
ABSTRACT
Introduction Therapeutic Mammoplasty (TM) is a Oncoplastic Breast Surgery (OBS) technique suitable for medium-to-large breasts with ptosis with large or multifocal/multicentric (MF/MC) tumors. Several studies have indicated that TM expands the scope, extent, and application of breast conservation surgery. This report describes in detail TM outcomes in Indian breast cancer (BC) patients.
Methods From our single institutional cohort (n = 211), we present data related to surgical techniques, clinical management, oncological safety, cosmetic and patient reported outcomes (PROMs, based on Breast-Q questionnaire) from BC patients who underwent TM (categorized as simple, complex, extreme and split-reduction type)
Results Mean age at diagnosis was 48.7 years. Majority of these patients had advanced stage (II/III) disease. 178 patients consented and 171 completed 1 year follow-up from 3 main groups (a) simple (n=87) (b) complex (n =39) and (c) extreme TM (n = 49). The post-operative complication rates were low (<10%) without any delay in adjuvant treatment. Cosmetic scores were good-to-excellent (n = 154). Post-1-year PROMs (n=149) revealed good-to-excellent score for satisfaction with breast, cosmetic outcome and psychosocial well-being for all TM types.
Conclusion Our study is a first detailed report describing a multi-factorial audit in TM single institutional cohort in Indian BC patients. We propose that our TM technique/s may be optimally suited for BC scenarios common in India namely (a) advanced stage BC patients with moderate-to-large breasts with mild/severe ptosis (b) multifocal, multicentric tumors (c) LABC at initial presentation.
INTRODUCTION
Breast conservation therapy (BCT) which involves breast conversation surgery (BCS) followed by adjuvant radiotherapy (RT) is now established as a standard of care for Breast Cancer (BC) (Fisher et al. 1989; Silverstein et al. 2015a). Several studies have shown equivalent survival rates between BCS and mastectomy after a 20-year follow-up (Losken et al. 2014; De La Cruz et al. 2016; Campbell and Romics 2017). Recent studies have suggested a better disease free and overall survival with improvement in quality of life (QoL) in patients undergoing BCT as compared with mastectomy (van Maaren et al. 2016; de Boniface et al. 2021).
However, unsatisfactory post-BCT cosmetic outcomes were observed in 30% cases in which large size (∼10-20%) of the breast tissue was excised (Egro et al. 2015). Such poor cosmesis has been attributed to post-BCS breast defect or asymmetry between the breasts or nipples. As of today, BCT has limited applications in patients with multi-focal or multi-centric disease and/or with extensive microcalcifications. Conventionally, multifocal and multi-centric cancers have been labelled as a contraindication for BCS, though low recurrence rates have been observed in patients with multiple ipsilateral breast cancer treated with BCT (Winters and Bernaudo 2018).
The concept of Oncoplastic Breast Surgery (OBS) was first introduced in the 1990’s by Prof. Audretsch when he described the technique of partial reconstruction of the breast, using plastic surgical technique (Losken and Ghazi 2012). OBS is now increasingly being accepted as standard-of-care in surgical management of BC cases across the world due to the benefits such as oncological safety with concurrent improvement in aesthetic results and Quality of Life (QoL) (Chen et al. 2015; Silverstein 2016; De La Cruz et al. 2016).
OBS procedures involving partial breast reconstruction are classified according to volume replacement or volume displacement techniques (Savalia and Silverstein 2016). Therapeutic Mammoplasty (TM) is a commonly used volume displacement technique suitable for OBS in women with medium/large breasts with ptosis. TM combines advantages of oncologically safe wide excision of tumor with breast reduction, mastopexy and contralateral symmertrisation techniques (Winters and Bernaudo 2018). This technique increases application of BCS and scope of BCT by facilitating larger tumors excision margins, lower re-excision rates, decreases rates of positive margins and reduction in rate of mastectomies (Macmillan et al. 2014; Potter et al. 2020). TM has been shown to achieve satisfactory outcomes by reducing the breast size thereby facilitating better delivery and distribution of RT regimens, achieving contralateral breast symmetry and improving the QoL. The oncological safety and efficacy of TM have been confirmed in early BC cases indicated by higher rates of overall survival (OS), disease free survival (DFS) with low recurrence, lower complication rates and superior cosmesis (Iwuchukwu et al. 2012). Furthermore, TM offers a pragmatic option for BCS in women who present with LABCs (>5cms), multifocal or multicentric tumors or extensive microcalcifications wherein a mastectomy would be a surgical procedure of choice (Silverstein et al. 2015a; Losken et al. 2017). However, even though indicated for smaller ptotic breasts in selective cases, TM may not be effective due to paucity of breast tissue resulting in extremely small size and cosmesis of operated breast (Savalia and Silverstein 2016).
