
ABSTRACT
Background SARS-CoV-2 variants of concern (VOC) are more transmissible and have the potential for increased disease severity and decreased vaccine effectiveness. We sought to estimate the effectiveness of BNT162b2 (Pfizer-BioNTech), mRNA-1273 (Moderna), and ChAdOx1 (AstraZeneca) vaccines against symptomatic SARS-CoV-2 infection and severe outcomes (COVID-19 hospitalization or death) caused by the Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2) VOCs during December 2020 to May 2021.
Methods We conducted a test-negative design study using linked population-wide vaccination, laboratory testing, and health administrative databases in Ontario, Canada.
Findings Against symptomatic infection caused by Alpha, vaccine effectiveness with partial vaccination (≥14 days after dose 1) was higher for mRNA-1273 (83%) than BNT162b2 (66%) and ChAdOx1 (64%), and full vaccination (≥7 days after dose 2) increased vaccine effectiveness for BNT162b2 (89%) and mRNA-1273 (92%). Protection against symptomatic infection caused by Beta/Gamma was also higher with partial vaccination for mRNA-1273 (77%) than BNT162b2 (60%) and ChAdOx1 (48%), and full vaccination increased effectiveness for BNT162b2 (84%). Against Delta, vaccine effectiveness after partial vaccination tended to be lower compared to Alpha for mRNA-1273 (72% vs. 83%) and BNT162b2 (56% vs. 66%), but was similar to Alpha for ChAdOx1 (67% vs. 64%). Full vaccination with BNT162b2 increased protection against Delta (87%) to levels comparable to Alpha (89%) and Beta/Gamma (84%). Vaccine effectiveness against hospitalization or death caused by all VOCs was generally higher than for symptomatic infection after partial vaccination for all three vaccines.
Interpretation Our findings suggest that even a single dose of these 3 vaccines provide substantial protection against these 4 VOCs, and 2 doses likely provide higher protection. Jurisdictions facing vaccine supply constraints might consider delaying second doses to more rapidly achieve greater overall population protection.
INTRODUCTION
SARS-CoV-2 variants of concern (VOC) are more transmissible and have the potential for increased disease severity and decreased vaccine effectiveness.1 Few studies have reported the effectiveness of COVID-19 vaccines against infection or severe outcomes caused by VOCs.2-6 Four VOCs, Alpha (B.1.1.7), Beta (B.1.351), Gamma (P.1), and Delta (B.1.617.2), have been circulating at various times in Ontario, Canada, where a delayed second-dose strategy was implemented due to vaccine supply constraints.
We aimed to estimate the effectiveness of BNT162b2 (Pfizer-BioNTech), mRNA-1273 (Moderna), and ChAdOx1 (AstraZeneca) vaccines against symptomatic SARS-CoV-2 infection and severe outcomes (COVID-19 hospitalization or death) caused by Alpha, Beta, Gamma, and Delta between December 2020 and May 2021.
METHODS
We employed a test-negative design to compare vaccination status between test-positive individuals (with symptomatic infection or a severe outcome) and symptomatic but test-negative individuals.7 We included community-dwelling Ontarians aged ≥16 years who had symptoms consistent with or a severe outcome attributable to COVID-19, and who were tested for SARS-CoV-2 between 14 December 2020 and 30 May 2021. We excluded individuals who tested positive for SARS-CoV-2 prior to their selected index date.
Data sources and definitions
Comprehensive province-wide datasets for SARS-CoV-2 laboratory testing, SARS-CoV-2 public health surveillance, COVID-19 vaccination, and healthcare system use were linked using unique encoded identifiers and analyzed at ICES (formerly the Institute for Clinical Evaluative Sciences). Details have been described previously.8
Vaccination status
We obtained information regarding COVID-19 vaccination status, including vaccine product, date of administration, and dose number, from COVaxON, a centralized COVID-19 vaccine information system in Ontario.
COVID-19 testing and identification of variants
Data on laboratory-confirmed SARS-CoV-2 infection detected by real-time reverse transcription polymerase chain reaction (RT-PCR) were collected from the Ontario Laboratories Information System (OLIS) for both individuals who tested positive (treated as cases) and individuals who tested negative (treated as controls). We used specimen collection date as the index date because symptom onset date was inconsistently available in OLIS. We used the first positive test for cases, and a randomly selected negative test for controls with multiple negative tests during the study period.
