
ABSTRACT
Measures to quantify changes in the pace of biological aging in response to intervention are needed to evaluate geroprotective interventions for humans. Here, we report an advance on our original method (Belsky et al. 2020). We used data from the Dunedin Study 1972-3 birth cohort tracking within-individual decline in 19 organ-system integrity indicators across four timepoints spanning two decades to model Pace of Aging. We distilled two-decade Pace of Aging into a single-time-point DNA-methylation blood-test using elastic-net regression and DNA-methylation data restricted to exclude probes with low test-retest reliability. The resulting measure, DunedinPACE, showed high test-retest reliability, was associated with functional decline, morbidity, and mortality, and indicated accelerated Pace of Aging in young adults with childhood adversity across five datasets. DunedinPACE effect-sizes were similar to GrimAge-clock effect-sizes and larger than those for other benchmark DNA-methylation-clocks. DunedinPACE is a novel blood biomarker of the pace of aging for gerontology and geroscience.
INTRODUCTION
Guided by research on the cellular hallmarks of aging, model-organism studies are yielding treatments that slow the accumulation of deterioration in cells and organs (Barzilai et al., 2018; Bellantuono, 2018; Campisi et al., 2019). However, human geroprotector trials face a barrier when it comes to outcome measures: humans’ long lifespan makes it prohibitively time-consuming to test whether a treatment extends healthspan (Justice et al., 2018). What is needed is a way to measure each clinical trial participant’s personal pace of biological aging, before, during, after, and at long-term follow-up, to test whether a gero-protective therapy slows that pace, and whether benefits fade out (Moffitt et al., 2017; Sierra et al., 2021).
An ideal research design for isolating biological patterns that differentiate faster and slower aging is longitudinal follow-up of a cohort of individuals who are all the same chronological age. We originally applied this design to test the geroscience-derived hypothesis that the process of biological aging was ongoing in healthy young adults and, critically, that it was already variable decades before most chronic diseases onset (Belsky et al., 2015; Elliott et al., 2021). We studied a single-year birth cohort of all 1,037 babies born in the city of Dunedin, New Zealand, during 1972-73 and followed-up through midlife. Because aging can be understood as gradual, progressive deterioration simultaneously affecting different organ systems, we tracked declines in the cardiovascular, metabolic, renal, hepatic, immune, periodontal, and pulmonary systems of each participant using multiple biomarker measurements of each organ system, first at ages 26, 32, and 38 years, and subsequently including a fourth assessment at age 45 years. Modelling this one-of-a-kind dataset yielded a metric which quantified how slowly or rapidly each participant had been aging. We called this metric the Pace of Aging.
People with faster Pace of Aging tend to experience more rapid aging-related decline in physical and cognitive functions and develop early signs of brain aging (Belsky et al., 2015; Elliott et al., 2019, 2021; Rasmussen et al., 2019). This evidence suggests that intervention to slow Pace of Aging could preserve functions lost with aging and extend healthspan. However, Pace of Aging takes many years to measure and requires data from several types of clinical and biological assays, limiting its utility in clinical trials. To address this limitation, we applied machine-learning tools to genome-wide DNA methylation data from Dunedin cohort members’ blood samples to distill the multi-timepoint, multi-assay Pace of Aging measure into a single-timepoint, single-assay blood biomarker: DunedinPoAm (for Dunedin Study Pace of Aging from methylation) (Belsky et al., 2020). DunedinPoAm was designed to measure Pace of Aging biological change over time from a single blood sample. Like the original Pace of Aging, people with faster DunedinPoAm scores more often experienced declines in cognitive and physical functioning by midlife and showed more rapid facial aging (Belsky et al., 2020); in older adults, faster DunedinPoAm predicted increased risk of disease and death (Belsky et al., 2020; Graf et al., In Press); in young people, experiences of early-life adversity were linked to faster DunedinPoAm (Belsky et al., 2020; Raffington et al., 2021).
DunedinPoAm provided proof of concept that Pace of Aging could be measured from a single blood test. But DunedinPoAm was based on biological change observed over just twelve years spanning the transition from young adulthood to midlife, limiting the scope of biological change that could be observed. And this biological change was measured from just three assessment waves, limiting the precision. In addition, similar to other DNA methylation composites measured from microarray data, the measure had only moderate test-retest reliability (Higgins-Chen et al., 2021), limiting its value to clinical trials seeking to test within-participant changes from pre-treatment baseline to post-treatment follow-up. To address these limitations, we incorporated new data from the Dunedin cohort extending Pace of Aging follow-up to include a fourth measurement occasion in the fifth decade of life (Elliott et al., 2021) and restricted DNA-methylation data to exclude probes with poor reliability (Sugden et al., 2020) to refine our DNA-methylation biomarker of Pace of Aging. The longer follow-up period, which allowed us to observe more aging-related change in system integrity, and the additional measurement occasion included in analysis improve the power and precision of our modeling of longitudinal change in system integrity (Brandmaier et al., 2018; Rast and Hofer, 2014). The refined DNA-methylation dataset used for machine-learning improves reliability of measurement. We name the novel algorithm DunedinPACE, for Dunedin (P)ace of (A)ging (C)alculated from the (E)pigenome.
RESULTS
We developed the DunedinPACE measure reported here by analyzing the pace of biological aging in a 1972-73 birth cohort (N=1037), the Dunedin Study. This analysis consisted of two parts. The first part of analysis followed our original method (Belsky et al., 2015) to quantify Pace of Aging from two decades of longitudinal organ-system integrity data (Elliott et al., 2021). First, we measured longitudinal changes in 19 biomarkers assessing cardiovascular, metabolic, renal, hepatic, immune, dental, and pulmonary systems, measured at ages 26, 32, 38 and, most recently in 2019, 45 years (Supplementary Table S1 provides measurement details about the variables). Second, linear mixed-effects modelling was used to fit growth models to estimate each study member’s personal rate of change for each of the 19 biomarkers. Third, these personal rates of change were combined across biomarkers to calculate each Study member’s personal Pace of Aging. In line with the geroscience hypothesis (Kaeberlein, 2013; Kennedy et al., 2014), which states that aging represents progressive decline across organ systems, we calculated each Study member’s Pace of Aging as the sum of age-dependent annual changes across all biomarkers:  . The resulting Pace of Aging was then scaled to a mean of 1, so that it could be interpreted with reference to an average rate of 1 year of biological aging per year of chronological aging. Study members showed wide variation in their Pace of Aging (Mean=1 biological year per chronological year, SD=0.29). Over the two decades that we measured biological aging, the Study member with the slowest Pace of Aging aged by just 0.40 biological years per chronological year, while the Study member with the fastest Pace of Aging accrued 2.44 biological years per chronological year (Elliott et al., 2021).
. The resulting Pace of Aging was then scaled to a mean of 1, so that it could be interpreted with reference to an average rate of 1 year of biological aging per year of chronological aging. Study members showed wide variation in their Pace of Aging (Mean=1 biological year per chronological year, SD=0.29). Over the two decades that we measured biological aging, the Study member with the slowest Pace of Aging aged by just 0.40 biological years per chronological year, while the Study member with the fastest Pace of Aging accrued 2.44 biological years per chronological year (Elliott et al., 2021).
The second part of the analysis followed our original method to distill Pace of Aging into a blood test (Belsky et al., 2020). Using Illumina EPIC array DNA methylation data from blood collected at age 45, we developed DunedinPACE to provide a surrogate for the 20-year Pace of Aging. Briefly, we used elastic-net-regression (Zou and Hastie, 2005) to develop a DNA methylation algorithm to predict the 20-year Pace of Aging. Analysis included the subset of probes included on both the Illumina 450k and EPIC arrays which we previously determined to have acceptable test-retest reliability (ICC>0.4, n=81,2392) (Sugden et al., 2020). Following the method established by Horvath (Horvath, 2013) and used in our prior analysis, we fixed the alpha parameter of the elastic net at 0.5. The final lamda value selected by the analysis was 0.042. The resulting algorithm included 173 CpG sites. The CpGs included in DunedinPACE are listed in Supplemental Table S2.
DunedinPACE distills the 20-year Pace of Aging into a single-timepoint DNA methylation blood test
DunedinPACE demonstrated a high in-sample correlation with Pace of Aging to age 45 (r=0.78, Figure 1a). These values indicate improved fit of the DunedinPACE model to the 20-year Pace of Aging as compared to the original DunedinPoAm version’s fit to the 12-year Pace of Aging (in-sample correlation r=0.6). Correlations among the 12- and 20-year Pace of Aging measures and the DunedinPoAm and DunedinPACE DNA methylation measures are shown in Supplemental Figure 1a.

