
Abstract
Background Medical students experience significant stress and anxiety during undergraduate education. Coaching is a possible way of supporting these students throughout this challenging time. To assess the benefits of coaching for medical students, a pilot study providing coaching was performed. This pilot assessed how coaching affected the mental health of medical students and how coaching was received by them.
Methods Twelve third-year medical students were each given eight 30-60 minute coaching sessions. Each participant took the Hospital Anxiety and Depression Scale (HADS) and the Perceived Stress Scale (PSS) pre-, mid-and post-coaching. After coaching, there were three open-ended questions to measure the reactions to coaching and a scale to determine the likelihood of accessing coaching in the future.
Results There was a significant effect of coaching on perceived stress(p=.023); a trend toward significant effect of coaching on anxiety(p=.057); and no effect of coaching on depression. Qualitative analysis indicated Affective responses (gaining perspective and self-awareness); Cognitive responses (goal setting and working through solving problems); and Skills responses (developing reflection abilities and critical thinking). Attributes of coaching included perceiving coaching as a positive, individualized and supportive experience that students were highly likely to access again.
Conclusions Coaching holds promise as an intervention offered to medical students to reduce stress and anxiety, and provide positive support for students, preparing them for their professional futures.
Key Points
Appreciate the stress and anxiety that medical students manage in medical school.
Coaching is an option that holds promise to support medical students.
Coaching has possible long-term outcomes that could help future physicians navigate their professional paths more effectively.
Students value individualized, positive support during medical school
Background
Medical students in their undergraduate education may experience significant stress and anxiety because of the transitions and identity formation they are experiencing (Dyrbye et al.,2006)(Kumar et al.,2019). They are engaged in coursework and decisions about clerkships, sub-internships, applications for residency, and interviews, critical for their future professional and personal development. These students need to be supported in navigating this journey, make the best decisions for themselves and develop skills in finding their own most meaningful paths. Coaching is a way of supporting students throughout this tumultuous time while providing an opportunity for the development of agency, confidence and thoughtful decision-making as they assume their professional roles.
Coaching has been a mainstay in the executive environment, yet it has been slow to become integrated in academia. There have been efforts in recent years to offer coaching to faculty, staff and students entering their undergraduate years and coaching has emerged in graduate programs, such as medical school(Cary et al.,2019)(Dieorio and Miller,2016)(Dieorio and Hammoud, 2019). The delivery of coaching for medical students seems to exist in pockets and frequently the model and format are not clearly articulated, yet there has been a trend toward the development of these programs (Dieorio and Miller,2016). Recent publications have sought to clarify the distinction of coaching from advising and mentoring(Dieorio et al., 2021).
Coaching for the purposes of this study is defined as a way of learning and aims at transformation, driven by the person’s choices. With its base in a professional relationship of mutual trust and respect, coaching focuses on the person’s aspirations and goals; and works to facilitate their achievement. Coaching embraces provocative and appreciative inquiry, which leads to new insights and shifts. The International Coaching Federation (ICF) defines coaching as partnering with clients in a thought-provoking and creative process that inspires them to maximize their personal and professional potential(ICF, www.coachingfederation.org).
The effects of coaching during medical school are beginning to be studied, measured and appreciated (Wolff et al.,2020)(Lovell 2018)(Jasinsk et al.,2020). There is support in the literature for the well-being of physicians from coaching (Dyrbye et al,2019). A pilot study, performed by Fried and Irwin with coaching for undergraduate students in Canada, measured perceived stress, anxiety and depression, and found significant changes in stress reduction and qualitative support for the positive experience of coaching (Fried and Irwin, 2016).
For the purpose of assessing the benefits of coaching with medical students, a pilot study providing coaching for students throughout their third year of medical school was performed. The aim of this yearlong coaching pilot was to assess how coaching might affect the mental health (stress, anxiety and depression), self-awareness and overall wellbeing for medical students in their third year, during which they are making critical decisions and anticipating their futures. The results might inform the future use of coaching as an integrated part of the educational experience to support students in a meaningful way as we prepare them to embark on their professional training beyond medical school.