We obtained information on variants from the Public Health Case and Contact Management system (CCM), which contains results of screening tests for mutations and whole genome sequencing to assign SARS-CoV-2 lineage or variant of concern (VOC). All RT-PCR positive specimens with cycle threshold values ≤35 were screened for N501Y and E484K mutations by multiplex RT-PCR (VOC PCR).9
At the beginning of 2021, whole genome sequencing was performed on specimens that had specific mutations detected by VOC PCR to confirm they were indeed VOCs. From 3 February 2021, specimens with the N501Y mutation, and from 22 March 2021, specimens with the E484K mutation, and cycle threshold values ≤30 were sequenced for surveillance purposes.9,10 A subset of RT-PCR-positive specimens without any mutations detected by VOC PCR were also selected for sequencing for surveillance purposes.9 Additionally, VOC PCR testing and sequencing were performed for specific indications such as recent travellers, partially or fully vaccinated individuals, cases of suspected reinfection, or to support investigations of outbreaks and potential super-spreading events.11 Ontario started sequencing 10% and 50% of VOC PCR-screened specimens on 2 May 2021 and 30 May 2021, respectively.
In addition to those classified into SARS-CoV-2 lineages based on sequencing, we considered specimens positive for the N501Y mutation and negative for the E484K mutation (N501Y+/E484K-) as Alpha. Both Beta and Gamma have N501Y and E484K mutations, but because insufficient numbers of specimens were sequenced to distinguish these 2 VOCs so that vaccine effectiveness could be estimated for Beta and Gamma separately, we combined the N501Y+/E484K+ specimens as well as those identified through sequencing to be Beta and Gamma into a combined Beta/Gamma group. We classified specimens collected after 1 April 2021 that were negative for both N501Y and E484K (N501Y-/E484K-) mutations as either probable, possible, or unlikely Delta cases based on the predicted probability that it was Delta. To do this, we created a logistic regression model of the probability a N501Y-/E484K-case was Delta based on the date of specimen collection and the forward sortation area (geographical unit based on the first three characters of the postal code) ranked by the cumulative incidence of laboratory-confirmed SARS-CoV-2 cases between 23 January 2020 and 28 March 2021 and grouped into deciles.12 For each decile, we examined the trajectories of the daily counts of N501Y-/E484K-specimens between 1 April 2021 and 30 May 2021 to estimate the predicted probability that a N501Y-/E484K-specimen represented Delta. We classified specimens with >75% probability of being a Delta case to be ‘probable Delta’ cases, those with 25-75% probability to be ‘possible Delta’ cases, and those with <25% probability to be ‘unlikely Delta’ cases. Our approach correlates well with sequencing results (n=538) for the province indicating a rapid increase in the proportion of N501Y-/E484K-cases being identified as Delta from mid-March to mid-May 2021.13 We grouped the probable Delta cases with those identified through sequencing. We classified specimens with no lineage information and N501Y-/E484K-specimens collected prior to 1 April 2021 as non-VOC SARS-CoV-2. We also grouped the ‘unlikely Delta’ cases with the non-VOC specimens. We excluded N501Y-/E484K+ cases from our analyses.
Outcomes
For vaccine effectiveness against symptomatic infection, individuals who were symptomatic and tested positive for SARS-CoV-2 in OLIS were considered as cases. For severe outcomes, test-positive individuals who had a hospitalization or death up to 13 June 2021 (regardless of the presence of any symptoms recorded at the time of RT-PCR testing) were identified from CCM and considered as cases. Individuals who were symptomatic but only had tests negative for SARS-CoV-2 in OLIS were considered as controls for both outcomes. However, for severe outcomes, we excluded symptomatic test-negative individuals who later tested positive between 31 May 2021 and 13 June 2021.