The Therapeutic Mammoplasty study (TEAM) is a large, international, multicentric cohort study to evaluate the safety and efficacy of TM in women undergoing BCS for invasive or pre-invasive BC as per consensus guidelines developed by European breast units (O’Connell et al. 2018). The TEAM study has reported that TM procedure is a safe and effective alternative to mastectomy or standard BCS. Recently, data from the national iBRA-2 and TEAM studies were combined to compare the safety and short-term outcomes of TM and mastectomy with or without immediate breast reconstruction. This data indicated that BCS was possible in 87 % TM cases without delay in adjuvant treatment indicating that TM may allow high-risk patients who are not candidates for IBR to avoid mastectomy safely (Dave et al. 2016; O’Connell et al. 2018).
Majority of Indian BC patients present with larger tumors in advanced stages (Doval et al. 2020). This limits the scope of upfront BCS with or without OBS, unless they have a favorable breast-to-tumor ratio. In such patients, OBS with the TM procedure has been shown to effectively extend the boundaries of surgical excisions (Silverstein 2016). However, the field of OBS is still nascent in India and is practiced predominantly by a handful of breast surgeons from Tier 1 cities. This limited OBS uptake could be attributed to multiple barriers such as lack of awareness, healthcare economics, logistics challenges at public and private sectors hospitals, psychological taboos for women to undergo a unilateral or bilateral BCS and paucity of well-trained OBS surgeons (Koppiker et al. 2019a).
With this background, we undertook the current study to investigate and analyze the outcomes of TM with focus on oncological safety and efficacy in Indian BC patients. From our single-institution TM cohort, we present data on 211 patients who were candidates for OBS or a mastectomy (based on their tumor characteristics) but finally underwent a TM after analyzing the feasibility and safety of the procedure along with careful counseling and Standard operating procedures (SOPs). Based on the guidelines of the TEAM protocol, we report the clinicopathological profiles of our cohort and experiences related to various TM surgical techniques (i.e., simple, complex, extreme oncoplasty and split reduction mammoplasty). We discuss in detail our observations on surgical and oncological outcomes, complication rates, time to adjuvant therapy, RT outcomes and patient reported outcomes (PROMs) amongst Indian BC patients undergoing TM.
METHODOLOGY
1 Types of Therapeutic Mammoplasty
1.1 Simple Therapeutic Mammoplasty
Simple Therapeutic Mammoplasty is a procedure in which the tumor lies within a normal reduction pattern. In these cases, the superior, inferior or superomedial pedicles are routinely used (Savalia and Silverstein 2016).
1.2. Complex Therapeutic Mammoplasty
This technique is used when the tumors are outside the primary reduction pattern. The reconstruction is carried out either by extensions of the primary pedicles or by the use of secondary pedicles. Extended or Secondary pedicles are the other parts of the breast that are generally excised, which are used to fill the defects. The later are preferred as they have better blood supply reaching the most distant areas of the pedicle as compared to extended ones (Savalia and Silverstein 2016).
1.3. Extreme Therapeutic Mammoplasty
Extreme Oncoplasty is the application of OBS to include extreme situations where conventionally a mastectomy would be advised. These include large multi-centric, multi-focal tumors, extensive DCIS and poor response to NACT requiring large areas of resection (Koppiker et al. 2019b).
1.4. Split Reduction Mammoplasty
Split Reduction is a TM procedure applicable when the tumor lies outside the reduction pattern and the skin over the tumor needs to be removed (Silverstein et al. 2015b).
2. Surgical Procedures
2.1 Pre-operative Markings
In the pre-operative planning, appropriate markings are placed on both breasts based on wise pattern or vertical scar incision. The nipple area complex is positioned between 19-23 cm from sternal notch, which is often determined by placing the fingers at the inframammary fold and projecting on the anterior surface of the breast in the meridian.
2.2 Wise Pattern or Vertical Scar Incision
The 1st step of the surgery begins by marking out the wise pattern incision. The area of the appropriate pedicle (based on the type of the therapeutic mammoplasty procedure) which carries the nipple is marked and de-epithelized. The next step is to localize the tumor and excise it with wide margins by going through one of the limbs of the wise pattern. This localization is performed either pre-operatively by stereotactic guide-wire placement or by placement of wire and needle on the operating table using a high-resolution ultrasonography.
2.3 Oncological Clearance and NAC Positioning
Nipple-Areola complex (NAC) is marked out, and the incision is made around the areola carefully. The tumor and its quadrant are then widely excised through one of the limbs of wise pattern incision. If required, further imaging of the specimen is performed using specimen mammography to ensure that the tumor is excised with wide margins. After this step, the shaved margins of the cavity are further excised and sent for frozen sections to assess margin positivity. If any positive margins are close to the tumor, they are re-excised. Once clarity about the tumor margins of the excision cavity is achieved, the decision is made to use one of the appropriate pedicles (based on the type of TM technique deployed).
2.4 Marking Out the Tumor Bed for Targeting Radiotherapy
The tumor bed is marked with Liga clips in the superior, inferior, medial and lateral, the base and anterior margins. Once the restructuring is completed, the margins of the tumor are determined. In our experience, the tumor margins remain contained in the initial tumor volume for targeted radiotherapy. The possibility of tumor margin getting repositioned in some other quadrant is less likely.
