
ABSTRACT
Background Severe coronavirus disease 2019 (COVID-19) is characterized, in part, by an excessive inflammatory response. Evidence from animal and human studies suggests that vagus nerve stimulation can lead to reduced levels of various pro-inflammatory cytokines. We conducted a prospective randomized controlled study (SAVIOR-I) to assess the feasibility, efficacy, and safety of non-invasive vagus nerve stimulation (nVNS) for the treatment of respiratory symptoms and inflammatory markers among patients who were hospitalized for COVID-19 (ClinicalTrials.gov identifier: NCT04368156).
Methods Participants were randomly assigned in a 1:1 allocation to receive either the standard of care (SoC) alone or nVNS therapy plus the SoC. The nVNS group received 2 consecutive 2-minute doses of nVNS 3 times daily as prophylaxis. Efficacy and safety were evaluated via the incidence of specific clinical events, inflammatory biomarker levels, and the occurrence of adverse events.
Results Of the 110 participants who were enrolled and randomly assigned, 97 (nVNS, n=47; SoC, n=50) had sufficient available data and comprised the evaluable population. C-reactive protein (CRP) levels decreased from baseline to a significantly greater degree in the nVNS group than in the SoC group at day 5 and overall (ie, all postbaseline data points collected through day 5, combined). Procalcitonin level also showed significantly greater decreases from baseline to day 5 in the nVNS group than in the SoC group. D-dimer levels were decreased from baseline for the nVNS group and increased from baseline for the SoC group at day 5 and overall, although the difference between the treatment groups did not reach statistical significance. No significant treatment differences were seen for clinical respiratory outcomes or any of the other biochemical markers evaluated. No serious nVNS-related adverse events occurred during the study.
Conclusions nVNS therapy led to significant reductions in levels of inflammatory markers, specifically CRP and procalcitonin. Because nVNS has multiple mechanisms of action that may be relevant to COVID-19, additional research into its potential to be used earlier in the course of COVID-19 and possibly mitigate some of the symptoms associated with post-acute COVID-19 syndrome is warranted.
INTRODUCTION
The clinical presentation of coronavirus disease 2019 (COVID-19) is highly variable, ranging from asymptomatic to critical multisystem failure (1). Initial symptoms of COVID-19 commonly include fever and cough that may progress to respiratory distress; supportive treatment with antipyretics, antitussives, and supplemental oxygen is often the standard of care (SoC) for these symptoms (1-3). Adults and children with mild to moderate symptoms of COVID-19 who are at risk for progressing to severe COVID-19 and/or hospitalization may receive treatment with neutralizing antibody drugs like bamlanivimab and etesevimab under an emergency use authorization (EUA) (4). Severe cases of respiratory distress may require hospitalization and invasive mechanical ventilation (3). Adults and children who are hospitalized and require supplemental oxygen, invasive mechanical ventilation, or extracorporeal membrane oxygenation may also be given the glucocorticoid dexamethasone in combination with baricitinib and remdesivir (5, 6).
As the treatment of COVID-19 evolved to include the use of glucocorticoids, it became apparent that the pathological sequelae of COVID-19 are due, in part, to an acute, excessive inflammatory response. The inflammatory reflex, a key function of the vagus nerve, modulates the host response to bacterial and viral infections (7, 8). In animal models of sepsis, electrical vagus nerve stimulation (VNS) has been shown to decrease the release of pro-inflammatory cytokines, attenuate multiple organ dysfunction, and improve survival (9-11). In humans, VNS has been demonstrated to reduce or prevent increases in circulating levels of proinflammatory cytokines, including tumor necrosis factor (TNF)-α, interleukin (IL)-1β, IL-6, and interferon-γ in a variety of models, with the specific cytokines affected varying among the disease states studied (12-15). These observations support the hypothesis that inhibition of inflammation with VNS could play a role in the clinical management of patients hospitalized for COVID-19. Owing to the invasive nature of vagus nerve stimulator implantation, historically, the applicability of VNS in critical care medicine was limited.
