
Summary
Background School-based COVID-19 contacts in England are asked to self-isolate at home. However, this has led to large numbers of missed school days. Therefore, we trialled daily testing of contacts as an alternative, to investigate if it would affect transmission in schools.
Methods We performed an open-label cluster randomised controlled trial in students and staff from secondary schools and further education colleges in England (ISRCTN18100261). Schools were randomised to self-isolation of COVID-19 contacts for 10 days (control) or to voluntary daily lateral flow device (LFD) testing for school contacts with LFD-negative contacts remaining at school (intervention). Household contacts were excluded from participation.
Co-primary outcomes in all students and staff were symptomatic COVID-19, adjusted for community case rates, to estimate within-school transmission (non-inferiority margin: <50% relative increase), and COVID-19-related school absence. Analyses were performed on an intention to treat (ITT) basis using quasi-Poisson regression, also estimating complier average causal effects (CACE). Secondary outcomes included participation rates, PCR results in contacts and performance characteristics of LFDs vs. PCR.
Findings Of 99 control and 102 intervention schools, 76 and 86 actively participated (19-April-2021 to 27-June-2021); additional national data allowed most non-participating schools to be included in the co-primary outcomes. 2432/5763(42.4%) intervention arm contacts participated. There were 657 symptomatic PCR-confirmed infections during 7,782,537 days-at-risk (59.1/100k/week) and 740 during 8,379,749 days-at-risk (61.8/100k/week) in the control and intervention arms respectively (ITT adjusted incidence rate ratio, aIRR=0.96 [95%CI 0.75-1.22;p=0.72]) (CACE-aIRR=0.86 [0.55-1.34]). There were 55,718 COVID-related absences during 3,092,515 person-school-days (1.8%) and 48,609 during 3,305,403 person-school-days(1.5%) in the control and intervention arms (ITT-aIRR=0.80 [95%CI 0.53-1.21;p=0.29]) (CACE-aIRR 0.61 [0.30-1.23]). 14/886(1.6%) control contacts providing an asymptomatic PCR sample tested positive compared to 44/2981(1.5%) intervention contacts (adjusted odds ratio, aOR=0.73 [95%CI 0.33-1.61;p=0.44]). Rates of symptomatic infection in contacts were 44/4665(0.9%) and 79/5955(1.3%), respectively (aOR=1.21 [0.82-1.79;p=0.34]).
Interpretation Daily contact testing of school-based contacts was non-inferior to self-isolation for control of COVID-19 transmission. COVID-19 rates in school-based contacts in both intervention and control groups were <2%. Daily contact testing is a safe alternative to home isolation following school-based exposures.
Introduction
Since the start of the COVID-19 pandemic, there have been four different degrees of disease control in schools, ranging from no controls at one extreme, to school closure at another extreme. Between these poles, different degrees of control have been applied, including isolation of suspected or confirmed cases, to isolation of close contacts of cases.[1]
With widespread availability of point of care testing for SARS-CoV-2, daily contact testing (DCT) has been modelled and piloted as an alternative to compulsory unsupervised isolation of contacts.[2,3,4] Within the pilots contacts could continue to attend school provided a daily SARS-CoV-2 test was negative. Daily testing performed with antigen lateral flow devices (LFDs) has been shown to be feasible,[5] with rapid turnaround times and relatively low cost and good detection of virus.[6, 7] In addition to allowing students and staff to remain at school, DCT might also make regular asymptomatic testing more popular or improve reporting of contacts, as it removes the social penalty of a positive case triggering isolation in contacts.[8] However, concerns about the performance of LFDs used outside of healthcare and other expert settings, have left uncertainty about whether DCT is appropriate for schools or more widely.[9]
A policy of routine self-isolation of contacts assumes this reduces the risk of onward transmission in schools. In practice its impact is unknown; adherence to isolation is incomplete,[10] and the number of isolation-days required to prevent an onward transmission has not been calculated. Evidence is lacking that the benefit of the policy outweighs the clear social[11, 12] and educational[13,14,15] disadvantages. Recent observational data from national English contact-tracing suggests that transmission following a contact event in secondary schools is infrequent, and occurs in <3% of educational contacts in teenagers.[16]
We undertook a cluster randomised controlled trial of DCT in students and staff at English secondary schools and colleges. We aimed to determine if DCT increases school attendance and to assess the impact of DCT on SARS-CoV-2 transmission.
Methods
Study design and participants
We conducted an open-label, cluster-randomised controlled trial to assess the effectiveness of offering daily testing of contacts with cases of COVID-19. The study took place in secondary schools and further education colleges in England. Schools and colleges (hereafter collectively referred to as schools) were eligible to participate if willing to follow the trial procedures and able to operate assisted testing on site. A representative of the institution provided consent electronically. Participating schools were funded for a single study worker located in the school. Participation in study procedures by student and staff contacts was voluntary for individuals and those who agreed provided consent by written or electronic completion of a consent form. Parents or guardians provided consent for participants <16 years old and for those who were otherwise unable to give consent themselves. The study protocol was reviewed and ethical approved granted by Public Health England’s Research Ethics and Governance Group (ref R&D 434). The study was done in accordance with the Declaration of Helsinki and national legislation. The trial is registered as ISRCTN18100261. A nested qualitative process study of acceptability and feasibility for students, parents and staff will be reported separately.
Randomisation
Schools were randomly assigned 1:1 to either a policy of offering contacts daily testing over 7 days to allow continued school attendance (intervention arm) or to follow usual policy of isolation of contacts for 10 days (control arm). Stratification was used to ensure schools representative of those in England were balanced between study arms (Table 1, details in supplement).
The number of students and staff at each school are based on participant lists provided as part of the study and for students from the UK Government Department for Education for schools not actively participating after randomisation. 1n (%); Median (IQR).
Procedures
Schools followed national policy on testing for COVID-19, offering twice weekly asymptomatic testing with LFDs. Individuals with positive LFD results were required to self-isolate immediately and requested to obtain a confirmatory PCR test within 2 days.[17] Those with indicator symptoms of possible COVID-19 (new cough, fever, loss or change in taste or smell) were required to self-isolate along with their household and obtain an urgent PCR test.
If a student or staff member had a positive LFD or PCR, close contacts (“contacts”) were identified by schools using national guidelines (see supplement). Those with close contact with a case in the two days prior to symptom onset (or prior to positive test if asymptomatic) were required to self-isolate for 10 days.[18]
At schools in the intervention arm, close contacts were offered DCT as an alternative to self-isolation, provided the contact with was school-based (i.e. a staff member or student), the contact did not have indicator symptoms of COVID-19 and they were able to attend for on-site testing at the school. Contacts were not eligible for DCT if they had a household member who was isolating due to testing positive for COVID-19. Contacts who did not consent to DCT were required to self-isolate for 10 days.
Participants who agreed to DCT swabbed their own anterior nose; swabs were tested by school staff using a SARS-CoV-2 antigen LFD (Orient Gene).[19] Participants who tested negative were informed and were released from isolation that day to attend education, but were asked to self-isolate after school and on non-testing days (weekends/holidays). Those with 5 negative tests over ≥7 days were released from self-isolation, allowing for no testing at weekends. Where a close contact tested positive, they were instructed to self-isolate along with their household, their contacts were identified, and the process repeated for these contacts.
Data collection
Schools provided a list of all students and staff, including personal identifiers and demographics. For randomised schools that stopped active participation prior to providing these details, a list of students was obtained from the UK Government Department for Education (DfE).
Schools reported the number of staff and students present on each school day, and numbers absent for COVID-19-related reasons and separately numbers absent for other reasons. For schools who stopped participating details, where available, were obtained from DfE records.
Schools recorded each SARS-CoV-2 infection (“index case”) brought to their attention, including PCR-positive cases and LFD-positive cases without a subsequent PCR test. LFD-positive-PCR-negative individuals were not considered cases. The school-based close contacts of each index case, whether or not the contact consented to study procedures, and LFD results were recorded. During the trial, the trial management team were blinded to the combined data.
PCR testing
Results of routine SARS-CoV-2 tests performed outside of the study in staff and students were obtained from national public health data (“NHS Test and Trace”). Dedicated study PCR testing was also undertaken in consenting contacts in both study arms on day 2 and day 7 of the testing/isolation period. In addition, study PCRs were obtained from all LFD/PCR positive individuals for later analysis (see supplement).
Outcomes
The co-primary outcomes were (i) the number COVID-19-related absences from school amongst those otherwise eligible to be in school and (ii) the extent of in-school Covid-19 transmission. The latter was estimated from rates of symptomatic PCR-positive infections recorded by NHS Test and Trace, after controlling for community case rates. Both these end points could be assessed using study data for actively participating schools, but also using national administrative data on student attendance and student and staff lists for non-participating randomised schools. Rates of symptomatic PCR-positive community tests were compared as the incidence of these tests was not expected to be impacted by the study intervention, whereas more intensive sampling of asymptomatic contacts in the intervention arm may have detected more asymptomatic infection.
Secondary outcomes reported include DCT participation rates in the intervention arm, the proportion of asymptomatic research PCR tests and symptomatic routine PCR tests in contacts that were positive, and the performance characteristics of LFD vs. PCR testing in participants in the intervention arm tested on the same day.
Statistical analysis
Rates of COVID-related absence were compared on an intention to treat (ITT) basis using quasi-Poisson regression, adjusting for randomisation strata groups and participant type (student/staff) and accounting for repeated measurements from the same school over time (see supplement for details of this and following analyses).