2.5 Choice of Pedicles for Various TM Techniques
After this step, the appropriate pedicles are marked out and dissected according to the location of the tumor. According to quadrant diagrams, if the tumor is at 12 O’clock position in UOQ, an extended inferior pedicle is used. If a tumor is present in outer quadrants (i.e., at 2,3 or 4 O’ clock position of left breast or at 8,9 or 10 O’clock positions of the right breast), dual pedicle technique is preferentially used. In this technique, the inferior pedicle fills up the gap and the NAC are positioned on a superior, superomedial or lateral pedicle. The main aim of the dual pedicle technique is to contour the defect with one pedicle and position the NAC on the other, thereby providing a dual vascular supply.
2.6 Axillary Management
Once these wise pattern incisions are carried through to the chest wall, the lateral dissection is taken into the axilla and the axillary dissection or sentinel node excision is performed through the same incision. No separate incision is taken on the axilla. Care is taken to dissect out the lateral thoracic artery and to ensure that the lateral pillar is well perfused by various perforators. Thereafter, the incisions are closed. Drains are not inserted in the axilla unless an axillary clearance has been performed.
2.7 Split Reduction Therapeutic Mammoplasty Technique
In this technique, the lower limb of the wise pattern is shifted over the tumor site. Then the outer limb of the wise pattern is shifted upwards to lie over the tumor so that there is no incision in the IMF on the outer side (Silverstein et al. 2015b).
3. Clinical Management
BC diagnosis was based upon clinical examination and radiological evaluation of breast and axilla using Full Field Digital Mammography (FFDM) with 3-D Tomosynthesis (Siemens Mammomat Inspiration™) and Ultrasonography (Siemens Acuson S2000™). Histopathological studies on tru-cut biopsy samples (majority of cases) or vacuum assisted biopsy (for index tumors, Encor Ultra™) samples were performed for confirming diagnosis of breast carcinoma. Similarly, ultrasonography and fine needle aspiration cytology was used for investigating axillary lymph node metastasis. Confirmed BC cases underwent breast surgery at a network hospital site. The oncologic management with chemo-radiation protocols was undertaken by a multi-disciplinary clinical team in accordance with the current NCCN guidelines (Koppiker et al. 2019b).
4. Radiation Therapy
The RT dose planning was aimed at achieving a Biologically Effective Dose (BED) of 50 Gy for all patients. The breast along with the supraclavicular region (if indicated) was irradiated by 6 MV photon beams using Forward Plan Field-in-Field Intensity Modulated Radiation Therapy (F-P FiF IMRT) or Volumetric Modulated Arc Therapy (VMAT). Two tangential fields along with multiple sub-fields were used for this treatment. CT images (5 mm thickness) were obtained with the patient immobilized in a vacuum cushion (Vacloc) at different transverse sections covering the region of interest with adequate margins to create a 3D image. Volume delineation (CTV, Contralateral breast, Lung and Heart) on CT images was performed on Eclipse™ contouring station. Computerized treatment planning was performed on Eclipse™ treatment planning system (TPS) (Version 13.5.35) for F-P FiF IMRT plans and Monaco® (Version 5.11) TPS for VMAT plans. High energy linear accelerator (Elekta Synergy, Elekta Medical System™, UK) with 80 leaves Multi Leaf Collimator (MLCi) was used for tangential treatments to the breast field. RT plan was accepted if at least 95% of prescribed dose covers the 100% of planning target volume (PTV). Hot spot in PTV was accepted up to 110% of prescribed dose. Tumor bed boost, wherever indicated, was performed using either an electron portal or Simultaneous Integrated Boost (SIB) technique.
5. Assessment of Post-Surgery Complications
Post-surgery outcomes were assessed by breast oncoplastic surgeons and radiation oncologists, respectively. As per the Clavien Dindo classification, post-surgery complications were classified as ‘major’ when they required surgical intervention and ‘minor’ when they were managed conservatively (Panhofer et al. 2014). We also noted the time between completion of surgery and start of adjuvant therapy to ascertain any delays in adjuvant therapy.
6. Patient Reported Outcome Measures (PROMs)
The PROMs were used to evaluate patient satisfaction and QoL after TM procedures. To assess PROMs, a standardized Breast-Q questionnaire was utilized. The Breast-Q module was divided into multiple independent scales. Higher scores indicate greater patient satisfaction and functionality (Koppiker et al. 2019b).
7. Data Analysis and Statistics
Proportional analysis was undertaken for determining cohort characteristics. Statistical analysis for inter and intra-group comparisons were undertaken using Students t-test (p=0.05).
RESULTS
A. Overview of TM Study Cohort
A1. Characteristics of Study Cohort
At our institution, 211 TM procedures have been performed on BC patients with moderate and large breasts with various grades of ptosis during the period of 2012-2019, Amongst these 211, 178 patients consented to data sharing. Only 171 patients were included in the final study cohort as they completed a minimum of 12 months post-surgery follow-up. Data collection was performed according to the recommendations of the TEAM protocol.