Non-invasive vagus nerve stimulation (nVNS) in this study was delivered by a handheld, portable vagus nerve stimulator (gammaCore Sapphire™, electroCore, Inc.) that delivers electrical stimulation to the vagus nerve fibers and is US Food and Drug Administration (FDA) approved for the prevention and acute treatment of migraine and cluster headache and Conformité Européenne (CE) marked in the EU for the prevention and treatment of symptoms of reactive airway disease and other conditions. Studies of nVNS in posttraumatic stress disorder and Parkinson disease have suggested that it can reduce systemic levels of inflammatory biomarkers in these conditions (14, 15).
We hypothesized that the administration of nVNS in the hospital setting could inhibit the inflammatory signaling process indicative of COVID-19 progression and potentially improve breathing. Here we report feasibility, efficacy, and safety findings from an initial prospective randomized controlled trial of nVNS for the treatment of respiratory symptoms of COVID-19 and inflammatory markers in hospitalized patients (ClinicalTrials.gov identifier: NCT04368156).
METHODS
Participants
This prospective randomized controlled study was conducted at Hospital Clínico Universitario de Valencia (Valencia, Spain). The clinical research plan was reviewed and approved by an institutional review board and an ethics committee before patient enrollment. Research was conducted in accordance with the Declaration of Helsinki. All patients provided written informed consent before participation.
Investigators enrolled patients ≥18 years of age who were admitted to the hospital, had positive test results for COVID-19, and were experiencing cough and respiratory involvement. Inclusion and exclusion criteria are further described in Table 1. After randomization, demographics and medical histories of participants were compiled and analyzed.
Inclusion and Exclusion Criteria
Randomization
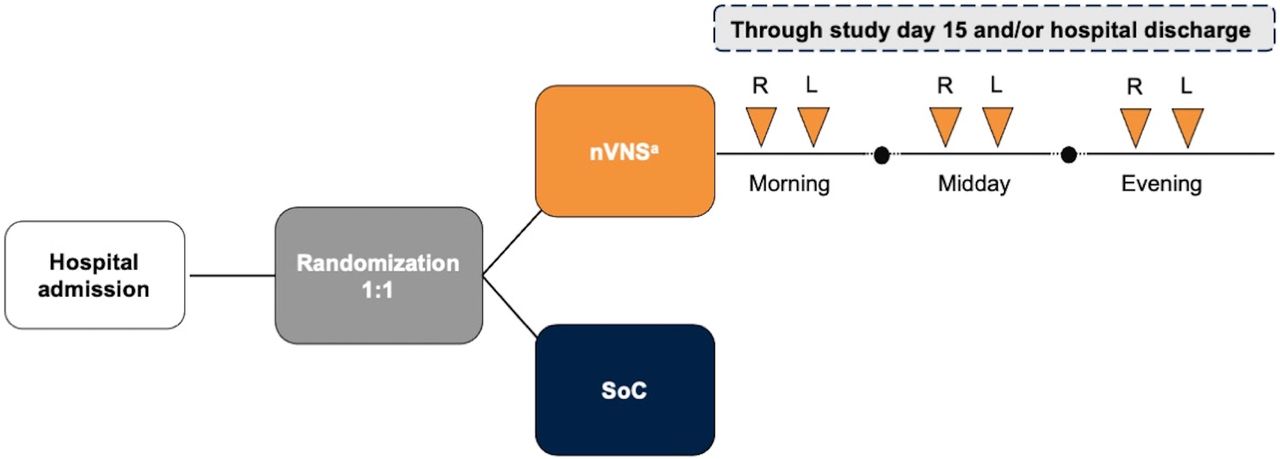
After providing informed consent, participants were randomly assigned in a 1:1 allocation to receive either the routine SoC alone or treatment with nVNS in addition to the SoC (Figure 1).