Covariates
We obtained information on the following covariates from administrative databases: age and sex from the Ontario Registered Persons Database (RPDB); postal code and Public Health Unit of residence from the RPDB and Statistics Canada Postal Code Conversion File Plus (version 7B); the number of SARS-CoV-2 RT-PCR tests for each individual during the 3 months prior to 14 December (a proxy for individuals who are at increased risk of exposure to SARS-CoV-2 infection and undergo frequent testing), and biweekly (weekly for Delta) period of RT-PCR test to account for the temporal viral activity and regional vaccine roll-out created using testing information from OLIS; comorbidities14 associated with increased risk of severe COVID-19 identified from various databases using validated algorithms and commonly used diagnostic codes and algorithms described previously,15 including Expanded Diagnostic Clusters and Special Population Markers from the Johns Hopkins ACG System (version 10)16; influenza vaccination status during the 2019/2020 and/or 2020/2021 influenza season (a proxy for health behaviours) determined from physician and pharmacist billing claims in the Ontario Health Insurance Plan and Ontario Drug Benefit databases, respectively; and neighbourhood-level information on median household income, proportion of the working population employed as non-health essential workers, average number of persons per dwelling, and proportion of the population who self-identify as a visible minority obtained from 2016 Census data. Details regarding these covariates are provided in Supplementary Table 1.8
Statistical analyses
We used multivariable logistic regression models to estimate the odds ratio comparing the odds of vaccination in test-positive cases with the odds of vaccination among test-negative controls, adjusting for the aforementioned covariates that are associated with COVID-19 and vaccine uptake.14,17,18 We calculated vaccine effectiveness using the following formula: Vaccine effectiveness = 1 – (odds ratio) x 100%.
We estimated vaccine effectiveness against SARS-CoV-2 infection and severe COVID-19 outcomes (hospitalization or death) caused by non-VOC SARS-CoV-2, Alpha, Beta/Gamma, and Delta separately by vaccine product (BNT162b2, mRNA-1273, and ChAdOx1) and number of doses received. For individuals who had received only 1 dose (i.e., partial vaccination) by the index date, we calculated vaccine effectiveness ≥14 days after the first dose. For individuals who had received 2 doses (i.e., full vaccination), we calculated vaccine effectiveness ≥7 days after the second dose. As a sensitivity analysis, and to facilitate comparisons with other studies, we also estimated vaccine effectiveness ≥21 days after the first dose for partial vaccination and ≥14 days after the second dose for full vaccination.
When estimating vaccine effectiveness against Beta/Gamma and Delta, we restricted both test-positive cases and test-negative controls to those who were tested on/after the dates of initial confirmation of these variants in Ontario (11 January 2021 for Beta/Gamma; 11 April 2021 for Delta). Furthermore, since the primary periods of circulation for non-VOC SARS-CoV-2 and VOCs varied relative to the vaccination campaign (i.e., more non-VOC SARS-CoV-2 circulated earlier in the campaign when fewer individuals were vaccinated, whereas Delta circulated later when more were vaccinated), we conducted a sensitivity analysis restricted to individuals who were tested between 5 April 2021 and 30 May 2021 when non-VOC SARS-CoV-2 and VOCs were concurrently circulating, thereby accounting for differences in vaccine availability and coverage over time.
Lastly, we estimated vaccine effectiveness stratified by age group (<60 years and ≥60 years). All analyses were conducted using SAS Version 9.4 (SAS Institute Inc., Cary, NC). All tests were two-sided and used p<0.05 as the level of statistical significance. We did not report estimates of vaccine effectiveness when 95% confidence intervals [CIs] were extremely imprecise (i.e., ranging between a very large negative number and nearly 100) or when vaccine effectiveness was estimated as 100% based on zero vaccinated test-positive cases and the 95% CIs were essentially infinite.
RESULTS
Over the study period, we identified 421,073 symptomatic community-dwelling individuals who were tested for SARS-CoV-2, with 28,705 (6.8%) positive for non-VOC SARS-CoV-2 and 40,828 (9.7%) positive for a VOC (Table 1). Cases of Delta were younger, more likely to be male, more likely to reside in Peel Region (a region west and northwest of Toronto that is characterized by high proportions of essential workers and visible minorities and experienced the highest incidence of SARS-CoV-2 infections during the study period), more likely to occur later in the study period, more likely to have had no previous SARS-CoV-2 tests, less likely to have any comorbidities, and more likely to reside in neighbourhoods with lower household income, crowded households, and greater proportions of essential workers and visible minorities than cases of other VOCs and non-VOC SARS-CoV-2 infections, as well as test-negative controls.
We identified 14,168 individuals with a COVID-19 hospitalization or death (Table 2). We observed largely the same patterns between individuals with severe outcomes caused by Delta versus those caused by other VOCs and non-VOC SARS-CoV-2.