The BC cases reported in this cohort underwent various types of TM procedures namely (a) Simple (b) Complex (c) Extreme (d) Split-reduction. A representative case from each of these 4 TM categories are described in detail in the Supplementary section. The case description includes case summary alongwith images depicting pre-operative markings, intra-operative techniques and post-operative outcomes.
Demographic distribution of study participants and their clinico-pathological characteristics are summarized in Table 1a and 1b. In our study cohort, 166 patients had unilateral and 5 had bilateral breast cancers. Tumors were found in the UOQ in 74 (43.2%) patients, LOQ in 21 (12.3%) patients, UIQ in 33 (19.3%) patients and LIQ in 24 (14.2%) patients. The mean age of patients at diagnosis was 48.7 years. Majority of these patients were at Stage II or III. Majority cases were either IDC and/or DCIS. Clear margins were achieved in all the patients on the frozen section as well confirmed on final histopathology analysis. The average margin distance achieved was 12.5 mm. Axillary lymph node dissection was performed in 59 (33.3%) cases and sentinel node biopsy was performed in 113 (63.9%) cases.
Of the 40 (23.4%) patients who received NACT and 10 (5.9%) patients who received NAHT respectively, 14 (8.1%) patients achieved complete clinical response. In the post-operative period, adjuvant chemotherapy and/or RT was administered to patients according to clinical indications (Table 1a). 92 (54%) patients were administered adjuvant chemotherapy. Adjuvant RT data was available from 150 (88%) patients. None of the patients in our study cohort experienced any delays in their adjuvant therapies. While one case had local recurrence within 12 months, 2 cases recurred within 24 months (Table 1b).
A2: Post-Operative Complications
Post-operative complications were classified based on grades as per Clavien Dindo Classification adapted for Breast Cancer (Panhofer et al. 2014). There were 15 cases of complications in Grade 3a including cases of seroma (requiring aspiration). There was 1 case of Grade 2 (wound infection) and 14 cases of Grade 1 complications such as seroma/ haematoma not requiring drainage, minor skin necrosis, fat necrosis, delayed wound healing. All complications were treated conservatively in the outpatient settings (Table 2).
A3: Radiation Therapy
Of the 171 patients included in our study cohort, 150 patients underwent RT as clinically indicated (Table 3a). RT data on the remaining 21 cases (12%) was not available as these represented cases of phyllodes (n = 8), who rejected RT (n =11) or who were lost to follow-up (n =2). Out of the 148 cases 78 patients had left-sided lesions, 86 patients had right-sided lesion and 5 patients had bilateral lesions. While 73 of these 148 patients received RT to the whole breast alone, 65 received RT to the breast along with the supraclavicular region. Forward Plan Intensity Modulated Radiation Therapy (IMRT) was used to treat 123 patients. 16 patients were treated using Volumetric Modulated Arc Therapy (VMAT) and 1 patient received Simultaneous Integrated Boost (SIB). 113 patients received electron-boost. 9 patients underwent APBI. (Supplementary Table 1). The RT regimen for various types of TM procedures is depicted in Table 3b and was considered effectively safe.
A4: Patient Reported Outcome Measures (PROMs)
Prom’s data was collected from the study participants after minimum period of 12 months post-surgery with the Breast-Q questionnaire. Out of 171 study participants, 149 (87.1%) responded to the questionnaire. PROMs were used to assess patient reported satisfaction and QoL after various types of TM procedures (namely simple, complex and extreme oncoplasty). Table 4 indicates patient reported improvement in the four areas evaluated after surgery. While 76% patients expressed satisfaction with breasts, 83% reported satisfaction with overall outcome. Furthermore, majority patients reported satisfaction with psychosocial well-being (85%), and sexual well-being (75%) and physical well-being (73%). This trend of high percentage of patient satisfaction was observed from PROMs patients who have undergone all 3 types of therapeutic mammoplasty procedures, namely simple, complex and extreme oncoplasty (Table 4 and Figure 4).
