
Abstract
Background Drug-resistant focal epilepsy is often caused by focal cortical dysplasia (FCD). The impact of FCD location on clinical presentation and surgical outcome is largely unknown. We created a large neuroimaging cohort of patients with individually mapped FCDs to determine predictors of lesion location and postsurgical seizure freedom to aid presurgical decision-making.
Methods The Multi-centre Epilepsy Lesion Detection (MELD) project collated a retrospective cohort of 580 patients with epilepsy due to FCD from 20 epilepsy centres worldwide. MRI-based maps of individual FCD lesions with accompanying demographic, clinical and surgical information were collected for each patient. We mapped the distribution of FCD lesions across the cerebral cortex and examined for associations between clinical factors and lesion location.
Findings FCDs were non-uniformly distributed across the brain, concentrating in the superior frontal sulcus, frontal pole and temporal pole. Age of epilepsy onset was typically before age 10. Earlier epilepsy onset was associated with lesions in primary sensory areas while later epilepsy onset was associated with lesions in association cortices. Lesions in temporal and occipital lobes tended to be larger than frontal lobe lesions. Seizure freedom rates varied with FCD location, being around 30% in visual, motor and premotor areas to 75% in superior temporal and frontal gyri. These differences are likely attributable to reduced resection volumes due to neurosurgical caution around eloquent cortex.
Interpretation The MELD project has gathered the largest neuroimaging cohort of patients with FCD to date. The location of the FCD is non-uniformly distributed across the cerebral cortex and is an important determinant of its size, the age of epilepsy onset and the likelihood of seizure freedom post-surgery. Using an open-science collaborative initiative, we have characterised the spatial distribution of a focal pathology to identify data-driven, patient-specific predictors of lesion location and postsurgical seizure freedom to inform clinical decision-making.
Funding Rosetrees Trust
Evidence before this study To identify previous research on lesion location and surgical outcome in FCD, we searched PubMed using the terms “focal cortical dysplasia” OR “FCD”, AND “location” OR “lobe”, AND “outcome”. The search was for full manuscripts from database inception until 24 November 2020 without language restrictions and yielded 307 results. Only five papers had sample sizes of over 200 patients with focal cortical dysplasia. All five studies found that temporal resections are associated with better postsurgical seizure freedom. However, four of these studies limit lesion localisation to temporal and extra-temporal, with none describing lesion location beyond coarse lobar categorisations.
Added value of this study This is the first study to map the distribution of FCD lesion locations across the cerebral cortex in a large cohort of patients, and provide a 3D probability map of the non-uniform distribution of lesions across the cerebral cortex. We demonstrate that the location of a FCD is significantly associated with age of epilepsy onset and is a predictor of postoperative seizure freedom. Our openly available methodological developments provide novel tools for linking focal neurological abnormalities to their clinical presentation and subsequent surgical outcome.
Implications of all the available evidence Neuroimaging of patients with drug-resistant epilepsy should be carefully reviewed by radiologists to look for structural aetiologies, such as FCD, which are amenable to surgery. As our study showed FCDs are non-uniformly distributed across the cerebral cortex, our probability map can help radiologists in the clinical search for FCDs, which can be subtle lesions. Lesion location is significantly associated with age of epilepsy onset and post-operative seizure freedom. Individualised, patient-specific predictors of lesion location and surgical outcome will ultimately improve the diagnosis, prognosis and treatment of patients with complex neurological conditions.
Introduction
Epilepsy is one of the most common neurological conditions, with a lifetime risk of 1 in 26.1 Focal cortical dysplasia (FCD) is a malformation of cortical development and a common cause of drug-resistant epilepsy.2,3 In many patients, FCD is amenable to surgical resection, with reported long term seizure freedom rates of 69%.4
FCDs can be categorised into distinct histopathological subtypes.2 FCD Type I is characterised by cortical dyslamination, FCD Type II by dysmorphic neurons and dyslamination, and is subdivided into IIa and IIb, with the latter having balloon cells. FCD Type III is associated with another principal lesion, e.g. hippocampal sclerosis.
FCDs can occur anywhere in the cerebral cortex, but different histopathological subtypes show some lobar specificity.2,3 FCD Type II lesions are more frequently found in the frontal lobe, whereas FCD Type I and III are more frequently located in the temporal lobe. To date, most studies analysing localisation used coarse lobar categorisations4 or have been limited by small sample sizes5. Despite anatomical mapping of lesions being available using presurgical MRI6–8 and the emergence of large collaborative neuroimaging studies,9 these techniques have not been used to map the topography of FCDs.
