
Abstract
Importance Cognitive impairment is a common feature of both symptomatic and remitted states of depression that is associated with poorer psychosocial outcomes and treatment non-response. As such, finding treatments to maintain or enhance cognition in people with depression is imperative.
Objective To investigate the efficacy of computerized cognitive training (CCT) on cognitive and functional outcomes in people with depression.
Data Sources MEDLINE, EMBASE and PsycINFO databases were screened through the Ovid interface for eligible studies from inception to 29 June 2020, with no language or publication type restrictions.
Study Selection Two independent reviewers conducted duplicate study screening and assessed against the following inclusion criteria: (1) adults with depression, (2) CCT with minimum three hours practice, (3) active or passive control group, (4) cognitive and/or functional outcomes measured at baseline and post-intervention, (5) randomized controlled trials. Of 3666 identified studies, 24 met selection criteria.
Data Extraction and Synthesis The methods used followed the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines. Data extraction and risk of bias assessment using the revised Cochrane Risk of Bias Tool (RoB2) was conducted independently by two reviewers. Analysis of the pooled results was conducted using robust variance estimation (RVE) based on a correlational dependence model.
Main Outcomes and Measures The primary outcome was change from baseline to post-intervention in overall cognition. Secondary outcomes were depressive symptoms, psychiatric symptoms, psychosocial functioning, daily functioning, subjective cognition, global cognition and domain-specific cognitive function.
Results Twenty-four studies encompassing 28 comparisons and 1,141 unique participants met inclusion criteria. The pooled effect size of CCT for overall cognition was small and significant (g=0.26; 95% CI 0.15 to 0.36; P<.001; τ2=0.057; I2=37%; prediction interval −0.25 to 0.76) and for depressive symptoms was small and significant (g=0.24; 95% CI 0.04 to 0.45; P=.02; τ2=0.075; I2=46%; prediction interval −0.37 to 0.86). Evidence of small-study effect was found for both overall cognition and depressive symptoms, with trim-and-fill analysis imputing two studies for each. Sensitivity analyses of overall cognition and depressive symptoms revealed the main analyses to be robust. Benefits of CCT were also found for psychosocial functioning and domain-specific cognitive function in abstract reasoning, learning/encoding efficiency, retrieval fluency, high working memory, low working memory, inhibition and processing speed. No significant effect was found for psychiatric symptoms, subjective cognition, global cognition or domain-specific cognitive function in short-term memory and shifting. No separate pooled analyses were conducted for daily functioning or verbal reasoning, updating and visual processing domains due to two or less studies reporting outcomes for each. A moderating effect of dose was found for overall cognition, with larger doses of CCT associated with greater effect size estimates.
Conclusions and Relevance This systematic review and meta-analysis indicates that CCT is an efficacious intervention for overall cognition, depressive symptoms, psychosocial functioning and domain-specific cognitive function for people with depression.
Introduction
Cognitive impairment is a central feature of depression1 observed frequently in both symptomatic and remitted states, which is associated with poorer psychosocial functioning2 and treatment non-response3-5 and is only partially responsive to antidepressants6. Additionally, comorbid depression is common in people with chronic diseases and may interfere with the management of medical disorders and treatment adherence, leading to worse functional outcomes7. Moreover, as one of the most robust dementia risk factors, depression increases the risk of dementia in later life by approximately 80%8 and given its prevalence may independently account for around 8% of dementia cases worldwide9. Thus, interventions that effectively target cognition alongside other symptoms in people with depression may have a key role in supporting everyday function10, as well as in delaying or preventing cognitive decline and dementia8,11.
Computerized cognitive training (CCT) is a safe and scalable cognitive training approach that focuses on repeated and controlled practice on cognitively demanding tasks10,12. CCT is appealing as it can be adapted to individual needs, provides ongoing feedback and can be delivered inexpensively in both clinical and community settings. Support for CCT has been found for cognitive and functional outcomes across many clinical and non-clinical populations13-18, however, efficacy varies across populations, outcomes and design factors such as dose and supervision13,14,17.