We compared the incidence of symptomatic PCR-positive SARS-CoV-2 infection between arms on an ITT basis using quasi-Poisson regression, adjusting for randomisation strata groups, participant type and community SARS-CoV-2 case counts at the lower tier local authority level (LTLA) in the prior week.
To account for incomplete participation in DCT, we present complier average causal effects (CACE) estimates for both primary outcomes, which estimate the impact of the intervention amongst those actively participating.
We report uptake of LFD testing for intervention arm participants, on a per day and per participant basis. We used logistic regression to investigate factors associated with per individual participation rates, including the randomisation stratification groups, participant type, age, sex, and ethnicity.
The proportion of close contacts testing positive on an asymptomatic research PCR test or symptomatic community PCR test was compared between study arms using logistic regression. Given there were relatively few events, adjustment was made only for randomisation strata groups and local case counts in the previous week.
We compared the performance of LFD to PCR testing in participants tested by both methods on the same day, regarding PCR testing as the reference standard.
Sample size and power
The challenge with setting a non-inferiority margin for transmission events is that the meaning of a non-inferiority margin is highly dependent on the control group event rate, and it was not possible to determine the transmission event rate in the control group before the start of the trial and it is subject to on-going change in any case. However, it was considered at the time of writing the study protocol that an upper bound of the confidence interval of a relative increase in transmission of up to 50% would be acceptable. Given the uncertainties in the absolute rates of transmission events in each arm, we powered the trial to detect a difference in school attendance (details in supplement).
Role of the funding source
The UK Government Department of Health and Social Care sponsored the trial and was involved in study design and matching of NHS Test and Trace data with study records, data curation and interim monitoring. Otherwise, the study sponsor had no role in data analysis and interpretation or writing of the report.
Results
201 schools were randomised (Table S1) and started participating in the study between 19-April-2021 and 10-May-2021 and continued until 27-June-2021; 76/99(77%) control and 86/102(84%) intervention schools actively participated in the study, returning student/staff lists and attendance data (Figure 1). The remaining 39 stopped active participation, between randomisation and the study starting (of those providing reasons: 20 stated resource constraints, 3 intervention schools cited concerns about the protocol, 2 control schools did not wish to be in the control arm, 1 intervention school on local authority public health advice).
Participating schools and randomisation strata.

The former depends on availability of daily school attendance data for students and staff aggregated at school level. The latter depends on provision of student and staff lists to enable matching of identifiers with NHS Test and Trace national community testing data. DfE, UK Government Department for Education. School participation was defined based on submission of student/staff lists and attendance data for at least part of the study.
Baseline characteristics
Schools were randomised using 9 school-type strata (Table 1). Schools in the control and intervention arms had a median(IQR) 1014(529-1376) and 1025(682-1359) students and 142(91-189) and 125(91-173) staff respectively. Ages, sex and ethnic groups in students and staff were similar between the study arms, most students were aged 11-18 years (Table 2).
Note students aged ≥19 years attended further education colleges providing courses for students at any age. Data based on 96 control schools and 101 intervention arm schools with data on student demographics and 76 and 86 schools respectively with data on staff. 1n (%).
Index case events and contacts
The 76 and 86 actively participating control and intervention schools reported 338 and 450 index cases (students or staff) respectively. These index cases resulted in 5097 and 6721 recorded contacts in 4400 and 5797 individuals at 48 and 59 control and intervention arm schools.
A total of 247 and 343 control and intervention arm index cases had ≥1 recorded school-based contact, where the 10 days following the contact event included ≥1 study school day. The remaining index cases had no reported close contacts, e.g. having tested positive during a weekend/holiday. These 4463 and 5763 contacts in 47 and 59 control and intervention schools involved a total of 22,466 and 27,973 school days where without the intervention students and staff would have been asked to isolate at home. In the intervention arm, this represented a theoretical maximum of 27,973/4,105,826(0.68%) school days where DCT could potentially prevent COVID-related absences. On 13,846/27,973(49.5%) days an LFD result was recorded (or the contact had already completed follow-up, i.e., recorded ≥5 tests or a positive test). In 1241 contact episodes, the contact declined to participate in DCT (5598 person-school-days;19.9%) and on 2600(9.2%) person-school-days a participating contact was unavailable testing (i.e. did not attend school or declined testing). Testing on 4457(15.8%) person-school-days did not occur after the whole cohort of contacts or school was sent home to isolate, following either school or public health agency intervention (Figure 2A). These participation pauses occurred at 14 schools, 5 due to school capacity issues, 6 due to school or public health agency concern about Delta variant, and 3 due to public health concern about cases in the school as a result of transmission in the community. No pause was instituted because of perceived excess transmission attributed to the intervention.

Panel A shows the number of contacts in the intervention arm by study day, by participation or reason for non-participation. Note the school “half-term” holiday (31-May-2021 to 04-June-2021). Panel B shows the percentage of contacts in the intervention arm participating, by study day; the bars are coloured according to the number of contacts under follow up on a given day. Panel C shows the percentage of contacts participating in LFDs in 59 intervention arm schools reporting ≥1 contact affecting school days. For each contact event return of ≥3 LFD results or a positive LFD result is used to summarise participation in the intervention. The bars are coloured by strata group, which summarises the 9 strata used for randomisation. LFDs, lateral flow tests. Schools with no contacts participating are shown with a small negative value on the y-axis to aid visualisation.
Per day DCT participation was highest at the start of the study and lowest in the week prior to the “half-term” holiday (31-May-2021 to 04-June-2021) when participation fell, predominately due to school-wide participation pauses (Figure 2A,2B).
Using reporting of ≥3 LFD results or a positive LFD result to summarise participation per contact rather than per day, 2432/5763(42.4%) contacts participated, with differing rates by school (Figure 2C). The median(IQR) participation across the 59 schools was 63%(40-79%). Staff were more likely to participate than students (adjusted OR, aOR=2.67;95%CI 1.35-5.27;p=0.005). Participants identifying as Chinese ethnicity were more likely and those identifying as “Other” ethnicity were less likely to participate compared with those identifying as white. Amongst schools with ≤17% of students receiving free school meals, participation rates were higher in schools with students aged 11-16 years compared to 11-18 years (Table 3).
Participant age is omitted from the multivariable model due to collinearity with participant type. Results from logistic regression, adjusting confidence intervals to account for repeated measurements from the same school. 1n (%); Median (IQR); 2OR = Odds Ratio, CI = Confidence Interval. Note week 7 is the school “half-term” holiday, when school-based lateral flow testing was not undertaken. Note participation in the final week of the study appears lower than in Figure 2, as participation is summarised as completion of ≥3 LFDs, and contacts in the final week may not have completed testing before the end of the study.
