15-30 times less frequent within 7 days of vaccination, and 50 times less frequent within 42 days of vaccination, by age (Table 4).

*x-axis reports through 161 days since last dose.
Death certificates or autopsy reports were available for clinical review for 808 (18·1%) reports of deaths analyzed. Among these, causes of death were most commonly diseases of the heart (46·5%) and COVID-19 disease (12·6%) (Supplemental Table 2, Supplemental Table 3). Among the 3,664 reports of death without a death certificate or autopsy, causes of death were most commonly unknown/unclear (54·1%), diseases of the heart (17·0%), and COVID-19 disease (8·7%). Causes of death by age among reports with death certificate or autopsy reports available are shown by age (Supplemental Table 4).
No adverse health outcome alerts were identified in EB data mining. However, five mRNA COVID-19 administrative error alerts (e.g. ‘product temperature excursion issue’) with disproportionality (EB05>2) were identified during the surveillance period.
v-safe
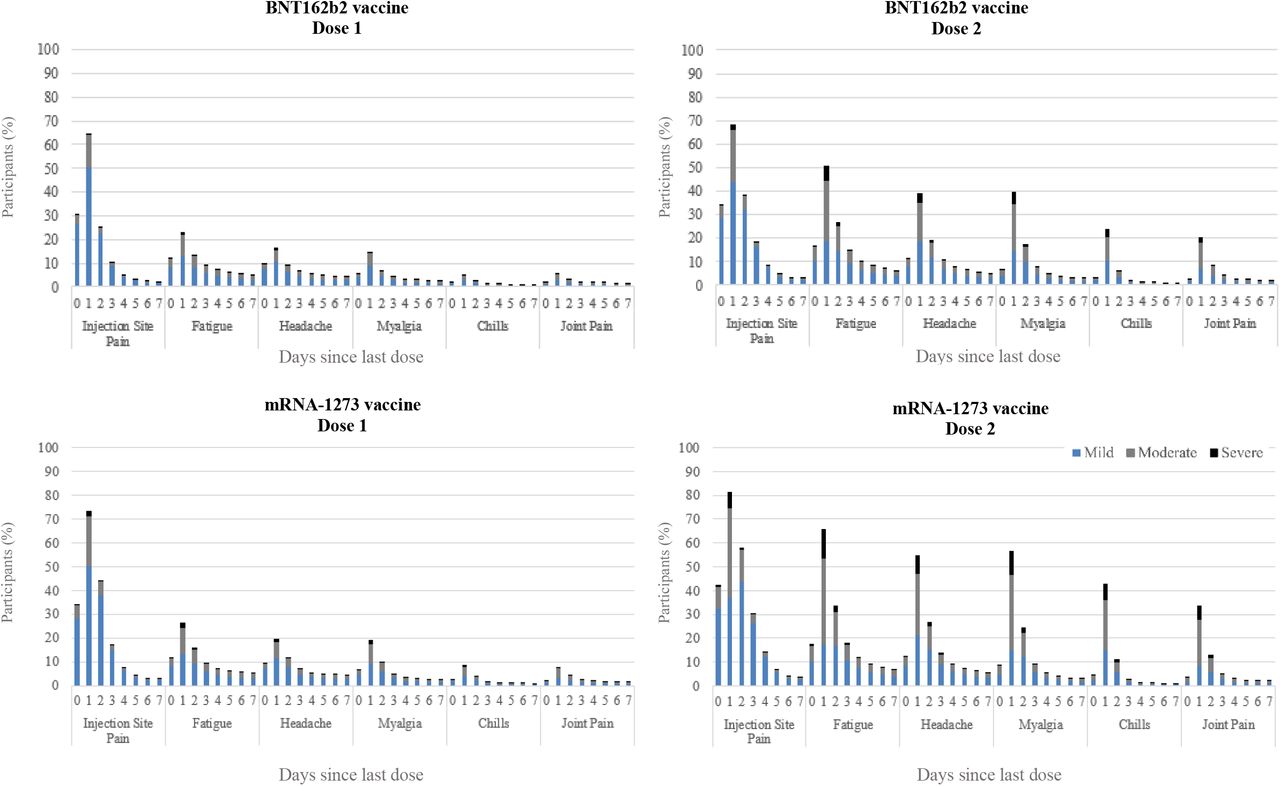
During the analytic period, 7,914,583 mRNA COVID-19 vaccine recipients enrolled in v-safe and completed at least one post-vaccination health survey during days 0–7 (Table 5). The median age of v-safe participants was 50 years (IQR: 36–63), 62·9% were female, and 59·4% identified as non-Hispanic White. A total of 6,775,515 participants completed at least one survey during day 0–7 after dose 1 (3,455,778 following BNT162b2; 3,319,737 following mRNA-1273). Of these participants, 68·6% reported a local injection site reaction and 52·7% reported a systemic reaction. Of the 5,674,420 participants who completed surveys after dose 2, a greater percentage reported an injection site reaction (71·7%) and/or a systemic reaction (70·8%) (Table 6). Local injection site reactions were reported more frequently after mRNA-1273 (dose 1: 73·3%; dose 2: 78·4%) than after BNT162b2 (dose 1: 64·0%; dose 2: 65·3%). A similar pattern was found for systemic reactions after mRNA-1273 (dose 1: 54·3%; dose 2: 75·8%) versus BNT162b2 (dose 1: 51·3%; dose 2: 66·1%). The most frequently reported events after dose 1 of either mRNA vaccine included injection site pain (66·2%), fatigue (33·9%), and headache (27·0%); these were also more frequent after dose 2: injection site pain (68·6%), fatigue (55·7%), headache (46·2%). Differences in proportions of reactogenicity by dose number were similar after stratifying by age (<65 vs. ≥65 years) and sex. More reactogenicity was reported among younger participants aged <65 years and by females. (Supplemental Table 5).
Local and systemic reactions by manufacturer, dose, days after vaccination, and severity are shown in Figure 1. The majority of reported symptoms were mild. Participants reported moderate and severe reactogenicity most commonly on day 1 after dose 2 of either vaccine. The proportion of participants who reported symptoms was greatest on day 1 and then decreased subsequently. The highest proportion of participants reported severe symptoms on day 1 following dose 2 of mRNA-1273 (Supplemental Table 7). On all other days, proportions of participants reporting severe symptoms did not exceed 3.0% for any individual symptom (Supplemental Tables 6 and 7).