To date two meta-analyses have investigated the efficacy of CCT in people with depression, reporting improvements in depressive symptoms and mixed results for cognition19,20. However, both mixed randomized controlled trials (RCTs) with other designs and included a combination of CCT with other approaches. Additionally, only one meta-analysis19 investigated daily functioning, leaving CCT efficacy for functional outcomes unknown. Thus, the potential of CCT as an intervention for people with depression has yet to be systematically and robustly evaluated. Moreover, investigations of the extent to which population characteristics, design factors and study quality may relate to outcomes are required to inform clinical guidelines10. We therefore aimed to investigate the efficacy of CCT on cognitive and functional outcomes in people with depression and to examine design factors that may moderate CCT efficacy.
Methods
This review adheres to the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines21 and largely follows methods established in our previous reviews of CCT.16,17,22 The protocol has been prospectively registered with PROSPERO (CRD42020204209). A protocol paper is currently under review and available as preprint.23
Eligibility Criteria
We included RCTs studying the effects of CCT compared to control conditions on one or more cognitive, depressive symptoms, psychosocial or functional outcome(s) in adults with depression at baseline (at any clinical stage). Depression was established according to standard diagnostic criteria, diagnostic interviews, expert clinical diagnosis or a mean score greater than a validated cut-off on an established clinical measure (eTable 1 in the Supplement). There was no restriction on study population apart from studies targeting primarily people with dementia or major psychiatric comorbidities; when the study population included a mixed sample (e.g., ≥50% of the sample received antipsychotic medication), the study was only included if data just for eligible participants could be obtained. CCT was defined as a minimum of 3 hours of practice on standardized computerized tasks or video games with clear cognitive rationale, administered on personal computers, mobile devices or gaming consoles. Eligible controls included passive (wait-list, no-contact) and active (e.g., sham CCT, recreational activities) control groups. Studies combining CCT with other non-pharmacological interventions (e.g., psychotherapy, physical exercise) or with pharmacological interventions were eligible as long as both arms received the same adjacent interventions. All eligible comparisons in multi-arm studies were included.
Information Sources and Study Selection
We searched MEDLINE, EMBASE and PsycINFO through the OVID interface for eligible articles from inception to 29 June 2020. No restrictions on language or type of publication were applied. The electronic search was complemented by hand-searching the references of included articles and previous reviews of CCT16-18,23,24 as well as clinical trial registries. The full search strategy is shown in eTable 2 in the Supplement. Two independent reviewers (NHL and AR) conducted duplicate screening of titles and abstracts as well as full-text screening of potentially eligible articles. Disagreements at each stage were resolved by consensus or by involvement of a senior reviewer (AL), who also contacted the corresponding authors of primary studies for additional information. The final list of included studies was reviewed and approved by AL.
Data Extraction and Coding
Data were extracted and coded in duplicate by two reviewers (NHL and RM), supervised by a neuropsychologist (HMG). Outcome data were extracted as mean and standard deviation (SD) for each group at each time point, or when this was not available, as measures of mean difference and SD or confidence intervals (CI). Missing or incomplete data were requested from the corresponding authors of the studies. Coding of cognitive outcomes was conducted according to the Cattell-Horn-Carroll-Miyake (CHC-M) framework25. Following this framework, each cognitive outcome was classified into a broad cognitive domain (e.g., executive function) as well as a more specific narrow cognitive domain (e.g., inhibition). Cognitive screening instruments, such as the Mini-Mental State Examination, were classified as global cognition16,17. The classification of individual outcome measures into domains is presented in eTable 3 in the Supplement. Non-cognitive outcomes included depressive symptoms, psychiatric symptoms, psychosocial functioning, daily functioning and subjective cognition. The classification of baseline depressive symptoms severity for subgroup analysis is presented in eTable 4 in the Supplement.
Risk of Bias Within Studies
Two independent reviewers (NHL and RM) assessed the risk of bias of eligible comparisons within studies using the revised Cochrane Risk of Bias Tool (RoB2).26 Disagreements were resolved by consensus or by consultation with a senior reviewer (AL). In contrast to the original RoB2 macros, studies with “some concerns” or “high” risk of bias in domains 3 (bias due to missing outcome data) or 4 (bias in measurement of the outcome) were considered as having some concerns or high risk of bias, respectively.
Data Synthesis
Analyses were conducted using the packages robumeta27 and clubSandwich28 and metafor in R, version 4.0.2 (The R Foundation for Statistical Computing). Between-group differences in change from baseline to post-intervention were converted to standardized mean differences and calculated as Hedges’ g with 95% CI for each eligible outcome measure. Multivariate analyses were performed using robust variance estimation (RVE) based on a correlational model with rho=0.8 to account for the non-independence of multiple effect sizes within studies.29 The primary outcome was change from baseline to post-intervention in overall cognition, assessed through one or more non-trained measures of objective cognition using standardized neuropsychological tests. Secondary outcomes included depressive symptoms, psychiatric symptoms, psychosocial functioning, daily functioning, subjective cognition, global cognition and domain-specific cognitive function.