COVID-related absences
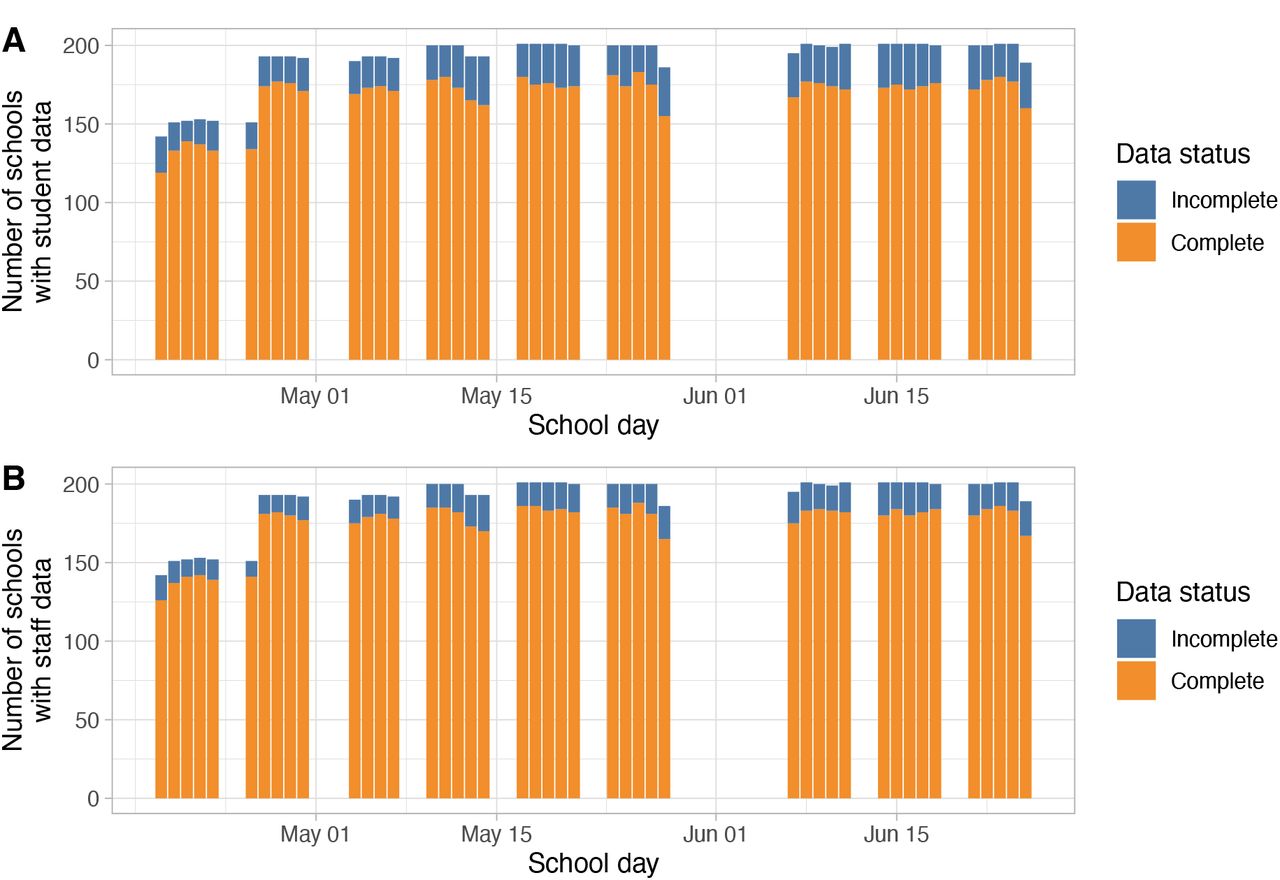
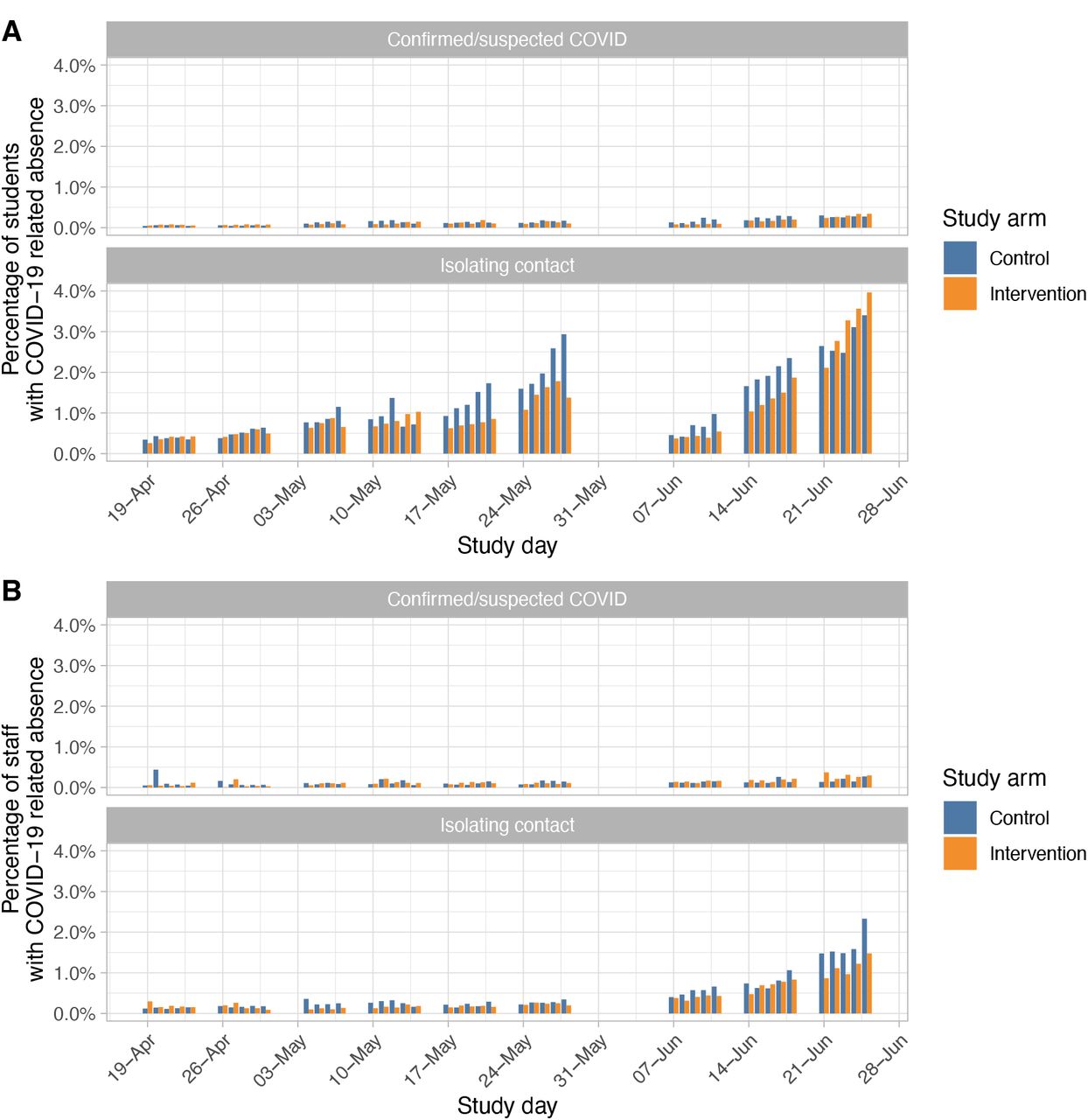
Rates of student and staff COVID-related absence, due to known or suspected COVID or as a contact, were compared. Student attendance data were available for part or all of the study from 91(92%) of control and 99(97%) intervention schools; with data for 3551/4146(86%) and 3836/4261(90%) of possible school-school day combinations (Figure S1). Similarly, staff attendance was available from 94(95%) control and 100(98%) intervention arm schools, for 3767/4146(91%) and 3925/4261(92%) days. 95,545 and 102,134 students and 14,687 and 14,811 staff were reported in control and intervention arm attendance data. (Total numbers of students and staff in aggregate attendance data differ to totals from student/staff identifier lists used to identify symptomatic cases [Table 2], reflecting different underlying data sources and different schools with available data).
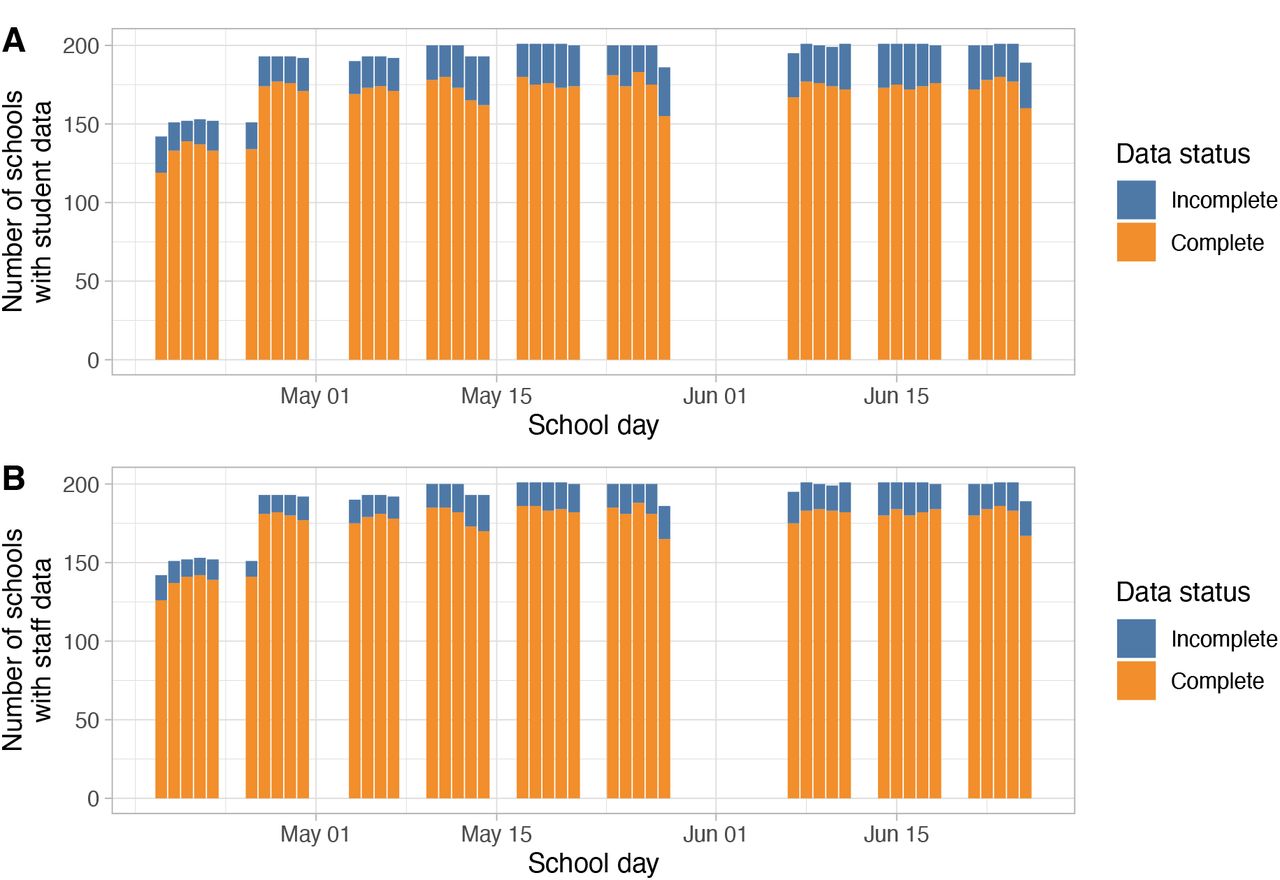
Individuals were considered at risk of a COVID-related absence on school days following enrolment of the school into the study from 19-April-2021 onwards up to 25-June-2021. National holidays, the school “half-term” holiday (31-May-2021 to 04-June-2021), and individual school non-school days were excluded. The total height of the bar represents the number of randomised schools entered into the study on that day excluding any schools with a non-school day. Although 4 schools continued throughout the half-term holiday, this period was removed from the analysis for all schools.