Methods
The Duke University Health System Institutional Review Board for Clinical Investigations conducted a review of this study and declared it to be Exempt from further review in September, 2019 (Protocol ID: Pro00103592). Twelve third-year medical students (10% of the cohort) were recruited from two emails sent in September and January to the third-year class explaining coaching, the pilot project and offering eight coaching sessions to each interested student. The email described the definition of coaching, its purpose, procedures and the assessment measures used in this study. The 30-60 minute sessions were spaced at least monthly, with modifications made for individual student schedules. As per coaching protocol, the students selected the topics for coaching discussion at each session and determined the goals for that session. Sessions were initially held in person (ten students) or via Zoom (two students out of the country), but ultimately all transitioned to Zoom due to the COVID pandemic of 2019/2020. The same coach provided all coaching sessions. This coach completed the academic training of the International Coaching Federation (ICF) and earned the credential of Associate Certified Coach. The ICF approved Competencies, Model and the Code of Ethics for ICF framed the practice of this coach. Figure 1 provides the model of coaching that guided the coaching sessions.

All responding participants signed a consent form and no demographic data was collected outside of gender. A Readiness Assessment for Coaching, adapted by the researchers, with permission from the developer (Gordon-Jones, S), was used to determine the students’ receptivity to coaching. This assessment has 10 items to which the medical student selected yes or no, to determine readiness to participate in coaching. Scores of 9-10 indicate Definitely Ready for coaching; 7-8 indicate Ready for Coaching; 4-6 indicate Coachable with areas to clarify; and 1-3 indicate Not Ready for Coaching. Students needed scores of seven or higher to be eligible for participation in the pilot. There is no reliability and validity data for this assessment.
Each participant, using a self-generated unique identification code to insure de-identification of the data, took the Hospital Anxiety and Depression Scale (HADS) and the Perceived Stress Scale (PSS) pre-, mid-and post-coaching. These scales are easy to administer and are reliable, validated tools(Bjellanda et al.,2002)(Aseri and Zohair, 2015)(Measurement Instrument Database for the Social Sciences, www.midss.org)(Cohen et al.,1983)(Zigmond and Snaith, 1983). The HADS was devised by Zigmond and Snaith to measure anxiety and depression in a general medical population of patients and includes fourteen questions (seven to assess anxiety and seven to assess depression) that are scored from 0-3 indicating the extent to which a student experiences the feeling in the question (Zigmond and Snaith, 1983). Separate scores for anxiety and depression are calculated, with higher scores indicating more anxiety or depression. The Perceived Stress Scale (PSS) was developed by Cohen et al to measure the degree to which situations in life are appraised as stressful and consists of fourteen questions on a 0(Never)-4(Very Often) point scale, with higher scores indicating more stress (Cohen et al.,1983).
Additionally, at the conclusion of coaching, there were three open-ended questions about the coaching experience and a scale to indicate the likelihood of accessing coaching in the future, as shown in Table I.
The HADS and the PSS were administered in hard copy and the open-ended questions were collected via a Qualtrics online survey. Data were analyzed in aggregate and individually for each student utilizing a one-way ANOVA with repeated measures and a Tukey’s post hoc test. The qualitative data were analyzed for emerging themes by consensus of two authors using an applied thematic analysis approach (Guest et al.,2012). All qualitative responses were reviewed by each of the two authors independently and discussed together to determine consensus of the underlying focus of each phrase. Themes emerged and were clarified through consensus.
Results
Of the twelve medical students, eleven identified as female and one identified as male.
Two students were out of the country, so coaching was virtual throughout their experience, whereas ten students transitioned to meeting virtually midway through the coaching. We had 100% response rate for all assessments.
