
Abstract
Objective Pregnancy is a risk factor for severe Covid-19. Looking for safe vaccines that evoke protective maternal and fetal antibody response is important.
Methods We searched from registries (ClinicalTrials.gov, the WHO Clinical Trial Registry, and the EU Clinical Trial Registry) and databases (MEDLINE, ScienceDirect, Cochrane Library, Proquest, and Springer) up until June 20, 2021. Articles were selected based on inclusion and exclusion criteria after duplicates were removed. Infection rate, maternal antibody response, placental antibody transfer, and adverse events were described. This systematic review was performed with quality assessment and semi-quantitative synthesis according to PRISMA guidelines.
Results Twelve observational studies with a total of 40.509 pregnant women included. The mRNA based vaccines (Pfizer-BioNTech and Moderna) can prevent future SARS-CoV-2 infections (p=0.0004). Both vaccines did not affect pregnancy, delivery, and neonatal outcomes. The most commonly encountered adverse reactions are injection-site pain, fatigue, and headache but only transient. Antibody responses were rapid after the prime dose of vaccines. After booster, antibody responses were higher and associated with better placental antibody transfer. Longer intervals between first vaccination dose and delivery were also associated with higher antibody fetal IgG and better antibody transfer ratio.
Conclusions The Pfizer-BioNTech and Moderna vaccines are efficacious for preventing future SARS-CoV-2 infections. These vaccines can be considered as a safe option for pregnancy and their fetus. Two doses of vaccines were recommended for more robust maternal and fetal antibody responses. Longer latency was associated with higher fetal antibody responses.
Systematic Review Registration PROSPERO (CRD42021261684)
INTRODUCTION
The impact of coronavirus disease 2019 (Covid-19) on pregnancy remains unclear due to insufficient information, while most available studies have evaluated the impact of the disease only in the general population. The risk of severe Covid-19 in pregnancy appears to be no greater than for the general population; pregnant women are at a higher risk for acquiring viral respiratory infections and severe pneumonia due to the unique physiological changes in their immune and cardiopulmonary systems.1,2 Although most pregnant women had mild to moderate symptoms only, SARS-CoV-2 infection is found more severe in pregnant women than their nonpregnant counterparts, with an increased risk of hospital admission, intensive care unit stay, and death.3
Despite their higher risk of SARS-CoV-2 infection, pregnant and lactating women were not included in any initial Covid-19 vaccine trials, resulting in data scarcity to guide vaccine decision making in these populations.4 A prior study revealed that most pregnant women with Covid-19 admitted to the hospital were asymptomatic, which allows these undetected patients to transmit the virus to others.5,6 This finding shows that efforts to prevent SARS-CoV-2 infection, one of them by vaccination, are critical for investigation on this population.
To facilitate comprehending the Covid-19 vaccine in pregnancy, we performed a systematic review to critically evaluate and summarize the latest evidence of Covid-19 vaccination regarding the efficacy, immunogenicity, and safety profile in the pregnant population.
METHODS
This systematic review adhered to PRISMA (Preferred Reporting Items for Systematic Review and Meta-Analysis) 2020 guidelines7 and has been previously registered in the PROSPERO database (CRD42021261684).
Eligibility criteria
We accepted any study (retrospective, prospective, cohort, randomized controlled trials (RCT), case series, case control, cross-sectional, crossover) to be included in the review. The authors screened the title and abstract of independently for eligible studies based on the following criteria: (1) pregnant women; (2) adult (≥18 years) female study population; (3) the study involved Covid-19 vaccine of interest; (4) the study compared the intervention group with control (non-pregnant women, unvaccinated, or none); (5) eligible studies should have reported at least one of our outcomes of interest; (6) English language. Our primary outcomes included infection rate, maternal titer antibody, local and systemic adverse events. Our secondary outcomes included neonatal outcome, cord blood titer antibody, and placental transfer ratio. We excluded review articles, irrelevant, non-human studies, and duplications.