Students had 55,718 COVID-related absences during 3,092,515 person-days-at-risk in the control arm (1.80%), and 48,609 during 3,305,403 person-days-at-risk in the intervention arm (1.47%, Figure 3). Rates of staff COVID-related absences were 3704/566,502(0.65%) in the control arm and 2932/539,805(0.54%) in the intervention arm.
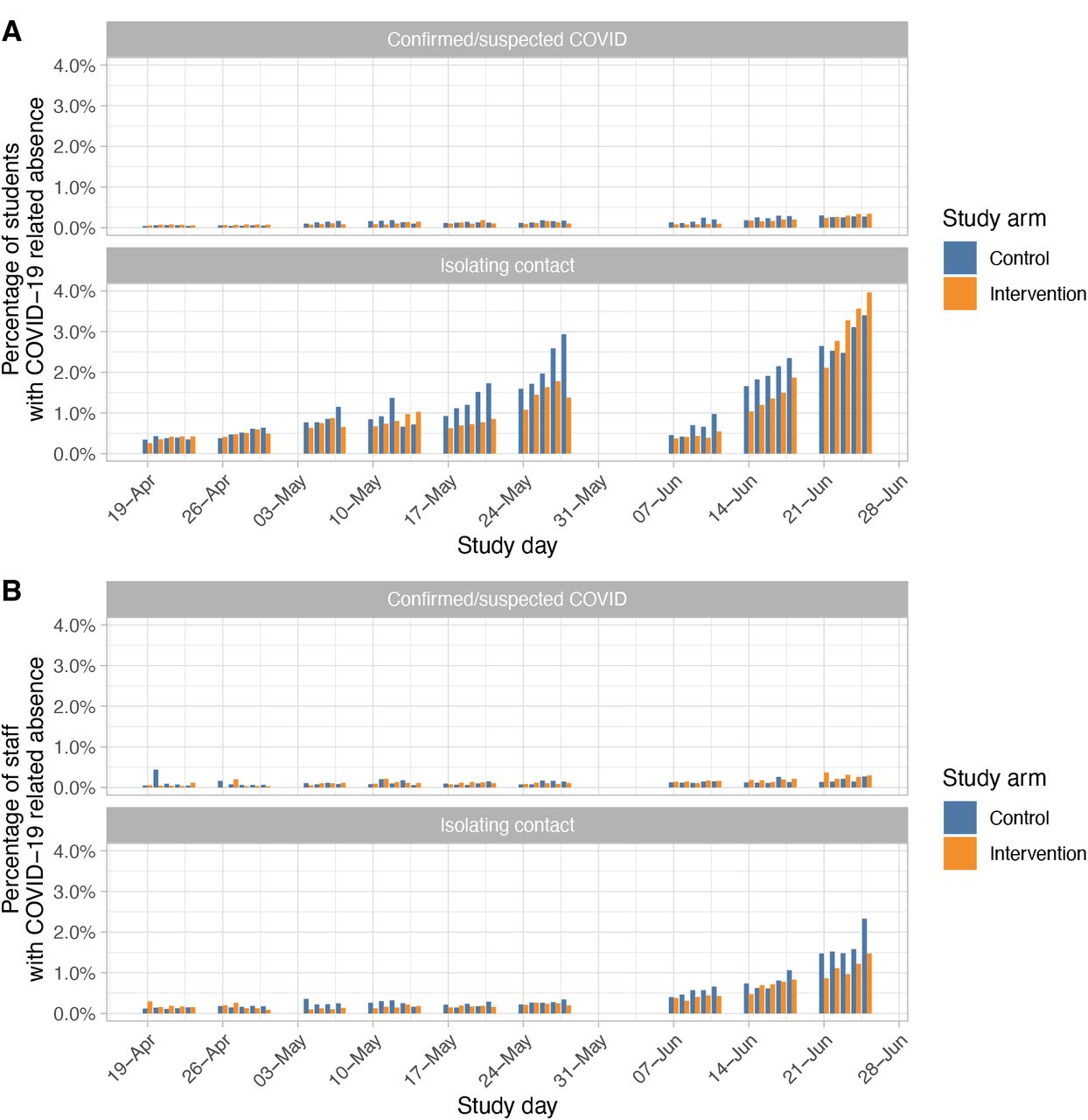
Note the school “half-term” holiday (31-May-2021 to 04-June-2021).
On an ITT basis, adjusting for the randomisation strata group and participant type, the adjusted incidence rate ratio, aIRR, for COVID-related absence in the intervention arm was 0.80 (95%CI 0.54-1.19;p=0.27) (Table 4;Table S2). Overall, staff were less likely to be absent for COVID-related reasons than students (aIRR=0.39;95%CI 0.31-0.48;p<0.001), but there was no evidence a difference in the effect of the intervention between students and staff (heterogeneity p=0.98). As no covariate changed with time, the originally proposed approach has a more conservative confidence interval than required. We repeated the analysis aggregating the data per school and participant type, yielding an aIRR of 0.80 (95%CI 0.62-1.03;p=0.085;Table S3).
Results of a quasipoisson regression model using data accounting for clustering by school using variance adjustment. 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Results of a quasipoisson regression model using data aggregating data to a single row per school and participant type. 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
aIRR, adjusted incidence rate ratio for rates; aOR, adjusted odds ratio for proportions; CI, confidence interval.
As per day participation in the intervention arm was 49.5%, we estimated the impact of the intervention among those participating; the point estimate showed a greater reduction in absences (CACE aIRR=0.61 (95%CI 0.30-1.23;Table S2). Applying this point estimate to COVID-related absence in control arm students (1.80%), would equate to a 39% relative and 0.70% absolute reduction in school days missed due to COVID. CACE estimates were relatively unaffected by the choice of imputation strategy for schools with missing compliance (Table S4). Separate ITT and CACE results for students and staff are provided in Tables S5 and S6.
Results of quasipoisson regression models using data accounting randomisation strata group, participant type and for clustering by school using variance adjustment are shown. IRR, Incidence Rate Ratio, CI = Confidence Interval, CACE, complier average causal effect.
Results of a quasipoisson regression model using data accounting for clustering by school using variance adjustment. 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Results of a quasipoisson regression model using data accounting for clustering by school using variance adjustment. 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
There was no evidence of an impact on all-cause absence rates (ITT aIRR=0.97, 95%CI 0.82-1.16, p=0.77), with non-COVID-related reasons responsible for most absences (Table S7).
Results of a quasipoisson regression model using data accounting for clustering by school using variance adjustment. 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect. Overall, all-cause absences were considerably higher than COVID-related absences, 19.7% in students and 8.3% in staff, in part because students in two school years were granted study leave during weeks 7-10 of the study, and only a minority of several large further education college students were expected to attend each day.
Symptomatic PCR-confirmed SARS-CoV-2 infection
PCR results from symptomatic SARS-CoV-2 infections in students were available for 96/99(97%) control schools and 101/102(99%) intervention schools and staff results for 76(76%) and 85(83%) respectively.
614 and 683 students at control and intervention schools tested PCR-positive while at risk and reported symptoms during 6,966,653 and 7,541,525 days at risk (61.7 and 63.4 cases/100,000 population/week). Rates in staff were 43/790,219 (38.1/100,000/week) and 57/819,487 (48.7/100,000/week). Incidence rose during the study, as the Delta variant spread nationally[20] similarly in each arm (Figure 4A). Incidence was higher than the number of index cases reported by schools, partly because not all randomised schools actively reported cases and additionally because even in active schools not all community-diagnosed infections were reported or recorded (Table S8).
Index cases were reported to schools by students and staff and recorded by schools in study records. Details of students and staff at schools allowed matching to national testing data (NHS Test and Trace).

Weekly incidence is shown per 100,000 at risk. The shaded area is the mean rate ± 1 standard deviation using a negative binomial model to account for over-dispersion (theta=0.28).
Adjusting for the randomisation strata, participant type, and the background community rate of reported SARS-CoV-2 infection in the previous week, there was no evidence of difference between study arms in symptomatic PCR-confirmed infection (ITT aIRR=0.96;95%CI 0.75-1.22;p=0.72) (Table 4;Table S9). Overall rates of infection were lower in staff than students (aIRR=0.75;95%CI 0.61-0.92;p=0.006), but there was no evidence that the effect of the intervention differed in staff and students (heterogeneity p=0.41). Infection rates in students were approximately linearly related to local case counts, plateauing as community incidence rose (Figure S2); estimates were similar with varying plausible lags between community case counts and student and staff infections (Table S10).

Model, with a 4 knot spline (with default positioned knots) adjusted for strata group and study arm, shown for Government-funded, 11-18y, free school meals ≤17% schools in the control arm.
Results of a quasipoisson regression model accounting for clustering by school using variance adjustment. In the adjusted analysis, adjustment is also made for community case counts in the prior week using a 4 knot spline (default placed knots, with number up to five chosen on the basis of BIC in a Poisson regression model) (see Figure S2). 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Results are shown for quasipoisson regression models adjusting for randomisation strata group and participate type, accounting for clustering by school using variance adjustment, with varying adjustments for community case rate. Adjustment for community case counts in the prior week is using a 4 knot spline (default placed knots). 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
A CACE analysis allowing the impact of the intervention to be estimated given theoretical full participation, also showed no evidence of difference between study arms in symptomatic PCR-confirmed infection (aIRR=0.86;95%CI 0.55-1.34). CACE estimates were relatively unaffected by the choice of imputation strategy for schools with missing participation data (Table S11).