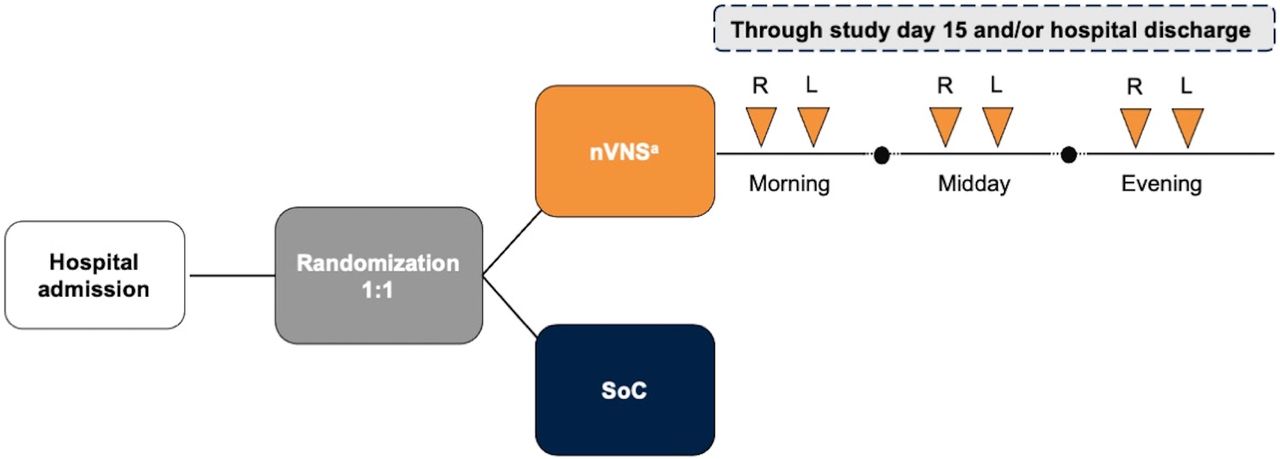
Study Design
aEach stimulation was 2 minutes in duration.
L indicates left side; nVNS, non-invasive vagus nerve stimulation; R, right side; SoC, standard of care.
Procedures
In the active treatment group, nVNS was administered using gammaCore Sapphire™ (electroCore, Inc.; Figure 2), which delivers a low-voltage electrical signal consisting of five 5-kHz pulses repeated at a frequency of 25 Hz. The participant or hospital staff member applied a conductive gel to the stimulation surfaces and applied nVNS to the region of the neck skin where the vagus nerve is located (ie, between the trachea and the sternocleidomastoid muscle, above the palpable carotid pulse). For prophylactic treatment, participants or hospital personnel administered 2 consecutive 2-minute doses of nVNS (1 on each side of the neck) 3 times daily (morning, midday, and evening).

The nVNS Device (gammaCore Sapphire™)
Image provided courtesy of electroCore, Inc.
nVNS indicates non-invasive vagus nerve stimulation.
The SoC group was treated according to routine clinical standards for COVID-19 as defined by hospital protocol. Hospital protocol evolved rapidly as the pandemic progressed. Early on, patients remained on mechanical ventilators with no specific additional treatments. As the pandemic progressed, treatment protocols evolved to incorporate glucocorticoids, antivirals, monoclonal antibodies, and prone mechanical ventilation. This led to a range of SoC treatments being used in this study.
Assessments and Outcomes
Efficacy and safety were evaluated via the incidence of specific clinical events and levels of cytokines and other biomarkers of inflammation, as summarized in Table 2. Because this was the first study of nVNS use in a new disease state, all outcomes were considered exploratory. Participants were assessed for adverse events (AEs), including their seriousness and relationship to nVNS, throughout the study.
Summary of Study Assessments
Statistical Analyses
As this was the first study of nVNS for the treatment of patients hospitalized with COVID-19, there are no previously published data on the anticipated effect size in humans, and a formal power analysis could not be performed.