Search strategy and selection of studies
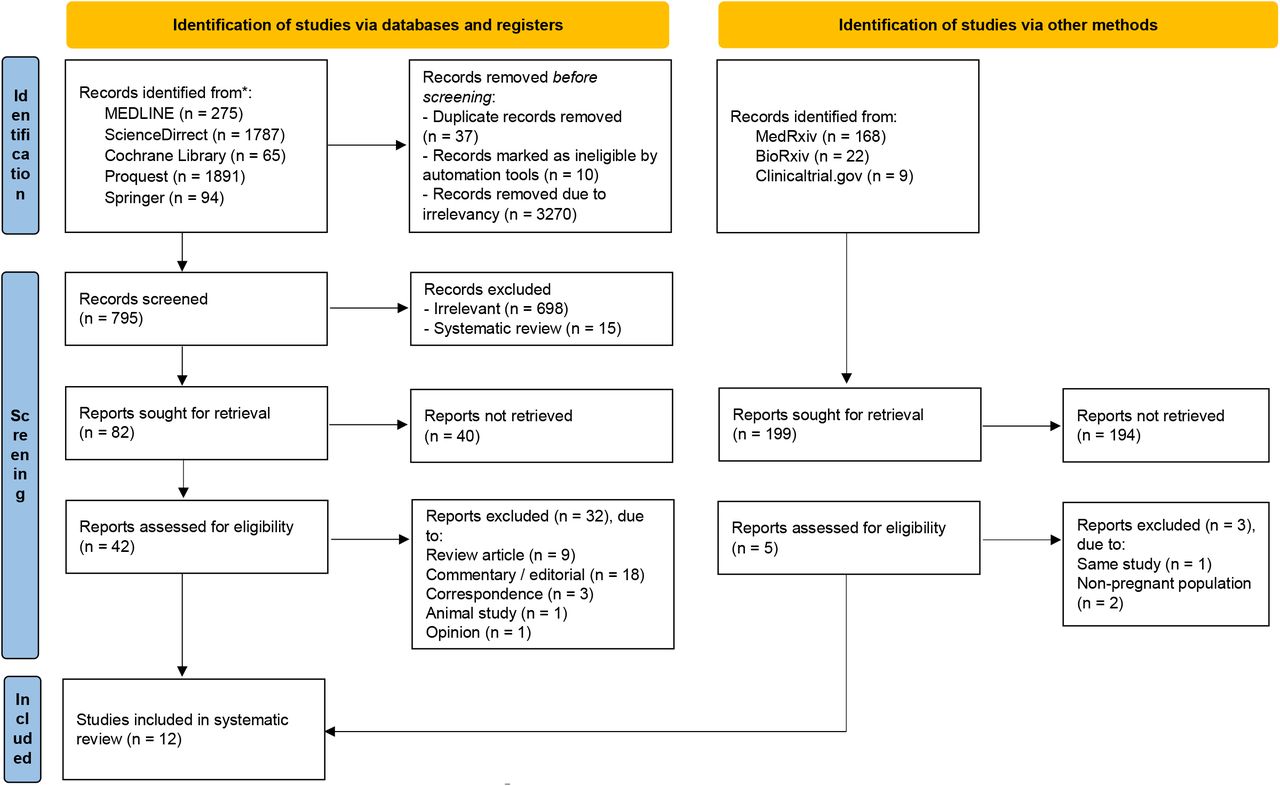
The authors comprehensively conducted keyword searching of articles published in trial registries (ClinicalTrials.gov, the WHO Clinical Trial Registry, and the EU Clinical Trial Registry) and databases (MEDLINE, ScienceDirect, Cochrane Library, Proquest, and Springer) up until June 20, 2021. Our research is limited to studies involving humans with no language restrictions. Manual search, including in BioRxiv and MedRxiv, and the bibliographical search were also conducted to obtain additional evidence. The following keywords were used: “((SARS-CoV-2) OR (COVID-19)) AND ((pregnancy) OR (pregnant)) AND ((vaccine) OR (vaccination))”. The search strategies are available in Supplementary Materials. We exported all studies retrieved from the electronic searches into Mendeley reference manager for removing duplication and screening. The two review authors (NRP and IAW) independently screened the title and abstract of the articles to identify potentially eligible studies and subsequently screened the full texts independently. Any disagreements between the two review authors were resolved by discussion until reaching consensus. Excluded studies were described in the PRISMA flow diagram alongside their reasons for exclusion (Figure 1).