Results are shown of quasipoisson regression models using data adjusting randomisation strata group, participant type, and community case rates in the prior week, with allowance for clustering by school using variance adjustment. IRR, Incidence Rate Ratio, CI = Confidence Interval, CACE, complier average causal effect.
Similar results were obtained in a secondary analysis of any positive PCR-result from routine community-based testing (Figure 5B) (ITT aIRR=0.96;95%CI 0.76-1.20;p=0.71 and CACE aIRR=0.88;95%CI 0.57-1.41) (Table S12). There was no evidence of a difference in the effect of the intervention for students and staff (ITT model, heterogeneity p=0.21). Separate analyses for students and staff for symptomatic and any PCR-positive infection are presented in Tables S13-S16.
Results of a quasipoisson regression model accounting for clustering by school using variance adjustment. In the adjusted analysis, adjustment is also made for community case counts in the prior week using a 4 knot spline (default placed knots, with number up to five chosen on the basis of BIC in a Poisson regression model) (see Figure S2). 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Incidence of PCR-confirmed infection in contacts
PCR testing of asymptomatic contacts was undertaken in 886 non-overlapping contact episodes in the control arm, 14(1.6%) tested PCR-positive, 1 (0.1%) indeterminate and 871 (98%) negative. In 2981 intervention arm contacts, 44(1.5%) tested positive, 14(0.5%) indeterminate and 2923(98%) negative. Adjusting for randomisation stratification group and community case counts in the prior week, there was no evidence that the proportion of contacts testing positive varied between study arms (aOR=0.73;95%CI 0.33-1.61;p=0.44) (Table S17). Of control and intervention arm contacts testing positive/indeterminate, 4/15(27%) and 19/58(33%) went on to have a positive symptomatic test (exact p=0.76).
Results of a quasipoisson regression model accounting for clustering by school using variance adjustment. In the adjusted analysis, adjustment is also made for community case counts in the prior week using a 4 knot spline (default placed knots, with number up to five chosen on the basis of BIC in a Poisson regression model) (see Figure S2). 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Results of a quasipoisson regression model accounting for clustering by school using variance adjustment. In the adjusted analysis, adjustment is also made for community case counts in the prior week using a 4 knot spline (default placed knots, with number up to five chosen on the basis of BIC in a Poisson regression model) (see Figure S2). 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Results of a quasipoisson regression model accounting for clustering by school using variance adjustment. In the adjusted analysis, adjustment is also made for community case counts in the prior week using a 4 knot spline (default placed knots, with number up to five chosen on the basis of BIC in a Poisson regression model) (see Figure S2). 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Results of a quasipoisson regression model accounting for clustering by school using variance adjustment. In the adjusted analysis, adjustment is also made for community case counts in the prior week using a 4 knot spline (default placed knots, with number up to five chosen on the basis of BIC in a Poisson regression model) (see Figure S2). 1IRR = Incidence Rate Ratio, CI = Confidence Interval. ITT, intention to treat; CACE, complier average causal effect.
Results of a logistic regression model are shown, with variance adjustment to allow for repeated measurements in participants from the same school. 1OR = Odds Ratio, CI = Confidence Interval. As a sensitivity analysis the model was also refitted regarding those with indeterminate results as positive, yielding an adjusted OR for the intervention arm of 0.89 (95%CI 0.34, 1.86; p=0.76).
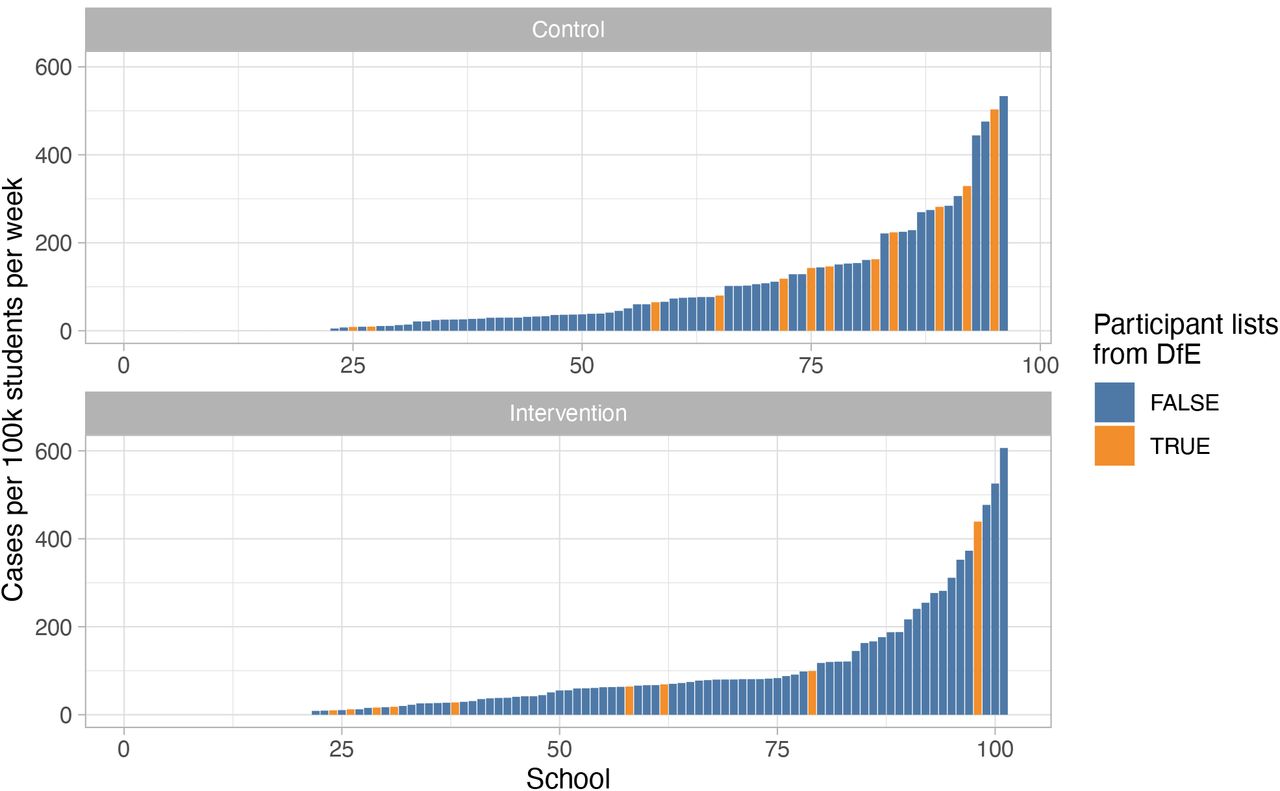
We also compared the proportion of contacts with a symptomatic PCR-positive test, which included those initially testing positive while asymptomatic above who went on to have a symptomatic test. This analysis is contingent on schools reporting contacts, with several control arm schools with higher incidence not actively participating and reporting contacts (Figure S3). In the control arm 44/4665(0.9%) of contacts tested PCR-positive within 10 days, compared to 79/5955(1.3%) in the intervention arm. Adjusting for randomisation strata groups and community case counts, there was no evidence that the proportion of contacts testing positive differed between arms (aOR=1.21;95%CI 0.82-1.79;p=0.34) (Table S18).

Schools actively participating in the study and therefore potentially reporting contacts are shown in blue. Schools not actively participating, for which, student lists where obtained from the Department for Education (DfE) are shown in orange.