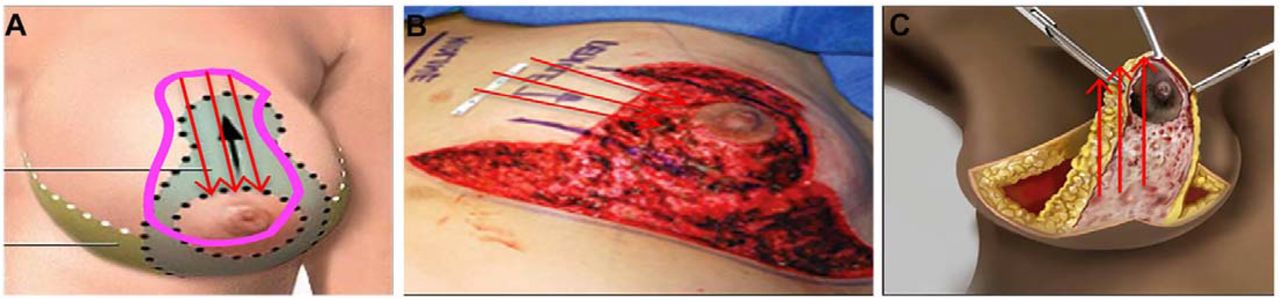
A. Superior pedicle mammoplasty, B. Superomedial pedicle mammoplasty, C. Inferior pedicle mammoplasty.

Study cohort details
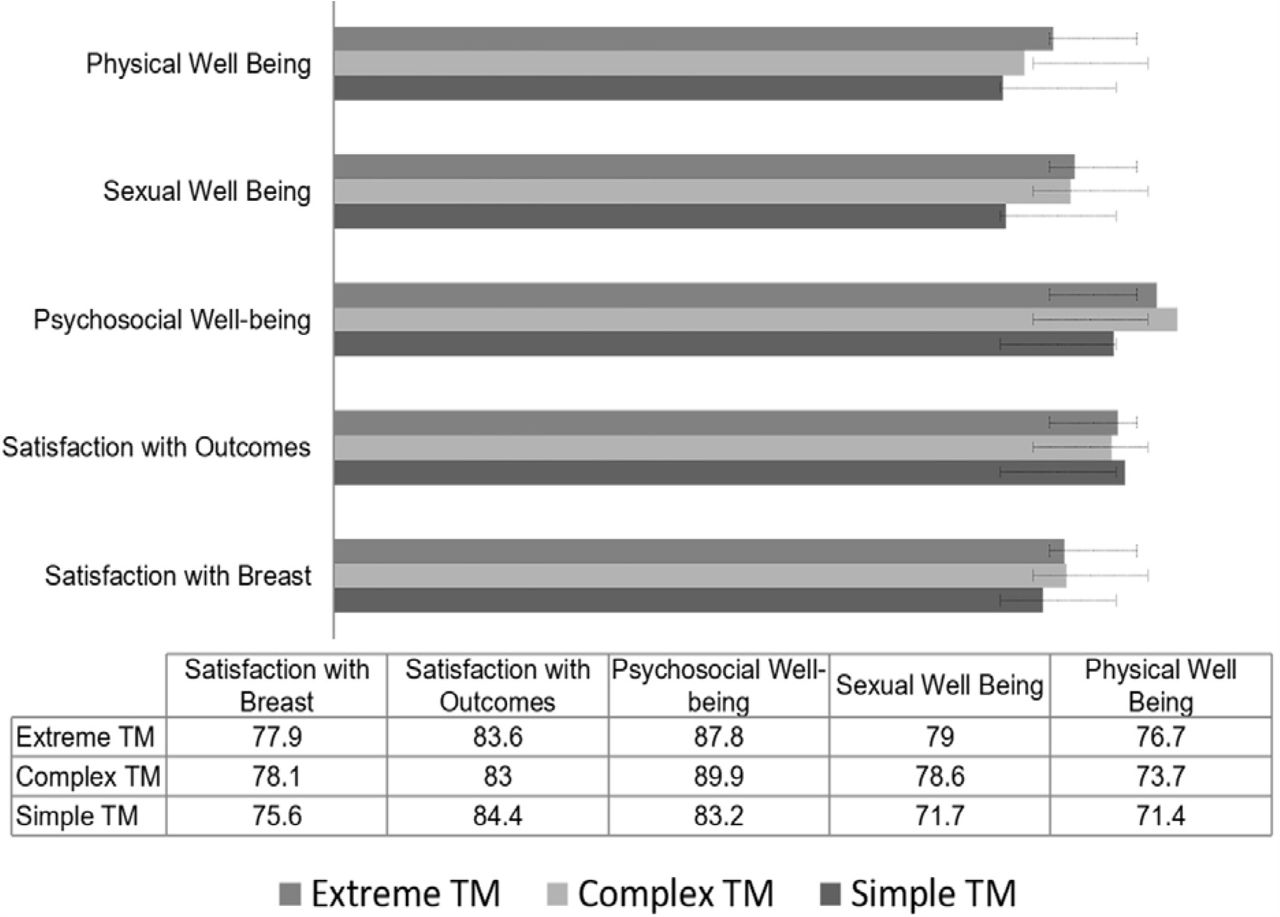
Breast Q based PROMs were analyzed for BC cases that underwent simple/complex/extreme TM procedures.
B5: Cosmetic Score Analysis
Out of 171 Therapeutic mammoplasty cases, cosmetic scores available for 154 patients based on independent assessment by 3 surgeons.
DISCUSSION
In this report, we present the first comprehensive, single-institutional study on TM outcomes in Indian breast cancer patients based on the recommendations of the TEAM protocol (O’Connell et al. 2018). We present best practices from our center on the feasibility and application of various TM procedures, experiences from surgical and oncological outcomes and PROMs to propose a wider acceptance of TM in various clinical indications.