Panel A shows the association of DunedinPACE with the 20-year Pace of Aging in the Dunedin Study cohort (r=0.78). Panel B shows effect-sizes for associations of DunedinPACE with measures of physical and cognitive functioning and subjective signs of aging in Dunedin Study members at age 45 years. Colors indicate groupings of measures (physical functions in shades of orange, cognitive functions in shades of yellow, subjective signs of aging in shades of green). Panel C shows binned scatterplots of associations of DunedinPACE with declines in physical and cognitive function and subjective signs of aging. Plotted points show average values for “bins” of approximately 20 Study members. Regression slopes are estimated from the raw, un-binned data. In Panel C, y-axis scales are denominated in units of standard deviations computed from the baseline measurement for all outcomes except self-rated health, for which the y-axis shows probability of incident fair/poor self-rated health. Changes were calculated over the interval between age-38 and age-45 assessments for all measures except cognition, for which change was calculated over the interval between the age-13 and age-45 assessments.
Consistent with the high correlation of DunedinPACE with 20-year Pace of Aging, effect-sizes for associations of DunedinPACE with measures of physical and cognitive functioning and subjective signs of aging measured at age 45 in the Dunedin Study were similar to effect-sizes for the 20-year Pace of Aging. Effect-sizes for DunedinPACE are graphed in Figure 1b. Comparison with effect-sizes for the 20-year Pace of Aging reported previously (Elliott et al., 2021; Rasmussen et al., 2019) are shown in Supplemental Figure 1b.
We also repeated analysis of decline in physical and cognitive functions included in our original report of DunedinPoAm. This analysis tested associations between DunedinPACE and worsening in physical functions and subjective signs of aging between the age-38 and age-45 assessments and change in cognitive functioning from adolescent baseline to the age-45 assessment. Effect-sizes are graphed in Figure 1c.
Comparison of DunedinPACE effect-sizes for associations with function tests and subjective signs of aging to effect-sizes for the original DunedinPoAm and the DNA methylation clocks proposed by Horvath, Hannum et al., Levine et al. (PhenoAge Clock), and Lu et al. (GrimAge Clock) are shown in Supplemental Figure 1c. DunedinPACE effect-sizes are similar to those for the GrimAge clock and larger than those for other DNA methylation clocks.
DunedinPACE shows exceptional test-retest reliability
A Pace of Aging measure should have high test-retest reliability in order to be able to quantify change from pre-treatment baseline to post-treatment follow-up in intervention studies or exposure-related changes in longitudinal observational studies. We first evaluated test-retest reliability of DunedinPACE using a publicly available database of 36 replicate adult-blood-sample Illumina 450k datasets (Lehne et al., 2015) (GEO Accession GSE55763). We estimated intraclass correlation coefficients (ICCs) for these replicates using mixed-effects regression. For the original DunedinPoAm, reliability was good (ICC=0.89 95% CI [0.79-0.94]). For DunedinPACE, reliability was excellent (ICC=0.96 [0.93-0.98]; Figure 2).We repeated this analysis in two additional databases of replicates reported by Sugden et al. (Sugden et al., 2020), a database of n=28 replicate Illumina EPIC-array datasets and a database of n=350 replicates in which one dataset was generated from the Illumina 450k array and the other dataset was generated from the Illumina EPIC array. DunedinPACE ICCs were 0.97 [0.94-0.98] in the EPIC-EPIC database and 0.87 [0.82-0.90] in the 450k-EPIC database.

The figure graphs DunedinPACE values for replicate Illumnina450k datasets for n=36 individuals in the dataset published by Lehne and colleagues (Lehne et al., 2015) (GEO Accession GSE55763). The ICC for DunedinPACE in the Lehne dataset is 0.96 95% CI [0.92-0.98].
Comparison of DunedinPACE reliability to reliabilities for the original DunedinPoAm and the DNA methylation clocks are shown in Supplemental Figure 2. DunedinPACE is as reliable or more so as compared to the GrimAge clock and more reliable in comparison to the other clocks.
DunedinPACE indicates a faster Pace of Aging in chronologically older individuals
In demography, the pace of biological aging in a population can be estimated from the rate of increase in mortality risk from younger to older chronological ages. In humans and many other species, mortality risk increases exponentially with advancing chronological age, suggesting that the pace of biological aging accelerates as we grow older (Gompertz, 1825; Kirkwood, 2015; Olshansky and Carnes, 1997). We tested if DunedinPACE indicated faster Pace of Aging in chronologically older as compared to younger individuals in data from the Understanding Society Study (n=1175, age range 28-95). Chronologically older Understanding Society participants had faster DunedinPACE Pace of Aging as compared to younger ones (r=0.32, Figure 3 Panel A). This correlation was threefold larger as compared to the correlation for the original DunedinPoAm (r=0.11).

Panel A shows a scatterplot and fitted slopes illustrating the association between chronological age (x-axis) and DunedinPACE (y-axis) in women and men in the Understanding Society sample. Data for women are plotted with yellow dots (orange slope) and for men with blue crosses (navy slope). The figure illustrates a positive association between chronological age and DunedinPACE (Pearson r = 0.32). Panel B shows a matrix of correlations and association plots among DunedinPACE and age-acceleration residuals of Horvath, Hannum, Levine-PhenoAge and Lu-GrimAge epigenetic clocks. The diagonal cells of the matrix list the DNA methylation measures. The half of the matrix below the diagonal shows scatter plots of associations. For each scatter-plot cell, the y-axis corresponds to the variable named along the matrix diagonal to the right of the plot and the x-axis corresponds to the variable named along the matrix diagonal above the plot. The half of the matrix above the diagonal lists Pearson correlations between the DNA methylation measures. For each correlation cell, the value reflects the correlation of the variables named along the matrix diagonal to the left of the cell and below the cell. Panel C graphs scatterplots of associations of DunedinPACE with three physiology-based measures of biological age (KDM Biological Age Advancement, r=0.30 [0.24-0.36]; Phenotypic Age Advancement, r=0.32 95% CI [0.26-0.38]; and Homeostatic Dysregulation r=0.09 [0.03-0.16]) and a plot of DunedinPACE means and 95% confidence intervals by self-rated health category (r=0.20 [0.15-0.26]).
Between-individual correlation of older chronological age with faster DunedinPACE could be confounded by differences in exposure histories across birth cohorts, i.e. not an effect of within-individual aging (Moffitt, 2020). To rule out such confounding, we conducted analysis of within-individual change in DunedinPACE in the US Veterans Administration Normative Aging Study (NAS). Among NAS participants with repeated-measures DNA methylation data (n=536), DunedinPACE increased by b=0.021 (SE=0.003) per 5 years of follow-up, or approximately 0.2 standard deviation units, similar to what we previously reported for the original DunedinPoAm (Belsky et al., 2020).
DunedinPACE shows faster Pace of Aging in individuals measured to be biologically older using prior measures derived from DNA methylation and physiological data, and who report poorer self-rated health
We compared DunedinPACE with the epigenetic clocks proposed by Horvath, Hannum et al., Levine et al., and Lu et al. (Hannum et al., 2013; Horvath, 2013; Levine et al., 2018; Lu et al., 2019), with measurements of biological age derived from physiological data, and with participants’ subjective perceptions of their own health status in data from the UK-based Understanding Society Study (n=1175, mean age=58, SD=15, 42% male).
Epigenetic Clock Analysis
For each epigenetic clock, we calculated the measure referred to as epigenetic “age acceleration” by regressing participants’ clock-estimated ages on their chronological ages and computing residual values. This measure is often used as an estimate of the aging rate. It quantifies the difference between the amount of aging expected based on a person’s chronological age and the amount of aging observed based on DNA methylation DunedinPACE was weakly correlated with age acceleration computed from the Horvath clock (r=0.13) and somewhat more strongly correlated with age acceleration computed from the Hannum and Levine clocks (Hannum r=0.26; PhenoAge r=0.36). These correlations were similar to what we observed for the original DunedinPoAm measure. For the GrimAge clock proposed by Lu et al., the correlation with the age-acceleration residuals was stronger (r=0.58) Correlations are plotted in Figure 3 Panel B.