Results of a logistic regression model are shown, with variance adjustment to allow for repeated measurements in participants from the same school. 1OR = Odds Ratio, CI = Confidence Interval
Performance characteristics of LFDs vs. PCR
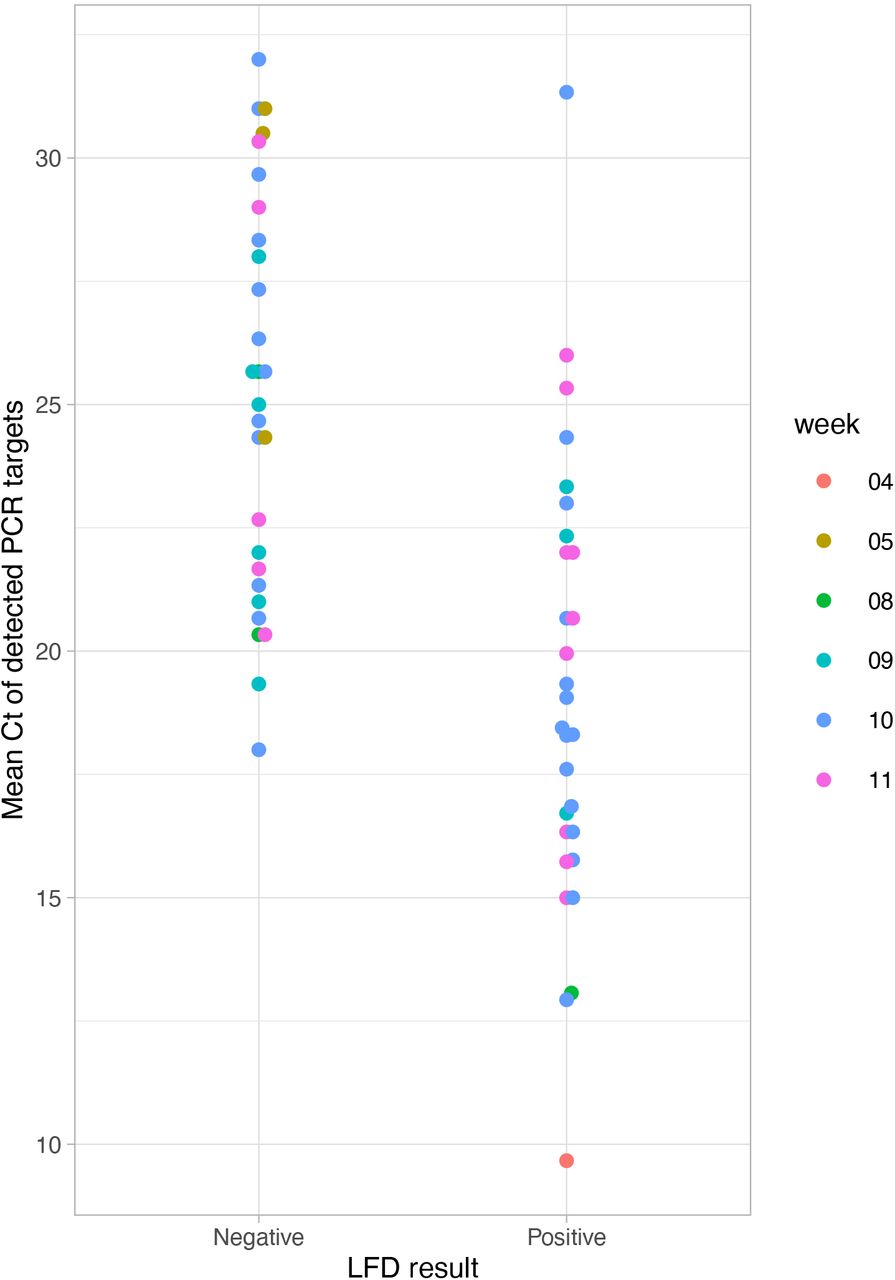
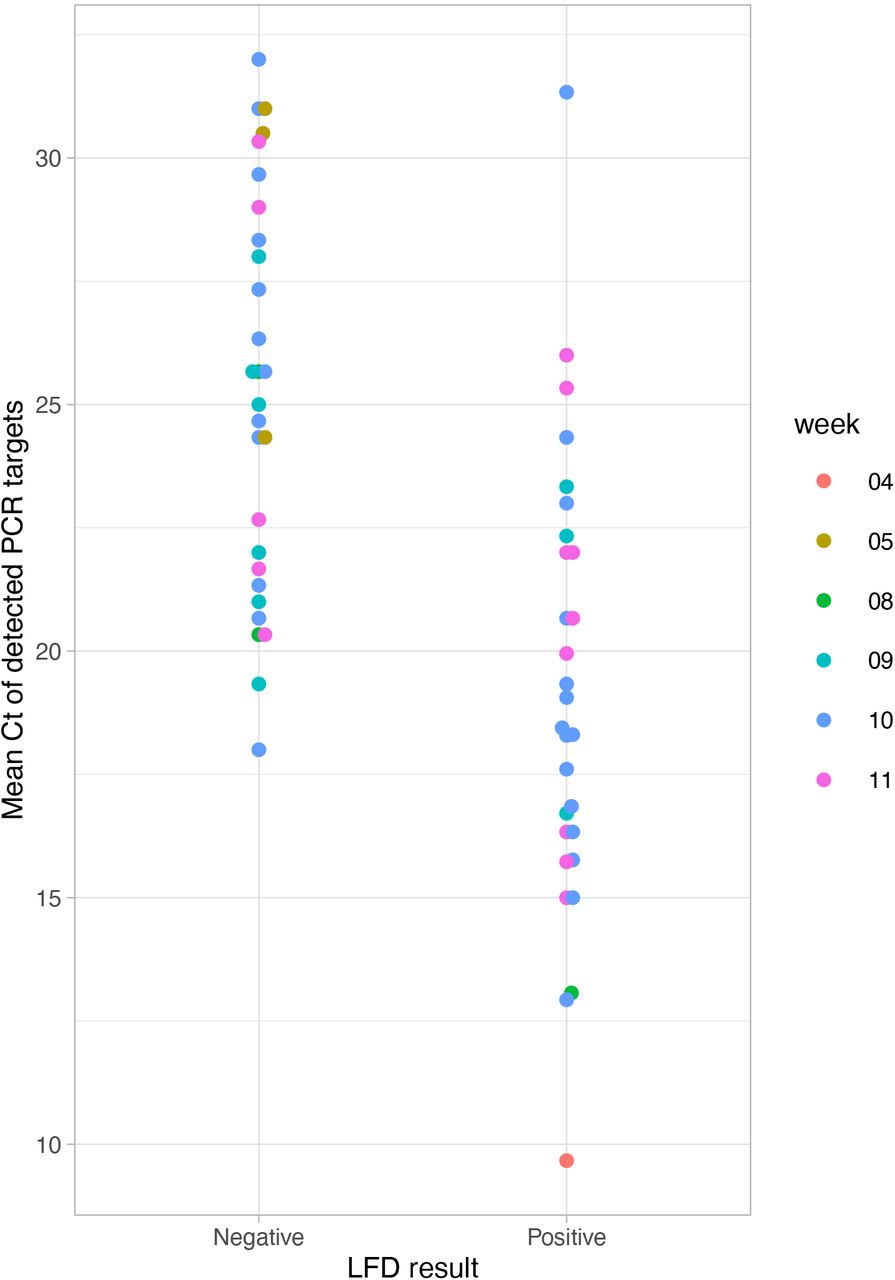
Across the study, and the non-randomised pilot phase, 4757 contacts completed at least one LFD during DCT generating 20,289 LFD results in total. For 3226 a paired PCR test was available from the same day, or up to 2 days later for those testing LFD-positive, 3166 were PCR-negative and 60 PCR-positive. Specificity was 3164/3166 (99.93%, exact binomial 95%CI 99.77-99.99%) and sensitivity 32/60 (53%, 40-66%) (Table S19). PCR-positive cycle threshold (Ct) values were lower in those testing LFD-positive (median 18.5, IQR 16.3-22) than LFD-negative (median 25.3, IQR 21.6-28.5) (Kruskal-Wallis p<0.001;Figure S4).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Among contacts testing positive by LFD, Ct values were available in 29/32 (90%). Points are coloured according to the period of the study in which the swab was collected, with 19-April-2021 as the start of week 1.
Sensitivity, specificity, positive predictive and negative predictive values given, with 95% confidence intervals calculated by exact binomial method.
Discussion
Daily LFD testing of school-based COVID-19 contacts was trialled as a voluntary alternative to 10 days of self-isolation. Although DCT avoids students and staff missing school days while isolating, at the conception of the trial there was uncertainty whether it would substantially increase SARS-CoV-2 transmission, e.g. via infections missed by LFD testing.[2] The trial provides evidence this was not the case.
We investigated the incidence of symptomatic infection as an unbiased outcome measure that could be ascertained across nearly all schools, as national public health policy was that all symptomatic children, whether or not they had a LFD test, should obtain a PCR test for SARS-CoV-2. As the intervention was not expected to impact the relative incidence of asymptomatic versus symptomatic infection this measure should also indicate the impact on all infections. Based on a non-inferiority margin of ensuring symptomatic infection did not increase by >50%, we show allowing student and staff contacts to remain in school after a negative lateral flow test was non-inferior to routine isolation. On an ITT basis, i.e. using lateral flow testing at participation rates seen in the trial, using data for students from 197/201 schools and staff data from 161/201 schools, we can be 97.5% confident that any increase in the rate of symptomatic infection did not exceed 22% more than seen in the control arm. Were all those eligible to participate in daily lateral flow testing to do so, then, based on a CACE model, we can be 97.5% confident that any increase does not exceed 34%. In both analyses the point estimate favours a slight to modest reduction in incidence with the intervention.
The range of absolute changes in symptomatic infection rates potentially seen with the intervention, depends on prevailing incidence. At the average incidence in the control arm during the study (0.06% students/week), the range of uncertainty in the impact of the intervention is equivalent to 1.2 fewer to 0.9 more infections/1000-student-school/month, or 3.6 fewer to 2.7 more at the highest weekly rate seen (0.18% students/week). Throughout the study, cases in both arms remained well below the >1% level seen in 2020 when schools remained open.[21] Staff had lower rates of infection than students. There was no evidence of a difference in the effect of the intervention for students and staff.
In both control and intervention arms it was uncommon for school-based contacts to become infected with no evidence of a difference in asymptomatic or symptomatic infection: 1.6% and 1.5% of students and staff participating in research PCRs tested positive while asymptomatic, and 0.9% and 1.3% tested positive in symptomatic testing for the control and intervention arms respectively. These figures are comparable to the estimates for school age children from national contact-tracing data.[16] Therefore, given precautions in place in schools during the trial (routine mask use was discontinued part way through the trial on 17-May-2021, but other precautions were maintained), the overall risks to students and staff following exposure to a contact at school are low. Indeed, whether the extent of transmission is sufficient to make any contact testing necessary and cost-effective will require careful discussion and may vary with changes in incidence, virus transmissibility or the prevalence of vaccine evasive strains. Participation in research PCR testing in control schools was lower than in the intervention schools, in part because participation in DCT facilitated intervention arm PCR-testing. It is unclear whether this caused any bias in the results for the research PCR tests, however we also found no difference in symptomatic infection rates in contacts.