Heterogeneity across studies was quantified using τ2 and expressed as a proportion of overall observed variance using the I2 statistic.30,31 Prediction intervals were calculated to assess the dispersion of true effects across settings.32 Univariate RVE meta-regressions of a priori potential moderators (design characteristics, population characteristics and overall risk of bias) were performed for overall cognition and depressive symptoms using robumeta and contrasts formally tested using Hotelling–Zhang test (F-statistic) with clubSandwich.33 Small-study effect for primary outcomes was assessed by visually inspecting funnel plots of effect size vs standard error34 and formally tested using the Egger’s test as a meta-regression in RVE.35 The Duval and Tweedie trim and fill36 was also used to assess the magnitude of small-study bias. Two-sided α<.05 indicated statistical significance.
Results
Study Selection
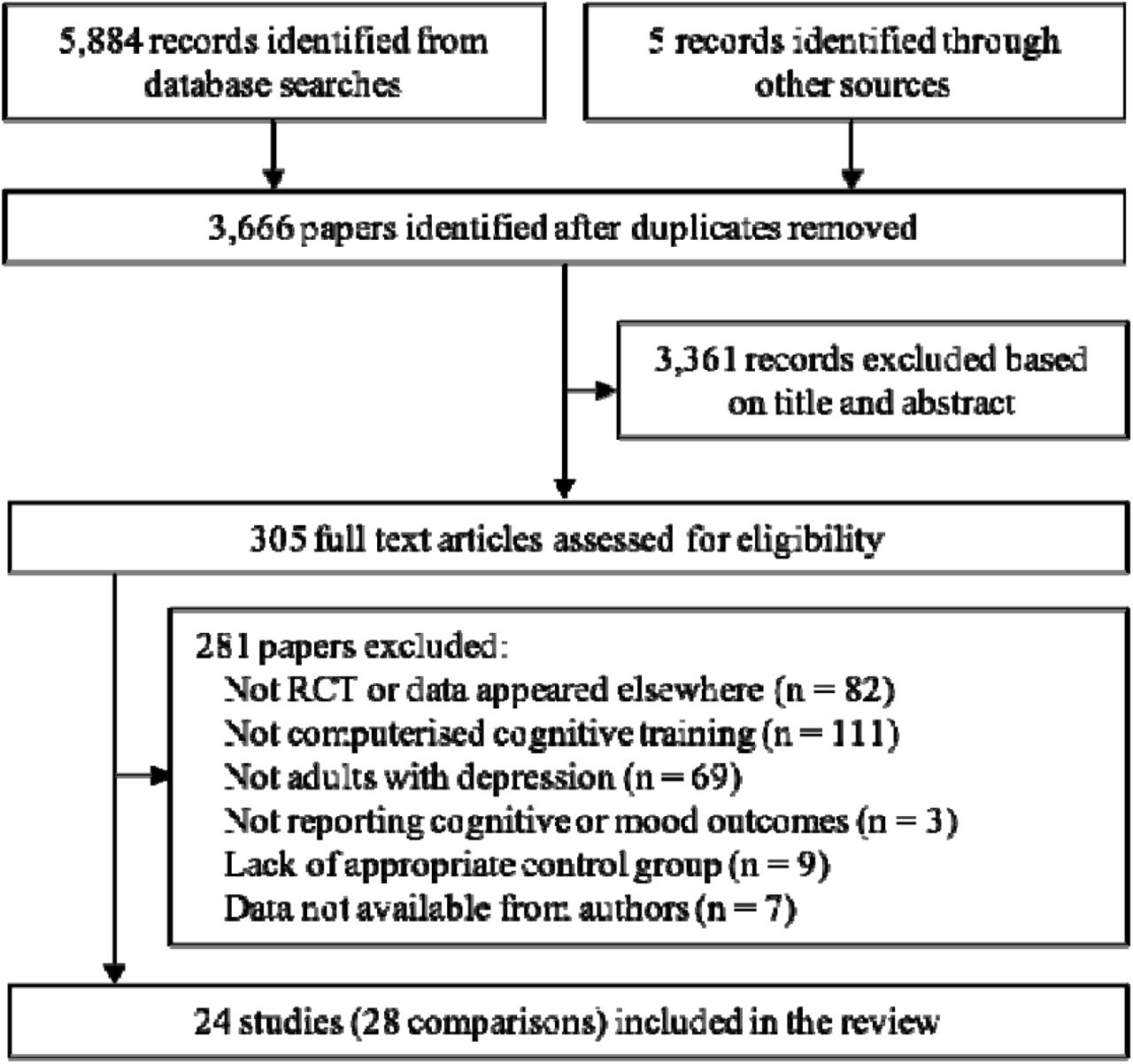
After removal of duplicates, we screened 3,661 articles for eligibility, of which 300 articles were assessed in full-text screening. Of these, 19 studies fulfilled inclusion criteria. A list of the excluded studies is provided in eTable 5 in the Supplement. Additionally, four eligible studies from our previous reviews37-40 and one eligible study published after the search41 were identified through manual search, thus giving a total of 24 studies eligible for inclusion (Figure 1). The authors of eight eligible studies were contacted for additional data, of which four42-45 provided data.