The gold-standard treatment for drug-resistant epilepsy is surgical resection.10 However, a significant proportion of patients (31% of FCD Type II and 42% of FCD Type I)4 continue to have seizures post-operatively. Identifying factors relating to seizure freedom is important. Some can be modified to improve patients’ clinical and surgical treatment. Others can be incorporated into machine-learning models to produce patient-specific predictions of seizure freedom for use in clinical planning and risk counselling. Across all focal epilepsies, duration of epilepsy, age at surgery, lesion lobe and histopathological diagnosis are predictors of postsurgical freedom.4 Within FCD, the most consistent predictive factors include complete resection of the FCD,11,12 temporal resections,13,14 having an MRI visible lesion15 and the underlying histopathology being FCD Type II.4 However, the relationship between precise lesion location and seizure freedom is unknown.
Detailed spatial mapping of FCD lesions would broaden our understanding of this disease, enabling linkage of a patient’s lesion location to presurgical clinical information. To this end, we created the Multi-centre Epilepsy Lesion Detection (MELD) project to collate a large neuroimaging cohort of patients, including MRI lesion maps with demographic, clinical and surgical variables. We aimed to 1) map the topographic distribution of epileptogenic FCDs across the cerebral cortex, 2) identify clinical predictors of lesion location and 3) establish predictors of post-surgical seizure freedom.
Methods
1. MELD project consortium
We established the MELD project (https://meldproject.github.io/) involving 20 research centres across 5 continents. Each centre received approval from their local institutional review board or ethics committee. Written informed consent was provided according to local requirements.
2. Participants
Patients over age 3 were included if they had a 3D preoperative T1-weighted MRI brain scan (1·5T or 3T) and a radiological diagnosis of FCD or were MRI-negative with histopathological confirmation of FCD. Participants were excluded if they had previous surgeries, large structural abnormalities in addition to the FCD or T1 scans with gadolinium-enhancement. Centres and patients were given pseudo-anonymised ID codes.
3. Site-level data collection and post-processing
MRI data collection and post-processing
T1-weighted MRI scans were collected at the 20 participating centres for all participants and cortical surfaces were reconstructed using FreeSurfer.16 Detailed protocols for structural MRI post-processing were adapted from openly available ENIGMA-epilepsy protocols.9
FCD lesion masking
FCD lesions were delineated on the T1-weighted MRI scans at each site according to our lesion masking protocol.17 For patients with a radiological diagnosis of FCD, a volumetric lesion mask was created using the preoperative T1 scan and 3D FLAIR (where available). For MRI-negative patients but with histopathological confirmation of FCD, the post-operative scan and other corroborative evidence, such as EEG and PET, were used to create the volumetric lesion mask. Volumetric lesion masks were mapped to cortical reconstructions and small defects were filled in using five iterations of a dilation-erosion algorithm. Patients’ lesions were registered to a bilaterally symmetrical template surface, fsaverage_sym.
Participant demographics
The following data were collected for all patients: age at preoperative scan, sex, age of epilepsy onset, duration of epilepsy (time from age of epilepsy onset to age at preoperative scan), ever reported MRI-negative and histopathological diagnosis (ILAE three-tiered classification system),2 seizure-freedom (Engel class I) and follow-up time in operated patients.
Participant demographic information and lesion masks were shared with the study coordinators for multi-centre analysis. At the point of retrieval by the study coordinators, all participant data were deidentified, as keys linking pseudo-anonymised IDs to patient identifiable information were stored securely by individual sites.
4. Location of focal cortical dysplasias in the cerebral cortex
Lesion masks from all patients were overlaid on the left hemisphere of the template cortical surface to visualise the distribution of lesions for all FCDs, as well as for histopathological subtypes (see Methods Section 5 for tests of interhemispheric asymmetry). Additional surface-based lesion maps for left and right hemispheres were generated for the whole cohort, patients who had and those who had not undergone resective surgery.
Lobar categorisations of lesion location were created based on the lobe which contained the most lesional vertices. For statistical comparisons of lobar location, lesions primarily located in the smallest lobes in the parcellation (cingulate and insula) were assigned to a second lobe (e.g. frontal) which the lesion mask also overlapped.
For the creation of a 3D lesion likelihood atlas, aggregated surface-based lesion map values were normalised to between 0 and 1, where the location with the highest number of FCDs had a value of 1. This lesion likelihood atlas was mapped back to the template MRI volume for use as a potential clinical aid in guiding radiological diagnosis.