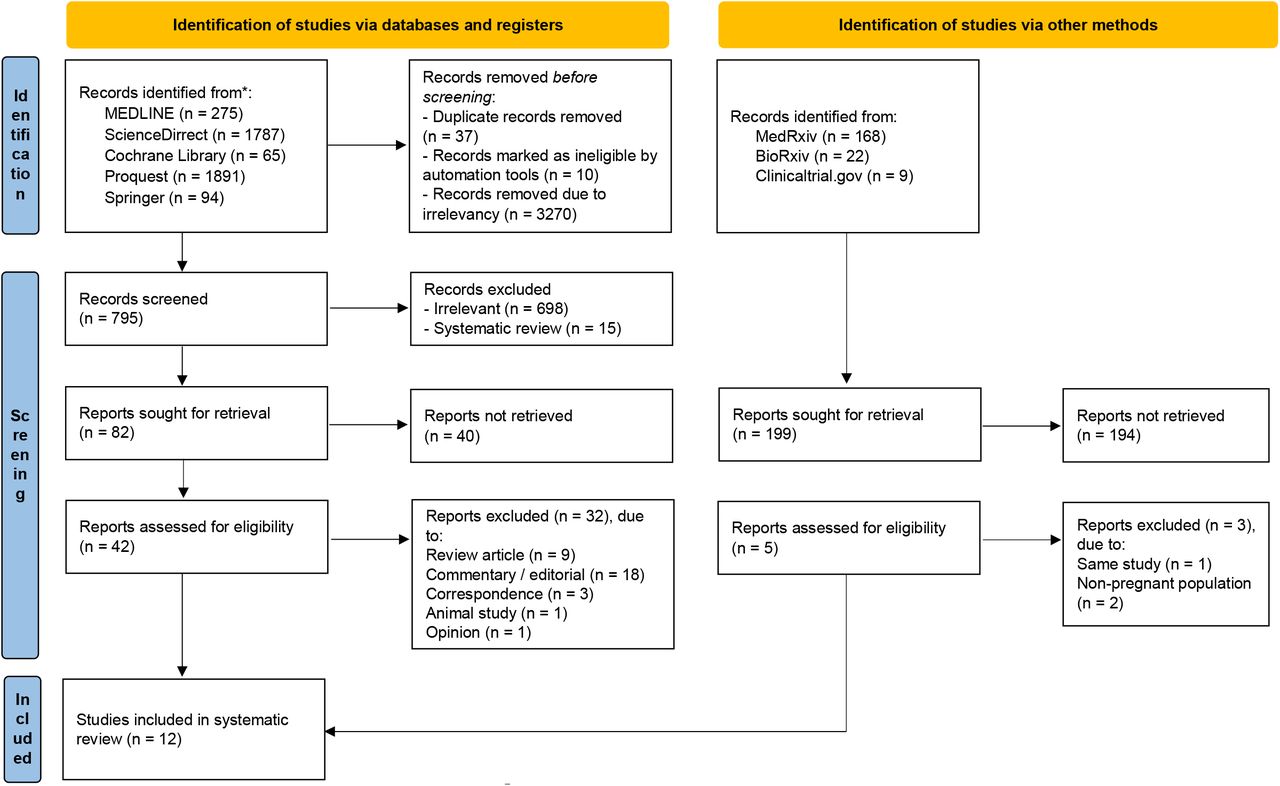
PRISMA flow diagram of study selection process7
Data extraction
The review authors (NRP, IAW, and DSB) independently extracted relevant data using structured and standardized form from each selected study. The following information was extracted: first author’s name and publication year, study design, country, sample size, gestational age at first vaccine, sample size, age, sample collection, vaccine type, and outcomes (infection rate, maternal titer antibody, cord blood titer antibody, placental transfer ratio and local and systemic adverse events). Any disagreements between the review authors were consulted with the expert and resolved by discussion until reaching consensus.