Physiology-based Measurements of Biological Age
We used published methods to measure participants’ biological ages from blood-chemistry, blood-pressure, and lung function data collected at the same time as the DNA methylation data. We computed indices of biological age using three different methods: the Klemera and Doubal method (KDM) Biological Age estimates the age at which a person’s physiology would appear normal in a reference population (Klemera and Doubal, 2006); the Phenotypic Age method estimates the age at which a person’s physiology-predicted mortality risk would be approximately normal in a reference population (Levine et al., 2018); the homeostatic dysregulation method estimates the extent to which a person’s physiology deviates from a state of health (Cohen et al., 2013). These algorithms generate correlated but distinct estimates of biological aging (Hastings et al., 2019; Parker et al., 2019). Algorithms were parameterized using a set of biomarkers available in Understanding Society and included in Levine’s original implementation of the Klemera-Doubal Biological Age (Levine, 2013) (albumin, alkaline phosphatase, blood urea nitrogen, creatinine, C-reactive protein, HbA1C, systolic blood pressure, forced expiratory volume in one second) and training data from the US National Health and Nutrition Examination Surveys (NHANES). Consistent with analysis of epigenetic age acceleration, participants with more advanced biological aging measured from physiological data also showed faster DunedinPACE Pace of Aging (KDM Biological Age Advancement r=0.30; Phenotypic Age Advancement r=0.32; Homeostatic Dysregulation r=0.09; Figure 3 Panel C).
Self-rated Health
Participants who rated themselves as being in worse health also showed faster DunedinPACE Pace of Aging. The difference in DunedinPACE between those rating their health as excellent and poor was large (Cohen’s d=0.74 [0.46-1.03]; Figure 3 Panel C).
Comparison of effect-sizes for associations with physiology-based measures of biological age and self-rated health between DunedinPACE and the original DunedinPoAm and the four DNA methylation clocks is shown in Supplemental Figure 3. DunedinPACE effect-sizes are similar to or larger than effect-sizes for the GrimAge clock and larger in comparison to the other clocks.
DunedinPACE is associated with morbidity and mortality
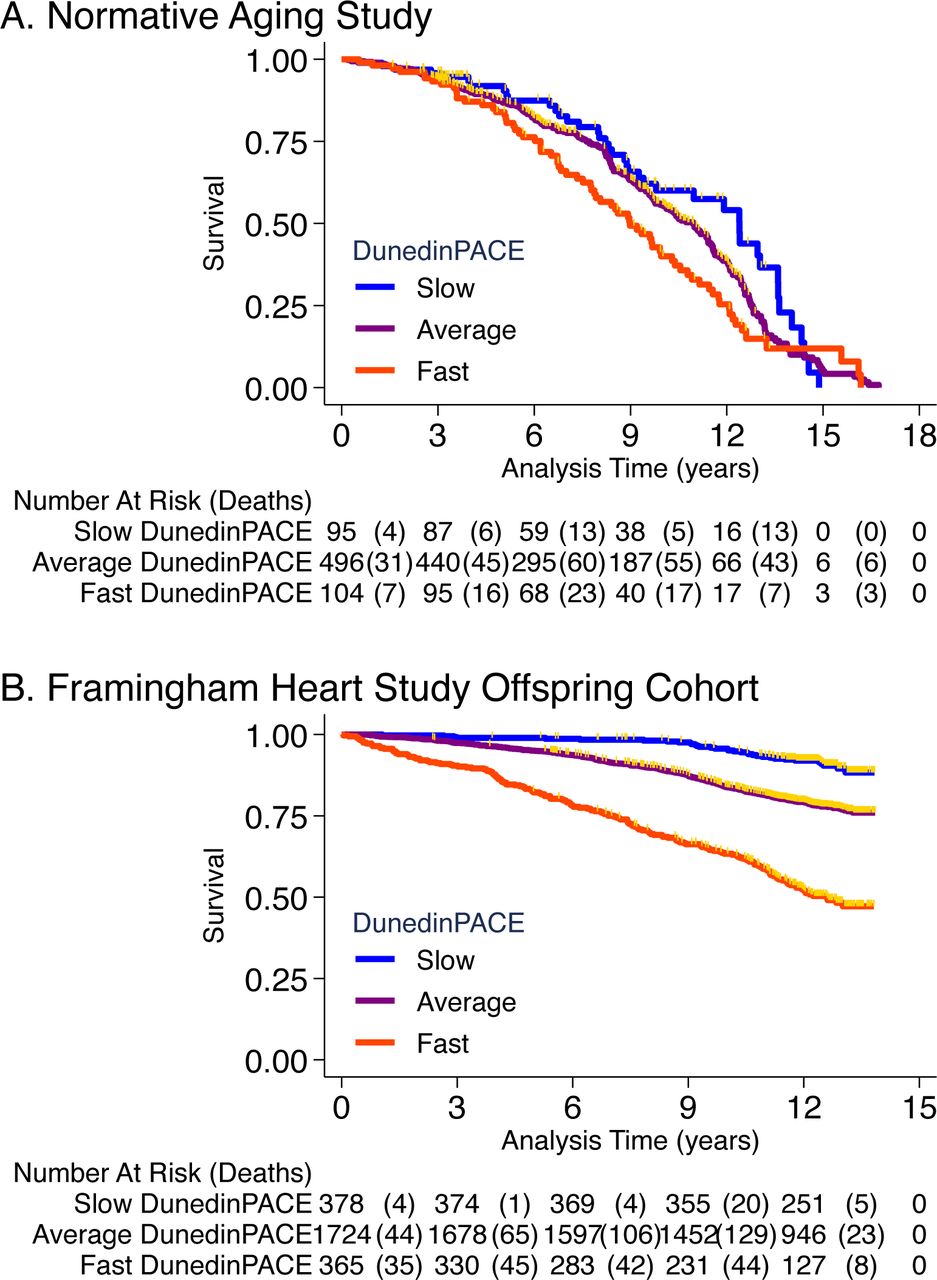
We conducted analysis of morbidity and mortality in older men in the VA Normative Aging Study (NAS) and in the Framingham Heart Study Offspring cohort.
NAS analysis was conducted using the same methods reported in our original article (Belsky et al., 2020). Briefly, analysis included n=771 older men with average age of 77 years (SD=7) at DNA methylation measurement. Over follow-up from DNA collection in 1999-2013, 46% died and 23% were diagnosed with a new chronic disease, including any of hypertension, type-2 diabetes, cardiovascular disease, chronic obstructive pulmonary disease, chronic kidney disease, and cancer. Participants with faster DunedinPACE were at increased risk for morbidity and mortality (for incident chronic disease morbidity, DunedinPACE HR=1.23 [1.07-1.42]; for prevalent chronic disease morbidity, DunedinPACE RR=1.16 [1.12-1.20]; for mortality, DunedinPACE HR=1.26 95% CI [1.14-1.40] Figure 4A).
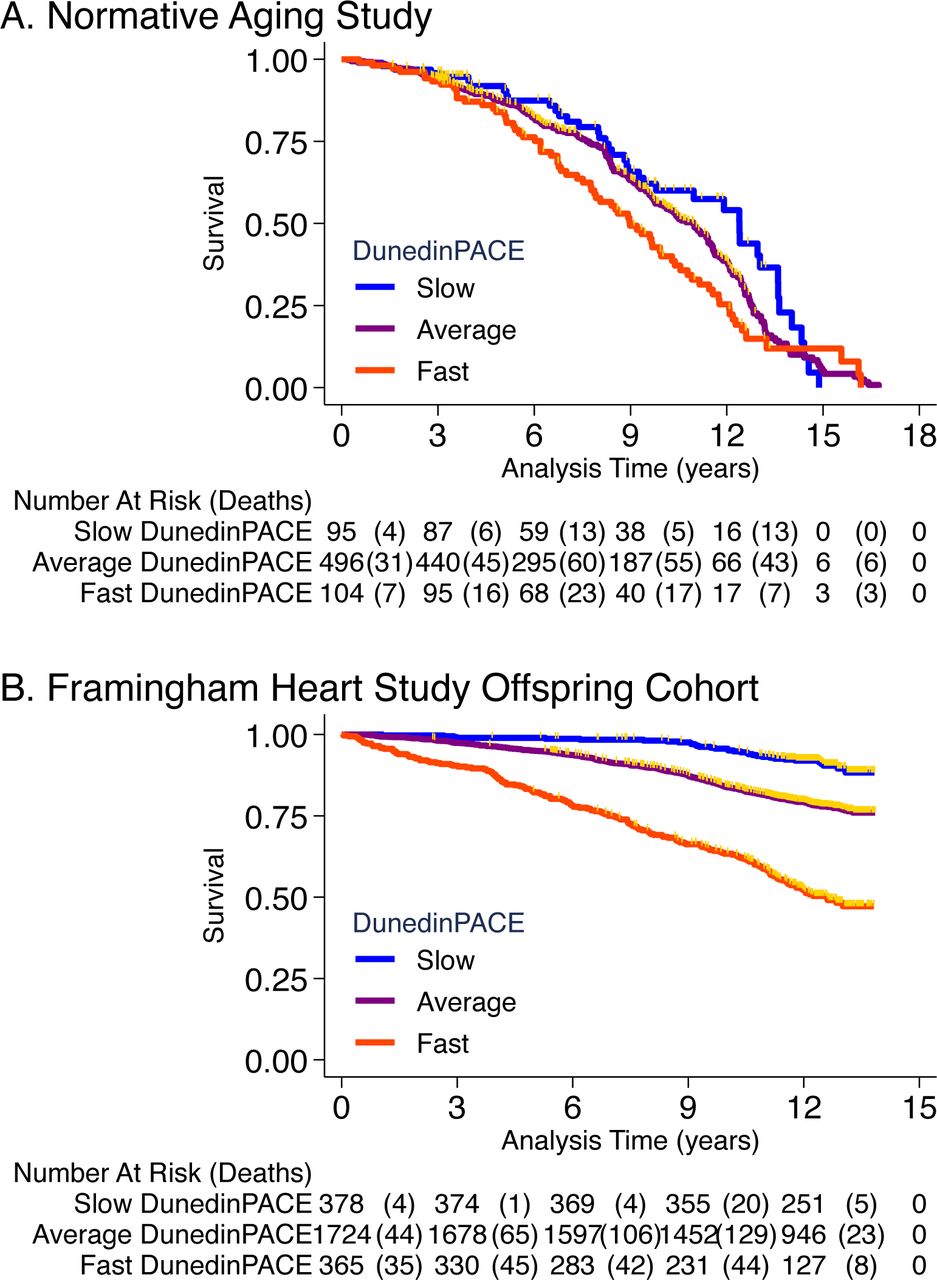
Panel A shows mortality in the Normative Aging Study (NAS). Panel B shows mortality in the Framingham Heart Study Offspring Cohort. The figure plots Kaplan-Meier curves for three groups of participants in each of the two cohorts: those with DunedinPACE 1 SD or more below the mean (‘slow’ DunedinPACE, blue line); those with DunedinPACE within 1 SD of the mean (‘average’ DunedinPACE, gray line); and those with DunedinPACE 1 SD or more above the mean (‘fast’ DunedinPACE, red line). Censoring of participants prior to death is indicated with a gold hash marks. The table below the figure details the number of participants at risk per 3 year interval and, in parentheses, the number who died during the interval.