Bootstrap reproducibility was used to assess the consistency of the overall spatial distribution of FCDs. FCD frequency maps from subsets of 20 to 250 patients were correlated with the map from a subset of 250 patients. This process was randomised and repeated 1000 times. Unstable maps had low correlations and indicated that the sample size was too small. A predictive learning curve was fitted to the R values of different subcohort sizes and interpolated to determine the sample size required for a consistent spatial distribution in the lesion pattern.18
5. Factors associated with lesion distribution
We trained logistic regression models to test for associations between lesion location and clinical data (Supplementary Figure 1). The model was fitted to assess which preoperative factors are associated with the presence or absence of lesions at a particular vertex (a point on the cortical surface). The following preoperative factors were included: age of epilepsy onset, sex, ever reported MRI-negative, duration of epilepsy and lesion hemisphere. Regression coefficients were tested for significance against those calculated on 1000 randomly permuted cohorts. Factors were deemed significant if their coefficient was less than 2·5% or greater than 97·5% of the coefficients from permuted cohorts. Approximately 5% of vertices would be significant by chance. A given factor was considered significantly related to lesion location if the number of significant vertices exceeded the 100-(5/nth) percentile number of significant vertices from the permuted cohorts, where n was the number of factors being tested.

A) Logistic regression model including age of epilepsy onset, sex, ever reported MRI-negative, duration of epilepsy and lesion hemisphere was fitted to predict the presence / absence of a lesion at every vertex. B) 1000 permuted cohorts created where presence / absence of a lesion at a particular vertex is random. C) Normal distribution of coefficients from permuted cohorts at vertex i. The coefficient from actual data (red) is greater than 97·5% of the coefficients from the permuted cohorts, and therefore vertex i is considered significant. D) Normal distribution of the percentage of vertices that were significant for a particular factor (e.g., age of onset) in the permuted cohorts. The factor (red) was considered significantly related to lesion location as the number of significant vertices exceeded the 99th percentile value from the permuted cohorts.
Post-hoc analysis of significant factors included testing for similarity between the surface-based map of the factor of interest (e.g. mean age of epilepsy onset or duration of epilepsy) and potential explanatory variables (e.g. the principal gradient of functional organisation from primary to association areas19 or mean lesion size). To account for spatial autocorrelation, statistical significance was established by comparing correlations with those from 1000 spherically rotated maps.20
6. Factors associated with seizure freedom
Using the cohort of operated FCD patients with seizure outcome and histopathological diagnosis, we calculated the proportion of patients who were seizure free with lesions at each vertex. We fitted a logistic regression model to predict seizure freedom using the following factors: duration of epilepsy, MRI-negative status, age at preoperative scan, histopathological FCD subtype and lesion lobe. We calculated the predicted percentage likelihood of seizure freedom from the logistic regression model for each patient.
To assess the association of lesion location with post-surgical seizure freedom, logistic regression models were fitted to predict seizure freedom at each cortical vertex based on which patients had lesions. Statistical significance for these regression models was established using the same permutation procedure as in Methods Section 5.
7. Data-driven search for inter-relationships between demographic, lesional and surgical variables
Relationships between demographic, lesion and surgical variables were systematically analysed (Figure 4B). Heavily skewed variables were normalised for statistical testing using a Box-Coxtransform. The Benjamini-Hochberg procedure was used to control the false discovery rate when conducting multiple comparisons, with α set to 0·05.21
8. Code
All data analysis was performed in Python using the following packages: NumPy, scikit-learn, scipy, pandas, nibabel, matplotlib, seaborn, PritPrince. All code for MELD preprocessing and Prediction Of Outcome & Location (POOL) is available to download from www.github.com/MELDProject.
Results
1. Participant demographics
Data was collected from 580 FCD patients. Demographic information is available in Table 1. Histopathological diagnosis was available in 380 patients (66%, Table 2). Post-surgical outcome data was available in 319 patients (75% of operated patients); 69% were seizure free (Engel class 1) at last follow-up (median follow up = 2 years). Seizure freedom rates across histopathological subtypes are presented in Table 2. Although FCD Type I had a lower mean seizure freedom (63%) than FCD Type IIA (70%) and FCD Type IIB (69%), there was no significant difference in outcome according to histopathological subtype.
Demographics Table
Histopathology and surgical outcome
2. Location of focal cortical dysplasias in the cerebral cortex
FCDs were evenly distributed between left and right hemispheres across the 548 patients with lesion masks (L:R 266:282). 32 patients did not have lesion masks and were excluded from subsequent analyses. Lesions were located throughout the cortex (262 frontal, 158 temporal, 90 parietal, 20 occipital, 10 cingulate, 8 insula). For visualisation, all lesions were mapped to the left hemisphere of fsaverage_sym (Figure 1A). The distribution of lesions was non-uniform, with propensity for FCDs in the superior frontal sulcus, frontal pole, temporal pole and superior temporal gyrus (Figure 1A & B). Lesion maps were unstable at sample sizes typical for neuroimaging cohorts of FCD, but improved as sample size increased (Figure 1C). A predictive learning curve determined that a sample size of around n=400 would be required for a stable distribution of lesions across the cortex. This provided support that our cohort (n=548) is sufficient to be representative.