Characteristics of Included Studies
The 24 included studies reported data from 28 eligible comparisons, encompassing 1,141 participants with mean age ranging between 34.15 and 73.96 years. The majority of studies included people with a diagnosis of MDD or a current major depressive episode (k=11 RCTs; n=498). Three studies46-48 specifically focused on people with partially and/or fully remitted depression (n=139). Five studies included people with multiple sclerosis37,49-52 (n=277). Five studies (n=230) targeted older adults, of which three were in people with Parkinson’s disease.39,40,53 Mean baseline depression severity was classified as mild depression (k=12; n=610) or moderate-severe depression (k=12; n=531). Studies including participants with fully remitted depression that had mean baseline depression severities below cut-offs46,47 were included in the mild depression subgroup. The most common type of CCT was multidomain training (k=15; n=604), followed by working memory training (k=4), attention training (k=2), memory training (k=2) and speed of processing training (k=1). For the purpose of subgroup analyses, studies using only single-domain training (attention, working memory, memory or speed of processing) were classified as single-domain. Thirteen studies used an active control group, seven studies had a passive control group, two studies had two CCT arms,48,54 one study had two active control groups44 and one study had both active and passive control groups.55 Overall risk of bias was assessed as low in seven studies, some concerns in five studies, high in nine studies and one study55 had one comparison assessed as low and the other as high (eTable 6 in the Supplement).
Primary Outcome: Overall Cognition
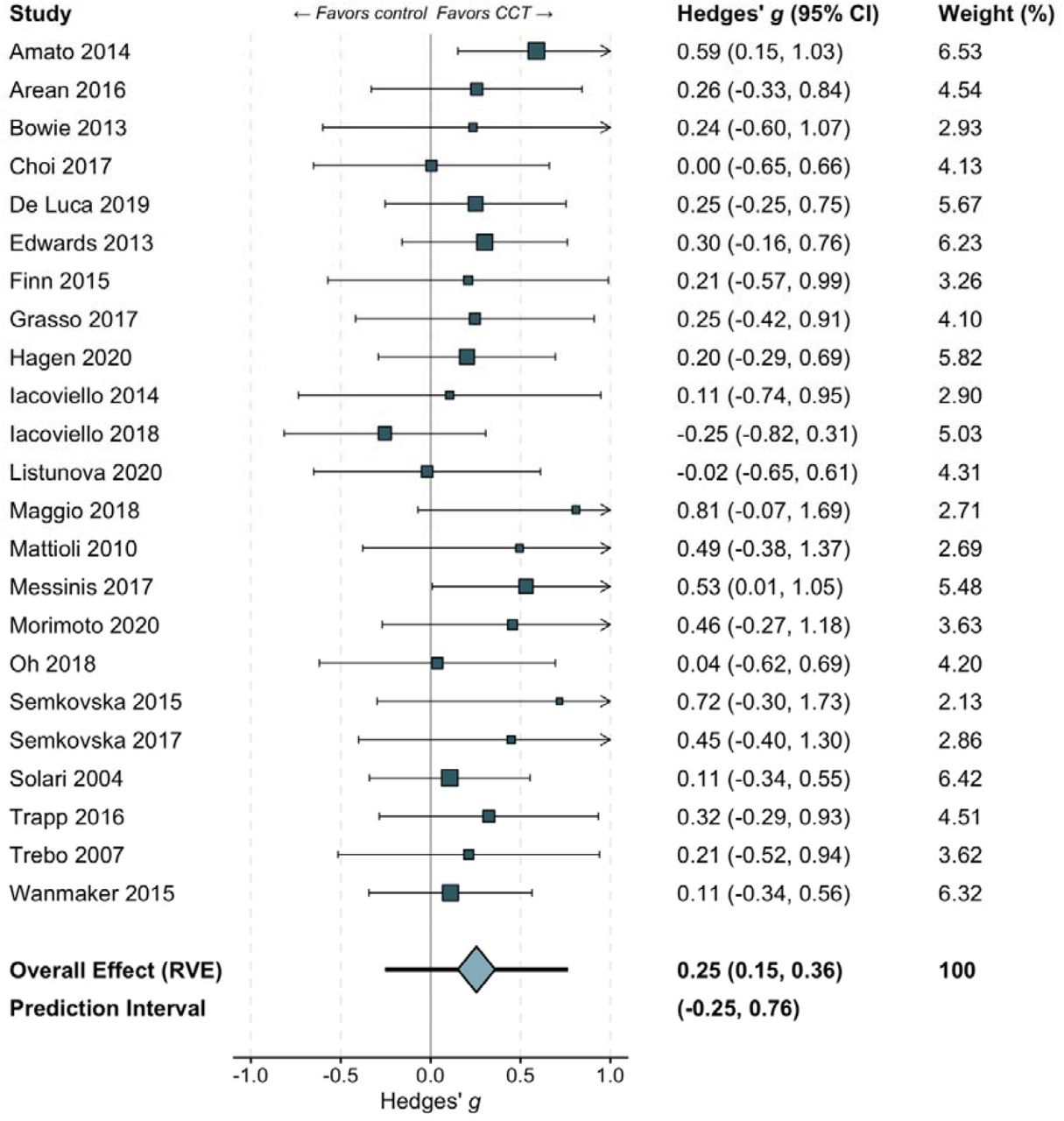
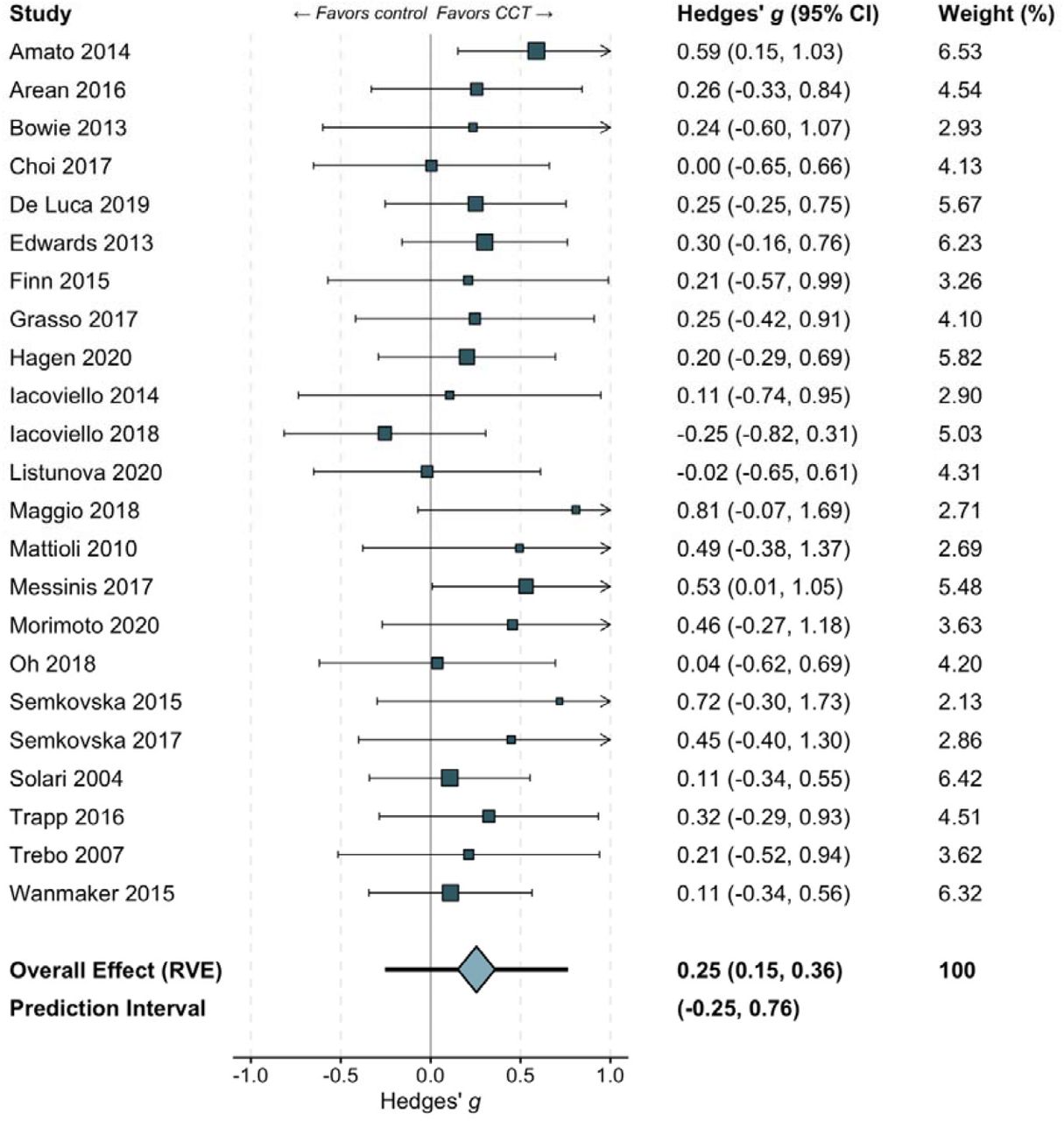
Twenty-three studies reported cognitive outcomes at baseline and post-intervention timepoints. The pooled effect size across these 23 studies and 242 effect sizes was small and statistically significant with moderate heterogeneity (g=0.26; 95% CI 0.15 to 0.36; P<.001; τ2=0.057; I2=37%; prediction interval −0.25 to 0.76, Figure 2). Funnel plot asymmetry was detected, indicating possible small-study effect (β=1.01; one-tailed P=.07; eFigure 1 in the Supplement). A trim and fill analysis imputed two studies; the adjusted effect size suggested negligible small-study bias (g=0.23; 95% CI 0.11 to 0.36; P<.001; eFigure 2 in the Supplement). Sensitivity analyses comparing a hierarchical (g=0.21; 95% CI 0.07 to 0.36; P=.008; Ω2=0.010; τ2=0.061) to a correlational model as well as correlation assumptions revealed the model assumptions of the main analysis to be robust (eTable 7 in the Supplement). An additional sensitivity analysis with studies with remitted depression populations removed further supported this (g=0.26; 95% CI 0.15 to 0.37; P<.001; τ2=0.050; I2=34%). The pooled effect size was similar across studies with high and low risk of bias, as well as across active- and passive-controlled comparisons (Table 2).
Study characteristics
Results of meta-regressions
Secondary Outcome: Depressive Symptoms
Nineteen studies reported depressive symptoms outcomes at baseline and post-intervention timepoints. The pooled effect size across these 19 studies and 26 effect sizes was small and statistically significant with moderate heterogeneity (g=0.24; 95% CI 0.04 to 0.45; P=.02; τ2=0.075; I2=46%; prediction interval −0.37 to 0.86). Funnel plot asymmetry was detected, indicating possible small-study effect (β=1.71; one-tailed P=.09; eFigure 3 in the Supplement). A trim and fill analysis imputed two studies; the adjusted effect size suggested minor small-study bias (g=0.18; 95% CI −0.02 to 0.38; P=.08; eFigure 4 in the Supplement). Sensitivity analyses comparing a hierarchal (g=0.25; 95% CI 0.06 to 0.43; P=.01; Ω2=0.000; τ2=0.053) to a correlational model as well as correlation assumptions revealed the model assumptions of the main analysis to be robust (eTable 7 in the Supplement). An additional sensitivity analysis with studies with remitted depression populations removed further supported this (g=0.23; 95% CI 0.00 to 0.45; P=.046; τ2=0.081; I2=48%). The pooled effect size was similar across studies with high and low risk of bias, as well as across active- and passive-controlled comparisons (Table 2).
Meta-regressions
Results of meta-regressions of categorical moderators for overall cognition and depressive symptoms are provided in Table 2. Greater doses (total number of hours of training) were associated with larger overall cognitive effect sizes (F2,11.2=6.49; P=.01). Increases in effect sizes with greater dose were also observed for depressive symptoms, but the association was not statistically significant (F2,8.7=0.17; P=.85), potentially due to higher heterogeneity and imprecision within dose subgroups. Session duration of ≥60 minutes was associated with greater cognitive effect size (F1,13.3=9.94; P=.007); analysis of depressive symptoms suggested the opposite relationship (i.e., larger effect in shorter sessions) but this association was not statistically significant (F1,12.4=2.98; P=.11). Meta-regressions of other categorical and continuous moderators (dose, frequency, length, year of publication and percent female) did not show an association with effect size for overall cognition or depressive symptoms.
Secondary Outcomes: Other Non-cognitive Outcomes
The pooled effect size across psychosocial functioning outcomes was moderate and statistically significant (k=8; g=0.33; 95% CI 0.11 to 0.54; P=.009; τ2=0.000; I2=0%). The pooled effect size across psychiatric symptoms outcomes was small but did not reach statistical significance (k=7; g=0.19; 95% CI −0.11 to 0.48; P=.16; τ2=0.024; I2=19%). The pooled effect size across subjective cognition outcomes was negligible and did not reach statistical significance (k=6; g=0.12; 95% CI −0.02 to 0.26; P=.08; τ2=0.000; I2=0%). Only two studies reported daily functioning outcomes, so no separate pooled analysis for daily functioning was conducted. Funnel plots and forest plots for non-cognitive outcomes are provided in eFigures 5-11 in the Supplement.
Secondary Outcomes: Global Cognition and Individual Cognitive Domains
The pooled effect sizes across fluid reasoning, abstract reasoning, retrieval fluency, general short-term memory, high working memory and low working memory outcomes were moderate and statistically significant. No studies reported verbal reasoning outcomes, so therefore the pooled analysis across fluid reasoning is solely reflective of abstract reasoning outcomes. The pooled effect sizes across long-term memory and retrieval, learning/encoding efficiency, executive function, inhibition, processing speed and perceptual speed outcomes were small and statistically significant. As perceptual speed is the only narrow domain under processing speed results for these two domains are identical. Small effect sizes that did not reach statistical significance were found for short-term memory, shifting and global cognition (k=3; g=0.24; 95% CI −0.86 to 1.34; P=.43; τ2=0.105; I2=47%) outcomes. Outcomes for updating and visual processing were only reported in two studies, so no separate pooled analyses for updating or visual processing were conducted. Results of RVE analyses of individual cognitive domains for which data were available are provided in Figure 4. Funnel plots and forest plots of global cognition and individual cognitive domains are provided in eFigures 12-36 in the Supplement.


{kind=link}
{kind=link}
{kind=link}
{kind=link}
Discussion
This systematic review and meta-analysis of 24 RCTs of narrowly defined CCT demonstrates that CCT is an effective intervention for improving overall cognition and mood in people with depression. In addition, benefits of CCT in people with depression were also found for psychosocial functioning and domain-specific cognitive function in abstract reasoning, learning/encoding efficiency, retrieval fluency, high working memory, low working memory, inhibition and processing speed. No significant effect was found for psychiatric symptoms, subjective cognition, global cognition or domain-specific cognitive function in short-term memory and shifting. Although it should be noted that due to the small number of studies reporting outcomes for psychiatric symptoms, subjective cognition and global cognition, statistical power to identify significant effects for these outcomes was limited. Additionally, no separate pooled analyses were conducted for daily functioning or verbal reasoning, updating and visual processing domains due to two or less studies reporting outcomes for each.
Results of the moderator analysis revealed a significant dose effect for overall cognition, with greater doses of CCT associated with greater improvement in overall cognition. Furthermore, subgroup analysis of control type did not reveal a benefit for active control conditions over passive control conditions for overall cognition or mood, which is consistent with previous meta-analyses of CCT19,20. For overall cognition, effect size estimates were not influenced by overall risk of bias, whilst for mood, although effect size estimates varied by overall risk of bias, the difference between subgroups was not statistically significant. No evidence for a significant moderating effect of training supervision, training frequency, session length, baseline depression severity, population, mean age, CCT type, country or trial pre-registration was found for overall cognition or mood, however these results should be interpreted with caution given the small number of studies in many subgroups.