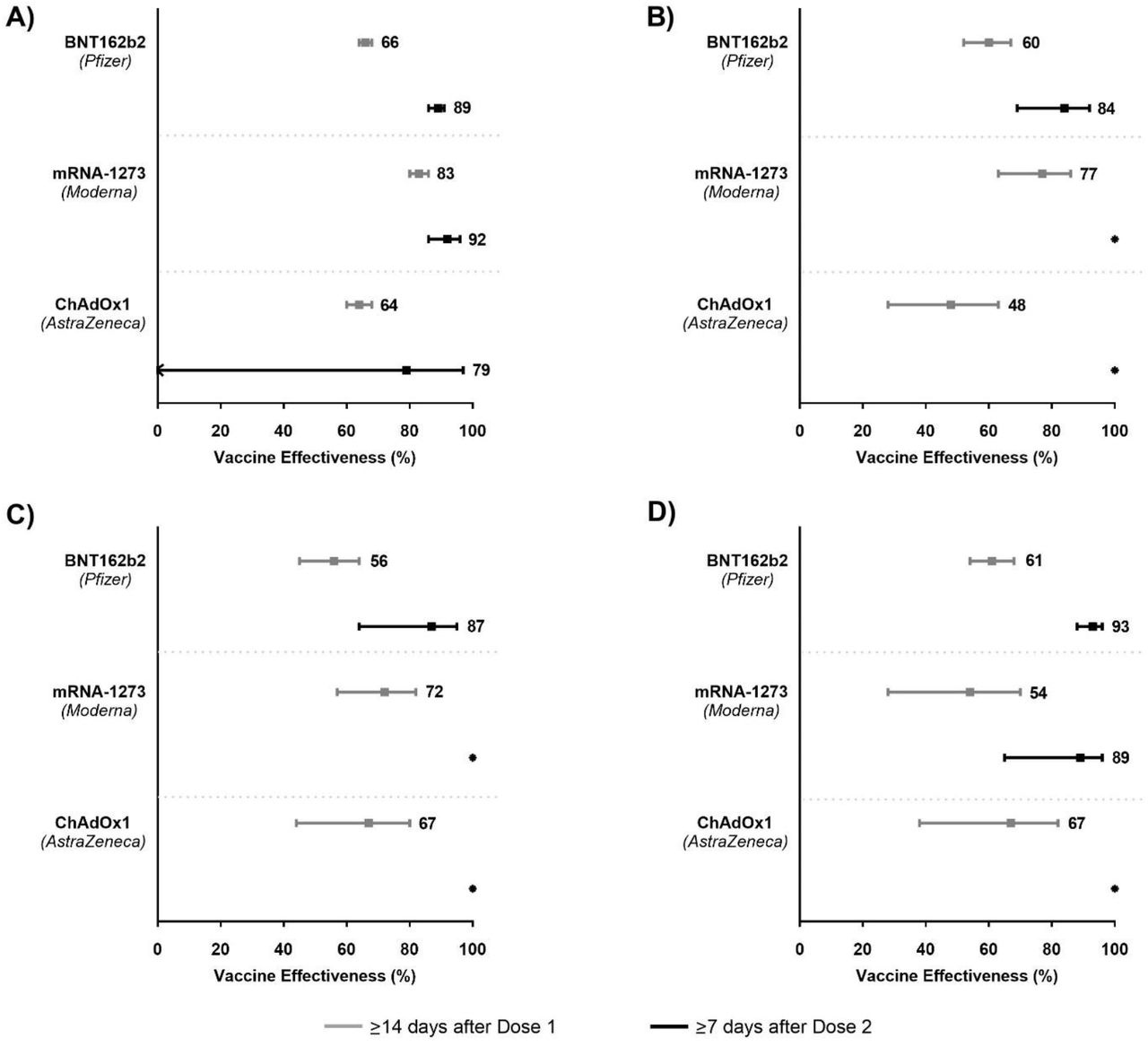
Against symptomatic infection caused by Alpha, vaccine effectiveness with partial vaccination (≥14 days after dose 1) was higher for mRNA-1273 (83%; 95% CI, 80–86%) than BNT162b2 (66%; 95% CI, 64–68%) and ChAdOx1 (64%; 95% CI, 60–68%) (Figure 1A). Full vaccination (≥7 days after dose 2) increased vaccine effectiveness for mRNA-1273 (92%; 95% CI, 86–96%) and BNT162b2 (89%; 95% CI, 86–91%) against Alpha, but could not be reliably estimated for ChAdOx1 due to a very low number of symptomatic test-positive individuals in those vaccinated with ChAdOx1 (Supplementary Table 2). Protection against symptomatic infection caused by Beta/Gamma was higher with partial vaccination for mRNA-1273 (77%; 95% CI, 69–92%) than ChAdOx1 (48%; 95% CI, 28–63%), and was intermediate for BNT162b2 (60%; 95% CI, 52– 67%) (Figure 1B). Full vaccination increased vaccine effectiveness for BNT162b2 (84%; 95% CI, 69–92%) but could not be reliably estimated for mRNA-1273 and ChAdOx1 due to an absence of any vaccinated test-positive cases (Supplementary Table 2). Against Delta, vaccine effectiveness after partial vaccination differed less across the 3 vaccines, ranging from 56% (95% CI, 45–64%) for BNT162b2 to 72% (95% CI, 57–82%) for mRNA-1273 (Figure 1C). Full vaccination increased vaccine effectiveness for BNT162b2 (87%; 95% CI, 64–95%), and again could not be reliably estimated for mRNA-1273 and ChAdOx1 due to zero vaccinated test-positive cases (Supplementary Table 2).