A) All FCD lesion masks mapped to the left hemisphere of the template cortical surface. The distribution of FCDs across the cerebral cortex is non-uniform and with higher concentrations in the superior frontal sulcus, frontal pole, temporal pole and superior temporal gyrus. B) 3D lesion likelihood atlas. Aggregated surface-based lesion map values were normalised to between 0 and 1 and mapped back to the template MRI volume. C) Sample size required for consistent FCD lesion map. Rank correlation (y axis) was calculated by comparing the lesion map from a smaller cohort to a larger withheld cohort (n=250). rrank increased with sample size. Predictive learning curve (red line) estimated that a stable map of lesion distribution requires a sample size of n=400. D) Distribution of FCD lesions according to histopathological subtype. E) Distributions of lesions across cortical lobes within each FCD histopathological subtype. The width of bars indicates the relative numbers of patients. Temporal lobe lesions made up larger proportions of FCD Types I and III, while frontal lobe lesions were more likely to be FCD Types IIA and IIB.
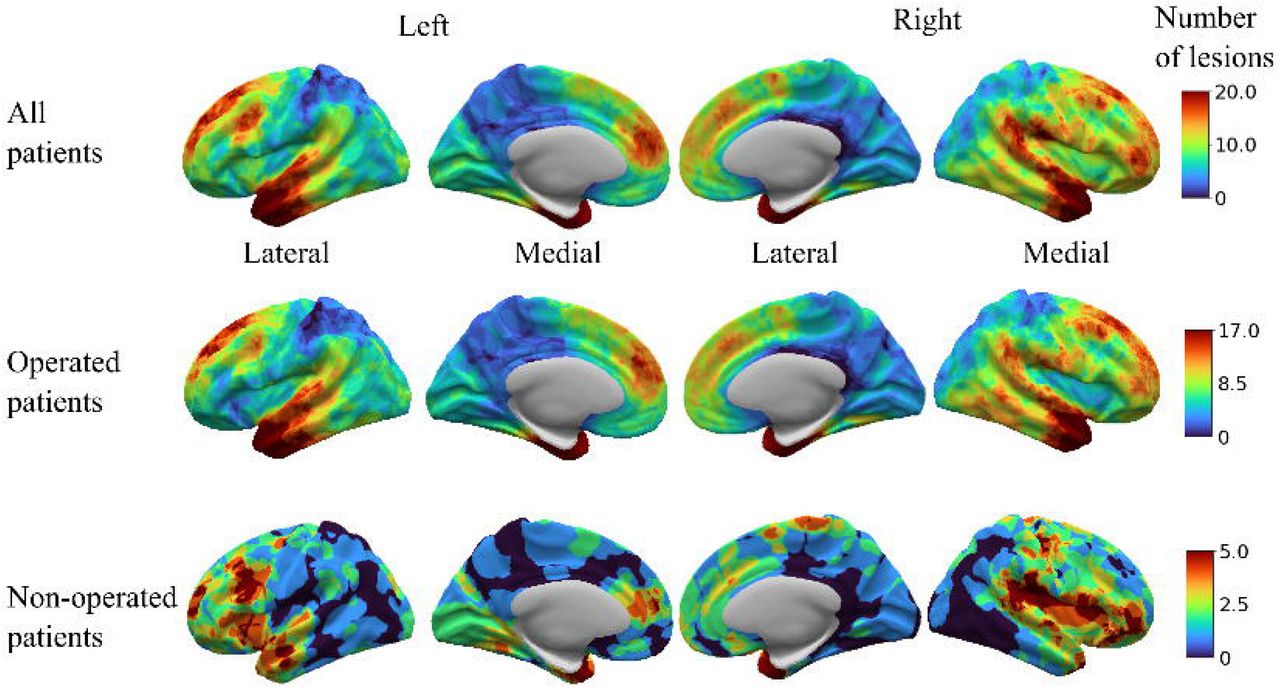
Lesion maps of histopathological subtypes (Figure 1D) showed that the distribution of FCD lesions across the cortex differs according to histopathological subtype, with a greater proportion of FCD Types I and III lesions located in the temporal lobe (Figure 1E). In the group of non-operated patients, lesions were most frequently located in the left inferior frontal gyrus and bilateral insula (Supplementary Figure 2). While numbers in this cohort were relatively small, this may represent deliberate avoidance of surgery in language areas and/or challenges in the diagnosis or surgical planning of insula lesions.

Distributions of FCD lesions on left and right hemispheres in the whole MELD cohort, patients who had undergone surgery and those that had not. The pattern in the whole and operated cohorts appear symmetric, whereas patients who had not undergone surgery appeared to have more lesions in left inferior frontal gyrus, near Broca’s area. Additionally lesions in the non-operated cohort appear to be more frequently located in the insula, a diagnostically and surgically challenging area for cortical resection.