1. Patient Selection
At our institution, routine pre-op counseling is performed by the surgeons to discuss options such as mastectomy, BCS and OBS. If the patient consents for TM, simultaneous contralateral breast reduction option for superior cosmetic outcomes is also discussed, especially, for women with ptotic breasts (Grades 1-3) and moderate-to-large sized breasts who would benefit significantly from this procedure.
2. Choice of TM Technique
TM-related decision-making algorithms are based on the tumor location and the breast sizes. In our practice, we have classified TM techniques into 4 categories with indications as follows:
Most of the cases in our study cohort have been operated using the dual pedicle technique in which NAC was carried on superior pedicle and the inferior pedicle was used to fill the defect caused by excision of the tumor.
In patients either with smaller breasts or with large excisions, we have frequently used the whole lower segments of the breast (i.e., inferomedial and inferolateral pedicles) so the breast mound is advanced into the defect and NAC is reimplanted onto the pedicle.
Owing to financial and logistical challenges, Indian patients have poor acceptance of a second operative procedure (Koppiker et al. 2019a). Therefore, we perform a single-step TM procedure that involves simultaneous reconstruction of the NAC and contralateral reduction mammoplasty for bilateral symmetrization in which the nipple may undergone resection with a NAC graft. If the patient does not consent for opposite symmetrization, alternative OBS procedures to TM are recommended.
3. Patient Demographics
Given that the medical, psycho-social-cultural and economic profiles of Indian BC patients are significantly different than western countries, we had to adapt our TM techniques accordingly.
In our TM cohort, the mean age of study participants was 48.7 years indicating a younger demography. In agreement with previous reports (Potter et al. 2020), majority of these BC patients (i.e., 109 (63.7%)) had comorbidities such as obesity and diabetes making them ineligible for mastectomy with immediate reconstruction. Our cohort demonstrates 45 (26.3%) patients underwent an upfront extreme oncoplasty and 50 (29.2%) patients received NACT followed by TM. Thus, TM may be a feasible surgical option for Indian BC cases with advanced stages with either a multifocal, multicentric tumors or LABC at initial presentation.
Typically, 50% of BCs affect the UOQ alone and the outer sector is known to harbor most of them (Clough et al. 2010). In our study, 118 (69%) patients had tumors in the upper quadrant, amongst which 74 (43.2%) were in the UOQ alone. Based on our experience, an extended inferior pedicle or a dual pedicle would provide optimal outcomes in such situations (Case Study #2-3?). However, TM (extreme or split reduction mammoplasty) would be a suitable option in cases with large excisions which were otherwise indicated for mastectomy (Case Study #4).
4. Surgical Outcomes/Complications
The complication rates of OBS procedures depend on the technique, length of the procedures, associated comorbidities and post-operative care (De La Cruz et al. 2016). In general, ∼14% OBS cases demonstrate overall post-operative complications ranging from fat necrosis, skin necrosis, hematoma seroma, delayed wound healing, nipple necrosis and/or wound infection (Campbell and Romics 2017).
To avoid variable reporting, we used the validated Clavien Dindo classification system in our study cohort (Panhofer et al. 2014). In agreement with literature, we recorded a relatively low rate of overall complications (i.e., a total of 30 (17.4%). Of these, 15 (8.7%) required an intervention while the others were treated conservatively in the out-patient department No readmissions were noted. In general, we observed low rate of Grade I/II complications after complex and extreme mammoplasty techniques in high-risk patients with comorbidities who are otherwise prone to developing post-op complications. Taken together, these observations indicate that TM could be a feasible option for Indian BC patients who present in advanced stages with either multifocal, multi-centric tumors or LABC at initial presentation.
In post NACT cases, we observed that TM technique was useful in removing large areas of residual calcifications or clinically large residual tumors, which could turn out to be just fibrosis. Hence, we have been able to improve our post-NACT BCS rate up to 70% (unpublished observations).
5. Post-Surgery Treatment
In our study, majority of patients had a average hospital stay of 2 days (including admission until discharge) consistent with the length of stay required for either a BCS or a mastectomy.
Majority of Indian BCs are diagnosed in advanced stages with node-positive status, thereby, necessitating adjuvant chemotherapy (PMID: 32246015). Duration of treatment for surgical complications is likely to affect the patient’s QoL resulting in delay in adjuvant treatment, which in turn, would influence overall oncological outcomes. In our study, the mean duration from TM to start of adjuvant treatment was 50 days without any delay. This observation was consistent with several studies that indicate OBS does not result in delay in adjuvant treatment (Harvey et al. 2014).
The optimal duration between OBS and RT has not been established. In our practice, we prefer commencing RT within 6 months of treatment in which adjuvant chemotherapy has been administered. If no ACT is required, we start RT within 5-6 weeks.