Quality assessment
Two review authors (IAW and DSB) independently assessed the risk of bias from each included studies using Newcastle-Ottawa Scale (NOS) assessment tool for cohort studies and Joanna Briggs Institute (JBI) critical appraisal checklist for case report, case series, and cross-sectional studies.8,9 Newcastle-Ottawa Scale contains eight items within three domains, including patient selection, comparability, and outcomes. A study with scores 7-9, 4-6, and 0-3 were considered to be high, moderate, and low-quality, respectively. Any discrepancies were resolved by discussion until reaching consensus.
Statistical analysis
Due to important differences in comparison of each study and various outcome measures, we could not generate meta-analyses of the included studies but rather we performed narratively synthesized the evidence using Synthesis Without Meta-analysis (SWiM) reporting guideline (intended to complement the PRISMA guidelines in these cases).
RESULTS
Study selection
The search strategy yielded 4112 and 199 records, respectively, from database searching and additional searching, in medRxiv, bioRxiv, and clinicaltrial.gov. After screening the titles and abstracts, 47 potentially eligible articles were reviewed. After the full-text assessment, twelve studies were included in this systematic review. The process of study selection in this review is described in the PRISMA flow diagram (Figure 1), along with the reason for exclusion.
Quality assessment
Eight cohort studies were assessed using the NOS assessment tool and considered as high quality since all of the studies scored 7-9 (see Table S1 in Supplementary Materials). The quality assessment of case report, case series, and cross-sectional studies using the JBI critical appraisal checklist was summarized in Supplementary Materials (Table S2 – S4).
Study characteristics
There are twelve observational studies with a total of 40.509 pregnant women who received Covid-19 vaccines included in this systematic review. Among these studies, ten studies (six cohort, one cross-sectional, one case series, and two case report) were conducted in the United States of America (USA) while other two cohort studies were carried out in Israel in 2021. The maternal age ranged from 16 to 54 years. All pregnant women reported receiving mRNA vaccine, either Pfizer–BioNTech or Moderna vaccine, except for four pregnant women who received unknown types of vaccine.18 Some studies compared vaccinated pregnant women with unvaccinated pregnant women, either naturally infected or not infected, or vaccinated non-pregnant women. The efficacy outcome was desribed as infection rate, while immunogenicity was described as maternal antibody response, fetal antibody response, and transplacental antibody transfer. Safety outcome was described as the adverse events, maternal outcomes, and neonatal outcomes. Adverse events were divided into local and systemic, local adverse events include injection-site pain and soreness, while systemic adverse events include fatigue, headache, myalgia, chills, fever and nausea.