The study protocol defined the safety population as all participants who signed the consent form and were enrolled in the study and the intention-to-treat population as all participants who were randomly assigned and, if in the nVNS group, used nVNS for at least 1 session. However, not all enrolled patients had data collected; thus, the evaluable population (ie, enrolled participants who signed the informed consent form and had baseline/demographic and medical history data collected) was used for analysis. Within the evaluable population, data for all endpoints at all time points were not obtained from every participant owing to the inherent challenges associated with executing a study in the rapidly changing treatment environment of the pandemic. Thus, the number of participants with observed laboratory data varied by analyte and is denoted for each. Imputation for missing data was not performed. Results of complete case analyses are presented. In addition, given the paucity of observed data after day 5, analyses are limited to data collection from baseline through day 5 of follow-up.
Participant demographics, baseline characteristics, and medical history were summarized for the sample as a whole and by treatment group using descriptive statistics. Treatment groups were compared using chi-square or Fisher exact tests (as appropriate) for categorical variables and t tests for continuous variables. Change from baseline in in fraction of inspired oxygen (FiO2), oxygen saturation, systolic and diastolic blood pressure (BP), and all laboratory assessments were analyzed using a repeated-measures approach with treatment, day, and treatment-by-day interaction as fixed categorical effects and baseline value as a fixed continuous covariate. An unstructured (co)variance structure was used to model within-patient correlation. For FiO2, oxygen saturation, systolic BP, and diastolic BP, day 0 was used as baseline, and day 1 was used as baseline for all laboratory assessments. The least squares mean (LSM) at day 5 and overall (ie, across all postbaseline data points collected through day 5, combined) was calculated for each treatment group. Differences between treatment groups were compared using F tests. The percentages of patients with C-reactive protein (CRP) levels <10 mg/L at days 1, 3, and 5 in each group were compared using chi-square test or Fisher exact tests, as appropriate. Length of hospital and intensive care unit stays were compared between treatment groups using the Wilcoxon rank sum test. Statistical analyses were performed with SAS 9.4 (SAS Institute Inc.). Values of p<0.05 were considered statistically significant. There were no adjustments for multiple comparisons.
RESULTS
Participants
The study began on April 20, 2020, and was completed on February 23, 2021. One hundred ten participants were enrolled and randomly assigned, 55 to each group; among these, 97 (47 in the nVNS group and 50 in the SoC group) had baseline/demographic and medical history data available and comprised the evaluable population (Figure 3). The mean participant age was higher in the SoC group than in the nVNS group, but baseline characteristics were otherwise similar between the groups (Table 3). No other significant differences were detected between treatment groups, although 7 participants in the nVNS group were severely ill, whereas only 2 participants in the SoC group were severely ill.

Participant Disposition
aExcluded participants had missing baseline demographic and/or medical history data.
nVNS indicates non-invasive vagus nerve stimulation; SoC, standard of care.