Framingham analysis included n=2,479 members of the Offspring cohort (54% women) with average age of 66 years (SD=9) at DNA methylation measurement during 2005-2008. Over follow-up through 2015, 23% died. Participants with faster DunedinPACE at baseline were at increased hazard of death over follow-up (HR=1.65 95% CI [1.51-1.79], Figure 4B).
Comparison of effect-sizes for associations with morbidity and mortality between DunedinPACE and the original DunedinPoAm and the DNA methylation clocks are shown in Supplemental Figure 4. DunedinPACE effect-sizes were similar to those for the GrimAge clock and larger than effect-sizes for the other measures.
Childhood exposure to poverty and victimization is associated with faster DunedinPACE Pace of Aging
A Pace of Aging measure should be sensitive to histories of exposure associated with earlier onset of morbidity and shorter lifespan and should provide indications of faster aging before clinical signs of aging-related disease develop, in time for prevention. To test if DunedinPACE indicated faster aging in young people with histories of exposure thought to shorten healthy lifespan, we analyzed data from n=1658 members of the E-Risk Longitudinal Study. The E-Risk Study follows a 1994–95 birth cohort of same-sex twins. Blood DNA methylation data were collected when participants were aged 18 years. We analyzed two exposures associated with shorter healthy lifespan, childhood low socioeconomic status and childhood victimization. Socioeconomic status was measured from data on parents’ education, occupation, and income (Trzesniewski et al., 2006). Victimization was measured from exposure dossiers compiled from interviews with the children’s mothers and home-visit assessments conducted when the children were aged 5, 7, 10, and 12 (Fisher et al., 2015). The dossiers recorded children’s exposure to domestic violence, peer bullying, physical and sexual harm by an adult, and neglect. 72% of the analysis sample had no victimization exposure, 21% had one type of victimization exposure, 4% had two types of exposure, and 2% had three or more types of exposure.
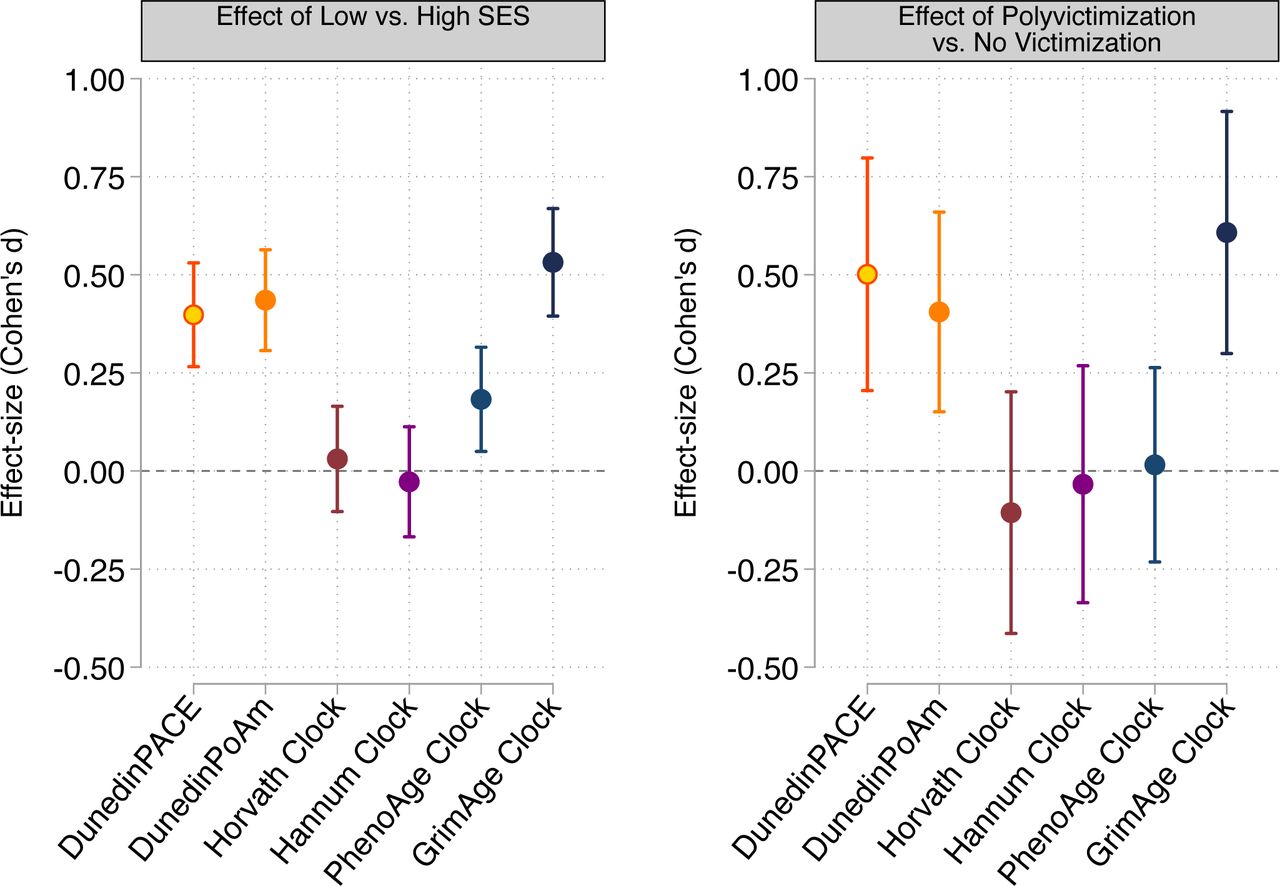
E-Risk participants with exposure to childhood poverty and victimization showed faster DunedinPACE Pace of Aging (For low as compared to high childhood socioeconomic status, d=0.38 95% CI [0.25-0.51]; for polyvictimization as compared to no victimization, d=0.47 [0.17-0.77]; Figure 5). These associations with early-life adversity were robust to covariate adjustment for cell counts estimated from the DNA methylation data, to covariate adjustment for smoking behavior (smoking status and quantity), and to a model specification that excluded smokers (Supplemental Table 4).