6. Oncological Outcomes
6.1 Margin Positivity
One of the potential advantages of TM is wide margins of excision, thus, achieving lower rates of re-excision (Singh and Losken 2012). According to the NCCN guidelines, “ no ink on margin” for invasive tumors and >2mm clear margins for DCIS are acceptable for negative margins (McIntosh et al. 2007). Literature reports indicate rates of positive margins (i.e., tumor extending to the inked surface) range from 0-36% with institutions reporting a 0% margin rate after conducting intra-operative frozen section analysis (McIntosh et al. 2007). When negative margins were considered as >2mm, the reported margin positivity rate was 8-16 % (Potter et al. 2020). In the TEAM protocol, 79% cases (of reported 385 TM procedures) have clear margins (O’Connell et al. 2018). We observed lower rates of margin positivity in our TM cohort which was consistent with previous reports (Silverstein et al. 2015a).
When margins are found to be positive following OBS, some units advocate a re-excision, while completion mastectomy is the procedure choice in the others (Savalia and Silverstein 2016). Further, based on the tumor biology, a RT boost to the tumor bed is another option for close margins (Ho et al. 2017). Re-excision in a case of OBS is challenging due to glandular re-arrangement during mammoplasty and should be considered carefully after discussing within the MDT, if the operating surgeon is confident of identifying the tumor bed and orientation (Jassem 2017).
In our study, only 3(1.7%) patients were reported to have close margins. Re-excision of margins were carried out in one patient, one patient underwent completion mastectomy and one received a boost to the tumour bed.
We attribute these encouraging results to our strict surgical SOPs as follows:
Careful placement of marking so that those closures are not tight
Maximum excision of the tumour achieved through one limb of the incision
Access to axilla through the same incision by identifying the lateral border of the Pectoralis major and minor. The Supero-lateral area and the lateral pillar is mobilized carefully to prevent devascularization from the lower lateral segment.
Sentinel lymph node biopsy performed through the same incision either with a nuclear dye or ICG
For sentinel node positive status, axillary dissection again carried out through the same incision.
Analysis of all tumor margins on frozen section and by a specimen mammogram.
Delay in breast restoration until the results on frozen section are negative.
Perform contralateral reduction while analysis of frozen sections is ongoing
Undertake interruptive sutures at the ‘T’ junction instead of continuous sutures to minimize necrosis.
6.2 Loco-regional Recurrence
In general, OBS is applicable in tumour sizes which are larger relative to patients that undergo traditional BCS (28350649)). Even though loco-regional recurrence has been attributed to failure of local control, recent reports indicate influence of tumour biology and size at presentation (De La Cruz et al. 2016).
In our study cohort, 66% BC patients were in Stage 2/3 and 46% were deemed high risk based on tumour biology (i.e, Her2 positive and TNBC status). These observations were in concurrence with reports that indicate 29-52% of BC cases in India are diagnosed at Stage 3 at initial presentation (Monica and Mishra 2020).
Hence, it was logical to expect a higher local recurrence rates with larger tumours. In our study, we observed 4 cases of local recurrences (2.3%) and 12 cases of distant metastases at 60 months of follow up (7%). Our results are consistent with previous reports of local recurrence rate of 3% and distant recurrence rate of 13%, with an overall survival rate of 92.5% over a median follow-up of 74 months (Rietjens et al. 2007). Based on these oncological outcomes, we conclude that TM is a oncologically safe procedure even in high-risk patients
7. RT related
In our opinion, in majority TM cases, margins around the tumor bed due not shift significantly due to following reasons:
During TM, adequate care is taken to check whether tumor bed is well delineated with markings by Liga clips, as soon as tumor is removed.
In some cases, the margins may get advanced into the tumor cavity to form the bed of the tumor cavity (such as in an extended inferior pedicle). Herein, for dealing with the tumor in the superior quadrant, the lower margin (which is the highest point of the extended pedicle) shifts into the tumor cavity, where exactly the boost is required.
3. In simple mammoplasty (or tumor in lower quadrant or superior quadrant), in which the tumor is in a tissue segment within the specimen, it is likely that some of the margins may shift into the tumor cavity but not shift away from it.
4. If the tumor is lying outside (i.e., in outer quadrant or supero-medial quadrant) and if the excision is large, central mound advancement can be performed to fill up these cavities. In this situation, even if the infero-medial margin may shift, being a supero-medial margin, but it will not go outside the tumor cavity.
5. For cavity on the outer side, if a dual pedicle technique is applied, even then inferior pedicle will be used only to fill in the gap.
Guidelines for optimal RT planning after TM are unclear and further methodical investigations are needed. Indeed, results are eagerly awaited from the MIAMI trial which is the first randomized trial design to address the clinical safety of TM associated with the excision of each cancer and the possibility of performing up to two tumor bed(s) boost(s) radiotherapy (ClinicalTrials.gov Identifier: NCT03514654).
Patient Reported Outcome Measures (PROMS)
In order to evaluate the patient acceptance of TM and improvement in QoL, we utilized Breast Q, a standard validated tool for assessment of patient reported outcome measures (PROMs). Previous reports have indicated that satisfaction with breasts was better in women who underwent OBS than in those who underwent a BCT alone (Dave et al. 2016).