Characteristics of the included studies
Outcomes of the individual studies
Infection Rate
Among pregnant women who received the Pfizer–BioNTech vaccine, 0.1% (3/2136) of pregnant women experienced Covid-19 infection within 14 days from vaccination and 0.4% (9/2136) after 14 days from vaccination. Additionally, among pregnant women who received Moderna vaccines, 0.4% (7/1822) of pregnant women experienced Covid-19 infection within 14 days from vaccination and 0.2% (3/1822) after 14 days from vaccination.10 Among unvaccinated vs vaccinated pregnant women, vaccination significantly reduced the risk of future infection (p=0.0004) and all infection cases, reported in the trimester I of vaccinated women, occurred prior to the first vaccination dose.19
Maternal antibody response
Vaccination induced IgG and IgM production in 71% (87/122) pregnant women; 16% (19/122) pregnant women produced only IgG whilst 13% (16/122) had neither detectable IgG nor IgM.14 Vaccination provided a rapid immunologic response after the first dose while infection provided a gradual immunologic response. Moreover, administration of the second dose can further increase the IgG level among vaccinated women.11,20 Spike- and RBD-IgG titer rose rapidly after prime dose (p<0.0001 and p<0.01, respectively); and after receiving booster, it became higher than that of the prime dose (p<0.05 and p<0.001, respectively).11
Vaccination elicited IgG responses against S1, S2, and RBD but not N protein. Meanwhile, infection elicited all IgG responses against S1, S2, RBD, and N protein. Among vaccinated pregnant women, S1 IgG and RBD IgG levels were higher (p=0.0009 and p=0.0045, respectively). Yet, S2 IgG and N IgG were higher in infected pregnant women (p=0.016 and p<0.0001, respectively).20 Meanwhile, Gray et al., (2021) reported that Spike IgG titer is higher in vaccination than that of natural infection in pregnant women.11
Maternal SARS-CoV-2 spike protein IgG levels between vaccinated and uninfected unvaccinated pregnant women are 22.8±14.5 AU and 0.04±0.05 AU, respectively (p<0.001). While for the IgM levels are 4.1±13.2 AU and 0.19±0.12 AU, respectively (p=0.001).13 Among pregnant women that received two vaccine doses, anti-spike-protein IgG concentration median is 319 (211-1033) AU/mL and anti-RBD-Specific IgG concentration median is 11150 (6154-17575) AU/mL.17 Meanwhile, in two women that only received one dose of vaccine, the anti-spike-protein IgG concentrations are 50 AU/mL and 52 AU/m; and the anti-RBD-Specific IgG concentrations are 293 AU/mL and 1137 AU/mL.17
Antibody response in pregnant and non-pregnant women was evaluated by Collier et al., (2021).12 The study reported the median of IgG levels between vaccinated and infected pregnant women. The RBD IgG titers were 27601 and 1321, respectively; while the neutralizing antibody titers were 910 and 148, respectively. The median of RBD IgG titers between vaccinated and infected non-pregnant women were 37839 and 771, respectively; while for the Neutralizing antibody were 901 and 193, respectively.12
Antibody transfer
A prospective case series reported that the IgG was detected in 89% (25/28) of cord blood, but none had detectable IgM.18 Moreover, antibody against SARS-CoV-2 RBD and neutralizing antibody was observed in cord blood. On vaccinated women, the maternal vs cord blood RBD IgG was 14953 AU vs 19873 AU, whilst for the neutralizing antibody was 1016 AU vs 324 AU.12 IgG against S protein was also detected in cord blood with concentration of 193 (111-260) AU/mL and its transfer ratio was 0.44 (0.25-0.61). Furthermore, the concentration of IgG against RBD was 3494 (1817-6163) AU/mL and its transfer ratio was 0.34 (0.27-0.56).17
Two different case report studies from mother who received two doses of BNT162b2 vaccine and mother who received one dose of Moderna vaccine, respectively, reported that SARS-CoV-2 specific IgG was detected in maternal blood and cord blood at a titer 1:25.600, while cord blood IgG concentration were detected at level of 1.31 U/mL.15,21
Regarding the number of doses received, antibody was detected in 98.5% (65/67) neonates from whom the mother received two doses of vaccine. From mothers who received only one vaccine dose, only 43.6% (24/55) neonates whose antibody was detected.14 Having received the second vaccine dose was positively correlated with infant IgG level (β=19.0 (95%CI 7.1-30.8)).18 In addition to doses, the interval from vaccination to delivery was correlated with IgG transfer ratio and infant IgG level. Increased latency from vaccination to delivery was positively correlated with IgG transfer ratio (β=0.2 (95%CI 0.1-0.2)) and infant IgG level (β=2.9 (95%CI 0.7-5.1)).18 For maternal-fetal IgG response, there was no statistical difference between vaccination and SARS-CoV-2 infection for S1 IgG (p=0.2936), S2 IgG (p=0.4212), RBD IgG (p=0.0702), and N IgG (p=0.7616).20