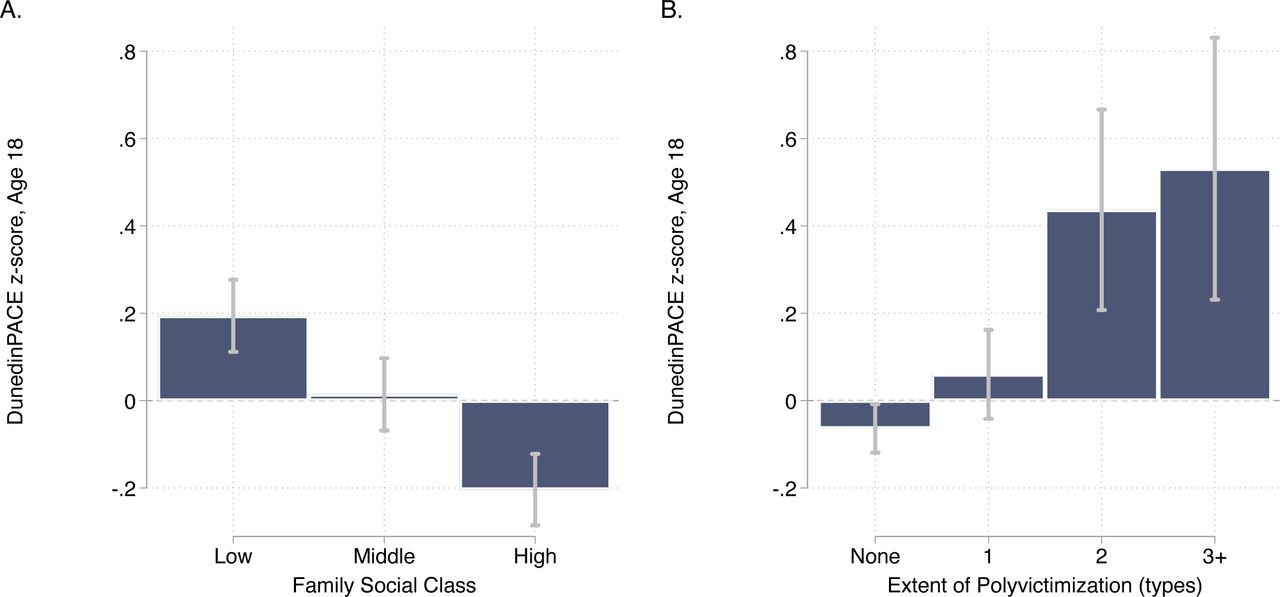
The figure graphs associations of childhood socioeconomic status (SES, Panels A and B) and childhood victimization (Panels C and D) with DunedinPACE measured at age 18 years in the E-Risk cohort. Panels A and C show box plots of the distributions of DunedinPACE values across strata defined by childhood SES and victimization. Panels B and D show plots of effect-sizes for comparisons of risk groups. In Panel B, the reference category is the group who grew up in high-SES households. In Panel D, the reference category is the group for whom no victimization was recorded during childhood. The plotted points and error bars correspond to Cohen’s d effect-sizes and 95% confidence intervals for four models: a base model including covariate adjustment for sex; a model including additional covariate adjustment for estimated cell counts; a model including additional covariate adjustment for smoking status and quantity at age 18, and a model including data only for E-Risk Study members who had never smoked. The figure shows that childhood adversity associations with DunedinPACE are mostly independent of variation in blood sample cell composition and smoking.
Comparison of effect-sizes for associations with childhood poverty and victimization between DunedinPACE and the original DunedinPoAm and the DNA methylation clocks are shown in Supplemental Figure 5. DunedinPACE effect-sizes were similar to those for the GrimAge clock and larger than effect-sizes for the other clocks.
Sensitivity Analysis
Results for analysis of all studies including covariate adjustment for cell counts and smoking are reported in Supplemental Table 4. Covariate adjustment for estimated cell counts and participant reports of smoking history resulted in modest attenuation of some effect-sizes, although DunedinPACE effect-sizes remained statistically different from zero in nearly all cases (associations with declines in balance and cognitive function were attenuated below the alpha=0.05 threshold in Dunedin Study analysis including smoking as a covariate; differences between un-victimized and those with one type of victimization were attenuated below the alpha=0.05 threshold in E-Risk Study analysis including smoking as a covariate; differences between high- and middle-SES groups were attenuated below the alpha=0.05 threshold in E-Risk Study analysis excluding smokers). Compared to the original DunedinPoAm, covariate adjustment for smoking tended to have a smaller impact on effect-size estimates for DunedinPACE. In follow-up analysis of the Understanding Society Study, we found that participant-reported smoking history explained 30% of variance in DunedinPoAm, but only 13% of variance in DunedinPACE. Results were similar in analysis of the Framingham Heart Study Offspring Cohort (R2=23% for DunedinPoAm vs. 12% for DunedinPACE).
DISCUSSION
We developed a novel DNA methylation measure of the pace of biological aging from analysis of two decades of longitudinal data from members of the Dunedin Study 1972-3 birth cohort. As in our original report, we utilized a two-step approach that first modeled the Pace of Aging from within-individual changes in organ-system integrity markers and then distilled this longitudinal change measure into a single-time-point DNA-methylation blood test. The new measure, DunedinPACE, advances DNA methylation measurement of the Pace of Aging for clinical trials of geroprotective therapies beyond our original DunedinPoAm measure in four ways: (1) Pace of Aging analysis included 20 years of follow-up (instead of 12); (2) Pace of Aging analysis included four time points of measurement (instead of three); (3) DNA methylation modeling of Pace of Aging excluded CpG sites for which probes were determined to have low test-retest reliability in blood datasets; (4) the algorithm to implement DunedinPACE includes a normalization step that allows DunedinPACE values for individual samples to be compared to the Dunedin Study cohort in which the measure was developed.
As a result of these advances, DunedinPACE provides a more precise measurement of the Pace of Aging as compared to the original DunedinPoAm and shows higher test-retest reliability. Analysis of this more precise and reliable measurement revealed stronger associations with signs of aging. DunedinPACE showed a stronger correlation with chronological age as compared to the original DunedinPoAm, consistent with demographic evidence that biological processes of aging accelerate in later life (Finch and Crimmins, 2016). In analysis of construct and criterion validity, DunedinPACE was associated with functional decline in midlife adults; it was correlated with measures of biological age derived from blood chemistry and DNA methylation data, and with research participants’ subjective perceptions of their own health; it was predictive of morbidity and mortality in midlife and older adults; and it indicated faster Pace of Aging in young adults with histories of exposure to poverty and victimization. DunedinPACE effect-sizes were similar to or larger than those for the original DunedinPoAm measure even as DunedinPACE was less influenced by participant smoking history. In analysis that took smoking history into account, DunedinPACE effect-sizes were more robust than those for DunedinPoAm, most notably in analysis of mortality in the Framingham Heart Study and of early-life adversity in the E-Risk cohort.
DunedinPACE effect-sizes in analysis of construct and criterion validity were also larger than those for benchmark DNA methylation clocks proposed by Horvath, Hannum et al., and Levine et al. (PhenoAge), and similar to those for the clock proposed by Lu et al. (GrimAge), and were robust to covariate adjustment for smoking and DNA methylation estimates of cell counts. DunedinPACE therefore represents an advance on the original DunedinPoAm measure and provides a novel tool for geroscience research that can complement existing DNA methylation measures of aging in analysis of observational studies and randomized trials.
We acknowledge limitations. Foremost, the Dunedin Study sample we analyzed to develop DunedinPACE is a relatively modestly sized cohort and is drawn from a single country. As additional cohorts develop the multi-time-point organ-system-function datasets to model Pace of Aging, integrating these data into DNA methylation algorithms to measure Pace of Aging may enhance precision. Nevertheless, DunedinPACE does show consistent evidence of criterion and construct validity in several additional datasets, boosting confidence in its external validity. In addition, our work on DunedinPACE thus far has not addressed population diversity in biological aging. The Dunedin cohort and the Understanding Society, NAS, Framingham, and E-Risk cohorts were mostly of white European descent. Follow-up of DunedinPACE in more diverse samples is needed to establish cross-population validity. Importantly, our original DunedinPoAm measure has been followed-up in diverse cohorts and has showed evidence of consistent validity across race/ethnic subgroups (Crimmins et al., 2021; Graf et al., In Press; Raffington et al., 2021; Schmitz et al., 2021). As with all proposed measures of biological aging, ultimately establishing DunedinPACE as a surrogate endpoint for healthspan will require evidence that it is modifiable by intervention and that intervention-induced changes result in changes in healthy-lifespan phenotypes (Justice et al., 2018; Prentice, 1989).
Within the bounds of these limitations, our analysis establishes DunedinPACE as a novel single-time-point measure that quantifies Pace of Aging from a blood test. It can be implemented in Illumina 450k and EPIC array data, making it immediately available for testing in a wide range of existing datasets as a complement to existing methylation measures of aging. Because of its high test-retest reliability, DunedinPACE offers a unique measurement for intervention trials and natural experiment studies investigating how the rate of aging may be changed by behavioral or drug therapy, or by environmental modification.