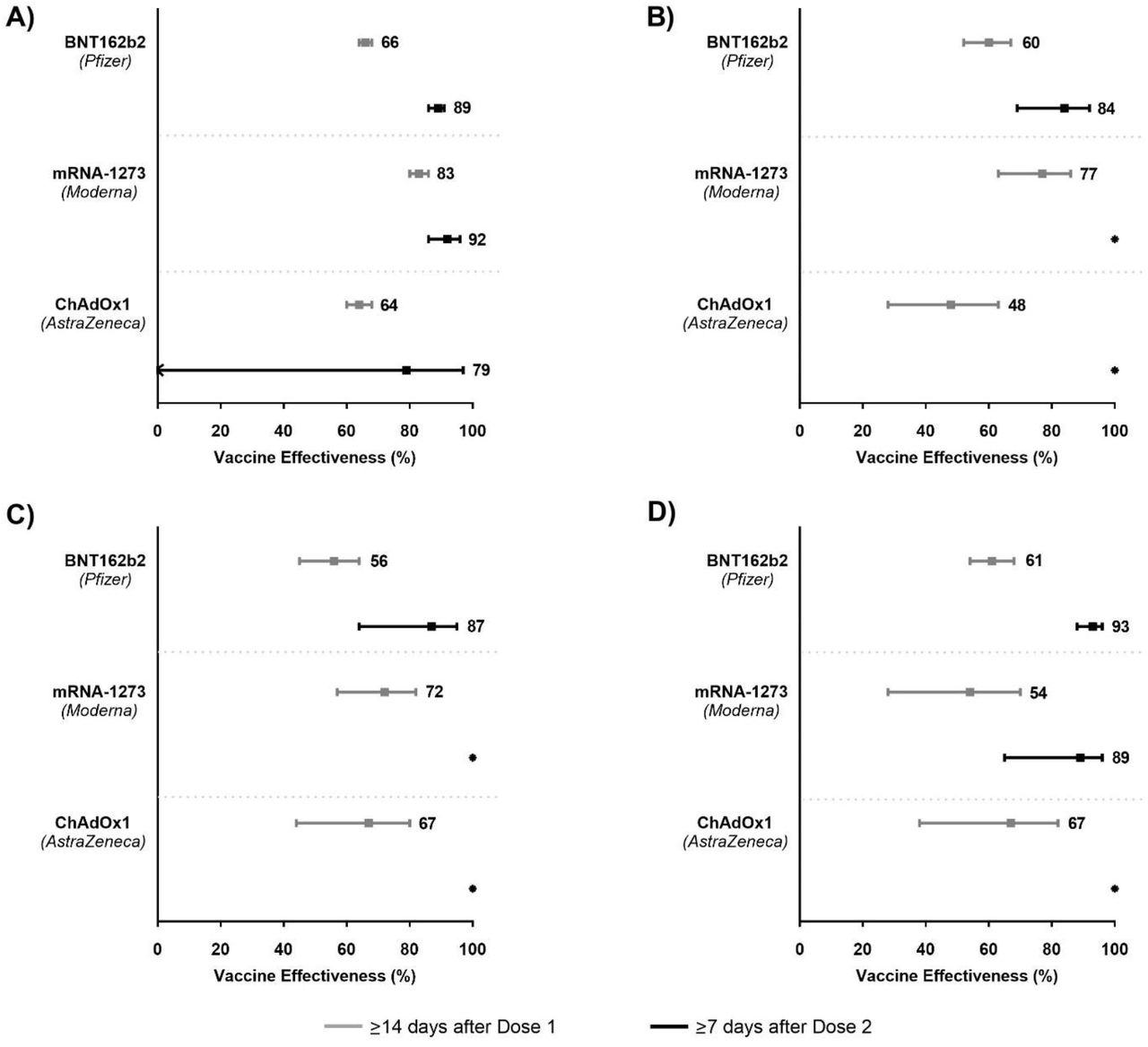
Models were adjusted for age, sex, public health unit region, period of test (weekly period for Delta, and bi-weekly period for non-VOC SARS-CoV-2 and other VOCs), number of SARS-CoV-2 tests in the 3 months prior to 14 December 2020, presence of any comorbidity that increase the risk of severe COVID-19, receipt of 2019/2020 and/or 2020/2021 influenza vaccination, and Census dissemination area-level quintiles of household income, proportion of persons employed as non-health essential workers, persons per dwelling, and proportion of self-identified visible minorities.