3. Relationships between demographic variables and lesion distribution
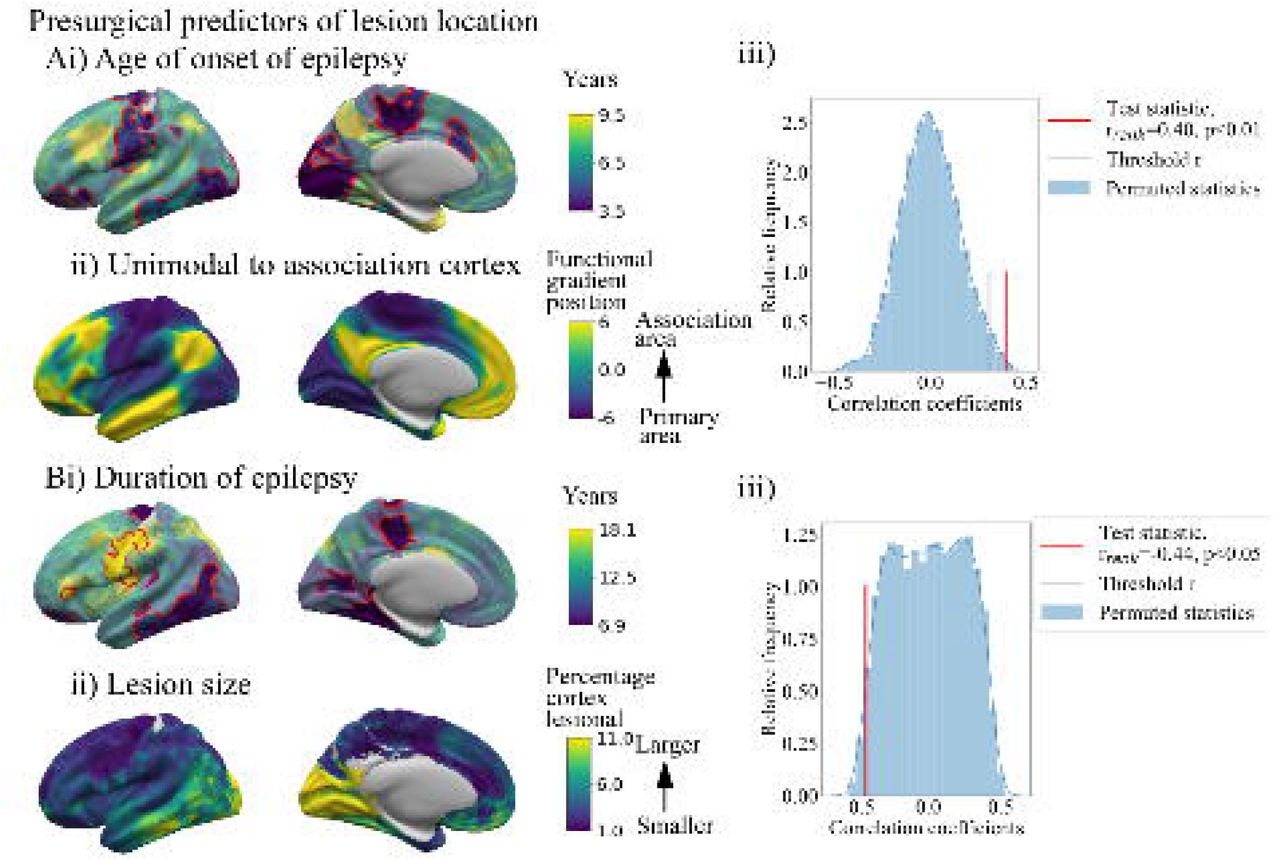
Age of epilepsy onset and duration of epilepsy were significantly related to lesion location (number of significant vertices > expected by chance p<0·01) (Figure 2). Hemisphere, sex and ever reported MRI-negative were not. The age of onset map was significantly correlated with the principal gradient of functional cortical organisation (Figure 2A).19 Lesions in primary areas were associated with a younger age of onset, while association areas had older ages of onset (rrank=0·40, pspin<0·01). Overall, lesions in temporal, parietal and occipital cortices were associated with a shorter duration of epilepsy (Figure 2B), whereas lesions around the central sulcus and frontal lobe were associated with a longer duration of epilepsy. This pattern closely resembled the distribution of lesion size, whereby cortical areas associated with longer durations like the frontal lobe tended to have smaller lesions (Figure 2B, rrank=-0.44, pspin<0·05).