MATERIALS AND METHODS
Data Sources
Data were used from five studies: Dunedin Study, Understanding Society Study, the Normative Aging Study (NAS), the Framingham Heart Study, and the Environmental Risk (E-Risk) Longitudinal Twin Study. In addition, we accessed the Gene Expression Omnibus dataset GSE55763. The datasets and measures analyzed within each of them are described below.
The Dunedin Study is a longitudinal investigation of health and behavior in a complete birth cohort. Study members (N=1,037; 91% of eligible births; 52% male) were all individuals born between April 1972 and March 1973 in Dunedin, New Zealand (NZ), who were eligible based on residence in the province and who participated in the first assessment at age 3. The cohort represents the full range of socioeconomic status on NZ’s South Island and matches the NZ National Health and Nutrition Survey on key health indicators (e.g., BMI, smoking, physical activity, GP visits) (Poulton et al., 2015). The cohort is primarily white (93%) (Poulton et al., 2015). Assessments were carried out at birth and ages 3, 5, 7, 9, 11, 13, 15, 18, 21, 26, 32, 38 and, most recently, 45 years, when 94% of the 997 study members still alive took part. At each assessment, each study member is brought to the research unit for a full day of interviews and examinations. Study data may be accessed through agreement with the Study investigators (https://moffittcaspi.trinity.duke.edu/research-topics/dunedin). Dunedin Study measures of physical and cognitive functioning and subjective signs of aging are described in detail in Supplemental Table 3.
GSE55763 is a publicly available dataset including technical replicate Illumina 450k DNA methylation array data for 36 adult human samples (Lehne et al., 2015). Data are available from the Gene Expression Omnibus (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE55763).
Understanding Society is an ongoing panel study of the United Kingdom population (https://www.understandingsociety.ac.uk/). During 2010-12, participants were invited to take part in a nurse’s exam involving a blood draw. Of the roughly 20,000 participants who provided clinical data in this exam, methylation data have been generated for just under 1,200. We analyzed data from 1,175 participants with available methylation and blood chemistry data.
Documentation of the methylation (University of Essex) and blood chemistry (University of Essex) data resource is available online (https://www.understandingsociety.ac.uk/sites/default/files/downloads/documentation/health/user-guides/7251-UnderstandingSociety-Biomarker-UserGuide-2014.pdf).
Physiology-based Biological Age Measures
We measured biological aging from blood chemistry, systolic blood pressure, and lung-function data using the algorithms proposed by Klemera and Doubal, Levine, and Cohen (Cohen et al., 2013; Klemera and Doubal, 2006; Levine, 2013; Levine et al., 2018), trained in data from US National Health and Nutrition Examination Surveys (NHANES; https://www.n.cdc.gov/nchs/nhanes/Default.aspx) following the methods described by Hastings (Hastings et al., 2019) and using the software developed by Kwon (https://github.com/dayoonkwon/BioAge). Following the procedure in our original eLife article (Belsky et al., 2020), we included 8 of 10 biomarkers included in Levine’s original implementation of the Klemera-Doubal method Biological Age (Levine, 2013): albumin, alkaline phosphatase (log), blood urea nitrogen, creatinine (log), C-reactive protein (log), HbA1C, systolic blood pressure, and forced expiratory volume in 1 second (FEV1). We omitted total cholesterol because of evidence this biomarker shows different directions of association with aging in younger and older adults (Arbeev et al., 2016). Cytomegalovirus optical density was not available in the Understanding Society database.
Self-rated Health
Understanding Society participants rated their health as excellent, very-good, good, fair, or poor. We standardized this measure to have Mean=0, Standard Deviation=1 for analysis.
The Normative Aging Study (NAS) is an ongoing longitudinal study on aging established by the US Department of Veterans Affairs in 1963. Details of the study have been published previously (Bell et al., 1972). Briefly, the NAS is a closed cohort of 2,280 male veterans from the Greater Boston area enrolled after an initial health screening to determine that they were free of known chronic medical conditions. Participants have been re-evaluated every 3–5 years on a continuous rolling basis using detailed on-site physical examinations and questionnaires. DNA from blood samples was collected from 771 participants beginning in 1999. We analyzed blood DNA methylation data from up to four repeated assessments conducted through 2013 (Gao et al., 2019; Panni et al., 2016). Of the 771 participants with DNA methylation data, n=536 (70%) had data from 2 repeated assessments and n=178 (23%) had data from three or four repeated assessments. We restricted the current analysis to participants with at least one DNA methylation data point. The NAS was approved by the Department of Veterans Affairs Boston Healthcare System and written informed consent was obtained from each subject before participation.
Mortality
Regular mailings to study participants have been used to acquire vital-status information and official death certificates were obtained from the appropriate state health department to be reviewed by a physician. Participant deaths are routinely updated by the research team and the last available update was on 31 December 2013. During follow-up, n=354 (46%) of the 771 NAS participants died.
Chronic Disease Morbidity
We measured chronic disease morbidity from participants medical histories and prior diagnoses (Gao et al., 2021; Lepeule et al., 2018). We counted the number of chronic diseases to compose an ordinal index with categories of 0, 1, 2, 3, or 4+ of the following comorbidities: hypertension, type-2 diabetes, cardiovascular disease, chronic obstructive pulmonary disease, chronic kidney disease, and cancer.
The Framingham Heart Study tracks the development of cardiovascular disease in three generations of families recruited in Framingham Massachusetts beginning in 1948 (Tsao and Vasan, 2015). We analyzed data from the Offspring Cohort, the second generation of study participants, who were recruited beginning in 1971. Blood samples used for DNA methylation analysis were collected from Offspring Cohort members at their 8th follow-up visit during 2005-2008. We analyzed data for n=2,471 cohort members with available DNA methylation and mortality data. This sample was 54% women and had an average age of 66 years (SD=9) at the time blood draws for DNA methylation analysis were conducted. Data for the Framingham Study were obtained from dbGaP (phs000007.v32.p13).
Mortality
Mortality ascertainment in our dataset extended through 2015. Participants contributed a maximum of 14 years of follow-up time. A total of 575 deaths were recorded at an average age of 81 years (SD=9).
The Environmental Risk Longitudinal Twin Study tracks the development of a birth cohort of 2,232 British participants. The sample was drawn from a larger birth register of twins born in England and Wales in 1994-1995. Full details about the sample are reported elsewhere (Moffitt and E-risk Team, 2002). Briefly, the E-Risk sample was constructed in 1999-2000, when 1,116 families (93% of those eligible) with same-sex 5-year-old twins participated in home-visit assessments. This sample comprised 56% monozygotic (MZ) and 44% dizygotic (DZ) twin pairs; sex was evenly distributed within zygosity (49% male). Families were recruited to represent the UK population of families with newborns in the 1990s, on the basis of residential location throughout England and Wales and mother’s age. Teenaged mothers with twins were over-selected to replace high-risk families who were selectively lost to the register through non-response. Older mothers having twins via assisted reproduction were under-selected to avoid an excess of well-educated older mothers. The study sample represents the full range of socioeconomic conditions in the UK, as reflected in the families’ distribution on a neighborhood-level socioeconomic index (ACORN [A Classification of Residential Neighborhoods], developed by CACI Inc. for commercial use): 25.6% of E-Risk families lived in “wealthy achiever” neighborhoods compared to 25.3% nationwide; 5.3% vs. 11.6% lived in “urban prosperity” neighborhoods; 29.6% vs. 26.9% lived in “comfortably off” neighborhoods; 13.4% vs. 13.9% lived in “moderate means” neighborhoods, and 26.1% vs. 20.7% lived in “hard-pressed” neighborhoods. E-Risk underrepresents “urban prosperity” neighborhoods because such households are likely to be childless.
Home-visits assessments took place when participants were aged 5, 7, 10, 12, and 18 years, when 93% of the participants took part. At ages 5, 7, 10, and 12 years, assessments were carried out with participants as well as their mothers (or primary caretakers); the home visit at age 18 included interviews only with participants. Each twin was assessed by a different interviewer. These data are supplemented by searches of official records and by questionnaires that are mailed, as developmentally appropriate, to teachers, and co-informants nominated by participants themselves. The Joint South London and Maudsley and the Institute of Psychiatry Research Ethics Committee approved each phase of the study. Parents gave informed consent and twins gave assent between 5-12 years and then informed consent at age 18. Study data may be accessed through agreement with the Study investigators (https://moffittcaspi.trinity.duke.edu/research-topics/erisk).
Childhood Socioeconomic Status (SES) was defined through a standardized composite of parental income, education, and occupation (Trzesniewski et al., 2006). The three SES indicators were highly correlated (r=0.57–0.67) and loaded significantly onto one factor. The population-wide distribution of the resulting factor was divided in tertiles for analyses.