When comparing vaccine effectiveness by product between VOCs, vaccine effectiveness after partial vaccination tended to be lower against Delta than against Alpha for mRNA-1273 (72% vs. 83%) and BNT162b2 (56% vs. 66%), but was similar to Alpha for ChAdOx1 (67% vs. 64%). Full vaccination with BNT162b2 increased protection against Delta to levels comparable to Alpha and Beta/Gamma.
Vaccine effectiveness against hospitalization or death caused by all studied VOCs was generally higher than for symptomatic infection after partial vaccination with all three vaccines (Figure 2). In particular, against Delta, vaccine effectiveness against severe outcomes after 1 dose of BNT162b2, mRNA-1273, and ChAdOx1 was 78% (95% CI, 65–86%), 96% (95% CI, 72–99%), and 88% (95% CI, 60–96%), respectively (Figure 2C). Full vaccination was associated with vaccine effectiveness estimates in the mid-90%s against Alpha and Beta/Gamma for BNT162b2 and against Alpha for mRNA-1273, but could not be reliably estimated for other VOC-vaccine combinations due to low numbers, or absence, of vaccinated test-positive cases.

{kind=link}
{kind=link}
Models were adjusted for age, sex, public health unit region, period of test (weekly period for Delta, and bi-weekly period for non-VOC SARS-CoV-2 and other VOCs), number of SARS-CoV-2 tests in the 3 months prior to 14 December 2020, presence of any comorbidity that increase the risk of severe COVID-19, receipt of 2019/2020 and/or 2020/2021 influenza vaccination, and Census dissemination area-level quintiles of household income, proportion of persons employed as non-health essential workers, persons per dwelling, and proportion of self-identified visible minorities.
In the sensitivity analyses, vaccine effectiveness estimates using longer intervals after vaccination were mostly very similar (estimates differed by <5%) to our primary analyses (Table 3). Where differences were >5%, the longer intervals yielded higher estimates. Similar vaccine effectiveness estimates were also observed when limiting the study period to 05 April 2021 to 30 May 2021 (Supplementary Table 3).
In age group-stratified analyses, vaccine effectiveness against symptomatic infection caused by all VOCs was lower or similar in older adults (aged ≥60 years) compared to younger individuals (aged <60 years) after partial vaccination (Supplementary Table 4). Vaccine effectiveness in older adults increased to levels comparable to younger individuals after full vaccination. Vaccine effectiveness was higher against hospitalization and death than symptomatic infection for both older and younger age groups.
DISCUSSION
We estimated that partial vaccination with BNT162b2 and mRNA-1273 were >55% and >70% effective, respectively, against symptomatic infection caused by currently circulating VOCs in Ontario, Canada. Partial vaccination with ChAdOx1 prevented nearly half of symptomatic infections by Beta/Gamma, and was >60% effective against Alpha and Delta. Vaccine effectiveness was substantially improved following full vaccination with mRNA vaccines.
Effectiveness of partial vaccination was substantially higher against hospitalization or death than against symptomatic infection for all VOC-vaccine combinations except for mRNA-1273 against Alpha because vaccine effectiveness against symptomatic infection was already high; full vaccination with mRNA vaccines further improved effectiveness against severe outcomes. We also found that the use of longer intervals after vaccination resulted in similar or higher estimates, restricting the analysis to a period when all VOCs were co-circulating yielded similar results, and the effectiveness of partial vaccination tended to be lower for older adults compared to younger adults.