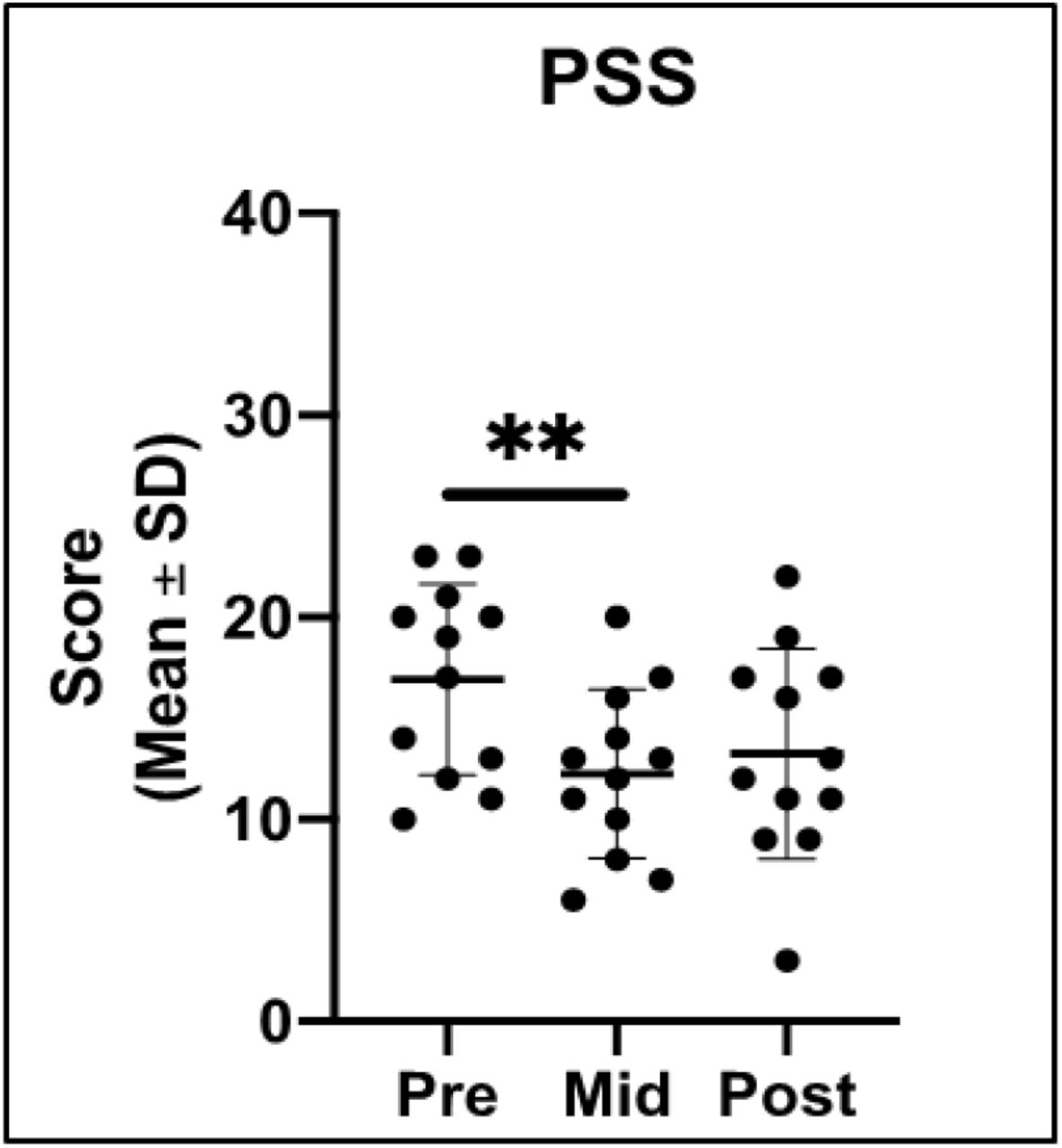
There was a significant effect of coaching on perceived stress. Average PSS scores decreased from 16.92 to 12.25 from pre-test to mid-test, F (1.497, 16.47) = 5.340, p=.023). After four coaching sessions (Mid), PSS scores were significantly lower than baseline (p=.006), as indicated in Figure 2.

There was a trend toward a significant effect of coaching on anxiety from pre- to mid-test (HADS-Anxiety; F (1.957, 21.53) = 3.407, p=.053), as indicated in Figure 3. However, from pretest to mid-point in the coaching the HADS-A scores decreased from 8.25 to 6.17, which did not reach significance (p=.079).