Additionally, despite differences between subgroups not reaching statistical significance, an interesting finding regarding the moderating effect of baseline depression severity was that the observed effect size estimates for mild vs moderate-severe subgroups for overall cognition and mood were inverse, with larger benefits for overall cognition associated with mild baseline depression severity and larger benefits for mood associated with moderate-severe baseline depression severity. Moreover, as moderate heterogeneity was observed in the main analysis and in several of the domain-specific analyses future more detailed investigation of potential moderators may be warranted to determine population characteristics and design factors that influence specific cognitive and functional outcomes. Consistent with Thérond and colleagues20 we found CCT efficacious for overall cognition. Results of our analysis for mood were also consistent with previous meta-analyses19, although our effect size estimate is slightly smaller and more precise. Our results contrast previous19,20 findings that CCT efficacy on overall cognition declines slightly with age, as well as Motter and colleagues19 imprecise and non-significant findings for executive function. However, these meta-analyses were based on substantially smaller numbers of studies and included studies other than RCTs and cognitive interventions other than CCT. Small to moderate effect size estimates on executive function, long-term memory and retrieval and general short-term memory, suggest that CCT can benefit cognitive abilities commonly impaired in both symptomatic and remitted states of depression2. Furthermore, the moderate effect size estimate found for psychosocial functioning is particularly encouraging as both symptomatic and remitted states of depression are associated with poor psychosocial functioning2 and the psychosocial burden of comorbid depression in chronic diseases often poses challenges to care provision7.
Our results also show the beneficial effect of CCT to be similar to, or in the case of a sub-group analysis of RCTs of people with depression, to be greater than, the effect of antidepressants on overall cognition6. Additionally, no cognitive benefit of antidepressants in people with depression has been found for working memory6, a domain often impaired in people with depression2. Thus, the significant moderate effect sizes that were found in our analysis for the broad domain general short-term memory and narrow domains high working memory and low working memory are particularly encouraging. Furthermore, unlike antidepressants, which have toxicity risks and are associated with unwanted side-effects, such as weight gain and sedation, CCT is safe and has no side-effects.
To the best of our knowledge, this is the first systematic review and meta-analysis of RCTs investigating CCT in people with depression across a range of cognitive and functional outcomes, thus providing a comprehensive synthesis of the current evidence. Unlike previous reviews that included various research design and cognitive interventions19,20, we employed strict eligibility criteria, allowing a robust evaluation of the efficacy of CCT in people with depression across various cognitive and functional outcomes as well as an examination of population characteristics and design factors that may moderate efficacy. Nonetheless, some limitations should be addressed. First, since most studies focused on short-term cognitive and functional outcomes, the durability of the observed benefits on cognition and functioning as well as long-term outcomes, such as reduced conversion to dementia, is unknown. Second, the included studies employed a variety of CCT programs targeting different cognitive domains, thus further dismantling of the specific CCT components that make up an efficacious intervention for various cognitive and functional outcomes in people with depression remains an important area of investigation, which could be explored through individual patient data meta-analysis. Third, many studies did not report functional outcomes, leaving pooled analysis for daily functioning unable to be conducted and results of analyses of psychiatric symptoms, psychosocial functioning and subjective cognition underpowered and to be interpreted with caution. Fourth, only three studies46-48 specifically focused on people with partially and/or fully remitted depression, leaving subgroup analysis for this population also underpowered. Future studies should make efforts to include functional outcomes as well as cognitive outcomes and to investigate the durability of effects of CCT in both symptomatic and remitted states of depression.
Overall, CCT is efficacious for improving overall cognition, mood, psychosocial functioning and domain-specific cognitive function in abstract reasoning, learning/encoding efficiency, retrieval fluency, high working memory, low working memory, inhibition and processing speed in people with depression. Efficacy data for psychiatric symptoms, subjective cognition, global cognition and domain-specific cognitive function in short-term memory and shifting are inconclusive, and no analyses for daily functioning or verbal reasoning, updating and visual processing domains were conducted due to a lack of reported outcomes. Furthermore, greater efficacy for overall cognition can be expected from higher doses of CCT.
Data Availability
Supplementary tables and figures are available from the link below.
REFERENCES