Our vaccine effectiveness estimates against symptomatic COVID-19 infection with Alpha and Beta/Gamma after partial vaccination with mRNA or ChAdOx1 vaccines are similar to estimates against infection from British Columbia (67% for mRNA vaccines against Alpha and 61% against Gamma)19 and Qatar (88% for mRNA-1273 against Alpha)6 but higher than estimates after partial vaccination against infection or symptomatic COVID-19 reported from Qatar (for BNT162b2, 30% against Alpha and 17% against Beta3; 61% for mRNA-1273 against Beta6), England (49% for BNT162b2 and 51% for ChAdOx1 against Alpha)4 and Scotland (27% for BNT162b2 and 39% for ChAdOx1 against Alpha)2. Our estimates after partial vaccination are also higher than the estimates for severe, critical, or fatal disease with BNT162b2 in Qatar (54%)3 but comparable with the estimates for hospitalization in England (83%)5 caused by the Alpha variant with BNT162b2 or ChAdOx1 and for severe, critical, or fatal disease with mRNA-1273 caused by Alpha/Beta in Qatar (82%)6. Similarly, we estimated higher vaccine effectiveness against symptomatic COVID-19 with the Delta variant after partial vaccination with mRNA or ChAdOx1 vaccines than the effectiveness against symptomatic or asymptomatic infections reported in other studies (30–33% for BNT162b2 and 18–33% for ChAdOx1).2,4 Against hospitalization with the Delta variant, our vaccine effectiveness after partial vaccination was lower for BNT162b2 and higher for ChAdOx1 than another study (78% vs. 94% for BNT162b2 and 88% vs. 71% for ChAdOx1).5 However, after full vaccination, our estimates against both outcomes for all VOCs were comparable with estimates reported in previous studies.2-5 Our estimates against symptomatic infection with Alpha and Delta are higher than vaccine efficacy estimates for BNT162b2 or ChAdOx1 after dose 1, and comparable after dose 2 of BNT162b2.20
The heterogeneity in vaccine estimates, particularly after partial vaccination, across studies could result from a number of factors, including differences in study design, study population, SARS-CoV-2 test assays and testing criteria, comprehensiveness of test results recorded in databases, outcome definitions and ascertainment, timing of VOC circulation, vaccine priority groups, vaccine rollout, interval between vaccine doses, and variables adjusted to control for possible confounding.21
Province-wide data allowed us to estimate the effectiveness of all three vaccines in use in Canada against symptomatic infection and severe outcomes caused by the four VOCs currently in circulation in Canada. The test-negative study design has the advantage to control for bias resulting from differences in healthcare-seeking behaviour between vaccinated and unvaccinated individuals.
There are some limitations of our study. First, VOC classification in this study relied on a combination of mutation screening and whole genome sequencing, and the criteria for sequencing evolved over the course of the pandemic. Our definition of Delta specimens relied largely on a proxy measure of a N501Y-/E484K-result on mutation screening and a combination of date and geographic location, which were used to infer probable Delta variant specimens. Thus, a small proportion of specimens classified as Delta may have been non-VOC SARS-CoV-2 specimens. Second, since vaccine effectiveness is likely impacted by age, interval between vaccine receipt and index date, vaccine product, and VOC, and given that the eligibility criteria for vaccination (e.g., initial prioritization of older age groups), availability of certain vaccine products, and distribution of circulating VOCs all varied over time, comparisons of vaccine effectiveness estimates between combinations of vaccine products and VOCs should be made with caution. However, we included a sensitivity analysis that restricted the study period to individuals tested during April and May (to ensure that all VOCs and non-VOC SARS-CoV-2 were circulating and to mitigate temporal confounding caused by the aforementioned factors), which yielded very similar results to our primary analysis. Third, it is possible that we may have underascertained severe outcomes if they were not recorded in the CCM database, such as when severe outcomes occur after completion of case follow-up or when case volumes exceed public health system capacity and public health investigation of each laboratory-confirmed case is not possible. This may have resulted in overestimation of vaccine effectiveness against severe outcomes. Fourth, we used specimen collection date as the index date because of lack of available data on symptom onset date in OLIS, which precluded us from restricting the study population to individuals who were tested within 10 days of symptom onset. Thus, we may have underestimated vaccine effectiveness by increasing the risk of false-negative cases by extending the interval between symptom onset and testing. Last, despite our best efforts to adjust for potential confounders and the use of the test-negative design, these results may nonetheless be susceptible to residual confounding given the observational nature of the study.