Childhood Victimization
As previously described (Danese et al., 2016), we assessed exposure to six types of childhood victimization between birth to age 12: exposure to domestic violence between the mother and her partner, frequent bullying by peers, physical and sexual harm by an adult, and neglect.
DNA Methylation Data
DNA methylation was measured from Illumina 450k Arrays in GSE55763, NAS, Framingham, and E-Risk and from Illumina EPIC 850k Arrays in the Dunedin Study and Understanding Society. DNA was derived from whole blood samples in all studies. Dunedin Study blood draws were conducted at the cohort’s age-38 assessment during 2010-12 for the prior DunedinPoAm measure, and at the cohort’s age-45 assessment during 2017-2019 for the new DunedinPACE measure. Understanding Society blood draws were conducted in 2012. NAS blood draws were conducted during 1999-2013. Framingham blood draws were conducted during 2005-2008. E-Risk blood draws were conducted at the cohort’s age-18 assessment during 2012-13. Dunedin methylation assays were run by the Molecular Genomics Shared Resource at Duke Molecular Physiology Institute, Duke University (USA). Understanding Society and E-Risk assays were run by the Complex Disease Epigenetics Group at the University of Exeter Medical School (UK) (www.epigenomicslab.com). NAS methylation assays were run by the Genome Research Core of the University of Illinois at Chicago. Framingham methylation assays were run by the University of Minnesota and John’s Hopkins University (dbGaP phs000724.v9.p13). Processing protocols for the methylation data from all studies have been described previously (Dai et al., 2017; Hannon et al., 2018; Marzi et al., 2018; Panni et al., 2016).
Methylation Clocks
We computed the methylation clocks proposed by Levine et al. and Lu et al. (Levine et al., 2018; Lu et al., 2019) using the methylation data provided by the individual studies and the Horvath Lab’s webtool (http://dnamage.genetics.ucla.edu/new).
The new Dunedin Pace of Aging methylation algorithm (DunedinPACE) was developed using elastic-net regression analysis carried out in the Dunedin Study, as described in detail in the Results. The criterion variable was Pace of Aging. Development of the Pace of Aging is described in detail elsewhere (Belsky et al., 2015; Elliott et al., 2021). Briefly, we conducted mixed-effects growth modeling of longitudinal change in 19 biomarkers measuring integrity of the cardiovascular, metabolic, renal, hepatic, pulmonary, periodontal, and immune systems. Biomarkers were measured at the age 26, 32, 38, and 45 assessments. Biomarkers are listed in Supplemental Table 1. For each biomarker, we estimated random slopes quantifying each participant’s own rate of change in that biomarker. We then composited slopes across the biomarkers to calculate a participant’s Pace of Aging. Pace of Aging was scaled in units representing the mean trend in the cohort, i.e. the average physiological change occurring during one calendar year (N=955, M=1, SD=0.29). Of the N=818 Dunedin Study members with methylation data at age 45, N=817 had measured Pace of Aging (M=0.99, SD=0.30). This group formed the analysis sample to develop DunedinPACE.
To compute DunedinPACE in the GSE55763, Understanding Society, NAS, Framingham, and E-Risk datasets, we applied the scoring algorithm derived from elastic net regression in the Dunedin Study. CpG weights for the scoring algorithm are provided in Supplemental Table 2. To apply the scoring algorithm, a panel of 20,000 probes that represent the underlying distribution of all probes included in the analysis to develop DunedinPACE are drawn from the target dataset. This new dataset is then quantile-normalized to match the reference distribution from the Dunedin Study. The set of 20,000 probes is composed of the 173 probes that make up the DunedinPACE algorithm and 19,827 additional probes selected at random from the full set of probes included in analysis to develop DunedinPACE (i.e. probes passing quality control checks, which are included on Illumina 450k and EPIC arrays, and which were reliable at an ICC threshold of 0.4 in the analysis by Sugden et al. (Sugden et al., 2020)).
Statistical Analysis
We conducted analysis of Dunedin, GSE55763, Understanding Society, NAS, Framingham, and E-Risk, data using regression models. We analyzed continuous outcome data using linear regression. We analyzed count outcome data using Poisson regression. We analyzed time-to-event outcome data using Cox proportional hazard regression. To estimate intraclass correlation coefficients for technical replicates in GSE55763, we used mixed-effects regression models. For analysis of repeated-measures longitudinal DNA methylation data in the NAS, we used generalized estimating equations to account for non-independence of repeated observations of individuals (Ballinger, 2004), following the method in previous analysis of those data (Gao et al., 2018), and econometric fixed-effects regression (Wooldridge, 2012) to test within-person change over time. For analysis in E-Risk, which include data on twin siblings, we clustered standard errors at the family level to account for non-independence of data. For regression analysis, methylation measures were adjusted for batch effects by regressing the measure on batch controls and predicting residual values. Dunedin Study, Understanding Society, Framingham, and E-Risk analyses included covariate adjustment for sex (the NAS included only men). Understanding Society, NAS, and Framingham analyses included covariate adjustment for chronological age. (Dunedin and E-Risk are birth-cohort studies and participants are all the same chronological age.) Sensitivity analyses testing covariate adjustment for leukocyte distributions and smoking are reported in Supplemental Table 4. Leukocyte distributions were measured from complete blood count data in the Dunedin Cohort and were estimated from DNA methylation data for other cohorts.
Code for analysis
Code used for analysis and to prepare figures will be accessible via GitHub upon acceptance of the article for publication.
Code to calculate DunedinPACE from Illumina 450k or Epic Array Data
R code to implement DunedinPACE will be available via GitHub upon publication of the article.
Data Availability
Datasets are available from the data owners. Data from the Dunedin and E-Risk Study can be accessed through agreement with the Study investigators. Instructions are available at https://sites.google.com/site/moffittcaspiprojects/. The data access application form can be downloaded here: https://sites.google.com/site/moffittcaspiprojects/forms-for-new-projects/concept-paper-template. Data from the Understanding Society Study is available through METADAC at https://www.metadac.ac.uk/ukhls/. All details are on the Metadac website (https://www.metadac.ac.uk/data-access-through-metadac/). The data access application form can be found here https://www.metadac.ac.uk/files/2019/02/v2.41-UKHLS-METADAC%26%2365534%3Bapplication-form-2019-2hak8bv.docx. Data from the Normative Aging Study were obtained from the Study investigators. Data are accessible through dbGaP, accession phs000853.v1.p1. Data from the Framingham Heart Study were obtained from dbGaP, accession phs000007.v32.p13. GSE55763 is a publicly available dataset available from the Gene Expression Omnibus (https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE55763).
https://www.ncbi.nlm.nih.gov/geo/query/acc.cgi?acc=GSE55763
https://sites.google.com/site/moffittcaspiprojects/forms-for-new-projects/concept-paper-template
SUPPLEMENTAL FIGURES

Panel A shows correlations among the 12-year and 20-year Pace of Aging measures and the DunedinPoAm and DunedinPACE DNA methylation measures. Panel B graphs effect-sizes for associations of DunedinPoAm and the 20-year Pace of Aging with measures of physical and cognitive functioning and subjective signs of aging measured when Dunedin Study participants were aged 45 years. Panel C graphs effect-sizes for associations of DunedinPACE, DunedinPoAm, and the DNA methylation clocks proposed by Horvath, Hannum et al., Levine et al. (PhenoAge), and Lu et al. (GrimAge) with measures of physical and cognitive functioning and subjective signs of aging measured when Dunedin Study participants were aged 45 years. Panel D graphs effect-sizes for associations of aging measures with measures of change in physical functioning and subjective signs of aging over ages 38-45 years and with cognitive functioning from adolescent baseline to age-45 follow-up. In Panels C and D, the * indicates measures reverse-coded for analysis.

The figure plots intraclass correlation coefficients (ICCs) estimated from replicate DNA methylation datasets for DunedinPACE, original DunedinPoAm, and the DNA methylation clocks proposed by Horvath, Hannum et al., Levine et al. (PhenoAge), and Lu et al. (GrimAge). Error bars show 95% confidence intervals. The three panels of the figure show analysis of three separate datasets reported previously in the articles by Lehne et al. (Lehne et al., 2015) and Sugden et al. (Sugden et al., 2020).

Figure shows effect-sizes estimated from the Understanding Society data (n=1,175). Effect-sizes are reported as standardized regression coefficients interpretable as Pearson r values. Error bars show 95% confidence intervals. DNA methylation clocks were residualized for chronological age prior to analysis. Models included covariates for chronological age and sex. Physiology-based measures of biological age were computed from Understanding Society biomarker data (albumin, alkaline phosphatase, creatinine, C-reactive protein, blood urea nitrogen, glycated hemoglobin, systolic blood pressure, and forced expiratory volume in 1 second) based on algorithms derived in data from the US NHANES according to the methods developed by Levine et al. (Levine et al., 2018), Klemera and Doubal (Klemera and Doubal, 2006), and Cohen et al. (Cohen et al., 2013).