Participant Demographics, Baseline Characteristics, and Relevant Medical History
Efficacy
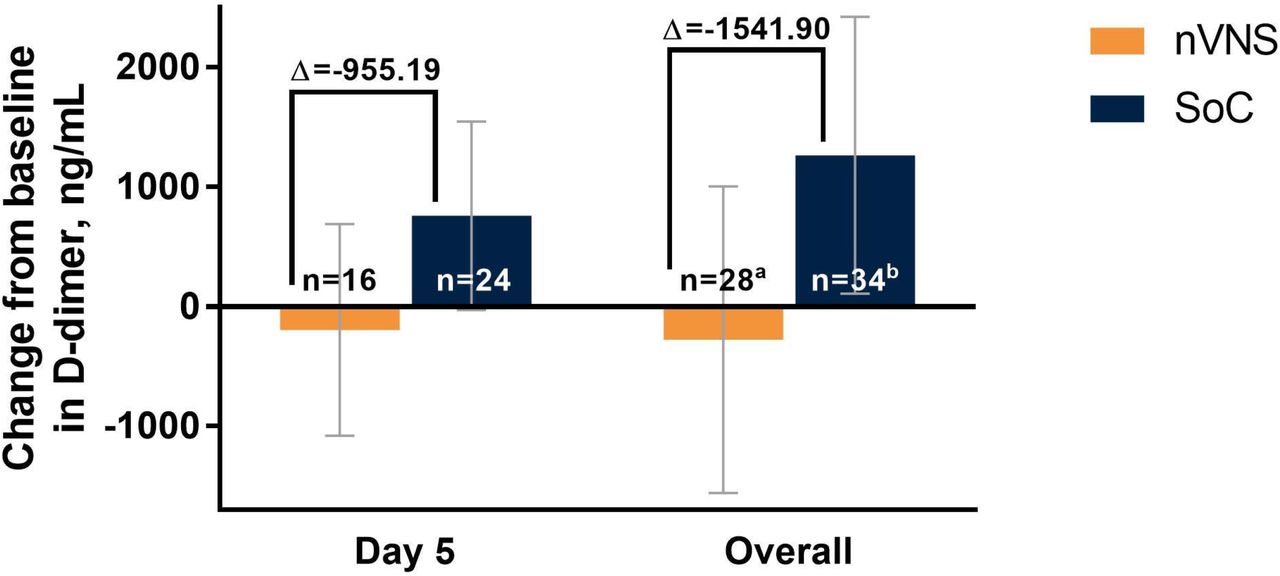
The analyses identified significant treatment differences for certain biomarkers of inflammation. Decreases from baseline in CRP levels were significantly greater for the nVNS group than for the SoC group at day 5 and overall (ie, all postbaseline data points collected through day 5, combined; Figure 4A). At baseline (day 1), CRP levels were normal (<10 mg/L) for very few participants in both treatment groups, but by days 3 and 5 the percentage of participants with normal CRP levels had increased markedly and was significantly greater in the nVNS group than in the SoC group (Figure 4B). Compared with the SoC group, the nVNS group had a significantly greater decrease from baseline in procalcitonin level at day 5 (Figure 5). At day 5 and overall, levels of D-dimer were decreased from baseline for the nVNS group and increased from baseline for the SoC group, although the difference between the treatment groups did not reach statistical significance (Figure 6). No significant treatment differences were seen for the other clinical or biochemical markers that were evaluated (Supplemental Table 1).

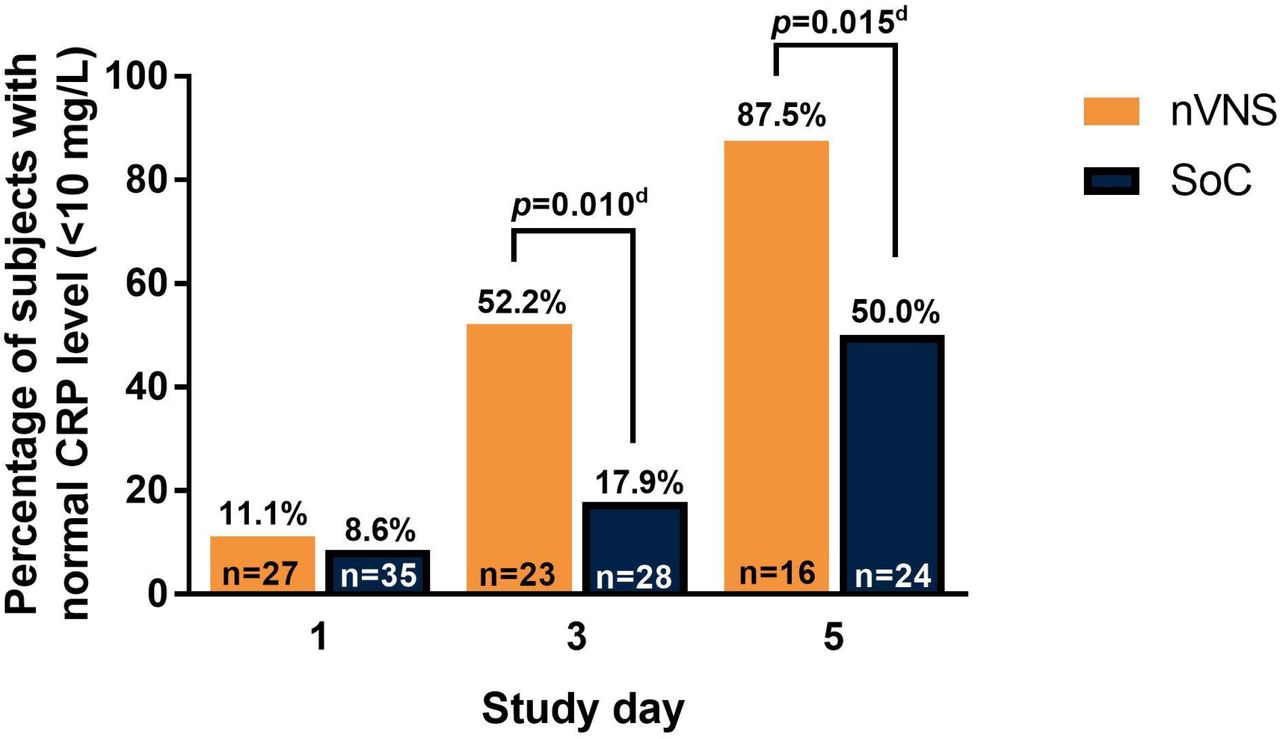
Changes From Baseline in CRP Level (A) and Percentage of Participants With Normal CRP Levels (<10 mg/L) (B) by Treatment Group Among Hospitalized Patients With COVID-19
Error bars denote 95% CIs.
ap values are from F tests comparing LSM changes from baseline for the nVNS and SoC groups. b39 observations from 27 participants. c52 observations from 35 participants.dp values are from chi-squared or Fisher exact test, as appropriate.
COVID-19 indicates coronavirus disease 2019; CRP, C-reactive protein; LSM, least squares mean; nVNS, non-invasive vagus nerve stimulation; SoC, standard of care.

Changes From Baseline in Levels of Procalcitonin by Treatment Group Among Hospitalized Patients With COVID-19
Error bars denote 95% CIs.
ap values are from F tests comparing LSM changes from baseline for the nVNS and SoC groups.b34 observations from 26 participants. c45 observations from 33 participants.
COVID-19 indicates coronavirus disease 2019; LSM, least squares mean; nVNS, non-invasive vagus nerve stimulation; SoC, standard of care.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes From Baseline in Levels of D-dimer by Treatment Group Among Hospitalized Patients With COVID-19
Error bars denote 95% CIs.
a40 observations from 28 participants. b50 observations from 34 participants.
COVID-19 indicates coronavirus disease 2019; LSM, least squares mean; nVNS, non-invasive vagus nerve stimulation; SoC, standard of care.
Safety
Overall changes in BP were assessed using 163 postbaseline observations from 46 participants in the nVNS group and 224 observations from 50 participants in the SoC group. Diastolic BP showed little change from baseline in the nVNS group (LSM, –0.04 mm Hg) and increased slightly in the SoC group (LSM, 2.72 mm Hg), with the difference between groups being statistically significant (–2.76 mm Hg; p=0.031; data not shown). Changes from baseline in systolic BP were small in both the nVNS group (LSM, –1.74 mm Hg) and the SoC group (LSM, 0.78 mm Hg), with no significant difference noted between groups (–2.52 mm Hg; p=0.301).
No serious nVNS-related AEs occurred during the study. In the context of the COVID-19 treatment ward, data on individual nonserious AEs were not recorded.
DISCUSSION
Preclinical studies first initiated nearly 20 years ago demonstrated that VNS is capable of modulating inflammation via the cholinergic anti-inflammatory pathway in experimental bacterially induced sepsis (9, 10, 16-18). However, the invasive nature of the surgical intervention required to apply direct VNS did not support the translation of this treatment to the clinical setting of sepsis or cytokine storm. In 2017, FDA approval of the first transcutaneous cervical vagus nerve stimulator made it possible to investigate whether nVNS could reduce systemic inflammation in critical illness. Coincidentally, the development of nVNS technology was originally predicated on vagus nerve regulation of bronchoconstriction, the evidence for which led to the FDA to issue an EUA for nVNS use in adults with known or suspected COVID-19 (19, 20).
Recently, nVNS was suggested as a potential approach for treating respiratory symptoms and modulating the cytokine storm associated with COVID 19 (19). In patients with COVID-19, elevated inflammatory biomarker levels predict poor prognoses and clinical outcomes, including respiratory failure and mortality (21-23). High CRP levels (>40 mg/mL) are predictive of severe disease and mortality, whereas lower CRP levels are associated with less risk of disease progression (22). Procalcitonin and D-dimer also have been suggested as biomarkers of poor outcomes in COVID-19 (24). Procalcitonin levels have been found to be >4 times greater in patients with severe illness and up to 8 times greater in those with critical illness than in patients with moderate illness (25), and elevated procalcitonin values have been associated with a longer duration of mechanical ventilation (26). The current study was the first to systematically evaluate the effects of VNS on inflammation associated with a replicating virus. Although the study was exploratory in nature, its results suggest significant modulation of CRP by nVNS as early as day 3, with a more robust effect by day 5. There was also evidence for modulation of procalcitonin levels by nVNS, with a significant effect observed on day 5. D-dimer levels also decreased (nonsignificantly) with nVNS.
Another clinical challenge associated with acute COVID-19 is a hypercoagulable state and an accompanying increased risk of stroke, heart attack, and chilblain-like lesions or “COVID toes” (27-29). Elevated levels of CRP, procalcitonin, and D-dimer each individually have been shown to be predictive of thrombotic complications, critical illness, and/or death during hospitalization for COVID-19(30). Together, results from several recent studies suggest that elevations in CRP, procalcitonin, and/or D-dimer levels are associated with more severe disease and greater mortality (21-23, 25, 30-32). In the current study, differences between the nVNS and SoC groups in changes in D-dimer levels approached statistical significance, with an increase noted in the SoC arm and a slight decrease seen in the nVNS arm.
As the COVID-19 pandemic continues and new variants emerge, the need for additional treatment options persists. Our findings suggest that nVNS has mechanistic effects in acute COVID-19 that have potential applicability to address other aspects of the pandemic (eg, early treatment to prevent the progression of symptoms or treatment for symptoms of post-acute COVID-19 syndrome).
Studies of nVNS in asthma and chronic obstructive pulmonary disease have suggested that nVNS can be beneficial for the relief of acute bronchoconstriction and respiratory distress (19, 33, 34). Additionally, published case reports of 2 patients who used nVNS to manage respiratory symptoms of COVID-19 described rapid relief from chest congestion, chest tightness, and dyspnea as well as discontinuation of opioid and cough suppressant medications after nVNS therapy (19). These findings provided the impetus to conduct this prospective randomized study to investigate the effects of nVNS in patients with COVID-19 across a broad range of clinical and biochemical endpoints. Although no clear pulmonary benefits were noted, any potential acute benefit of nVNS on oxygen saturation likely was obscured by the inconsistency in the timing of such measurements. In hindsight, we recognize that measurement of oxygen saturation immediately before and immediately after nVNS application would have been a more prudent approach but would have placed an additional burden on health care resources that were already strained. Rapidly evolving treatment paradigms during the pandemic led to changes in the SoC during the course of the study, and no attempt was made to limit best clinical judgement. Such changes led to inconsistencies in baseline treatment among study participants, which might have hampered the ability to detect pulmonary benefits of nVNS.