Our real-world vaccine effectiveness estimates suggest that even a single dose of these 3 COVID-19 vaccine products provide considerable protection against symptomatic infection and severe outcomes caused by these 4 currently circulating VOCs, and that 2 doses are likely to provide even higher protection. Our findings have public health policy implications worldwide. Notably, jurisdictions facing COVID-19 vaccine supply constraints may benefit from delaying the second dose to maximize the number of individuals receiving partial protection from the first dose, thereby potentially providing greater overall protection of the population more rapidly.
Data Availability
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Contributors
JCK and HC designed and oversaw the study. SH and HC obtained the data and conducted all analyses (data set and variable creation and statistical modelling). BC contributed to data analyses and data preparation for the symptomatic data set. HC and SH verified the data in the study. SN did the literature search. SN and JCK drafted the manuscript. All authors contributed to the analysis plan, interpreted the results, critically reviewed and edited the manuscript, approved the final version, and agreed to be accountable for all aspects of the work.
Declaration of interests
KW is CEO of CANImmunize and serves on the data safety board for the Medicago COVID-19 vaccine trial. The other authors declare no conflicts of interest.
Funding
This work was supported by the Canadian Immunization Research Network (CIRN) through a grant from the Public Health Agency of Canada and the Canadian Institutes of Health Research (CNF 151944). This project was also supported by funding from the Public Health Agency of Canada, through the Vaccine Surveillance Reference Group and the COVID-19 Immunity Task Force. This study was also supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH). JCK is supported by Clinician-Scientist Award from the University of Toronto Department of Family and Community Medicine. PCA is supported by a Mid-Career Investigator Award from the Heart and Stroke Foundation.
Ethics approval
ICES is a prescribed entity under Ontario’s Personal Health Information Protection Act (PHIPA). Section 45 of PHIPA authorizes ICES to collect personal health information, without consent, for the purpose of analysis or compiling statistical information with respect to the management of, evaluation or monitoring of, the allocation of resources to or planning for all or part of the health system. Projects that use data collected by ICES under section 45 of PHIPA, and use no other data, are exempt from REB review. The use of the data in this project is authorized under section 45 and approved by ICES’ Privacy and Legal Office.
Data sharing
The dataset from this study is held securely in coded form at ICES. While legal data sharing agreements between ICES and data providers (e.g., healthcare organizations and government) prohibit ICES from making the dataset publicly available, access may be granted to those who meet pre-specified criteria for confidential access, available at www.ices.on.ca/DAS (email: das{at}ices.on.ca). The full dataset creation plan and underlying analytic code are available from the authors upon request, understanding that the computer programs may rely upon coding templates or macros that are unique to ICES and are therefore either inaccessible or may require modification.
Disclaimers
This study was supported by ICES, which is funded by an annual grant from the Ontario Ministry of Health (MOH) and the Ministry of Long-Term Care (MLTC). This study was supported by the Ontario Health Data Platform (OHDP), a Province of Ontario initiative to support Ontario’s ongoing response to COVID-19 and its related impacts. The study sponsors did not participate in the design and conduct of the study; collection, management, analysis and interpretation of the data; preparation, review or approval of the manuscript; or the decision to submit the manuscript for publication. Parts of this material are based on data and/or information compiled and provided by the Canadian Institute for Health Information (CIHI) and by Cancer Care Ontario (CCO). However, the analyses, conclusions, opinions and statements expressed herein are solely those of the authors, and do not reflect those of the funding or data sources; no endorsement by ICES, MOH, MLTC, OHDP, its partners, the Province of Ontario, CIHI or CCO is intended or should be inferred.
Acknowledgments
We would like to acknowledge Public Health Ontario for access to case-level data from CCM and COVID-19 laboratory data, as well as assistance with data interpretation. We also thank the staff of Ontario’s public health units who are responsible for COVID-19 case and contact management and data collection within CCM. We thank IQVIA Solutions Canada Inc. for use of their Drug Information Database. The authors are grateful to the Ontario residents without whom this research would be impossible.
Footnotes
Updated abstract; included additional sensitivity analyses and age stratified analyses results; updated manuscript and supplemental file.
References