We did not clearly demonstrate superiority of the intervention in terms of avoiding student and staff absences from school related to COVID. This possibly reflects that the trial was relatively underpowered given the large extent of variation in absence rates over time and between schools, requiring overdispersion to be accounted for in the regression models fitted. Pooling the data on a per school basis, in an ITT analysis, our point estimate showed a 20% decrease in COVID-related absences, but with a broad range of uncertainty (95%CI 0.62-1.03), similarly in the CACE analysis amongst those who participated the point estimate was a 38% reduction, but with broader uncertainty (95%CI 0.29-1.33).
That reductions in COVID-related absences were not greater reflects firstly that not all those eligible chose to participate, and secondly that not all absences were amenable to the intervention, e.g. those who with household contacts were ineligible. However, despite the lack of statistical evidence from the trial, in the absence of increased transmission, it is reasonable to assume that a policy of allowing students and staff to remain in school, would indeed lead to increased attendance, but this may be more limited than might be initially anticipated.
Overall participation rates in LFD testing in intervention arm contacts were 42% of a per person basis with marked variation between schools (range 0-100%). Although contacts at government-funded schools with students 11-16 years old with a low percentage of free school meals were most likely to participate, other school types were similar. Staff were more likely to participate than students. A qualitative analysis of interviews with participants to understand why some participated and others did not will be presented separately. Additionally, at some stages, schools paused the intervention either because of capacity limitation or because public health officials were concerned about the spread of the Delta lineage or rising transmission in the community. No local public health teams reported concern that transmission was observed to increase because of this study.
Previous estimates for the performance of antigen LFDs compared to PCR testing have varied markedly.[6, 22] Here we estimate the overall sensitivity of school-based LFD testing in largely asymptomatic individuals as 53%, which falls within the range of previously reported rates. It is worth noting the findings on transmission in this study are in the context of this level of performance. Specificity was 99.93%. As LFD performance varies by viral load[23] this overall performance is subject to change as the population viral load distribution changes. Consistent with previous reports[6] we find that higher viral loads, i.e. lower PCR cycle threshold values, are associated with increased sensitivity, and therefore LFDs are more likely to detect those who are most infectious.[16]
The study has several limitations. Schools and colleges, despite provision of dedicated resources, were not always able to participate due to competing pressures, and it is also likely as a result that data capture was imperfect, e.g. it is possible that not all PCR-positive cases were reported to schools, and not all contacts may have been documented for all index cases. However, how the primary outcome measures are assessed is robust to this. We used the incidence of symptomatically driven testing as a primary endpoint as this was least likely to be affected by the two testing strategies; in fact, there was little difference in the incidence of all community PCR tests between the study arms. Relying on linkage to Test and Trace data is also a potential weakness, as it depended on imperfectly recorded identifiers, however this would not be expected to differ between study arms. Furthermore, using incidence data means we do not directly measure within school transmission, rather we estimate it by controlling for the rate of community infections, as a proxy for the extent of introductions into the school. The trial was conducted during periods of low to moderate COVID-19 incidence. We therefore did not estimate the impact of DCT in high incidence settings. In the last two weeks of the study, the community rate of infections rose making the DCT protocol unwieldy for some schools, given the space and staff required to perform testing.
Future work includes whole genome sequencing of positive samples from school members and from the community, which may help analyse the transmission networks in schools, including during periods of higher incidence in a manner successfully achieved for SARS-CoV-2[24, 25] and a number of healthcare-associated pathogens.[26, 27] This study includes staff and students from secondary schools and colleges of further education but most of the participants were students aged 11-18 years. Therefore, it is unclear the extent to which it can be generalised to other settings, and other context-specific studies are required.
Overall, this study shows that in secondary school and college of further education students and staff infection of following contact with a COVID-19 case at school occurs in less than 2%. There was no evidence that switching from isolation at home to daily contact testing, at least in the settings of the schools studied, increased rates of symptomatic COVID in students and staff. Daily contact testing is a safe alternative to home isolation following school-based exposures and should be considered an alternative to routine isolation of close contacts following school-based exposures.
Transparency declaration
DWE reports lecture fees from Gilead outside the submitted work. RO and DC are consultants employed by DHSC as part of Deloitte’s broader project work supporting the delivery of NHS Test and Trace. TF reports honoraria from Qatar National Research Fund (QNRF) outside the submitted work, no other author has a conflict of interest to declare.
Funding
This study was funded by the UK Government Department of Health and Social Care and supported by the UK Government Department for Education and Office for National Statistics. The work was also supported by the National Institute for Health Research Health Protection Research Unit (NIHR HPRU) in Healthcare Associated Infections and Antimicrobial Resistance at Oxford University in partnership with Public Health England (PHE) (NIHR200915) and the NIHR Biomedical Research Centre, Oxford. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health and Social Care, the Department for Education, the Office for National Statistics or Public Health England. BCY is an NIHR clinical lecturer. BCY, TEAP and LY received grants from DHSC to fund this work. DWE is a Robertson Foundation Fellow. For the purpose of open access, the authors have applied a CC BY public copyright licence to any Author Accepted Manuscript version arising from this submission.
Data availability
Data from the trial will be available within the Office for National Statistics Secure Research Service. Applications for access can be made by Accredited Researchers. For more details please see - https://cy.ons.gov.uk/aboutus/whatwedo/statistics/requestingstatistics/approvedresearcherscheme.
Supplementary methods
Randomisation
Schools were randomly assigned 1:1 to either a policy of offering contacts daily testing over 7 days to allow continued school attendance (intervention arm) or to follow usual policy of isolation of contacts for 10 days (control arm). Randomisation was performed in blocks of 2 and stratified using nine strata to ensure a sample representative of schools and colleges in England. Stratification was performed according to school type, size, presence of a sixth form, presence of residential students and proportion of students eligible for free school meals (as a marker of social deprivation), the nine strata are listed in Table 1. Randomisation was performed by a trial team member in Stata (version 16).
10 schools participated in a non-randomised pilot of the study protocol in March 2021. During the main study they continued to follow the intervention procedures, but do not contribute to the analysis of randomised outcomes.
Procedures
Forms of close contact applicable to schools as defined in national guidelines were, face to face contact (within 1 metre for any length of time) or skin to skin contact or someone the case coughed on; or within 1 metre for ≥1 minute; or within 1-2 metres for >15 minutes. Any person who met the definition of being in close contact with a case in the two days prior to symptom onset (or prior to positive test if asymptomatic) was required to self-isolate for 10 days.
In the intervention group, daily contact testing was performed with a lateral flow device on arrival at school or college each morning. Day 1 of testing began the day after a case was identified. Where there was a delay to the start of testing, contacts could opt to start DCT within 3 days of a case being identified. Testing was done over 7 consecutive days, and a minimum of 5 test was required (allowing for no testing on weekends). Five negative tests, including one on or after the 7th day of testing was required to complete DCT, at which point contacts were released from self-isolation. Contacts who opted to stop testing during the process reverted to self-isolation for 10 days. Contacts who tested positive during DCT were instructed to self-isolate for 10 days from the positive test.
Data collection
Data were collected using a web-based data capture system (Voyager, IQVIA).
Schools reported in aggregate the number of staff and students present on each school day, and numbers absent for COVID-19-related reasons and separately numbers absent for other reasons. Attendance data for individual participating students and staff members were not collected.
PCR testing
Results of routine community tests performed outside of the study for SARS-CoV-2 in staff and students were obtained from national public health data (“NHS Test and Trace”). Matching of results to study participant identifiers was undertaken by the UK Government Department of Health and Social Care (DHSC). Results were matched based on an exact match of (surname, date of birth, home postcode) OR (first name, surname, date of birth, testing centre and school lower-tier local authority [LTLA]) OR (first name, surname, year of birth, home postcode). An iterative approach with manual review of school-reported and Test and Trace cases was used to define the matching rules. Test and Trace results recorded whether the individual was symptomatic or not prior to testing.
Routine community-based testing was undertaken by a network of accredited diagnostic laboratories, with high-throughput national “Lighthouse laboratories” undertaking testing with the ThermoFisher TaqPath assay undertaking the most tests.
Dedicated study PCR testing was also undertaken. All individuals who tested positive for SARS-CoV-2 by either LFD or PCR for SARS-CoV-2 infection who consented were asked to provide a swab of nose and throat for PCR testing. Additionally, all close contacts in either study arm who consented to participate were asked to provide a swab of nose and throat for PCR testing on day 2 and day 7 of their testing/isolation period. For contacts undergoing DCT the test was done on the nearest school day.
Swabs for PCR testing were sent by courier or mail to a central laboratory and forwarded for testing at an accredited clinical microbiology laboratory (Oxford University Hospitals NHS Foundation Trust). Samples were stored at -20°C for up to 2 weeks. RNA extraction was performed using the KingFisher (Thermo Fisher) automated extraction system. SARS-CoV-2 PCR was performed using the Thermo Fisher TaqPath COVID-19 kit. Detection of both N and orf1ab targets was required for a positive result, with the cycle threshold (Ct) for one target ≤32 and the other ≤33. Samples with no detected viral targets were considered negative and all other samples indeterminate.