Local adverse events
Among pregnant women, injection-site pain is the most common adverse event in both the Pfizer– BioNTech and Moderna vaccines. Following the Pfizer–BioNTech vaccination, as many as 84% (7602/9052) in the first dose and 89% (5886/6638) in the second dose experienced injection-site pain. While for the Moderna vaccine, 93% (7360/7930) and 96% (5388/5635) following the first and the second dose, respectively, experienced injection-site pain.10 It was also reported 88% (73/84) pregnant women experienced injection-site soreness following the first dose vaccination and 57% (44/84) following the second dose. Additionally, 75% (12/75) non-pregnant women experienced injection-site soreness after the first and the second dose of vaccine.11
Between pregnant and non-pregnant women, sore arms or pain were observed in 97% (37/38) pregnant women and 90% (894/991) non-pregnant women following Pfizer–BioNTech and Moderna vaccination.16
Systemic adverse event
Systemic adverse events between two doses of Pfizer–BioNTech and Moderna were reported. Following Pfizer–BioNTech the first vs the second dose of vaccine, six most experienced systemic adverse events were fatigue (27% (2406/9052) vs 64% (4231/6638)); headache (17% (1497/9052) vs 47% (3138/6638)), myalgia (9% (795/9052) vs 44% (2916/6638)), chills (3% (254/9052) vs 26% (1747/6638)), fever (3% (256/9052) vs 25% (1648/6638)), and nausea (5% (492/9052) vs 20% (1356/6638)). For the Moderna vaccine, fatigue (33% (2616/7930) vs 81% (4541/5635)), headache (20% (1581/7930) vs 65% (3662/5635)), myalgia (15% (1167/7930) vs 66% (3722/5635)), chills (6% (442/7930) vs 49% (2755/5635)), fever (6% (453/7930) vs 46% (2594/5635)), and nausea (8% (638/7930) vs 34% (1909/5635)). Numerically, the incidence of each event is higher in the second dose. Moreover, the Moderna vaccine had more systemic adverse events than that of the Pfizer– BioNTech vaccine.10 Seizure was reported in a woman who received mRNA vaccine (p=0.0369), but it was known that the patient has a history of seizure disorder and the anticonvulsant level in the blood was borderline low.16
Maternal outcomes
Maternal outcomes were described as pregnancy outcomes and delivery outcomes. Compared to unvaccinated pregnancy, vaccination did not significantly affect pregnancy or delivery outcomes. The adverse outcome index between vaccinated and unvaccinated pregnancy was insignificant (p=0.9524). Between these group, there were no statistical difference in pregnancy outcome such as eclampsia/pre-eclampsia (p=1), gestational hypertension (p=0.6038), gestational age (p=0.7028), and thromboembolism incidence (p=1).19 Moreover, the abortion rate was reported at 12.6% (104/827) and 9.4% (60/636) had preterm birth. Statistically, vaccination also did not affect delivery outcomes such as birth trauma (p=1), uterine rupture (p=1), unplanned ICU admission (p=0.1956), quantitative blood loss>1000mL (p=0.4452) or hemorrhage with transfusion (p=0.3531), mode of delivery (p=0.6517), and stillbirth (p=1).19
Neonatal outcomes
As many as 15% (2/13) required NICU admission, 8% (1/13) experienced TTN, and 8% (1/13) required supplemental oxygen or CPAP. Preterm delivery was reported in 8% (1/13) of women.11 Moreover, 0.1% (1/725) were stillbirth, 3.2% (23/724) had small size for gestational age and 2.2% (16/724) had congenital anomalies. No neonatal death was reported.10 On statistical analysis, NICU admission (p=0.5821), 5 minute Apgar <7 (0.7617), hypoxic ischemic encephalopathy (p=1), and low birth weight (p= 0.5321) or very low birth weight (p= 0.2332), did not differ significantly between vaccinated and unvaccinated women.19
DISCUSSION
Main Finding