*Top five reactions determined by reported frequency after dose 2 of both mRNA COVID-19 vaccines in v-safe, excluding fever because it was not rated mild, moderate, or severe.
†Mild was defined as “noticeable symptoms but they aren’t a problem”, moderate was defined as “symptoms that limit normal activities, and severe symptoms “make normal daily activities difficult or impossible”
Reported health impact was greater following dose 2 of either vaccine (32·1%) compared with dose 1 (11·9%) and after mRNA-1273 of either dose compared with BNT162b2 (Table 6). After dose 2 of BNT162b2, 20·5% were unable to do normal activities, and 12·3% were unable to work. After dose 2 of mRNA-1273, 32·8% were unable to do normal activities, and 20·0% were unable to work. Less than 1·0% reported receiving medical care after receiving either dose of either vaccine. Fewer participants reported an emergency room visit (dose 1: 0·1%; dose 2: 0·2%) or hospitalization (dose 1: 0·03%; dose 2: 0·04%).
When stratified by sex, females reported a health impact more frequently than males, peaking on day 1 after vaccination (Supplemental Figure 2). Following dose 2 of mRNA-1273 vaccine, 41·4% of females reported an inability to perform normal activities in the day 1 survey, and 23·5% an inability to work. Among males receiving dose 2 of mRNA-1273 on the day 1 survey, 25·6% were unable to perform normal activity and 16·9% were unable to work (Supplemental Table 8).

{kind=link}
{kind=link}
{kind=link}
Top left: Female participants reporting health impact after receiving BNT162b2 vaccine. Top right: Female participants reporting health impact after receiving mRNA-1273 vaccine. Bottom left: Male participants reporting health impact after receiving BNT162b2 vaccine. Bottom right: Male participants reporting health impact after receiving mRNA-1273 vaccine.
Discussion
In this analysis of the first six months of VAERS and v-safe data, when over 298 million doses of mRNA vaccines were administered, we report reactogenicity following mRNA COVID-19 vaccination, and reported adverse events, including deaths. Reactogenicity was similar to what was reported from clinical trials and from early post-authorization monitoring.3-5,10,11 In both VAERS and v-safe, local injection site and systemic reactions were commonly reported. V-safe participants more frequently reported transient reactions following mRNA-1273 compared with BNT162b2, and more frequently following dose 2 of either vaccine. Females and individuals aged <65 years reported AEs and reactions more frequently. Analysis of deaths reported to VAERS demonstrated lower than expected reported mortality rates compared with background mortality rates.
Safety monitoring of COVID-19 vaccines has been the most comprehensive in recent U.S. history. COVID-19 vaccine safety has been monitored with established systems, including the Vaccine Safety Datalink (VSD)23 and VAERS, and a new system, v-safe, developed specifically for COVID-19 vaccine safety monitoring. During the study period, all COVID-19 vaccines were administered under EUAs, which require vaccine providers to report serious safety events that follow vaccination to VAERS. Heightened public awareness of the COVID-19 vaccination program, outreach and education to healthcare providers and hospitals about COVID-19 EUA AE reporting requirements, and adherence to EUA reporting requirements by providers and health systems, are likely contributing to the high volume of VAERS reports following mRNA vaccination. Data from U.S. safety monitoring systems have been reviewed regularly by the ACIP COVID-19 Vaccine Safety Technical (VaST) work group24 and at public ACIP meetings.25 Specific safety evaluations have covered serious AEs including anaphylaxis,14 thrombosis with thrombocytopenia syndrome (TTS),26 myocarditis,27 and Guillain-Barré Syndrome (GBS).28 ACIP has assessed the benefit-risk balance of each of the currently licensed or authorized U.S. COVID-19 vaccines; these evaluations have not prompted any changes in U.S. COVID-19 vaccine recommendations.27,28
Reactogenicity findings from VAERS and v-safe were similar to those from a large study of reactogenicity conducted in the United Kingdom.29 The observed patterns may be explained in part by host characteristics known to influence reactogenicity, including age, sex, and the presence of underlying medical conditions.30 Females have more vigorous antibody responses31 to certain vaccines and also tend to report more severe local and systemic reactions to influenza vaccine.32 Females may also be more likely than males to respond to surveys.33,34 Younger persons may be more comfortable with smartphone-based surveys and more likely to respond to surveys, generally.35,36
Using v-safe data, we were able to assess the effects of mRNA vaccination on daily life activities for the first time in adults. Effects on daily activities were most frequently reported on day 1 after vaccination. Reports about the health impact measures used in v-safe, while self-assessed and subjective, correlate with reports about reactogenicity: more health impact was reported by females than males, by participants aged <65 years compared with older participants, after dose 2 compared with dose 1, and by those who received mRNA-1273 versus BNT162b2. Reports of seeking medical care after mRNA vaccine were rare; v-safe did not ask which symptoms prompted the participant to seek medical care. Reactogenicity and its associated health effects, even if transient, may deter some from seeking vaccination. Surveys found that nearly half of unvaccinated adults aged <50 years expressed concern about missing work due to vaccine side effects and that employees provided time off were more likely to get vaccinated;37,38 employer policies that accommodate this might increase vaccination coverage.39
Patterns of VAERS reports following mRNA COVID-19 vaccination were similar to reports following receipt of other vaccines routinely administered to adults; most reported events were non-serious.40-43 EB data mining findings did not suggest any unexpected vaccine safety problems based on pre-specified statistical thresholds. Serious AEs have been detected following receipt of COVID-19 vaccines during U.S. safety monitoring and reviewed in detail in other reports.26-28 Reports of anaphylaxis and myocarditis following mRNA vaccination prompted clinical guidance and management recommendations.27,44-47 TTS26 and GBS28 have been associated with Janssen COVID-19 vaccination (Ad26.COV2.S) but not with mRNA vaccination to date.
In our review and analysis of death reports to VAERS following mRNA vaccination, we found no unusual patterns in cause of death among the large number of death reports received. Reporting rates of death to VAERS among vaccinated persons in 7- and 42-day periods following vaccination were lower than expected background mortality rates. Under the COVID-19 vaccine EUA regulations, healthcare providers are required to report deaths and life-threatening potential adverse events that follow COVID-19 vaccinations to VAERS regardless of their potential association with vaccination. These requirements make comparing the number of reported deaths to VAERS for COVID-19 vaccines to reported deaths following other adult vaccines48 difficult. Older individuals and those in long-term care facilities with the highest baseline mortality risk were initially prioritized for COVID-19 vaccination while most U.S. immunization programs target pediatric and adolescent populations.49 The concentrated reporting of deaths on the first few days following vaccination follows patterns similar to those observed for other adult vaccinations.48 This pattern may represent reporting bias, as the likelihood to report a serious AE may increase when it occurs in close temporal proximity to vaccination.
There are clear limitations in any review of preliminary mortality data. A comparison to national mortality data,20,50 suggests that certain causes of death such as accidents, suicides, or cancer, are less likely to be reported to VAERS. The predominance of heart disease as a cause of death reports to VAERS warrants continued monitoring and assessment, but may be driven by non-specific causes, like cardiac arrest, that might be chosen as a terminal event if no immediate explanation is available. Death certificate or autopsy reports were available only for a small proportion of deaths reported to VAERS. Finally, VAERS is designed as an early warning system to detect potential safety signals8 and VAERS data alone generally cannot establish causal relationships between vaccination and AEs. Other studies and surveillance systems, including the VSD, are needed to better understand patterns of mortality following mRNA COVID-19 vaccination.23,51
This study has several strengths, including the large population under surveillance and comprehensive capture of national data from two complementary surveillance systems. Because the U.S. government purchased all COVID-19 doses and collected administration data, we were able to calculate VAERS reporting rates using the number of mRNA vaccine doses administered.52 In contrast, past VAERS analyses for other vaccines could only use doses distributed, which are always greater than doses administered as denominators, underestimating vaccine adverse event reporting rates. Data concerning how reactogenicity following mRNA vaccination affects daily activities and work during the week following vaccination from v-safe provide information has not been previously described. Limitations of this analysis include a limitation shared by all analyses using VAERS data: it is a passive reporting system subject to underreporting and variable or incomplete reporting.8 While VAERS death reports were individually reviewed by CDC physicians and follow-up is ongoing to obtain additional and missing records, other serious AE reports were not individually reviewed. Additionally, VAERS reports require interpretation to determine if AE reports meet clinical case definitions.53 EB data mining has multiple limitations,21,22 including that the absence of a disproportionality alert for an event does not rule out a possible corresponding adverse event. A new concern with disproportionality scores, which are adjusted by year to control for time-dependent confounders, is that during the study period most VAERS reports were for COVID-19 vaccinations. As all VAERS reports are used for vaccine-event comparisons in EB data mining, potential associations with mRNA COVID-19 vaccines plausibly could be missed. A limitation of v-safe is the need for smartphone access. Because a subset of all vaccine recipients chose or were able to participate in v-safe, the results likely are not generalizable to the entire vaccinated U.S population. In addition, participants in v-safe may be lost to follow up as there is no requirement for continuous enrollment. Finally, this report only included v-safe responses received during the first week post-vaccination.
During the first six months of the U.S. COVID-19 vaccination program, more than 50% of the eligible population received at least one vaccine dose.19 VAERS and v-safe data from this period demonstrate a post-authorization safety profile for mRNA COVID-19 vaccines that is generally consistent with pre-authorization trials3,4 and early post-authorization surveillance reports.10,11 Serious AEs have been identified following mRNA vaccinations; however, based on the most current information, these events are rare. Vaccines are the most effective tool to prevent serious COVID-19 disease outcomes54 and the benefits of immunization in preventing serious morbidity and mortality clearly favor vaccination.26-28 VAERS and v-safe, two complementary surveillance systems, will continue to provide data needed to inform immunization policy makers, medical and immunization providers, and the public about the safety of COVID-19 vaccination.
Acknowledgements
We wish to acknowledge the following contributors: CDC: Amelia Jazwa, Tara Johnson, Charles Licata, Stacey Martin, Florence Lee, Carla Black; FDA: Jane Baumblatt, Deborah Thompson, Kerry Welsh, Narayan Nair, Kosal Nguon (Commonwealth Informatics); v-safe participants; Oracle v-safe development team.
Footnotes
The findings and conclusions in this report are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC) or the Food and Drug Administration (FDA). Mention of a product or company name is for identification purposes only and does not constitute endorsement by the CDC or the FDA.
Funding: No external sources of funding were used. CDC received nonfinancial technical support to develop and maintain the v-safe infrastructure from Oracle.
References




Subject Area
Reviews and Context
4
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
31
Blogs/Media
Author Videos