Overall, we report high levels of satisfaction on PROMs, which is expected, as the aim of TM is to provide an aesthetically pleasing breast. In our study (Figure 4), a comparison of the PROMs amongst the 3 types of mammoplasties (i.e, simple, complex and extreme oncoplasty) demonstrates almost equal scores indicating that even complex techniques are well accepted. We have previously reported that in BC patients that have undergone mastectomy and immediate breast reconstruction, the lowest response rate was for ‘sexual well-being’ (Shekhawat et al. 2015; Koppiker et al. 2019b). It is well known that a cancer patient may suffer from sexual dysfunction, which is often under-reported. In the current study, we report a higher mean score of 75.3 for sexual wellbeing. This may be attributed to better body image and self-esteem arising from the satisfactory outcomes from TM procedure and contralateral reduction mammoplasty.
Our encouraging results could be credited to a multitude of factors at our institution such as adequate counselling, high level of patient involvement in the decision-making process, surgical expertise, lower complication rates, personalised hospital services and optimal post-operative care for a long duration.
Our study focus was to evaluate patient’s perception of the aesthetic results, which quite often are different than a clinician’s perspective. In support of the PROMs, independent assessment by 3 different surgeons indicated that over 90% cases exhibited good-to-excellent cosmetic outcomes
CONCLUSION
Our study represents a first detailed report on surgical, oncological and PROMs outcomes after TM surgery in Indian BC patients as observed in a single breast oncoplasty institution. We conclude that our TM technique(s) is best suited for even advanced stage patients with moderate-to-large breasts with mild/severe ptosis.
In general, our study observations are compliant with the guidelines of TEAM protocol except few non-compliances such as lack of MRI which has poor uptake in India due to cost barriers. Our conclusions are supported by availability of large study cohort, detailed surgical methodology, thorough data collection in pre-, intra and post-surgery phases along with PROMs and long-term follow-up. Furthermore, TM procedure may not be applicable for smokers, severe diabetics and morbidly obese women. In general, TM should not be performed if the patient does not consent for bilateral symmetrisation. Our PROMs data indicates excellent acceptance of the TM procedures as indicated by data from patient satisfaction even after RT regimens. These positive outcomes are well-attributed to detailed counseling of patients during various stages of their clinical management.
It may be inaccurate to extrapolate the study findings to the general Indian population due to the large variability in socio-cultural, psychological and economical ground realities across the country. Similar TM-focused studies from other Indian breast units will be needed in future to corroborate the observations from our study. Indeed, SOPs from our study inclusive of surgical techniques and PROMs would be useful for replications by other breast surgeins. However, it should be noted that only few breast units in India offer such OBS surgery choices due to paucity of well-trained breast surgeons. Therefore, anticipating this need, we have established special training initiatives for aspiring OBS surgeons in India. If the techniques and outcomes of OBS are popularized and the broad indications of TM are clearly defined, it is possible that more eligible BC patients will receive the benefits of this procedure over the alternative breast surgery options.
Data Availability
The study investigators would like to state that all data related to the manuscript will be available for further review on request after consultation with institutional ethics committees
CONSENT
The study was approved by an Independent Ethics Committee. All subjects gave their consent for the use of their personal and medical information including images in the publication of this study.
CONFLICT OF INTEREST STATEMENT
The author declares no competing interests.
ACKNOWLEDGEMENT
The study authors would like to thank all participants who consented to participate in this study. We acknowledge Bajaj Auto Ltd. for providing support to research activities at Prashanti Cancer Care Mission, Pune. We are grateful to the MAPI Research Trust for permission to use BREAST-Q (http://www.mapitrust.org) and the support from the management and staff of Ruby Hall Clinic, Pune where all surgeries were performed.
Footnotes
Email: dr.nutang{at}gmail.com; lalehBusheri{at}gmail.com; sgdixit{at}gmail.com; pragnyac89{at}gmail.com; dr.gautamsharan{at}gmail.com; upendradhar{at}hotmail.com; dr.harikiran89{at}gmail.com; smeetanare{at}hotmail.com, snehajoshipimpalkhare{at}gmail.com, n.sanket13{at}gmail.com,
ABBREVATIONS (arranged alphabetically)
- BC
- Breast Cancer
- BCS
- Breast Conservation Surgery
- BCT
- Breast Conservation Therapy
- DCIS
- Ductal Carcinoma In situ
- EO
- Extreme Oncoplasty
- IDC
- Intraductal Carcinoma
- NAC
- Nipple Areolar Complex
- OBS
- Oncoplastic Breast Surgery
- PROMs
- Patient Reported Outcome Measures
- QoL
- Quality of Life
- RT
- Radiation Therapy
- SIB
- Simultaneous Integrated Boost
- TRM
- Therapeutic Reduction Mammoplasty
- UOQ
- Upper Outer Quadrant




{kind=link}
{kind=link}
{kind=link}