It has been described that Pfizer-BioNTech and Moderna vaccines were efficacious for preventing future SARS-CoV-2 infection in pregnant women.19 Following Pfizer-BioNTech and Moderna vaccinations, the vast majority of pregnant women will have injection-site pain or soreness.10,11,16 Some most-experienced systemic adverse events were fatigue, headache, chills, myalgia, fever, and nausea.10,16 The incidence of these systemic adverse events were higher after the second dose compared to the first dose.10-12 Numerically, there were more individuals who experienced these systemic adverse events in Moderna vaccine group than that of Pfizer-BioNTech group.10 The adverse events were not statistically differ between pregnant and non pregnant women, except seizure. However, the woman was known to have a history of seizure disorder and the anticonvulsant level was measured borderline-low.19 Interestingly, the pregnancy, delivery, and neonatal outcomes did not differ between pregnant and non pregnant women.19
Maternal antibody response has been described formed following vaccination.11-15,17,18,20 Through vaccination, antibody response was formed rapidly; while through vaccination it was formed gradually.20 The number of IgG and IgM against SARS-CoV-2 were significantly increased after vaccination. The response was increased after a booster was given.11,13 Although vast majority of pregnant women had IgG seroconversion, IgM seroconversions were observed in a minority of pregnant women.18 After vaccination, IgG against S1, S2 and RBD formed whilst IgG against S1, S2, RBD and N protein formed following natural infections. Moreover, S1- and RBD-IgG were observed higher in vaccinated pregnant women. Meanwhile the S2- and N-IgG were observed higher in naturally infected pregnant women.20 Also, the RBD IgG and neutralizing antibody was higher in vaccinated individuals than that of naturally infected.12
Antibody transfer was also reported.12,14,15,17,18,20,21 Cord blood antibody and maternal antibody levels were about equal.18 Additionally, latency and number of doses were correlated with the antibody transfer strength.14,18 The longer the latency, the better the antibody transfer and the higher the IgG.18 A mother who received two doses of vaccines would have her infant getting higher IgG levels.18 Between infection and vaccination, there was no difference in maternal-fetal IgG response.20
Finding on other studies
A sufficient herd immunity threshold in a population will provide indirect protection for susceptible individuals from infected hosts.22 The threshold varies across different infections.23-25 In Covid-19, it was said that for a vaccine with 100% efficacy and providing life-long protection, we would need 60-75% herd immunity. This required number would be increased if the vaccine efficacy was reduced to 85%; a 75-90% herd immunity would be required.26 Although we described that Pfizer-BioNTech and Moderna vaccines are efficacious to prevent future SARS-CoV-2 infection, whether the efficacy of these vaccines is reduced in pregnancy remains unknown.
This herd immunity threshold may also vary across populations. It depends on some factors--epidemiological factors (e.g., population density and transmission dynamics) and immunological factors (e.g., immune stats of population).22 An approach to achieve this threshold is through mass vaccination campaigns.22 Thus, high vaccination coverage is important for achieving sufficient herd immunity.27,28
On note, not only pregnant individuals but also those who were not pregnant will experience these adverse reactions as well. In Moderna and Pfizer-BioNTech studies where pregnant women and children were excluded, the incidence of systemic adverse events increased after the second dose of vaccine.29,30 Following the Moderna vaccine booster, local pain was experienced by 83.2-89.9% of individuals, followed by fatigue (58.3-65.3%) and headache (46.2-62.8%). Meanwhile, there were 10.0-15.5% who experienced fever. These were generally resolved within 3.1-3.2 days.29 Following the Pfizer-BioNTech vaccine booster, injection-site pain was experienced by 66%-78% individuals, followed by fatigue (51-59%) and headache (39-52%). Meanwhile, fever was experienced by 11-16% of individuals. These adverse events were transient, resolved within 1-2 days.30
Safety is an important concern for Covid-19 vaccination in pregnant women. Based on a survey in 16 countries, pregnant women were less likely to accept vaccines for themselves. Given that a Covid-19 vaccine had 90% efficacy, 73.4% non-pregnant women intended to receive the vaccine while pregnant women were only 52%. The confidence in vaccine safety and effectiveness was one of the predictors for vaccine acceptance.31 However, vaccination safety did not differ among those who are pregnant or not. Moreover, vaccination did not affect pregnancy, delivery, and pregnancy outcomes. On the other hand, some conditions during pregnancy made pregnant women susceptible to severe disease of Covid-19.32
