
ABSTRACT
Background Vaccine hesitancy in the U.S. may limit the potential to alleviate the public health threat caused by the COVID-19 pandemic.
Methods We estimated trends in and correlates of vaccine hesitancy, and its association with subsequent vaccine uptake among 5,085 United States adults from the CHASING COVID Cohort study, a national longitudinal study. Trends in willingness to vaccinate were examined longitudinally in three rounds of interviews from September to December 2020. We assessed correlates of willingness to vaccinate in December 2020. We also estimated the association between willingness to vaccinate in December 2020 and subsequent vaccine uptake in February 2021.
Results Vaccine hesitancy and resistance decreased from 51% and 8% in September 2020 to 35% and 5% in December 2020, respectively. Compared to Non-Hispanic (NH) White participants, NH Black and Hispanic participants had higher adjusted odds ratios (aOR) for both vaccine hesitancy (aOR: 3.3 [95% CI: 2.6, 4.2] for NH Black and 1.8 [95% CI: 1.5, 2.2] for Hispanic) and vaccine resistance (aOR: 6.4 [95% CI: 4.3, 9.4] for NH Black and 1.9 [95% CI: 1.3, 2.7] for Hispanic). Willingness to vaccinate was associated with lower odds of vaccine uptake among 65+ year olds (aOR: 0.4, 95% CI: 0.3, 0.6 for hesitancy; aOR: 0.1, 95% CI: 0.01, 0.6 for resistance) and healthcare workers (aOR: 0.2, 95% CI: 0.1, 0.3 for hesitancy; aOR: 0.04, 95% CI: 0.006, 0.2 for resistance).
Conclusions Awareness and distribution efforts should focus on vaccine hesitant vulnerable populations.
INTRODUCTION
As the coronavirus disease-19 (COVID-19) pandemic continues to be a health crisis globally, widespread vaccination is the most effective and sustainable long-term mitigation strategy. Thirteen safe and efficacious vaccines were developed and authorized worldwide within a span of a year since the World Health Organization (WHO) declared the COVID-19 outbreak a pandemic.1 In the United States (U.S.), the three vaccines currently authorized for emergency use are the Pfizer-BioNTech BNT162b2 vaccine2, the Moderna mRNA-1273 vaccine3, and the Janssen Ad26.COV2.S vaccine.4 The Pfizer-BioNTech and the Moderna vaccines are both 2-dose mRNA vaccines, while the Janssen vaccine is a single dose, non-replicating viral vector vaccine. Forty-six percent of the U.S. population has received at least one dose and 34% have been fully vaccinated as of May 9, 2021; however vaccination rates vary by state and county.5 As vaccine eligibility criteria expand and coverage increases, we can expect dramatic reductions in COVID-19 incidence, hospitalizations, and mortality.6
For the COVID-19 vaccination program to be as impactful as possible, large numbers of people must be vaccinated quickly while also ensuring equity in access and uptake. Low vaccine acceptance and lack of easy access to vaccinations in vulnerable populations can be barriers to achieving both high and equitable vaccination coverage.7 This could create vaccination cold-spots where periodic disease outbreaks can still occur8 and vaccine-resistant strains might evolve.9 While the anti-vaccine sentiment remains a threat to COVID-19 vaccine uptake in the U.S., other factors, such as political mistrust, lack of assurance about safety and efficacy, and a lack of clear public health messaging may have influenced vaccine hesitancy specifically for the coronavirus vaccines.10 That COVID-19 vaccines became available in less than a year may have engendered concerns among the public, considering the average vaccine development timeline is around ten years.11 According to a Kaiser Family Foundation poll from August 2020, a majority (62%) believed that sociopolitical factors and pressures may have led to a rushed approval for the COVID-19 vaccine without the assurances of safety and efficacy, and only 42% of the participants were willing to get the COVID-19 vaccine if approved before the U.S presidential elections in November 2020.12 Based on a systematic review of surveys conducted between April and October 2020, the U.S. recorded lower COVID vaccine acceptance (ranging from 38% to 49% in different regions) compared to other developed countries such as Denmark (80%) and the UK (79%).13
Understanding COVID-19 vaccine hesitancy and addressing it promptly is essential to a successful and equitable vaccine roll-out. In this study, we aimed to: 1) measure trends in vaccine hesitancy in the U.S. for adults; 2) identify subpopulations that might be less willing to be vaccinated; 3) examine COVID-related risk perceptions and behavioral factors that correlate with vaccine hesitancy; and finally, 4) assess the association between vaccine hesitancy and subsequent vaccine uptake.