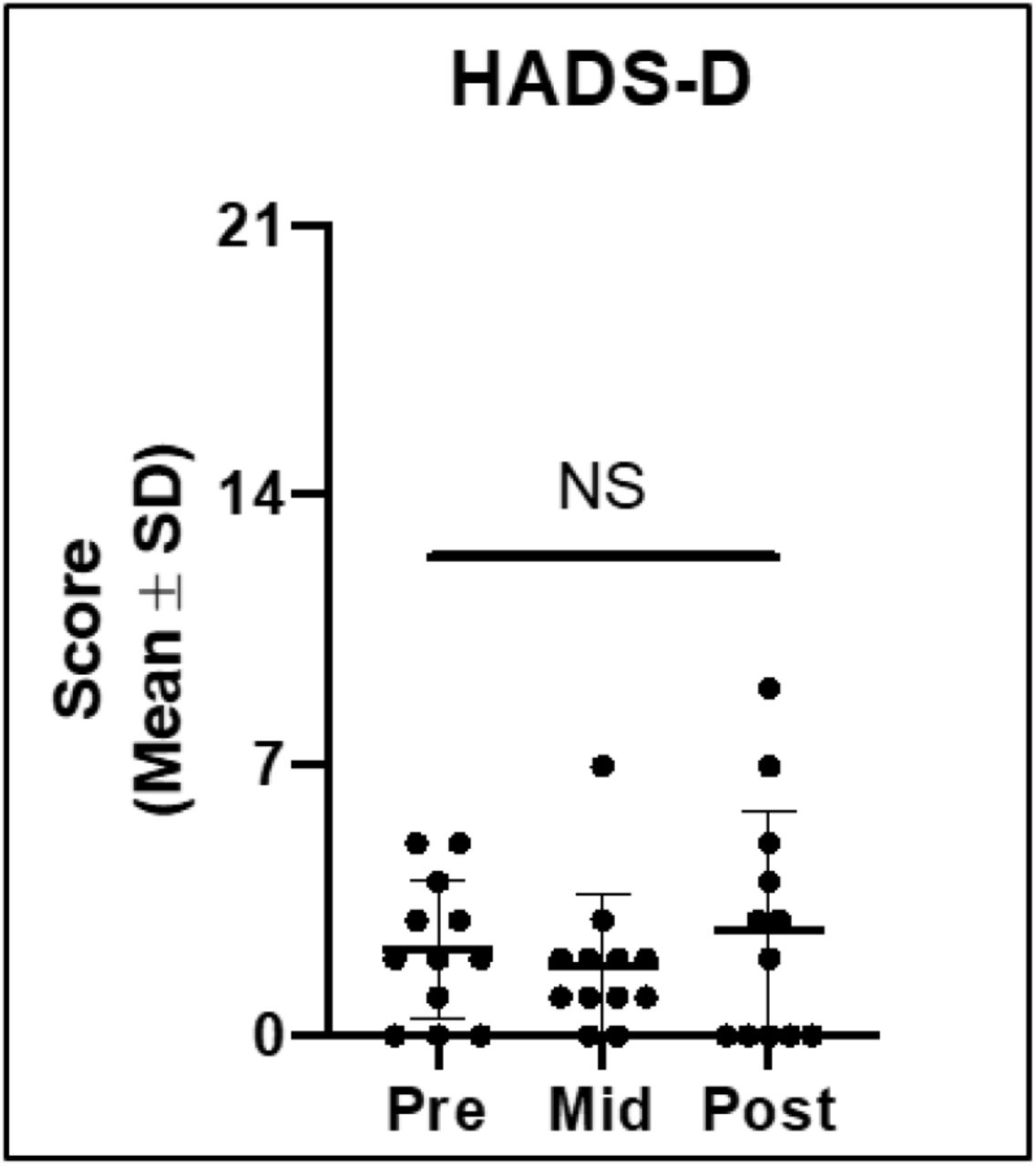
There was no significant effect of coaching on depression (HADS-D; p>.05), as shown in Figure 4.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
The measured changes from pre- to post coaching and mid- to post-coaching in PSS and HADS-A and HADS-D were not significant.
The qualitative analysis revealed responses in four domains: 1) Affective, 2) Cognitive, 3) Skills and 4) Attributes of the Coaching Experience. Affective responses included gaining perspective, self-awareness and positive feelings on the part of the student. Cognitive responses included goal setting and working through solving problems. Students indicated that the coaching helped them set both personal and professional goals. The Skills responses included developing reflection abilities and critical thinking.