Ai) Lesion location was significantly associated with the age of epilepsy onset (p<0·001). Vertices outlined in red are significant after comparison with 1000 randomly permuted cohorts. ii) Primary gradient of functional organisation from primary sensory-motor areas to association cortex. iii) Correlation between maps Ai) & Aii) compared to spatially permuted maps. Age of epilepsy onset for lesions in primary sensory-motor areas was significantly younger, with older age of epilepsy onset for lesions in association areas (rrank=0·40, pspin<0·01). Bi) Lesion location was significantly associated with the duration of epilepsy prior to surgery (p<0·001). Lesions located in precentral and frontal areas were associated with a longer duration of epilepsy, while occipital and temporal areas were associated with a shorter duration of epilepsy. ii) Mean size of lesion across the cortex. iii) Correlation between maps Bi) & Bii) compared to spatially permuted maps. Mean duration was significantly negatively correlated with the size of epilepsy lesion, where cortical areas with larger lesions had shorter durations of epilepsy (rrank=-0·44, pspin<0·05). Prolonged durations of epilepsy with smaller lesions may arise due to difficulties in presurgical diagnosis including identification of the abnormality on an MRI scan.
4. Factors associated with seizure freedom
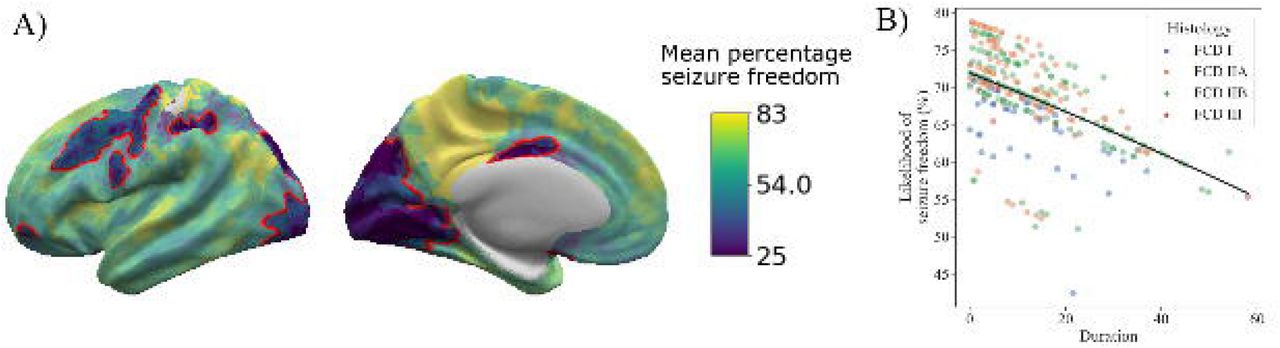
The percentage of patients who were seizure free post-surgery varied according to lesion location and, therefore, the area of cortex resected (Figure 3A). Visual, motor and some premotor areas were associated with significantly lower seizure freedom rates (30-40% of patients were seizure free), likely reflecting conservative resection around eloquent cortex. The logistic regression model fitted with the duration of epilepsy, histopathological diagnosis and lesion lobe, was consistent with previous findings, where seizure freedom decreased with longer duration of epilepsy (Figure 3B, β = -0·73, p<0·05). A 10-year increase in duration of epilepsy was associated with a 3% decrease in likelihood of seizure freedom. In contrast to the precise lesion locations, the more coarse categorisation of lesion locations by lobe was not significantly associated with seizure freedom.

A) Percentage of patients seizure free (%) according to lesion location across the cerebral cortex. Visual, motor and premotor areas had a low percentage of seizure free patients (30-40%). Superior temporal and superior frontal gyri had a high percentage of seizure free patients (70-80%). B) Impact of duration and histopathology on predicted percentage likelihood of seizure freedom, with logistic regression model fit using the duration of epilepsy, histopathological subtype, age of epilepsy onset, ever reported MRI-negative and lobe. Longer duration was significantly associated with poorer chance of seizure freedom (p<0·05). No significant effect of histopathology was identified.