METHODS
Study design and participants
This study was performed using data from the Communities, Households, and SARS-CoV-2 Epidemiology (CHASING) COVID Cohort study, which is a national prospective cohort study in the U.S. launched on March 28, 2020 to understand the spread and impact of the SARS-CoV-2 pandemic within households and communities. Details of survey methodology are described elsewhere.14 Briefly, study participants were recruited through social media platforms or through referrals using advertisements that were in both English and Spanish. Eligible participants were >=18 years old U.S. residents with a valid ZIP code and email address. As of May 9, 2021, 7 full survey rounds (Visit 0 [V0] to Visit 6 [V6]) were completed which captured longitudinal information on participant demographics, COVID-related exposures, outcomes, detailed symptoms, non-pharmaceutical intervention use, vaccine uptake, and other behavioral factors (Appendix Fig 1). For this study, we included participants who responded to vaccine-related questions starting at V3 (September 2020), which we treated as our baseline response for the longitudinal analysis. Participants were not excluded for missing subsequent surveys. The study was approved by the Institutional Review Board at the City University of New York (CUNY).

Number of participants who responded that they would immediately get the vaccine (green), delay getting the vaccine (pink), or never get the vaccine (blue) when it becomes available to them are depicted in each rectangular node with the width of flows proportional to how many individuals report that response. Plot shows how their responses varied from September (V3) to subsequent surveys in November (V4) and December (V5). Only participants who responded at all three time points are included in this plot. Of 2,302 participants who initially responded as vaccine hesitant in V3, 1,110 (48.2%) reported that they would immediately get the vaccine when it comes available to them in the V5 round (December 2020). Of the 353 participants who responded as vaccine resistant in V3, 171 (48.4%) continued to indicate resistance by V5, 167 (47.3%) changed to vaccine hesitant, and 15 (4.2%) reported that they would now immediately get the vaccine. Of 1,822 participants who reported that they would immediately get the vaccine when available to them in V3, 228 (12.5%) changed to being vaccine hesitant or resistant by V5.
Outcome definitions and ascertainment of willingness to vaccinate from V3-V5 and vaccine uptake at V6
In three surveys V3-V5 (September - December 2020) (Appendix Fig 1), we assessed participants’ willingness to vaccinate with the question “If a coronavirus vaccine became available would you: a) Immediately get the vaccine; b) Delay getting the vaccine; c) Never get the vaccine.” Those who responded that they would “Delay getting vaccine” were categorized as vaccine hesitant and those who responded that they would “Never get the vaccine” as vaccine resistant. The outcome, ‘willingness to vaccinate’, had three levels: vaccinate immediately, vaccine hesitant, vaccine resistant. Participants were asked if they were part of a vaccine trial (V3, V5) and about their perceptions of herd immunity (V3).
When the vaccine became available to healthcare workers and high-risk individuals, in December 2020 (V6), we queried vaccination uptake (“Have you been vaccinated against COVID-19 with an FDA approved vaccine/not in a vaccine trial: a) Yes; b) No; c) Don’t know/Not sure”), as well as about vaccine-related side effects, motivation for getting vaccinated, and reasons for delay. The outcome, ‘vaccine uptake’ at V6 was coded dichotomously (yes or no).