Attributes of the coaching experience included perceiving coaching as a positive, individualized and supportive experience. In the open-ended questions after coaching, students identified strengths and areas for improvement of their coaching experience. Students found their coaching experience would have been improved by meeting more frequently, meeting in person, meeting in a more private location and starting coaching earlier in medical school.
A wide variety of topics were chosen by the students for coaching, including choice of field for residency, residency program attributes and applications, assertiveness skills, delegation skills, work-life balance, self-care and boundaries in healthcare and life, among others. Many expressed that the questions asked by the coach had not been considered previously and facilitated self-reflection in planning for the future.
Examples of these responses are provided below in Table 2.
QUALITATIVE RESPONSES EXAMPLES
When asked about their likelihood of seeking future coaching, 92% (11/12) of respondents reported being likely to seek coaching in the future (score > 5) with 75% (9/12) indicating high likelihood (score > 7). The mean likelihood score was 8.3/10 with a median score of 8.5/10 and a range of 5.
Discussion
Our data reveal that coaching appears to have positive effects on stress reduction and anxiety reduction after four of the eight sessions (mid-point in the experience). Our data match the findings found in the Fried and Irwin study in that the mid- to post-results were not significant. (Fried and Irwin, 2016). The onset of COVID 19 restrictions that occurred midway through the coaching sessions required a change to virtual format for all students, which may have influenced the effects measured at the end of the sessions. The introduction of major changes and stresses in the lives of these students, resulting from the pandemic, may have had effects on our data and results. The lack of significant change from mid- to post coaching in our measures might indicate the effects of COVID 19 restrictions or may indicate that four sessions are optimal for achieving the changes we measured. The depression measures were not affected by the coaching, which is not surprising given that coaching is not intended as an intervention for depression.
Student responses revealed meaningful effects on their affective, cognitive and skill domains, as well as positive personal experiences from coaching. The qualitative themes we found echo those of the Fried and Irwin study, which were managing stress, self-awareness, appreciating different perspectives and self-reliance. (Fried and Irwin, 2016). A recent study of coaching with practicing physicians revealed that coaching reduced emotional exhaustion and symptoms of burnout, thus improving the quality of life and resilience for those physicians. (Dyrbye et al,2019) The range of topics chosen by students for coaching highlights the broadness of coaching as resource for these students. Coaching has potential for providing medical students with a positive experience and support to navigate the stresses and anxiety inherent in the medical school journey and beyond.
The limitations of this study that compromise its generalizability are the small sample size, the lack of a control group, limited demographic data collected, the lack of reliability and validity data for the Readiness Assessment tool and the students coming from one specific program and institution. The provision of coaching by a single coach in this study may be seen as a strength, such as consistency of skill, or limitation, due to being an unrealistic expectation in large-scale implementation of coaching. Future study with more students in different programs at different institutions, inclusion of a control group and more demographic data will add more evidence about the effects of coaching with medical students.
Conclusions
Coaching holds promise as an intervention that could be offered to medical students to reduce stress and anxiety, as well as provide support for affective, cognitive and skills development, preparing them for their professional futures.
Data Availability
Data is available from the corresponding author. There are no external datasets
Declarations
Ethics approval and consent to participate
The Duke University Health System Institutional Review Board for Clinical Investigations has conducted a review of this study and declared it to be Exempt from further review in September, 2019 (Protocol ID: Pro00103592).
Competing Interests
The authors declare that they have no competing interests
Authors Contributions
ER designed the study, provided the intervention, drafted and revised the manuscript, provided final approval and agreed to be accountable for all aspects of the work. TF contributed the analysis and interpretation of the data, revised, provided final approval of the manuscript and agreed to be accountable for all aspects of the work. KC assisted with the design of the study, assisted with data collection, analysis and interpretation, revised, provided final approval of the manuscript and agreed to be accountable for all aspects of the work.
Acknowledgements
The authors express gratitude to Sackeena Gordon-Jones for allowing them to adapt and utilize the Readiness Assessment for Coaching in this study. Additionally, the authors wish to express appreciation to Marilyn H. Oermann, PhD, RN, ANEF, FAAN, Duke School of Nursing, for her review of this manuscript and Duke AHEAD for funding and the Grant Committee for encouraging this project.
REFERENCES