Under normal circumstances, all AEs that occur during a clinical trial are documented, and their relationship to the study treatment is carefully assessed. Our intention was to record and evaluate AEs in this manner, but this was not feasible under the circumstances of the COVID-19 pandemic. Although individual AEs were not tabulated, all investigators reported that, in their opinion, there were no serious AEs related to nVNS during the study. This is consistent with findings from controlled clinical trials in which >1000 participants were treated with nVNS and no serious treatment-related AEs were reported, establishing the exceptional safety and tolerability profile of nVNS (35).
As is common in early-stage investigations, we investigated a broad range of exploratory endpoints in this study. Consistent data collection was challenging in the environment of the pandemic, and the duration of hospitalization during the study varied widely (range, 3-42 days). As a result, many participants had missing data for several analytes at some sampling time points. Despite these obstacles, nVNS therapy was associated with significantly greater improvements (vs the SoC alone) in levels of the inflammatory biomarkers CRP and procalcitonin. The effects of nVNS therapy in patients with COVID-19 are being further investigated in another ongoing clinical trial (SAVIOR-II, ClinicalTrials.gov Identifier: NCT04382391).
Conclusions
Novel treatment approaches are needed to address both acute COVID-19 and the emergent issue of post-acute COVID-19 syndrome. With multiple mechanisms of action that may be relevant to COVID-19, nVNS was granted an EUA to address its signs and symptoms. Our results show that nVNS therapy was associated with significant reductions in levels of the inflammatory biomarkers CRP and procalcitonin. Although there was some suggestion that nVNS might affect D-dimer levels, wide confidence intervals rendered the results nonsignificant. This, along with the time required for appreciable degradation of D-dimer in a normal clinical setting after an infection, makes it difficult to draw conclusions on the role of nVNS in modulation of this biomarker. Nevertheless, as severe COVID-19 is characterized by inflammation and a hypercoagulable state, further study of these laboratory findings is warranted, as are investigations into the potential utility of nVNS early in the course of COVID-19 for possible prevention of significant symptoms and/or to address symptoms in patients with post-acute COVID-19 syndrome.
ACKNOWLEDGMENTS
Statistical analyses were performed by Candace McClure, PhD, of North American Science Associates, Inc. The authors acknowledge Chris Czura, PhD, of Convergent Medical Technologies, Inc., for review of the manuscript and Nuria Bargues Martin of INCLIVA Instituto de Investigación Sanitaria for study support, statistical assistance, and review of the manuscript. Medical writing assistance and editorial support were provided by Elizabeth Barton, MS, of MedLogix Communications, LLC, under the direction of authors.
Footnotes
Study funding electroCore, Inc. (Rockaway, NJ, USA) developed the gammaCore Sapphire™ device and provided devices at no cost for use in this study. Statistical analysis for the study conducted by North American Science Associates Inc. (Minneapolis, MN, USA) and editorial support from MedLogix Communications, LLC (Itasca, IL, USA) were funded by electroCore, Inc.
Author disclosures CT has nothing to disclose.
EP has nothing to disclose.
MdMG has nothing to disclose.
JO has nothing to disclose.
MJF has nothing to disclose.
IB has nothing to disclose.
DLC has served as a consultant and advisory board member for Medtronic, Inc.
RV is Director of Research for the National Spine and Pain Centers, a consultant and advisory board member for Medtronic, Inc., and Chief Executive Officer for SGX Medical, LLC.
PS is an employee and was cofounder of electroCore, Inc., and receives stock ownership.
EJL is an employee of electroCore, Inc., and receives stock ownership.
Data availability statement: Data from the SAVIOR I study will be publicly available at ClinicalTrials.gov with the identifier NCT04368156. Individual participant data will not be shared.
REFERENCES




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
3
Community Reviews
0
Automated Services
2
Blogs/Media
Author Videos