Demographic characteristics
Participant age, race, ethnicity, income, education, and essential worker and healthcare worker status was determined at enrollment (V0, V1). Essential worker and healthcare worker status was asked again at V3 and the most recent reported status was assessed. Essential workers included anyone who reported working in law enforcement, emergency management, retail, delivery, transportation, agriculture, or school/daycare/childcare. Self-reported race/ethnicity was coded based on standardized OMB categories.15
Ascertainment of other exposures at V0-V5
To assess the effect of prior exposure to COVID-19 on willingness to vaccinate, we defined COVID-19 history as a dichotomous variable using three inputs: self-reported COVID-19 PCR diagnosis or seropositivity (Y/N between V0 and V5), self-identifying as a COVID-19 long hauler (Y/N between V4 and V5), or being seropositive for COVID-19 antibodies in tests performed for as part of our study between May and October. To measure COVID-19 risk perception, we asked participants if they were worried that they would get sick from coronavirus, that their loved ones would get sick from coronavirus, and that coronavirus will overwhelm hospitals (not at all worried, not too worried, somewhat worried, very worried). COVID-19 related anxiety was measured using the Generalized Anxiety Disorder-7 (GAD-7) scale, and participants were categorized as having “no/low anxiety” or “moderate/high anxiety” based on their median scores. We asked whether participants thought social distancing was practiced by most in their community (Y/N), and if they felt that the federal government was prioritizing the safety of citizens during the pandemic (agree/disagree/neutral).
To understand if vaccine hesitancy was correlated with the use of other non-pharmaceutical interventions (NPIs) we drew on participants’ responses to questions about their mask use and social distancing in public places at V5 (Specific questions in table 2). We assigned a score of 1 for responses that indicated lack of participant engagement with individual NPIs and 0 otherwise. We summed the coded behaviors to create a risk score. Participants engaging in 3 or more risk-taking activities (median risk score=3) were considered to be engaged in higher risk behavior. We separately assessed whether mask use and air travel anytime between V0 and V5 were associated with willingness to vaccinate at V5.
Statistical analysis
Chi-squared tests and corresponding p-values were used to describe the distribution of patient characteristics across willingness to vaccinate levels at V5. Mean change in willingness to vaccinate over time was assessed using the McNemar-Bowker test. Models were implemented within the ‘multgee’ and ‘nnet’ packages in R version 4.0.1.
Missing data
Participants who reported receiving the vaccine at V5 were not asked about willingness to vaccinate again in the survey (n=63). We imputed their outcome as “Immediately get the vaccine” assuming that if they received the vaccine at V5 they were willing to get it immediately. A small number of participants skipped the questions about vaccine hesitancy and were dropped (n=8 in V3, n=5 in V4, no one missing in V5). Missingness in willingness to vaccinate due to loss to follow up between V3 and V5 (n=518, [10.2%]) was not associated with outcome in V3. We assumed data missing due to loss to follow-up (LFTU) were Missing at Random and did no further imputation.
Changes in willingness to vaccinate between V3 and V5
Multinomial Generalized Estimating Equations (GEE) models were used to measure changes in the ‘willingness to vaccinate’ outcome over time between September (V3) and December (V5) by estimating odds ratios (OR) and 95% confidence intervals, adjusted for age, gender, race, and comorbidities. We included an interaction term between race/ethnicity and calendar time of interview in the model to test the hypothesis that the rate of change of vaccine hesitancy differed by race/ethnicity as found in some studies.16 Longitudinal correlation between participants was specified using an independence correlation matrix and variance was estimated using robust variance estimators.
Correlates of willingness to vaccinate at V5
Factors associated with willingness to vaccinate were drawn only from V5 because it is the closest time point at which hesitancy was measured before vaccines were rolled out, and hence the most relevant. To examine the determinants of willingness to vaccinate at V5 (December 2020), we performed multinomial logistic regression to estimate odds ratios (OR) and 95% confidence intervals (CI). Separate models were built to assess the effects of sociodemographic factors, COVID-19 history, behavioral characteristics, and COVID-19 risk perception respectively on willingness to vaccinate. Models were adjusted for sociodemographic factors that were statistically significantly associated with the outcome (p<0.05).
Association between willingness to vaccinate at V5 and vaccine uptake at V6
Associations between willingness to vaccinate in participants aged 65+ and healthcare workers (the only groups vaccine-eligible nationwide when survey V6 was administered) and the outcome of vaccine uptake were assessed using logistic regression models, which estimated odds ratios (OR) and 95% CI. Both models were adjusted for demographic characteristics, comorbidities, and prior COVID history. Participants who indicated they were enrolled in a vaccine trial at any visit were excluded (N=296).
RESULTS
A total of 5,085 participants were asked about willingness to vaccinate in the baseline September survey (V3), of whom 4,778 (93.9%) were retained in the November (V4) and 4,569 (89.8%) in December (V5) rounds. Both vaccine hesitancy and resistance decreased significantly over time (sTable 1), and there was substantial movement across groups in both directions (e.g., from hesitant to immediate and vice-versa, Figure 1).
Of the cohort participants who responded to the vaccine-related question at V5 (n=4,569), 59.6% said they would immediately get the vaccine, 34.9% were vaccine hesitant, and 5.5% were vaccine resistant (Table 1). Participants who were vaccine hesitant or resistant at V5 were more likely to be non-Hispanic (NH) Black, younger (18-39 years old), female, have low income, and less likely to have a college education.
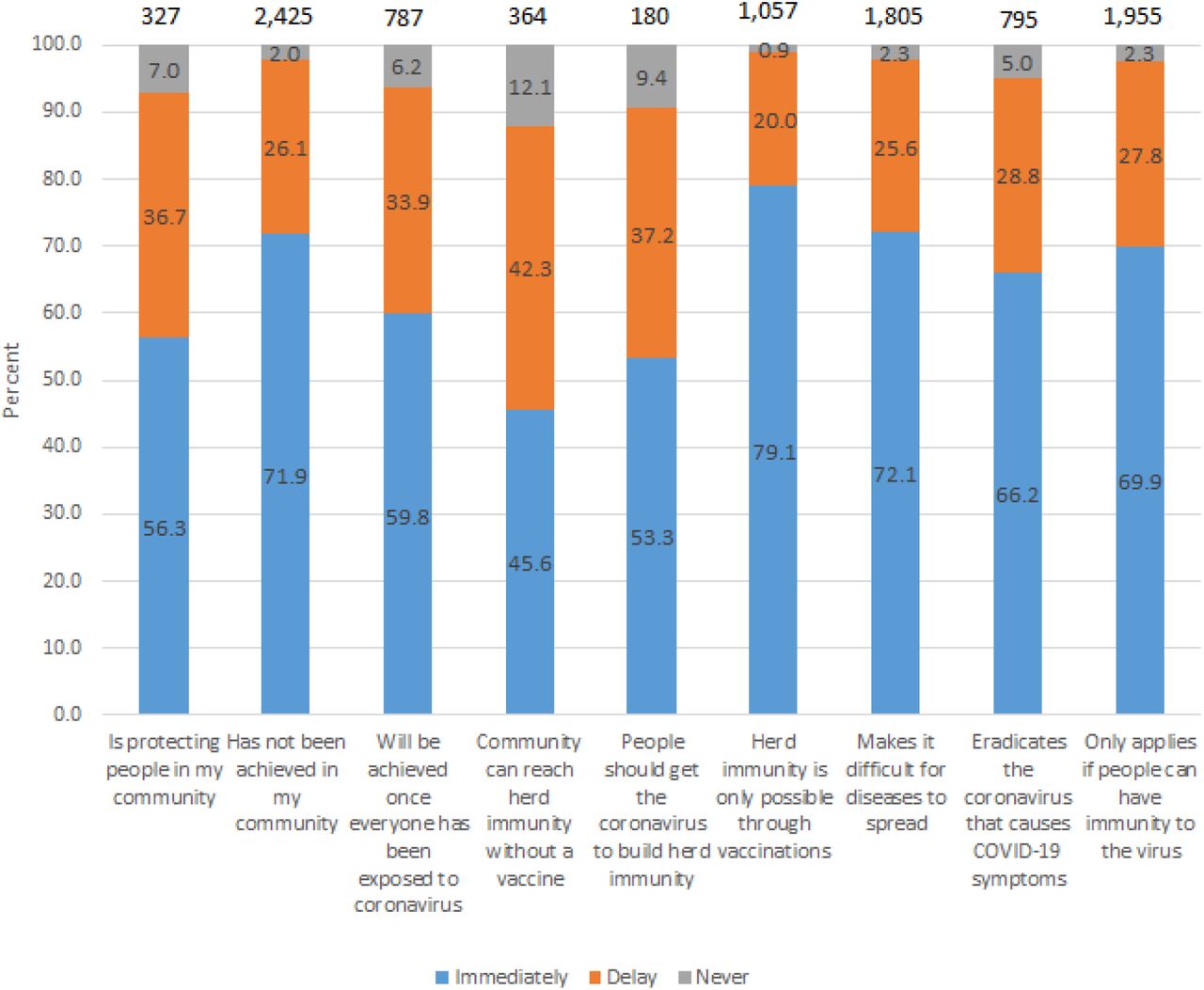
Most participants believed that herd immunity had not yet been achieved in their community (n=2,425) and 1,057 (22.4%) thought that herd immunity was only possible through vaccinations. Only a third (n=1,805) responded that herd immunity is required to slow down transmission and 795 (15.6%) thought that it will eradicate coronavirus. A small proportion (3.8%) felt that people should get the coronavirus to build herd immunity and 787 (10.6%) believed that herd immunity will be achieved once everyone has been exposed to coronavirus. (Figure 2).
{kind=link}
{kind=link}
Among participants who report specific beliefs about herd immunity, this stacked bar graph shows percentage that indicate that they would immediately get the vaccine (blue), delay getting the vaccine (orange), or never get the vaccine (grey). The number of participants who responded to the question is displayed on top of the bars and participants could select more than one option.
Trends in willingness to vaccinate
Overall, vaccine hesitancy decreased by 66% (aOR: 0.34, 95% CI: 0.31, 0.37) and vaccine resistance by 63% (aOR: 0.37, 95% CI: 0.32, 0.44) between September and December, adjusted by race/ethnicity, age, gender, and comorbidities (Table 2). Even though vaccine hesitancy and resistance decreased overall, the rate of change differed by race/ethnicity. In November compared to September, NH Black participants were 1.7 times (95% CI: 1.4, 2.1) more likely to be vaccine hesitant compared to NH White participants. By December, they were 2.8 times (95% CI: 2.1, 3.6) more likely to be vaccine hesitant compared to NH Whites. Hispanic participants were 1.1 times (95% CI: 0.9, 1.8) more likely than NH White participants to be vaccine hesitant in November compared to September. But by December, they were 2.1 times more likely to be vaccine hesitant (95% CI: 1.6, 2.4) compared to those NH White. Similar trends were observed for vaccine resistance but results were not statistically significant.
Correlates of willingness to vaccinate at V5 (December 2020)
Compared to NH White participants, adjusted odds ratios (aOR) for vaccine hesitancy were 3.3 (95% CI: 2.6, 4.3) for NH Black, 1.8 (95% CI: 1.5, 2.1) for Hispanic, and 1.3 (95% CI: 1.04, 1.7) for Asian/Pacific Islander/Alaskan Native participants (Table 3, Model 1). Male gender, older age, higher income, and college education were associated with lower odds of vaccine hesitancy in the adjusted model. Essential workers had lower odds compared to non-essential workers (aOR: 0.85, 95% CI: 0.7, 1.01) of being vaccine hesitant, adjusted for demographic factors mentioned above, and additionally for comorbidities and prior COVID-19 infection. Healthcare workers also had lower odds of vaccine hesitancy (aOR: 0.8, 95% CI: 0.6, 0.96) compared to non-healthcare workers. (Table 3, models 2 and 3).
Those with a history of COVID-19 (Had a prior PCR diagnosis, self-identified as a long hauler, or was tested seropositive in antibody testing done as part of the cohort) had greater odds of being vaccine hesitant (aOR: 1.19, 95% CI: 0.97, 1.4) compared to those without, adjusted for age, gender, race, income, and education. (sTable 2). Looked at separately, being seronegative was associated with lower likelihood of being vaccine hesitant (aOR: 0.7, 95% CI: 0.6, 1.02). Worry about themselves or their loved ones getting COVID-19 was associated with lower odds of vaccine hesitancy (aOR: 0.46, 95% CI: 0.4, 0.5) and vaccine resistance (aOR: 0.2, 95% CI: 0.1, 0.3), but COVID-related anxiety was not associated with either. Those who did not trust the federal government to prioritize the safety of citizens during the pandemic also were less likely to say they would delay the vaccine (aOR: 0.46, 95% CI: 0.4, 0.5) or refuse it (aOR: 0.16, 95% CI: 0.1, 0.2).
Participants who reported wearing a mask in the prior month had substantially lower odds of being vaccine hesitant (aOR: 0.24, 95% CI: 0.1, 0.4) and vaccine resistant (aOR: 0.06, 95% CI: 0.03, 0.1) (sTable 2). Recent air travel was also associated with lower vaccine hesitancy (aOR: 0.6, 95% CI: 0.5, 0.7). Those who engaged in more high-risk activities (such as not wearing masks consistently in public areas, not maintaining social distancing with non-household members, gathering in large groups) were more likely to be vaccine hesitant (aOR: 1.6, 95% CI: 1.4, 1.8) and vaccine resistant (aOR: 2.7, 95% CI: 2.0, 3.6).
Vaccine uptake at V6 among vaccine-eligible (65 years or older and healthcare workers as of February 2021)
Of the 568 participants in our sample who were 65+ years old at enrollment, 239 (42.1%) received at least one dose of coronavirus vaccine by February 2021 (V6). Among participants older than 65 years, vaccine hesitancy (aOR: 0.4, 95% CI: 0.3, 0.6), as well as vaccine resistance (aOR: 0.1, 95% CI: 0.01, 0.6), were associated with lower odds of vaccine uptake by V6, adjusted for race, sex, income, comorbidities, and prior COVID-19 infection (Table 4). Of the 519 healthcare workers, 283 (54.5%) received at least one dose of the vaccine by V6. Similar associations with vaccine uptake were observed for healthcare workers (aOR: 0.2, 95% CI: 0.1, 0.3 for hesitant participants and aOR: 0.04, 95% CI: 0.006, 0.2 for resistant participants). Vaccine uptake was lower among NH Black and Hispanic healthcare workers, but the association was not statistically significant.
Among unvaccinated participants who reported they would delay or never get the vaccine, the most frequently cited reasons for vaccine delay at V6 were concerns about long-term side effects (54.3%), a desire to have more information about the vaccine (42.8%), concerns about vaccine effectiveness (37.1%), and short-term side effects (35.6%). Reasons for delay did not vary by race/ethnicity. Among those willing to take the vaccine immediately, most (89.7%) responded that they wanted to be vaccinated to “avoid getting COVID-19”, end the pandemic (86.4%), protect themselves (84.5%), and protect others (80.7%).
DISCUSSION
Using a prospective cohort study, we measured trends in willingness to vaccinate among U.S. adults, factors associated with them, and the association between intention to vaccinate and subsequent vaccine uptake among those eligible early in the COVID-19 vaccine era. We found that vaccine hesitancy has decreased in our cohort over time since September 2020, but remained high at 39% in December 2020 when vaccines became available to select groups. Vaccine hesitancy and resistance differed by race/ethnicity, age, income, and education. Compared to NH Whites, cohort participants of all other races and ethnicities showed higher odds of vaccine hesitancy. While vaccine hesitancy decreased overall, it did so at a slower rate for participants of color compared to NH White participants, thereby widening the racial/ethnic gap in vaccine hesitancy over time. Importantly, in a subset eligible to vaccinate prior to their interview vaccine hesitancy and resistance were associated with lower subsequent vaccine uptake.
Given the wide spectrum over which vaccine hesitancy occurs 17, we differentiated between vaccine hesitancy and resistance to assess correlates of each separately. This delineation is important because the factors that drive vaccine hesitancy and resistance could be different, especially for the coronavirus vaccine, and public health policies will need to be tailored to each group to address their specific concerns. Vaccine hesitancy was more prevalent in the cohort compared to outright refusal and comparable to estimates from other U.S.-based surveys. 10,18–20 Similar to these studies we found age, sex, race/ethnicity, income, and education to be correlated with vaccine hesitancy. Communities of color, low income groups, and those with fewer years of education have experienced particularly high COVID-19 infection rates, hospitalization rates and mortality rates. 22–25 If vaccine uptake remains low in these groups, they may remain more susceptible to a higher COVID-19 burden.
Much has been published about racial/ethnic differences in vaccine hesitancy, and our findings were consistent with these studies.10,26–29 Even though overall vaccine hesitancy decreased with time, racial/ethnic gaps in vaccine hesitancy and resistance worsened. Distrust in the medical community has been an important theme, pertaining to not only COVID-19 vaccines but the healthcare system and medical research in general. Historical mistreatment, oppression, and unethical conduct from the government, medical establishments, and scientific research communities have adversely impacted racial and ethnic minorities, especially Black Americans.26,30,31 Studies have also shown racial disparities in vaccine uptake which indicate disparities in access.29 We also found lower vaccine uptake in NH Black and Hispanic populations among among healthcare workers, but this finding was not statistically significant, probably due to the small sample size of this subgroup. As vaccine eligibility expands, it will be important to assess if racial/ethnic disparities in vaccine hesitancy translate to disparities in uptake and if vaccine uptake remains low among minority individuals willing to vaccinate immediately. Future research should explore the nuances in the drivers of vaccine hesitancy among different racial and ethnic groups and inform a more equitable approach to vaccine implementation.
Our study found that participants with a known prior COVID-19 infection were more likely to be vaccine hesitant. People might believe they do not need a vaccine because they have prior immunity from natural infection. Based on the evidence that infection-derived immunity can wane over time 32, especially among those with mild or asymptomatic infections 33–35, the CDC recommends that people get vaccinated regardless of their infection history.36 There is also evidence that infection-induced immunity is not as robust as vaccine-induced immunity, and may not protect against reinfection with variants known to cause severe symptoms.37,38 Moreover, evidence suggests that the immune response to the first SARS-CoV-2 vaccine dose among those already infected is more robust compared to naive individuals with two vaccine doses.39 Thus, policy changes to requiring only one dose for those with evidence of prior infection might help increase vaccine uptake in these groups.
Among those who were eligible for the vaccine in December 2020 across most of the U.S., prior vaccine hesitancy and resistance were associated with low vaccine uptake. The main stated reasons for vaccine hesitancy in our cohort were needing more information, worry about short-term and long-term side effects, and concerns about vaccine effectiveness. Vaccine confidence could be increased in this group through targeted messaging about how short-term side effects are likely to be mild and serious long-term effects are extremely rare. Being transparent about the vaccine risks and investigating them immediately, like in the case of the Johnson & Johnson vaccine, can help ultimately increase public trust in regulatory bodies, even if it might result in increased hesitancy in the short term.40 Encouragingly, hesitancy decreased over time, probably as new information about vaccine safety and efficacy emerged and an increasing number of people got vaccinated without incident. To assuage concerns about effectiveness and safety, studies that estimate direct and population-level vaccine effects for the different coronavirus vaccines using real-world data in the U.S. are critical. That there were large differences in vaccine hesitancy/resistance by race/ethnicity, but no differences in the stated reasons for hesitancy/resistance suggests that public health messages around COVID-19 vaccinations are not reaching racial/ethnic groups equally.
Even though a majority of the participants understood that their community has not yet reached herd immunity thresholds, only a third responded that herd immunity is important to reduce transmission. Previous studies have shown that individuals with greater understanding and knowledge of herd immunity are more willing to vaccinate.41,42 In our study, we saw a similar trend where participants with more favorable views and a better understanding of herd immunity were more likely to say they would be vaccinated immediately. Educating the public about the nuances of herd immunity and the benefits of vaccine indirect effects can influence their decision to ultimately vaccinate 41.
The strengths of our study include prospective assessment of association between willingness to vaccinate and vaccine uptake, a diverse and geographically-representative cohort, and detailed data on demographics, biomarkers on prior COVID exposures, and behavioral characteristics that are not found in surveillance databases, electronic medical records, or polls. Due to the longitudinal nature of the study, we were able to assess individual-level changes in vaccine hesitancy over time. We are also well-positioned to assess how hesitancy correlates with actual vaccine uptake in the rest of our cohort in the coming months.
Our study also has limitations. Participants self-reported vaccination status as well as exposures, so the study is subject to misclassification and reporting bias. Because enrollment was done online, those without smartphones, computers, or a stable internet connection were less likely to be included. Sample sizes for the vaccine eligible subgroups were small. While we adjusted all models for demographic factors, there is a possibility of unmeasured/uncontrolled confounding. About 10% of our participants were LTFU between V3 and V5. While LTFU was not associated with the outcome, it was associated with age, sex, college education, serostatus, and COVID history, which could potentially bias our results.
In summary, even though coronavirus vaccine confidence has increased over time in our cohort overall, more than a third reported an intention to delay receiving the vaccine when it becomes available to them. Racial/ethnic gaps in vaccine hesitancy widened, despite overall decrease in hesitancy. To address these disparities, health education and awareness efforts should be better focused on vaccine hesitant low income and minority individuals to address vaccine-related concerns, and vaccine availability should be prioritized in communities where they reside to help ensure more equitable vaccine uptake. To mitigate the long-lasting impact of COVID-19 as a public health threat, it is important that no groups are left behind by vaccination initiatives.
Data Availability
All data referenced in the manuscript are available upon request.
FUNDING
Funding for this project is provided by The National Institute of Allergy and Infectious Diseases (NIAID), award number 3UH3AI133675-04S1 (MPIs: D Nash and C Grov), the CUNY Institute for Implementation Science in Population Health (cunyisph.org) and the COVID-19 Grant Program of the CUNY Graduate School of Public Health and Health Policy, and National Institute of Child Health and Human Development grant P2C HD050924 (Carolina Population Center). The NIH played no role in the production of this manuscript nor necessarily endorses the findings.
ACKNOWLEDGEMENTS
The authors wish to thank the participants of the CHASING COVID Cohort Study. We are grateful to you for your contributions to the advancement of science around the SARS-CoV-2 pandemic. We also wish to thank the other members of the CHASING COVID Cohort Study team, who have contributed their expertise throughout the study. We thank Patrick Sullivan and MTL for local validation work on the serologic assays for use with DBS that greatly benefited our study. We are also grateful to MTL Labs for processing specimen collection kits and serologic testing of our cohort’s specimens.
REFERENCES