During pregnancy, the upper respiratory tract was swollen and lung expansion was restricted. It makes pregnant women more susceptible to respiratory pathogens.33 Moreover, pro-inflammatory phase was present in the first trimester, for the implantation of the embryo and placenta, and third trimester, to prepare for the initiation of labor.34 In fact, severe Covid-19 is associated with cytokine storms.35 The pro-inflammatory phase during the first and third trimester of pregnancy, made them to be more prone to severe Covid-19.36
Individuals with significant medical comorbidities, the elderly, and pregnant women are highly vulnerable to Covid-19 infection.37,38 Although newborns and infants are less likely to get SARS-CoV-2 infections, they are more prone to severe SARS-CoV-2 infection.37,39,40 Passive immunity in neonates may be potentially protective. Administration of booster doses can enhance antibody transfer which may provide a better immunity in neonates. However, this fetal passive immunity may be altered due to placental sieving41, depending on the gestational age at first vaccine dose or infection. The longer latency interval from first dose of vaccination to delivery should be required for better antibody transfer.18
In contrast to natural viral infection such as in Zika dan DENV,42,43 antibody transfer observed following other vaccinations such as in pertussis and Influenza vaccines.44,45,46 Timeframe following natural SARS-CoV-2 infection may affect antibody transfer. An earlier Covid-19 infection may provide a better placental antibody transfer.20 Additionally, poor placental antibody transfer was exclusively observed only in the third trimester of pregnancy, even though the maternal antibody response was significantly higher.47 Natural infection may result in higher morbidity and mortality48, so vaccination should be the better option for the dyads.
Many SARS-CoV-2 mutations had altered Covid-19 transmissibility and, probably, severity.49,50,51 Moreover, these mutations can also impact a treatment efficacy, especially monoclonal antibody treatments due to immune escape.52,53,54 It had been reported, compared to the wild type of USA-WA1/2020 SARS-CoV-2, the binding strength of neutralizing antibodies formed after Pfizer and Moderna vaccination was observed 3.5- and 6-fold lower for B.1.1.7 and B.1351, respectively.12 Antibody resistance against B.1.1.7 and B.1351 was also reported by another study.55 In addition, in UK, it also was reported that B.1.617.2 had overtaken B.1.1.7. variants.56 Maximizing the second dose vaccine coverage may provide a stronger protection against this variant.57 However, we still need to know whether we would need a new vaccine or booster dose since there are evidence of reduced efficacy of currently available vaccine for these strains. This problem should be taken more seriously, and other public health measures are necessary as an effort to end this pandemic.58
Strength and limitation
To the best of our knowledge, this systematic review used the most recent evidence to describe the efficacy, safety and immunogenicity of Covid-19 mRNA vaccine in pregnancy. All studies included in this review were assessed as high quality studies. However, studies are all observational studies due to no RCTs reports of Covid-19 vaccination for pregnant women yet currently available. These studies reported only from mRNA type vaccines. Moreover, all available studies that were included were only from the United States and Israel.
CONCLUSION
In this study, mRNA vaccines, especially Pfizer-BioNTech and Moderna vaccines, are efficacious for preventing future SARS-CoV-2 infections. These vaccines can induce antibody responses for pregnant women and their fetus. Pregnant women should be given two doses of vaccine for more robust maternal and fetal antibody response. Longer latency was associated with more robust fetal antibody response. Almost all pregnant women who received vaccination, either in the first or second dose, will experience injection-site pain. Furthermore, the second dose of vaccine will produce more systemic adverse events than that of the first dose and administration of Moderna vaccine was observed to have a more frequent systemic adverse events. Biologically speaking, we may conclude that for a short term, vaccination did not affect pregnancy, delivery, or neonatal outcomes.
REFERENCES




{kind=link}
Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos