
Abstract
Background In children, SARS-CoV-2 is usually asymptomatic or causes a mild illness of short duration. Persistent illness has been reported; however, its prevalence and characteristics are unclear. We aimed to determine illness duration and characteristics in symptomatic UK school-aged children tested for SARS-CoV-2 using data from the COVID Symptom Study, the largest citizen participatory epidemiological study to date.
Methods Data from 258,790 children aged 5-17 years were reported by an adult proxy between 24 March 2020 and 22 February 2021. Illness duration and symptom profiles were analysed for all children testing positive for SARS-CoV-2 for whom illness duration could be determined, considered overall and within younger (5-11 years) and older (12-17 years) age groups. Data from symptomatic children testing negative for SARS-CoV-2, matched 1:1 for age, gender, and week of testing, were also assessed.
Findings 1,734 children (588 younger children, 1,146 older children) had a positive SARS-CoV-2 test result and calculable duration of illness within the study time frame. The commonest symptoms were headache (62.2%) and fatigue (55.0%). Median illness duration was six days (vs. three days in children testing negative), and was positively associated with age (rs 0.19, p<1.e-4) with median duration of seven days in older vs. five days in younger children.
Seventy-seven (4.4%) children had illness duration ≥28 days (LC28), more commonly experienced by older vs. younger children (59 (5.1%) vs. 18 (3.1%), p=0.046). The commonest symptoms experienced by these children were fatigue (84%), headache (80%) and anosmia (80%); however, by day 28 the median symptom burden was two. Only 25 (1.8%) of 1,379 children experienced symptoms for ≥56 days. Few children (15 children, 0.9%) in the negatively-tested cohort experienced prolonged symptom duration; however, these children experienced greater symptom burden (both throughout their illness and at day 28) than children positive for SARS-CoV-2.
Interpretation Some children with COVID-19 experience prolonged illness duration. Reassuringly, symptom burden in these children did not increase with time, and most recovered by day 56. Some children who tested negative for SARS-CoV-2 also had persistent and burdensome illness. A holistic approach for all children with persistent illness during the pandemic is required.
Funding Engineering and Physical Sciences Research Council (EPSRC), National Institute for Health Research (NIHR), Medical Research Council (MRC), Zoe Global Limited, The Wellcome Trust, Alzheimer’s Society.
Evidence before this study SARS-CoV-2 in children is usually asymptomatic or manifests as a mild illness of short duration. However, anecdotal cases have raised concerns of prolonged illness in children, with no clear resolution of symptoms several weeks after onset, as is observed in some adults. How common this might be in children, the clinical features of such prolonged illness in children, and how it might compare with illnesses from other respiratory viruses (and with general population prevalence of these symptoms) is unclear.
Added value of this study We provide systematic description of COVID-19 in school-aged children. Our data, collected in a digital surveillance platform through one of the largest citizen science initiatives, show that long illness duration after SARS-CoV-2 infection in school-aged children does occur, but is uncommon. Only a small proportion of children have illness beyond four weeks; and the symptom burden in these children usually decreases over time. Most children resolve all symptoms by eight weeks, providing reassurance about long term outcomes. Importantly, symptom burden does not outnumber that observed in long illness due to causes other than SARS-CoV-2 infection.
Implications of all the available evidence Our results confirm that COVID-19 illness in children and adolescents is resolved in the community, after short duration, low symptom burden and with no need of hospitalization in most cases. Our findings also highlight that allocation of appropriate resources will be necessary for any child with prolonged illness, whether due to SARS-CoV-2 infection or other illness. Our study provides timely and critical data to inform discussions around the impact and implications of the pandemic on UK paediatric healthcare resource allocation.
Introduction
To date, the COVID-19 pandemic has resulted in >120 million cases of infection and 2.5 million deaths globally,1 with widespread health, economic, and social chaos. In adults, severe acute respiratory syndrome-related coronavirus 2 (SARS-CoV-2) causes a predominantly respiratory illness2 of median duration 11 days.3 In contrast, children with SARS-CoV-2 infection are often asymptomatic (43%-68%4) or have relatively mild symptoms, most commonly cough and fever;4–9 and life-threatening illness or death is rare. 1,575 children (aged 0-17 years) hospitalised in England from 19 March 2020 to 3 March 2021 tested positive for SARS-CoV-2, noting that COVID-19 was not necessarily the reason for hospitalisation,10 and 29 deaths due to COVID-19 were reported in children and young people across the UK from 1 March 2020 to 29 January 2021 (0-9 years: seven deaths; 10-19 years: 22 deaths, 0.19% and 1.98% respectively of estimated all-cause deaths during this time period11). The pandemic has also seen emergence of a new rare condition, multisystem inflammatory syndrome in children (MIS-C), typically presenting 2-4 weeks after acute SARS-CoV-2 infection.12
Some adults with SARS-CoV-2 infection experience prolonged duration of illness, known variably as Long COVID (LC),3,13 ongoing symptomatic COVID-19, post-COVID-19 syndrome or post-COVID condition.14,15 Data from the King’s College London (KCL) COVID Symptom Study (CSS),16 currently the largest citizen participatory epidemiological study in the UK with over >4.5 million UK participants, showed that 13.3% adults with a positive SARS-CoV-2 test had symptoms for ≥4 weeks (LC28) and 4.5% for ≥8 weeks (LC56).3 Predictors of LC28 included older age, female gender, and higher symptom burden in the first week of illness.3 Whether some children may also experience prolonged illness duration after infection with SARS-CoV-215 and, if so, how this compares with illness after infection with other respiratory viruses, is currently unclear.
In September 2020, coinciding with full re-opening of primary and secondary schools in the UK, governance for CSS data usage was extended to allow analysis of data from children (i.e., individuals aged <18 years). The UK subsequently experienced further waves of the pandemic (up to 30,000 new cases per day in November 2020 and 60,000 new cases per day in January 2021),1,17 with 29 December 2020 the peak date for new specimens testing positive over the entire pandemic to date.17 During this time, there was widespread testing availability for individuals with key symptoms of fever, cough and anosmia, in contrast to the very limited access during the first wave, when testing was mostly restricted to individuals presenting to hospital.18,19
Stay-at-home directives and school closures during these later waves resulted in unusually low incidences of commonly circulating viruses such as influenza, adenovirus, and respiratory syncytial virus over the 2020-21 UK winter, both generally and in school-aged children specifically.20 However, overlap in symptomatology meant many individuals (both adults and children) with respiratory illnesses other than COVID-19 were tested for SARS-CoV-2.
Here we report overall illness duration, individual symptom prevalence and duration, and symptom burden in UK school-aged children testing positive for SARS-CoV-2, whose data were logged through the KCL CSS. We provide similar data for symptomatic children tested for SARS-CoV-2 but who were negative, during the same period. Lastly, we present the prevalence and characteristics of long COVID in children.
Methods
Data were acquired within the COVID Symptom Study (CSS), through a mobile application launched jointly by Zoe Global Ltd. and KCL on 24 March 2020.16 Briefly, individuals are prompted to report through a smartphone application and provide daily updates of their health status, symptomatology, any SARS-CoV-2 testing, vaccination, and health care access. Symptom assessment includes both direct questions for a list of symptoms (yes/no or other defined options, listed in Supplementary Table 1), and free-text entry.16 Adult contributors can also report as a proxy for other persons (children, spouses, elderly relatives, etc.). The relationship between the contributor and proxy-reported individual(s) is not solicited and there is no data linkage between the contributor and proxy-reported individual(s). Children aged 16-17 years can use the app directly as independent contributors or be proxy-reported by an adult.
UK data from school-aged children (aged 5-17 years) were available from the launch of the app to 22 February 2021, which latter date corresponds to eight weeks after the peak SARS-CoV-2 positive specimen date in the UK.17 Data were considered from launch of the app, and from 1 September 2020 (i.e., return-to-school). The cohort was analysed overall and within two age groups: younger children, aged 5-11 years, corresponding to primary school-aged children in the UK; and older children, aged 12-17 years, corresponding to secondary school-aged children in the UK (acknowledging that not all older teenagers attend school). Preschool-aged children (≤4 years) were not included in the current study.
Aligning with our previous publications in adults,3,16 children were considered symptomatic of COVID-19 if they were reported by proxy as having any of a specific list of symptoms associated with COVID-1916 (Supplementary Table 1), mainly informed by adult epidemiology,21 with first symptom(s) presenting within a timeframe of 1 week before and 2 weeks after confirmation of infection (either a SARS-CoV-2 polymerase chain reaction or a lateral flow test). Illness duration was calculated as time from first symptom(s) reported within the requisite time frame (having been previously asymptomatic) until time of recovery (defined as return to asymptomatic state or, if proxy-reporting ceased prior to logging of an asymptomatic report, time of final report). Individuals who had returned to asymptomatic state but for whom another symptomatic report was logged within one week of the last symptomatic report were considered as still being unwell from their initial presentation (i.e., allowing for waxing/waning of illness); calculation of illness duration incorporated these short periods of asymptomatic status. Individuals with reporting gaps longer than one week between symptomatic reports were excluded. Individual symptom prevalence and duration were assessed, with individual symptom duration calculated as time between the first and last report for that symptom. Symptom burden was calculated as the number of different symptoms reported at least once over a defined timeframe (during the first week, the first 28 days, at ≥28 days until end of illness, and over the entire duration of illness). Consistent with our previous study in adults,3 we termed illness with symptoms lasting longer than 28 days as LC28; and longer than 56 days, LC56. Thus, by virtue of data census dates LC28 could only be determined in proxy-reported children whose symptoms commenced on or before 24 January 2021, and for LC56 on or before 29 Dec 2020 (noting the peak positive specimen date in the UK was 29 December 202017).
Symptom profiles were also assessed in children with COVID-19 who presented for hospital-based care (presenting to the accident and emergency department or admitted to hospital), where presentation to hospital followed development of symptoms (i.e., when the positive SARS-CoV-2 test result was not a secondary finding in a hospitalised child).
Several additional direct symptom questions were added to the app on 4 November 2020 (Supplementary Table 2), some of which overlapped with existing questions (e.g., for cutaneous manifestations, questions on “rash” and “sensitive skin” were added to existing questions on “red welts”, “blisters”, and “sores”). These additional questions and resultant data are presented in Supplementary Table 2 and Supplementary Figure 1 respectively but were not included in illness duration or symptom burden calculations for the main analysis.
Free text reporting was also possible, across the entire period. Free text data were divided into themes using frequency of descriptive words; each item within the themes were subsequently independently scrutinised by two clinicians (MA, ELD) to ensure appropriate categorisation, and individuals reporting free text symptoms within those themes were then counted. Free text data are reported here as descriptive statistics (Supplementary Table 3) and were not included in calculating illness duration or symptom burden. Free text was also searched for specific neurological terms of interest (e.g., weakness, difficulties with balance, paralysis, seizures, fits, convulsions, paroxysms, tics) and symptoms potentially affecting attention, behaviour, learning, and school performance (e.g., anxiety, irritability).22 Symptoms already assessed by direct question (Supplementary Table 1) were excluded from the free text search, to avoid duplication.
Symptom profile and duration were also assessed in children who were tested but had a negative result for SARS-CoV-2. The same parameters regarding test timing relative to symptom onset were applied as for children with a positive test result. Illness duration and symptom profile were determined in a randomly selected control cohort of these children (matched 1:1 for age, gender, and week of testing), and compared to children with a positive test.
Proxy-reporting density (defined as the number of episodes of proxy-reporting over the duration of illness) and persistence (defined as proxy-reporting until return to healthy state) were also determined.
Prevalence data for common winter circulating viruses were obtained from the Public Health England weekly national influenza and COVID-19 surveillance report.20
Data are presented using descriptive statistics. Results are presented as median with interquartile ranges. Due to rarity (with most percentages less than 5%) confidence intervals were calculated using Poisson distribution. Comparisons of data between groups used Wilcoxon signed-rank test or Chi-squared test/Fisher’s exact test, as appropriate. Spearman correlation testing (which does not require Gaussian distribution of the data) was used to assess correlation of illness duration with age.
Ethics approval for this study was granted by the KCL Ethics Committee REMAS ID 18210, review reference LRS-19/20-18210 and all participants (here, the proxy-reporting adult) provided consent.
Results
Across the UK, 258,790 children aged 5-17 years were reported by proxy between 24 March 2020 and 22 February 2021, with a positive SARS-CoV-2 test result reported in 6,975 children. Among those, 1,912 (666 younger and 1,246 older) children had a calculable duration of illness with requisite logging frequency (at least once weekly). As only 36 children had illness onset prior to 1st September 2020, and as there was very limited community access to testing early in the UK pandemic experience,19 analyses of illness duration and symptom profiles were restricted to children with illness onset after 1 September 2020. Further, illness onset had to commence on or before 24 January 2021 to allow sufficient time for symptom duration ≥4 weeks to be evident, as per LC28 definition.3 Thus, overall, 1,734 children (588 younger children, 1,146 older children) had a calculable illness duration within the requisite time frame. Similarly, 1,379 individuals (445 younger; 934 older children) had symptoms commencing on or before 29 December 2020, allowing sufficient time for symptom duration ≥8 weeks to be evident, as per LC56 definition.3 A flow chart showing inclusion/exclusion steps is shown in Figure 1.

Legend: overall number for the entire cohort of children is given first; numbers within brackets separated by oblique refer to younger children and older children in that order. ‘Not valid result’ – PCR test result proxy-reported as “failed test” or “still waiting”. ‘Duration calculable’ – illness onset within defined timeframe of testing for SARS-CoV-2, and with defined endpoint (for details, please see Methods). ‘Irregular logging’ – proxy-reporting with intervals of >7 days between proxy-reports during illness duration). ‘Illness onset outside of study bounds’ - symptom onset before 1 September 2020 or after 24 January 2021. ‘Hosp’ – presenting to hospital (either admitted to hospital or seen in Accident and Emergency ward).
Among 16- and 17-year-old individuals, 29,047 contributed self-logged data (447 reporting testing positive) compared to 32,271 reported by proxy (1,197 reported as testing positive). Illness duration could only be calculated in 10 self-logged 16- and 17-year-olds, compared with 381 proxy-logged 16- and 17-year-olds; and self-reporting and proxy-reporting of the same young person could not be excluded. Thus, only proxy-reported data are presented here.
Illness in children who tested positive for SARS-CoV-2
The median illness duration in children with COVID-19 was six days [IQR 3;11] (Table 1). Illness duration was significantly shorter in younger compared with older children (five [IQR 2;9] vs. seven days [IQR 3;12]) (Mann-Whitney U test p<1.e-5); and age correlated strongly with illness duration (rs 0.19, p<1.e-4).
The cohort of children with positive SARS-CoV-2 testing is presented here both as younger and older groups; and for usual (i.e., short) vs. extended illness duration.
Individual symptom prevalence and duration are shown in Table 2, Figure 2 and Figure 3. Overall, the most reported symptoms were headache (62.2% overall: 55.1% younger children, 65.9% older children) and fatigue (55.0% overall: 43.9% younger children and 60.7% older children). Subsequent symptoms ranked by frequency were fever (43.7%), sore throat (36.2%), abdominal pain (27.7%), and persistent cough (24.7%) in younger children; and in older children sore throat (51.0%), anosmia (48.3%), fever (34.6%), and persistent cough (26.0%). During the first week of illness, median symptom burden was three [IQR 2;6] overall (three [IQR 2;5] symptoms in younger children, four [IQR 2;6] in older children). Sixteen younger children and 21 older children who tested positive for SARS-CoV-2 subsequently attended for hospital care. The symptom profiles of children attending hospital compared with children managed in the community are shown in Supplementary Figure 2. No formal statistical comparisons were undertaken between hospital and community cases, given the low numbers of hospital attendees.


Long illness duration in children who tested positive for SARS-CoV-2
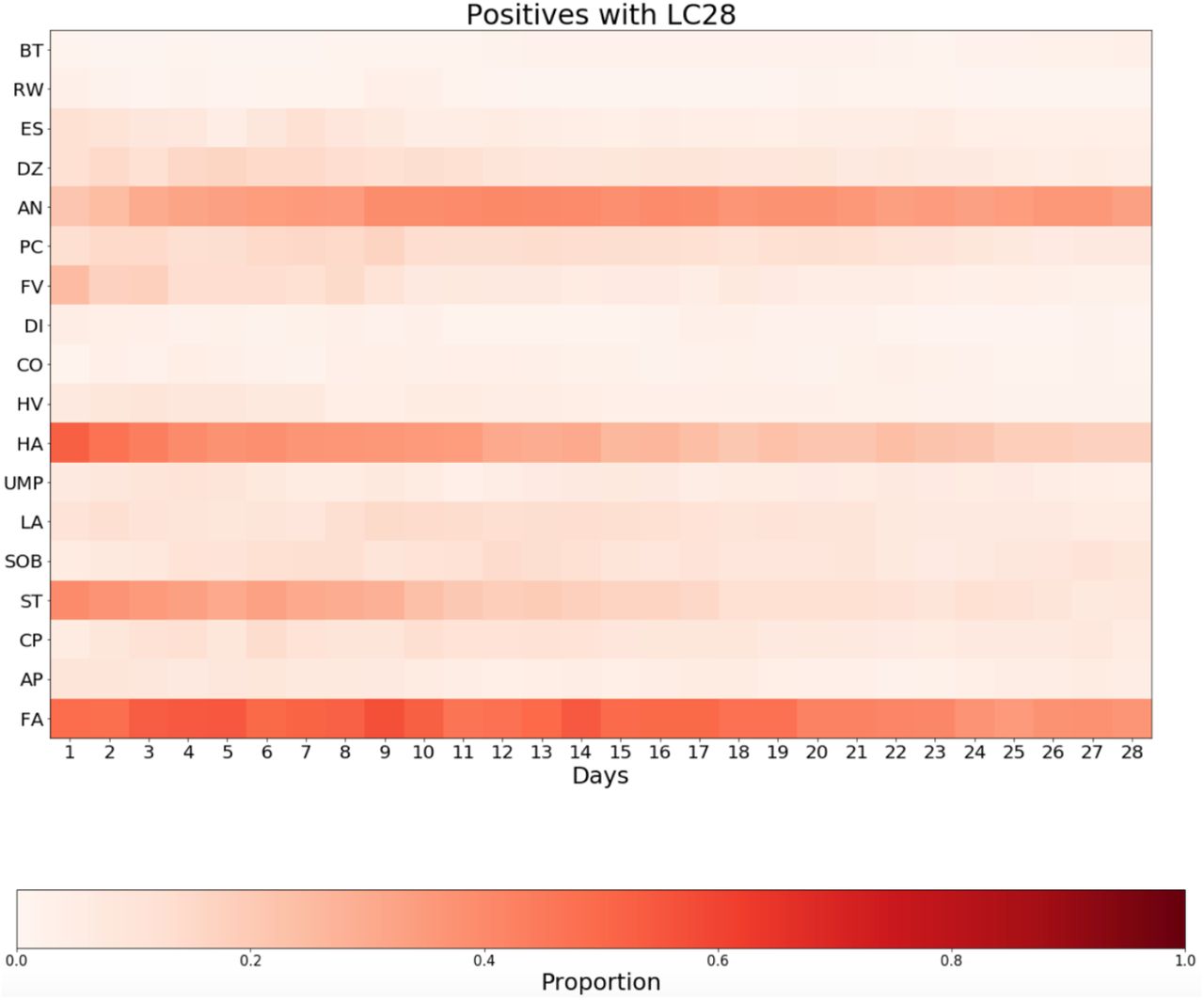
Overall, 77 (4.4% [95% CI 3.5-5.5]) of 1,734 children (18 younger children, 59 older children) had symptoms for ≥28 days, meeting the definition of LC28. The median symptom burden in these children was six symptoms [IQR 4;8] reported at least once during the first week of illness, and eight symptoms [IQR 6;9] reported at least once over the duration of their illness. However, by day 28 median symptom burden was low, at two [IQR 1;4] (younger children: three [IQR 1;4]; in older children, one [IQR 1;3]). The commonest symptoms experienced by children with LC28 over the duration of their illness were fatigue (experienced by 84.4% of children), headache (77.9%), anosmia (77.9%) and sore throat (74.0%). Figure 4 is a heat map of symptom profile and progression over the first 28 days in children with LC28.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Children with a positive SARS-CoV-2 test (n = 77 children)
Legend:
X-axis, duration in days.
Y axis, symptoms.
Legend: BT, blisters; RW, red welts; ES, eye soreness; DZ, dizziness and light-headedness; AN, anosmia; PC, persistent cough; FV, fever; DI, diarrhoea; CO, confusion; HV, hoarse voice; HA, headache; UMP, myalgias [unusual muscle pains]; LA, loss of appetite; SOB, dyspnoea [shortness of breath]; ST, sore throat; CP, chest pain; AP, abdominal pain; FA, fatigue. Colour bar provides percentage comparison.
Twenty-five (1.8% [95% CI 1.2-2.7]) of 1,379 children had symptoms for ≥56 days, meeting the definition of LC56.3 The median burden of symptoms in these children was six [IQR 4;8] symptoms reported at least once during the first week, and eight [IQR 6;10] symptoms reported at least once over the duration of their illness. The commonest symptoms experienced by children with LC56 over the duration of their illness were anosmia (84.0%), headache (80.0%), sore throat (80.0%) and fatigue (76.0%).
Consistent with correlation of illness duration with age across the cohort overall, older children were more likely to manifest symptoms ≥28 days, compared with younger children (59 (5.1%) of 1146 older children vs. 18 (3.1%) of 588 younger children, Chi-squared two-tail test p=0.046). However, this difference was no longer significant in the smaller number of children with illness duration ≥ 56 days (6 (1.3%) of 445 younger children vs. 19 (2.0%) of 934 older children, Fisher’s exact test p=0.52).
Symptom Reporting from Additional Questions (added 4 November 2020) and Free Text Analysis
Considering the additional questions added to the CSS app on 4 November 2020, rhinorrhoea was the most reported symptom (45.8% younger children; 53.5% older children) followed by sneezing (36.3% younger children; 36.6% older children) (Supplementary Figure 1), with similar prevalence when considered over the entire illness duration in children with LC28 overall (51.4% rhinorrhoea, 48.9% sneezing).
Potential neurological symptoms
As mentioned, headache and fatigue were the commonest symptoms in children testing positive for SARS-CoV-2, overall and in each age group. Dizziness (without differentiation between light-headedness and vertigo) was reported in 84 (14.3%) younger and 300 (26.2%) older children, with median duration of two [IQR 1;4] and two [IQR 1;5] days respectively. Symptoms consistent with confusion (encompassing confusion, disorientation, and drowsiness) were reported in 15 (2.6%) younger and 81 (7.1%) older children (median duration 2 day [IQR 1;2] and one day [IQR 1;3] respectively). No formal statistical comparisons of these symptoms in children with shorter or longer illness duration were made given the low prevalence of these symptoms in children with LC28 (Figure 4).
With respect to questions added to the app on 4 November 2020 (Supplementary Table 2), and with the sample size reduced because of the reduced timeframe, ‘brain fog’ was reported for 44 (8.7%) of 507 younger children (median duration one day [IQR 1;4]) and 188 (20.2%) of 932 older children (median duration two days [IQR 1;5]); and low mood was reported for 40 (8.0%) younger children (median duration two days [IQR 1;3.5]), and 145 (15.6%) older children (median duration two days [IQR 1;4.25]) (Supplementary Figure 1).
Free text searching for specific neurologic symptoms disclosed very few reports of weakness (two children) or tics (one child). No severe neurological manifestations (paralysis, ataxia, epileptic seizures, fits, convulsions, paroxysms) were reported (Supplementary Table 3). Irritability (three children), emotional difficulties (two children), and behavioural difficulties (one child) were reported rarely; impaired attention, impaired concentration, and anxiety were not reported.
Illness in symptomatic children who tested negative for SARS-CoV-2
15,597 symptomatic children (8,761 younger children, 6,836 older children), tested for SARS-CoV-2 infection but with a negative result, with logging at least once weekly and with calculable illness duration within the requisite time frame, were proxy-reported. Demographic details of the randomly selected matched control sample are shown in Table 1.
The median illness duration in these children was three days [IQR 2;7] (younger children three days [IQR 2;7]; older children four days [IQR 2;7]), significantly shorter than for children with a positive SARS-CoV-2 test (Wilcoxon signed rank test p<1.e-5). The individual symptom profile is shown in Supplementary Figure 4. The most frequently reported symptoms over the entire illness duration were sore throat (46.6%), headache (38.8%), fever (30.4%), fatigue (26.9%), and abdominal pain (24.7%) in younger children; and sore throat (60.6%), headache (48.8%), fatigue (37.2%), fever (20.4%) and persistent cough (20.6%) in older children.
Long illness duration in children who tested negative for SARS-CoV-2
Few children with a negative test for SARS-CoV-2 had illness duration for ≥28 days (15 of 1,734 children; 0.9%; 95% CI [0.5-1.4]). This was significantly fewer than children with a positive test, considered overall (Chi-squared 2-tail test p<1.e-10) and by age group (in younger children, three (0.5%) vs. 18 (3.1%); Fisher’s exact test: p=0.001; in older children, 12 (1.1%) vs. 59 (5.1%); Fisher’s exact test: p<1.e-8). The symptom profile of these children over the first 28 days is shown in Supplementary Figure 4. However, older children with a negative test for SARS-CoV-2 whose illness duration was ≥28 days had a greater symptom burden than was experienced by children with LC28, both at ≥28 days (Supplementary Figure 5), and over their entire illness duration (Supplementary Figure 6) (p=0.005 and p=0.025 respectively, Mann-Whitney-U tests).
Proxy-reporting density
Overall, proxy-reporting density (number of logging episodes/illness duration in days) was assiduous for all children. Reporting density was significantly higher in children with a negative test for SARS-CoV-2, compared to children with a positive test (reporting density in children negative vs positive: in younger children: 1 [IQR 0.68;1] vs. 0.89 [IQR 0.6;1]; and in older children 1 [IQR 0.67;1] vs. 0.8 [IQR 0.57;1]), noting the shorter illness duration in children with a negative test.
Proxy-reporting perseverance
Children were included in this study if their illness onset corresponded temporally to testing for SARS-CoV-2, and either a healthy report was received (1,551 (89.4%) of children with a positive test and 1,674 (96.5%) of children with a negative test) or proxy-reporting ceased.
Amongst children with a positive SARS-CoV-2 test, logging ceased in 183 children prior to a healthy report (22 children with LC28, 161 with [assumed] shorter illness duration). In children with LC28, a healthy report was received in 71.4% [55/77]. However, the remaining 22 children had already had symptoms logged for more than 28 days and thus fulfil the definition of LC28. In children with [assumed] shorter illness duration, a healthy report was received for 90.3% [1496/1657]. For the remaining 161 children, median symptom burden at last report was two [IQR 1;3]; and proxy-reporting usually ceased early in illness (logging cessation rates: 11.3% of children with illness duration <10 days; 5.5% ≥10 days). Thus, for children for whom proxy-reporting ceased prior to logging of a healthy report, we have assumed that proxy-reporting cessation coincided with illness resolution (i.e., that adults stopped proxy-reporting because the child had recovered) and illness duration was calculated assuming last day of logging corresponded to last day of illness.
We considered the impact of this assumption. Excluding all children with a positive SARS-CoV-2 test for whom a healthy report was not logged, median duration of illness in the remaining 1,551 was unchanged (6 days [IQR 3;11]) with prevalence of LC28 3.5% [55/1551], within the confidence intervals for LC28 using data from the entire cohort. Excluding only the 161 children with [assumed] short symptoms but including all children who had fulfilled the definition of LC28 (regardless of receipt of healthy report), prevalence of LC28 was 4.9% (77/1,573 children), again within the confidence intervals for LC28 using the entire cohort.
In children with a negative SARS-CoV-2 test, logging ceased in 60 children prior to a healthy report (four of 15 children with long illness duration, 56 of 1,719 children with [assumed] short illness duration). Proxy-reporting until logging of a healthy report was higher in children with a negative test, compared with children with a positive test (Chi-squared 2-tail test p<1.e-15).
Data governance did not allow assessment of familial relationships between proxy-reported individuals and the contributor; thus, we cannot comment whether concurrent illness of the contributor or other family members affected proxy-reporting.
Discussion
In this large study of UK school-aged children recruited via the CSS study app, we have shown that symptomatic infection with SARS-CoV-2 in children is usually short, with a median duration of illness of six days compared to 11 days in adults,3 and with low symptom burden (Figure 3). Prolonged illness duration can occur but is infrequent (4.4% with symptoms ≥28 days; 1.8% with symptoms ≥56 days), considerably lower than observed in adults using the same disease definitions (prevalence in adults of LC28: 13.3% and of LC56: 4.5%).3 Age is a risk factor for longer symptom duration (both overall, and specifically for illness duration ≥28 days), consistent with our previous findings in adults.3
Similar to adults,3 the commonest symptoms in children with COVID-19 were headache (62.2%) and fatigue (55.0%) (Table 2, Figure 2). A previous meta-analysis of studies in children with COVID-19, which included community-based and hospitalized children, identified fever (47%) and cough (42%) as the commonest symptoms.23 However, headache and fatigue were only assessed in half of contributing studies. In our (almost entirely community-managed) cohort, prevalence of fever was 37.7%, and persistent cough 25.5%. Anosmia (here, both anosmia and dysosmia) was also common in our cohort (39.6% overall: 22.4% of younger children, 48.3% of older children). Certainly, for older children this symptom was reported more often than was observed in a previous small study of adolescents (aged 10-19 years) with ‘mild to moderate’ COVID-19, ascertained from a single centre, in whom prevalence of anosmia was 24.1%,24 noting that anosmia was one of the core symptoms determining access to testing in the UK during our study period.
In children with symptoms ≥28 days, symptom burden was low by day 28 (median symptom burden of two). However, fatigue was a symptom at some stage in almost all (84.4%) of these children (Figure 4, Supplementary Figure 6). In adults, fatigue has been reported in many studies as the commonest symptom of long COVID, although prevalence varies. In our previous study in adults,3 fatigue was almost universal in LC28 (97.7% of cases experienced fatigue during their illness). Other studies have also reported persistence of fatigue after acute infection in adults (e.g., 53.1% at 60 days25; and 52.3% at 10 weeks26).
Considering the prevalence and persistence of headache and fatigue within the context of usual prevalence of these symptoms within the general paediatric population is difficult, as few large-scale epidemiological studies have been undertaken in children to provide normative population data. Considering headache, a systematic review of headache comprising 38 unselected population-based studies in individuals under 20 years reported that around 60% of children are “prone to headache”.27 A random sample of 2,165 school children from Aberdeen aged 5-15 years found that 1,166 (66%) had headaches over the previous year, which in 391 (22%) children were of sufficient severity to stop normal activities.28 Considering fatigue, a study of 2,936 children found that 129 (4.4%) had “more than a few days of disabling fatigue”.29 Prevalence of chronic fatigue syndrome (defined here as “disabling fatigue lasting >3 months with one additional symptom, where no other cause for the fatigue could be established”) was 1% in a study of 11-16-year-old children from three secondary schools in England.30 Prevalence of “chronic disabling fatigue” reported by the Avon Longitudinal Study of Parents and Children (defined here as fatigue lasting >6 months associated with absence from full-time school or that had prevented the child from taking part in activities ‘quite a lot’ or ‘a great deal’, and not due to excess of physical activity) was 1.5% and 2.2% at 13- and 16-years respectively.31 Considering fatigue after viral infection specifically, and choosing one of the younger published cohorts, median symptom duration with Epstein–Barr virus in symptomatic university students (i.e., older than the cohort reported in our study) was 10 days (mean 17, range 3-66 days), with fatigue persisting for a median of 15.5 days.32 These studies indicate the wide range of prevalence of these symptoms in paediatric populations generally.
The paucity of contemporaneous data comparing illness duration and symptom profiles from different viruses also complicates contextualisation of illness due to SARS-CoV-2 infection in children. A preprint paper comparing data from 55,270 children/adolescents with COVID-19 (3,693 of whom were hospitalized) with a non-contemporaneous cohort of 1,952,693 children with influenza during 2017-19 (hospitalised numbers unclear) suggests that dyspnoea, anosmia, and gastrointestinal tract symptoms are more common in children with COVID-19 than in children with influenza.33 However, symptoms and overall illness duration were only reported as present or absent at 30 days in both groups, preventing more granular comparisons.
Here, a strength of our study was our ability to compare contemporaneous illness profiles of symptomatic children testing positive vs. negative for SARS-CoV-2, matched for age, gender, and week of testing. Children testing positive for SARS-CoV-2 had longer median illness duration (six days vs. three days in negatives); and were more likely to have illness duration ≥28 days (4.4% vs. 0.9%). However, some children testing negative for SARS-CoV-2 also had symptoms that lasted >28 days, and these children had a higher symptom count both over the duration of their illness and at day 28 (Supplementary Figures 4, 5), acknowledging here that our sample size is small. We considered whether some children with long illness duration who tested negative for SARS-CoV-2 might have false negative results. However, there is no evidence that sensitivity and specificity of testing for SARS-CoV-2 are different in adults compared with children, with sensitivity for PCR SARS-CoV-2 tests around 95%.34
Additionally, the symptom profiles of children negative for SARS-CoV-2 (Supplementary Figures 4, 5, 6) suggest some differences in their illness compared with children with positive results. Relevantly, the prevalence of non-SARS-CoV-2 respiratory viruses (influenza A, influenza B, parainfluenza, adenovirus, rhinovirus, and respiratory syncytial virus) was unusually and extremely low over the UK winter of 2020/202135–37, with the exception of the commonly observed rhinovirus peak coinciding with the September return-to-school.20 With relaxation of personal protection and social distancing measures, it is likely that these illnesses will return to more usual (i.e., higher) levels of circulation in future UK winters. Our data highlight that other illnesses may also have a protracted and burdensome course in children, which will also need consideration in post-pandemic service delivery planning.
Short and long-term effects of COVID-19 on school performance and learning have been a recent matter of concern.38 In our cohort, neither attentional problems nor memory complaints nor anxiety were reported. Isolated cases of low mood and/or irritability were consistent with, if not lower than, previously reported statistics in the general school-aged healthy population.39 Our data do not support anecdotal reports of weakness and seizures as common features in children with COVID-19, whether of short or longer illness duration; and no severe neurological symptoms were reported. However, persistence of symptoms from any illness can be associated with low mood, with adverse long-term outcomes including school refusal and separation anxiety.40 Although self-reporting adults were able to participate in specific questions regarding mental health, these data could not be proxy-reported. This limits our ability to assess mental health issues comprehensively, and any potential impact on school performance and learning, in children during the COVID-19 pandemic whether testing positive or negative for SARS-CoV-2.
In considering how our data relates to other sources, the UK Office for National Statistics (ONS) conducted a round of testing for SARS-CoV-2 (irrespective of symptoms) from 2 to 10 December 2020, prior to the UK peak of infection, with deliberate oversampling of schools which had had the highest infection rates at the start of the academic year. 121 schools (41 primary, 80 secondary) in 15 local authorities were examined, with a total of 7,089 pupils.41 Primary school pupils and staff had a slightly lower percentage testing positive (0.94% and 0.99% respectively) for SARS-CoV-2 than secondary pupils and staff (1.22% and 1.64%). ONS warned that their conclusions might not have general validity; and these figures do not capture time fluctuations as the pandemic progressed. In our dataset, with data captured until 22 February 2021 (thus including the subsequent rise in numbers over Christmas and New Year), 6,043 of 258,790 (2.3%) of proxy-reported children were reported with a positive test (2.3% of younger children, 3.7% of older children), noting that reporting was voluntary, by proxy, and through a specific COVID-19 platform, and that testing was only available for symptomatic individuals. Additionally, the CSS app user base (considered as a whole) is not fully representative of the wider UK population, due to over-representation of female gender, white background, and above-average socioeconomic status.18 Further, we cannot characterise regional variability, as geographic information was not available for many participants.
We considered what proportion of the total number of school-aged children in the UK testing positive for SARS-CoV-2 were proxy-reported to the CSS. The different countries of the UK report data for children within different age groups and over varying time periods. In England there were 390,866 positive tests in young people aged 5-19 years from 1 September 2020 to 24 January 2021 (5-9 years: 69,641 children; 10-19 years: 321,225 individuals).20 In Scotland,15,869 children aged 0-14 years, and 14,597 young people aged 15-19 years have tested positive from the start of the pandemic to 30 March 2021.42 In Wales there were ∼28,300 cases in children and young people from the start of the pandemic to 30 March 2021.43 In Northern Ireland 13,268 individuals aged 0-19 years from the start of the pandemic to 30 March 2021.44 Thus, our study represents ∼1-2% of all school-aged children with positive tests across the UK during this time, noting that many of these national figures include young adults and preschool-aged children.
The ONS has also provided estimates of long COVID in children aged 2-16 years, with the most recent data release (April 2021) suggesting that 9.8% of children aged 2-11 years and 13.0% of those aged 12-16 years experience ongoing symptoms five weeks after testing positive for SARS-CoV-2, and 7.4% and 8.2% respectively are still reporting symptoms at 12 weeks.45 These latest figures include a control group (defined as those who were never symptomatic, never tested, never-self isolated, and never a contact of anyone testing positive for SARS-CoV-2) which suggested ‘baseline’ rates for the same symptoms of 2% amongst 2-to 11-year-olds and 1.7% amongst 12-to 16-year-olds. Earlier, in January 2021, ONS had reported long COVID symptoms by age; however, updated age-specific estimates for specific symptoms were not included in April 2021 data release. Overall ONS long COVID prevalence estimates were adjusted downwards between January and April 2021 (e.g., from 12.9% to 9.8% in 2-to 11-year-olds).45,46
There is some disparity between our prevalence data for LC28 in children and those of the ONS. At least part of the reason may be that the ONS required two consecutive asymptomatic visits to define the end of illness. Thus, individuals with relapsing/remitting symptoms in whom asymptomatic periods lasted longer than one week would be captured by ONS but not by our study. Consistent with this, the ONS’ sensitivity analysis of the impact of defining symptom discontinuity to a single asymptomatic visit radically lowered their prevalence estimates, especially for ongoing symptoms at 12 weeks, with estimates falling from 13.7% to 0.9% (ref47 - Table 11), much more in keeping with our results. Additionally, ONS estimates are based on both current and recalled data, collected in the first week of each month. In contrast, our app-based data collection was conducted in real time, with high density and persistence of proxy-reporting of children (whether the child had tested positive or negative for SARS-CoV-2). A recent Australian study reported 151 (of an initial cohort of 171) young children (median age three years [IQR 1;8]) who tested positive for SARS-CoV-2 and were followed for three to six months. Twelve (8%) children (median age two years) were reported to have symptoms 3-8 weeks after initial presentation (most commonly cough and/or fatigue), all of whom resolved by the end of the study to their baseline health.23 This small study concords more closely with our results. None-the-less, and with the methodology for the ONS experimental estimates not yet published, the ONS estimates have been used in many service provisions and government discussions, and reported widely in social and other media.48,49
Our study is part of one of the largest citizen science initiatives ever in the UK, with generation of real-time epidemiological data from over 4.5 million users across the UK. We leveraged previously published methodologies assessing illness duration and symptom profiling in adults, including assessment of long COVID.3 Our data census points allowed us to capture all children with illness duration ≥8 weeks, if they had presented before the date of peak specimen receipt in the UK; and our restriction to individuals whose symptom presentation concorded with test timing allowed an accurate determination of symptom onset. Moreover, by restricting analyses to start from 1 September, we avoided bias due to limited test availability during the first wave of the pandemic. However, despite general availability there were still some blocks to testing - in particular, that individuals were required at least one of a defined list of symptoms (specifically, fever, cough and anosmia),50 which list was largely informed by adult symptomatology and might not be sufficiently broad to capture some common paediatric manifestations of COVID-19, (e.g., abdominal pain, reported in 4% of paediatric cases4 and in 27.8% of our younger children). Related to this, the set of questions asked through the app, although refined between 24 March and 1 September, and again on 4 November 2020, was largely informed by research in adults. Although we cannot exclude the possibility that a paediatric version might capture other manifestations of COVID-19, the free text data did not suggest common themes emerging unique to paediatric populations. We did not undertake a formal qualitative analysis of the free-text data given (a) its ad hoc collection rather than a formal qualitative study, and (b) the potential bias arising from introduction of additional direct symptom questions from 4 November 2020 (i.e., once a symptom was asked about directly, it was unlikely that to be reported as free text). None-the-less, we have provided the data from free text responses, and from questions asked after 4 November 2020 in the Supplementary Material. We acknowledge that symptoms were reported by proxy rather than directly ascertained; however, this is common in clinical assessment of children, particularly younger children. Additionally, children cannot directly consent to research participation. We also acknowledge the possibility that older children may have reported for themselves using their relatives’ phone/log-in function and/or misused proxy-reporting from their own mobile phones; however, we have no means of capturing such activity.
Conclusions
Our national cohort of children and young people provides the first systematic description of COVID-19 in children. Our data show that long illness duration after SARS-CoV-2 infection in school-aged children is not common; however, a small proportion of children do have prolonged illness duration and persistent symptoms, validating these children’s experiences. Our LC56 data provide reassurance regarding the longer term outcome for these children. The symptom burden in children who tested negative for SARS-CoV-2 but had long illness duration highlights that allocation of appropriate resources will be necessary for any child with prolonged illness, whether due to SARS-CoV-2 infection or other illness. Our study provides timely and critical data to inform discussions around the impact and implications of the pandemic on UK paediatric healthcare resource allocation.
Data sharing
Data collected in the COVID Symptom Study smartphone application are being shared with other health researchers through the UK National Health Service-funded Health Data Research UK (HDRUK) and Secure Anonymised Information Linkage consortium, housed in the UK Secure Research Platform (Swansea, UK). Anonymised data are available to be shared with researchers according to their protocols in the public interest (https://web.www.healthdatagateway.org/dataset/fddcb382-3051-4394-8436-b92295f14259).
Declaration of interests
CH, SS, KR, JCP are employees of Zoe Global Ltd. All other authors have nothing to declare.
Acknowledgements
This work is supported by the Wellcome EPSRC Centre for Medical Engineering at King’s College London (WT 203148/Z/16/Z) and the UK Department of Health via the National Institute for Health Research (NIHR) comprehensive Biomedical Research Centre award to Guy’s & St Thomas’ NHS Foundation Trust in partnership with King’s College London and King’s College Hospital NHS Foundation Trust. Investigators also received support from the Medical Research Council (MRC) and British Heart Foundation, the UK Research and Innovation London Medical Imaging & Artificial Intelligence Centre for Value Based Healthcare, and the Wellcome Flagship Programme (WT213038/Z/18/Z). EM is funded by an MRC Skills Development Fellowship Scheme at KCL. CHS is supported by an Alzheimer’s Society Junior Fellowship (AS-JF-17-011). ZOE Global supported all aspects of building and running the app and service to all users worldwide.
Footnotes
↵* Equal contribution
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
19
Blogs/Media
Author Videos