Panel A plots effect-sizes for analysis of incident and prevalent chronic disease morbidity in the Normative Aging Study. Effect-sizes are reported as relative risks (RR) per standard deviation increment of the aging measures estimated from Poisson regression. Panel B plots effect-sizes for analysis of mortality in the Normative Aging Study and the Framingham Heart Study Offspring cohort. Effect-sizes are reported as hazard ratios (HR) per standard deviation increment of the aging measures estimated from Cox proportional hazard regression. For both panels, error bars show 95% confidence intervals. DNA methylation clocks were residualized for chronological age prior to analysis. All models included covariates for chronological age and sex.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Panel A plots effect-sizes for low socioeconomic status (SES) in childhood (vs. high SES in childhood). Panel B plots effect-sizes for childhood polyvictimization (vs. no childhood victimization). Effect-sizes are reported as Cohen’s d. For both panels, error bars show 95% confidence intervals. DNA methylation clocks were residualized for chronological age prior to analysis. All models included sex as a covariate. (All E-Risk participants are the same chronological age; no age covariate is needed.)
We measured Pace of Aging from repeated assessments of a panel of 19 biomarkers: Body mass index (BMI), Waist-hip ratio, Glycated hemoglobin, Leptin, Blood pressure (mean arterial pressure), Cardiorespiratory fitness (VO2Max), Forced vital capacity ratio (FEV1/FVC), Forced expiratory volume in one second (FEV1), Total cholesterol, Triglycerides, High density lipoprotein (HDL), Lipoprotein(a), Apolipoprotein B100/A1 ratio, estimated Glomerular Filtration Rate (eGFR), Blood Urea Nitrogen (BUN), High Sensitivity C-reactive Protein (hs-CRP), White blood cell count, mean periodontal attachment loss (AL), and the number of dental-caries-affected tooth surfaces (tooth decay). This list includes two new biomarkers, leptin and caries, not included in the original Pace of Aging (Belsky et al., 2015), both of which have now been assessed at multiple waves, allowing growth curve modeling. Telomere length was dropped because of an emerging and yet-unresolved field-wide debate about its measurement (Nettle et al., 2021). All other biomarkers were the same. The 20-year Pace of Aging measure is described in detail elsewhere (Elliott et al., 2021).
Supplemental Table 2. CpG sites included in the DunedinPACE DNA methylation algorithm. We will post Supplemental Table 2 once the article is accepted for publication.
Supplemental Table 4. Effect-sizes for analysis of DunedinPACE, DunedinPoAm, and DNA methylation clocks in models with covariate adjustment for age and sex only and for models with additional covariate adjustment for DNA methylation estimated cell counts and for smoking. Effect-sizes are reported for a one standard deviation increment of DunedinPACE. Outcome variables in Dunedin Study, Understanding Society Study, and E-Risk Study (Panels A, B, C, and E) were z-transformed for analysis; effect-sizes are interpretable as Pearson r or Cohen’s d. For Normative Aging Study and Framingham Analysis (Panel C), effect-sizes for time-to event outcomes are reported as hazard ratios (HR) and effect-sizes for prevalent chronic disease are reported as Risk Ratios.
Panel A. Effect-sizes for associations of aging measures with functional assessments at age 45 in the Dunedin Study. Effect-sizes are standardized coefficients from linear regressions of the outcomes on the aging measures. The models adjusted for cell counts (middle column of results) were adjusted for cell counts measured from complete blood count data (white blood cell count and percentages of lymphocytes, monocytes, neutrophils, eosinophils, and basophils). The models adjusted for smoking (left-most column of results) included a covariate for number of pack-years smoked.
Panel B. Effect-sizes for associations of aging measures with functional decline in the Dunedin Study. Decline was measured as change between the age-38 and age-45 assessments for all measures except cognition, for which change was computed over the interval beginning with an adolescent baseline test at age 13 and ending with the most recent cognitive assessment at age 45. Effect-sizes are coefficients from linear regressions of change scores on aging measures for all outcomes except incident fair/poor health, for which effect-sizes are risk ratios (RR) estimated from Poisson regression of incidence on the aging measures. Change scores were computed by standardizing baseline and follow-up measurements using the mean and standard deviation (SD) of the baseline assessment and computing the difference in standardized scores. A single unit of change therefore corresponds to 1 SD of variation at baseline. Effect-sizes are reported for a one SD difference in the aging measures. The models adjusted for smoking (left-most column of results) included a covariate for number of pack-years smoked.
Panel C. Effect-sizes for associations of aging measures with clinical-biomarker measures of biological age, and self-rated health in the Understanding Society Study. Effect-sizes are standardized coefficients from linear regressions of the outcomes on the DNA methylation measures of aging. The models adjusted for smoking included covariates for smoking status and current smoking quantity (cigarettes per day).
Panel D. Effect-sizes for associations of aging measures with mortality and morbidity in the Normative Aging Study and the Framingham Heart Study Offspring Cohort. Effect-sizes are standardized coefficients from linear regressions of the outcomes on the DNA methylation measures of aging. Analysis of mortality was conducted in both cohorts. Analysis of incident and prevalent chronic disease morbidity was conducted only in the Normative Aging Study. The models adjusted for smoking included covariates for smoking history (pack-years smoked) in the Normative Aging Study and for smoking status and current smoking quantity (cigarettes per day) in the Framingham Heart Study. Effect-sizes are hazard ratios (HR) from Cox proportional hazard models for analysis of mortality and incident morbidity and risk ratios (RR) from mixed-effects Poisson regression models for prevalent morbidity.
Panel E. Effect-sizes for associations of childhood socioeconomic status (SES) and childhood victimization with aging measures in the E-Risk Study. Effect-sizes are standardized coefficients (Cohen’s d) from linear regressions of the aging measures on exposure groups (low and middle SES vs. high SES; one, two, and three or more types of victimization vs. no victimization). Models included covariate adjustment for sex. Standard errors were clustered at the family level to account for non-independence of sibling data.
Acknowledgement
This research was supported by US-National Institute on Aging grants AG032282, AG061378, AG066887, and UK Medical Research Council grant MR/P005918/1.
The Dunedin Multidisciplinary Health and Development Research Unit is supported by the New Zealand Health Research Council Programme Grant (16-604), and the New Zealand Ministry of Business, Innovation and Employment (MBIE). We thank the Dunedin Study members, Unit research staff, and Study founder Phil Silva.
Understanding Society data come from The UK Household Longitudinal Study, which is led by the Institute for Social and Economic Research at the University of Essex and funded by the Economic and Social Research Council (ES/M008592/1). Information on how to access the data can be found on the Understanding Society website https://www.understandingsociety.ac.uk/. Data governance was provided by the METADAC data access committee, funded by ESRC, Wellcome, and MRC (2015-2018: MR/N01104X/1; 2018-2020: ES/S008349/1)
The Normative Aging Study is supported by the National Institute of Environmental Health Sciences (grants P30ES009089, R01ES021733, R01ES025225, and R01ES027747). The VA Normative Aging Study is supported by the Cooperative Studies Program/Epidemiology Research and Information Center of the U.S. Department of Veterans Affairs and is a component of the Massachusetts Veterans Epidemiology Research and Information Center, Boston, Massachusetts and is a component of the Massachusetts Veterans Epidemiology Research and Information Center.
The Framingham Heart Study is conducted and supported by the National Heart, Lung, and Blood Institute (NHLBI) in collaboration with Boston University (Contract No. N01-HC-25195, HHSN268201500001I and 75N92019D00031). This manuscript was not prepared in collaboration with investigators of the Framingham Heart Study and does not necessarily reflect the opinions or views of the Framingham Heart Study, Boston University, or NHLBI.
The E-Risk Study is supported by the UK Medical Research Council (grant G1002190), the US National Institute of Child Health and Development (grant HD077482), and the Jacobs Foundation. The generation of DNA methylation data was supported by the American Asthma Foundation.
This work used a high-performance computing facility partially supported by grant 2016-IDG-1013 (HARDAC+: Reproducible HPC for Next-generation Genomics”) from the North Carolina Biotechnology Center.
We would like to acknowledge the assistance of the Duke Molecular Physiology Institute Molecular Genomics Core for the generation of data for the manuscript.
AC, DC, DWB, KS, RP, and TEM are listed as inventors on a Duke University and University of Otago invention that was licensed to a commercial entity.
REFERENCES
REFERENCES
- 74.
- 75.
- 76.
- 77.
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.