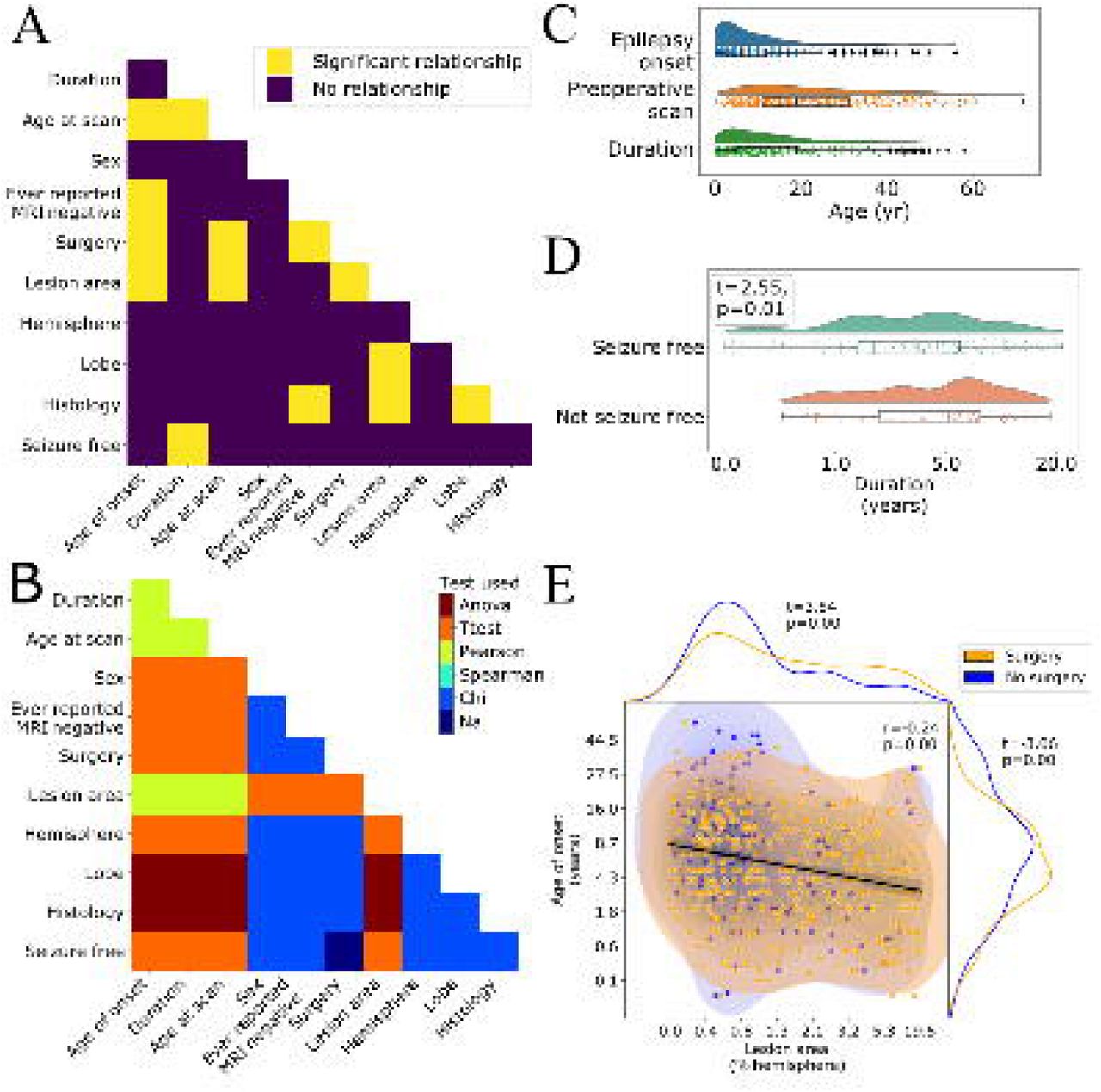
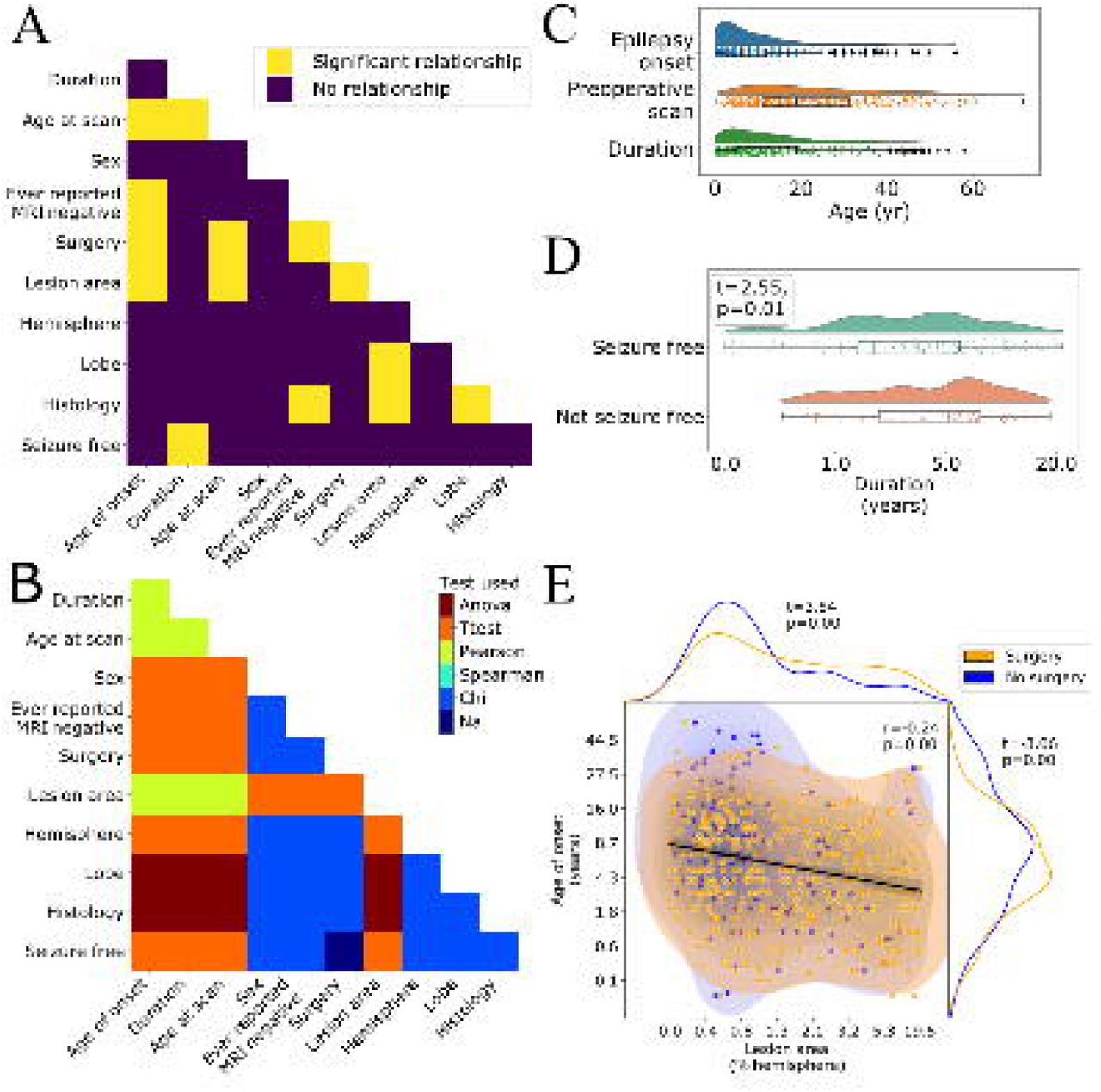
A) Pairwise comparison of demographic and clinical features. Significant relationships after correction for multiple comparisons are shown in yellow. B) Statistical test used for each pairwise comparison. C) Distributions of age of epilepsy onset, age at preoperative scan and duration of epilepsy. D) Duration of epilepsy is significantly associated with seizure freedom (t=2·55, p=0·01). Patients with longer durations of epilepsy are less likely to be seizure free. E) Age of epilepsy onset, lesion area (as a percentage of the total hemisphere size) and seizure freedom are significantly associated. Larger lesions are associated with younger age of epilepsy onset (r=-0·24, p<0·01) and are more likely to be operated (t=3·54, p<0·01). Similarly, patients with a younger age of epilepsy onset are more likely to be operated (t=-3·06, p<0·01).
5. Inter-relationships between demographic, lesional and surgical variables
Figure 4A displays significant relationships between demographic, lesional and surgical variables after systematic evaluation of all inter-relationships. Full statistics are reported in Supplementary Figure 3. Results of interest have been highlighted below.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Test statistics and uncorrected p values are displayed. See Figure 4 for a more detailed exploration of findings.
Relationships with age at preoperative scan