Statistical analysis
The rate of COVID-19-related absences from school amongst those otherwise eligible to be in school (i.e. not absent for another reason) were compared between the study arms. Students and staff were considered at risk of a COVID-related absence, while not absent for other reasons, on school days following enrolment of the school into the study from 19-April-2021 onwards until 27-June-2021. Weekend days, national holidays, the school half-term holiday (31-May-2021 to 04-June-2021), and individual school non-school days were excluded.
Total rates of COVID-19-related absence per school were compared on an intention to treat (ITT) basis, testing for superiority of the intervention, for all schools with available data irrespective of whether they participated after randomisation or not. Models were fitted using quasi-Poisson regression to account for overdispersion. Pre-specified adjustment was made for 6 study stratification groups (Government-funded, 11-16y, free school meals ≤17%; Government-funded, 11-18y, free school meals ≤17%; Government-funded, 11-16y, free school meals >17%; Government-funded, 11-18y, free school meals >17%; Independent schools; Other), combining several of the smaller original randomisation strata given small numbers in these strata, and for participant type (student or staff). Repeated daily measurements from the same school were accounted for using robust standard errors with clustering by school. We also present results combining data from each school during the study without robust standard errors.
We compared the incidence of symptomatic PCR-positive SARS-CoV-2 infection between arms using quasi-Poisson regression. Individuals were considered at risk of an infection on all calendar days (school days and non-school days) from the later of the date of the start of the study (19-April-2021) or enrolment of their school, up until the end of the last week of the study (27-June-2021). Weekly incidence data were used, adjusting for the 6 study stratification groups above, participant type, and community PCR-positive case rates in the local population in the prior week. Adjustment for community case rates was designed to allow the analysis to assess any excess in cases in the intervention arm over and above that expected from importation of community-acquired cases into the school. Sensitivity analyses examined the impact of using differing lag periods between community and school case counts of 1 and 4 weeks prior, and without adjustment for community case counts. Community case counts were obtained from nationally reported data, publicly available on the gov.uk website, at the LTLA level, using data from the LTLA within in which the school was situated. Repeated measurements from the same school were accounted for using robust standard errors with clustering by school. The relationship between community case rates in the prior week and the outcome was modelled using natural cubic splines to allow for non-linearity, up to 5 default-placed knots were allowed, choosing the final number of knots based on model fit according to the Bayesian Information Criterion. To avoid undue influence of outliers community case rates were truncated at the 2.5th and 97.5th centiles.
No interaction terms were included in either of the co-primary outcome models, however we tested for heterogeneity in the effect of the intervention on students and staff in separate models. We also present subgroup analyses in students and staff separately.
To account for incomplete participation in DCT, we present complier average causal effects (CACE) estimates for both primary outcomes, estimated using the randomisation arm as an instrumental variable and a two-stage regression approach. In this approach, we first fit two models: 1) the relationship between study arm and measured compliance, adjusting for the covariates above; 2) the relationship between measured compliance and the outcome, adjusting for covariates, but not study arm. These estimates are combined to estimate the impact of the intervention amongst those actively participating.
For the COVID related absence analysis compliance was calculated per school and participant type, as the sum over all study school days of individuals eligible for DCT returning a test result or already having completed follow up each day, divided by the sum of individuals eligible for DCT. For the symptomatic infection outcome, compliance was calculated per school, participant type and week, as other covariates varied by week. For schools in the control arm and those in the intervention arm not actively participating compliance was set to zero. For participating schools without any eligible contacts in a given week the median compliance per schools was used, and where no eligible contacts were identified during the study the median compliance per randomisation stratification group. Sensitivity analyses were performed using the 25th and 75th centiles for imputation instead of the median value.
For the symptomatic infection outcome, to account for repeated measurements by school, confidence intervals for CACE estimates were generated from 1000 bootstrap samples, using bias-corrected and accelerated bootstrap intervals, and sampling based on school clusters.
We report uptake of LFD testing for intervention arm participants, on a per day and per participant basis. For the per day analysis, we identified all school days between a contact being identified and day 10 following their first exposure to the index case. Participation was defined as either return of a test result or where testing had been completed, i.e. ≥5 test results were already available or a prior positive test had occurred. For the per participant analysis, we pre-defined participation as a school recording ≥3 negative or ≥1 positive LFD test result for the participant. We used logistic regression to investigate factors associated with per individual participation rates, including the randomisation stratification groups, participant type, age, sex, and ethnicity. We used variance adjustment as above to allow for clustering of results by school.
The proportion of close contacts testing positive on an asymptomatic research PCR test was compared between study arms using logistic regression, given there were relatively few events, adjustment was made only for randomisation strata groups and local case counts in the previous week (at the LTLA level as above). As individuals could be contacts on multiple occasions, including simultaneously with different index cases, we deduplicated our data to present one result per non-overlapping contact episode, defining each episode as the 10 days from the index case. We also use symptomatic community-based testing data from NHS Test and Trace to present the proportion of contact episodes associated with a symptomatic PCR positive result in the 10 days following the diagnosis of the index case. For both asymptomatic and symptomatic analyses we only consider contacts at risk prior to their first positive result in the study, as any subsequent result within the 70 days of the study could represent residual RNA from the first infection. We account for clustering of results by school as above.
We compared the performance of LFD to PCR testing in participants tested by both methods on the same day, regarding PCR testing as the reference standard. Additional data from a pilot phase of the study, involving 10 non-randomised intervention schools was included in this analysis only.
Analyses were performed using R (version 4.1), and the following libraries: tidyverse (version 1.3.1), ivtools (version 2.3), sandwich (version 3.0.1), and gtsummary (version 1.4.1).
Sample size and power
We powered to trial to detect a difference in school attendance. We assumed of 100 similarly-sized schools randomised to each arm, ∼50% would participate. In the control arm we assume 30% participation in national twice weekly LFD testing outside the trial, such that index cases would be identified at a rate of 1 per school per month, with each associated with 50 contacts. Hence with an isolation period of 10 days, 510 isolation days per school per month would occur in the control arm. For the intervention arm, we assume the intervention would increase uptake of routine LFD testing two-fold to 60% with the barrier of potential isolation removed. Therefore, the expected rate of index case detection from routine testing doubles to 2 per month. We assume that 70% of contacts will participate in DCT, such that only 15 per index case self -solate, with an additional 2 per index case self-isolating following a positive LFD in DCT, but without further contacts outside of the existing contacts. This results in an expected 170 missed school days per index case or 360 per month. Based on these assumptions we estimated that 58 participating schools in each arm provides 80% power (two-sided alpha=0.05) to detect a difference in attendance between the study arms. However, the number of pupils varied substantially by school and therefore the original analysis based on the sample size calculation (which assumed approximately equal school sizes) was not appropriate. Further, there was substantial evidence of over-dispersion which we also had to account for in the analysis.
Trial Steering Committee
Martin Llewelyn (University of Sussex) (Independent Chair), Carole Torgerson (University of York) (Independent member, educational research), John Tomsett (Independent member, head teacher), Susan Blenkiron (Independent member, parent). Non-voting members: Sidonie Kingsmill (DHSC Sponsor), Tessa Griffiths (DfE), Sarah Maclean (DfE), Tom Fowler (Public Health England), Catherine Hewitt (University of York) (Statistical advisor), Lucy Yardley (Behavioural Study) Tim Peto (Principal Investigator), Bernadette Young (Trial Clinician), David Eyre (Data Analysis), Saroj Kendrick (Trial Manager).
Trial Management Group
Tim Peto (Principal Investigator), Bernadette Young (Trial Clinician), Sarohj Kendrick (Project Manager), Chris White, Sylvester Smith, Nicole Solomon
Protocol Development
Tim Peto, Tom Fowler, Peter Marks, Nick Hicks, Susan Hopkins, Lucy Yardley, Richard Ovens, David Chapman, Sarah Tunkel
Independent Data Monitoring Committee
Neil French (University of Liverpool) (Chair), Katherine Fielding (London School of Hygiene and Tropical Medicine) (Statistician), Punam Mangtani (London School of Hygiene and Tropical Medicine), Catherine Hewitt (University of York) (unblinded statistical advisor), Nicole Solomon (secretariat)
Database curation
ONS DCT Group (Ian Diamond, Fiona Dawe, Ieuan Day, Lisa Davies, James McCrae, Ffion Jones, Paul Staite, Andrea Lacey, Joseph Kelly, Urszula Bankiewicz); DHSC Test and Trace Group (Joseph Hillier, George Beveridge, Toby Nonnemacher, Fegor Ichofu)
Analysis Group
Bernadette Young, David Eyre, Tim Peto, (thanks to Sarah Walker for statistical advice)
Writing Committee
Bernadette Young, David Eyre, Tim Peto
Acknowledgements
We would like to acknowledge all the students and staff at participating schools for contributing to the study, and in particular the study workers at each of the schools. We are thankful to the Microbiology department of Oxford University Hospitals NHS Foundation trust for performing PCR testing. Additionally, we acknowledge the support in conducting the study of the DHSC DCT project management team, especially Nichole Solomon, and the ONS DCT team. We thank DfE colleagues, especially Sara Cooper, Matt Mawer and Richard Lumley for their assistance. We thank Professor Sarah Walker for insightful advice.
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
6
Blogs/Media
Author Videos