The distributions of age at epilepsy onset, age at preoperative scan and duration of epilepsy revealed that overall there was a long interval between patients developing epilepsy and having their preoperative scan (Table 1, Figure 4C). While 68% of patients have epilepsy onset before age 10, 51% of patients wait over 10 years before having their preoperative scan and consequently undergoing presurgical evaluation. There was a small but significant negative correlation between age at scan and lesion surface area (r=-0·17, p<0·001), i.e., patients with larger lesions had presurgical evaluation younger. Older patients were less likely to have had surgery (t=-3·55, p<0·001).
Relationships between lesion size, histopathology, surgery and ever reported MRI-negative
Patients with earlier epilepsy onset had larger lesions (r=-0·24, p<0·001, Figure 4E), were less likely to have ever been reported MRI-negative (t=-3·70, p<0·001) and more likely to have had epilepsy surgery (t=-3·38, p<0·01, Figure 4E). Patients with larger lesions were more likely to have had surgery (t=3·69, p<0·001, Figure 4E). FCD Type IIA were more likely to have been MRI-negative than FCD Type IIB (χ2=12·2, p<0·01, Tukey’s post-hoc, p<0·01).
Relationships with lesional lobe
Lesion surface area was significantly associated with lobe (F=6·12, p<0·001), driven by temporal lobe lesions being larger than frontal (Tukey’s post-hoc p<0·01) and parietal lesions (Tukey’s post-hoc p<0·05). FCD Type I and III lesion more frequently located in the temporal lobe (Chi 70·2, p<0·001, Tukey’s post-hoc p<0·001, Figure 1E).
Predictors of seizure freedom
Patients with longer durations of epilepsy were less likely to be seizure free (t=-2·55, p<0·01). No other factors survived correction for multiple comparisons (Supplementary Figure 3).
Discussion
In this multi-centre study of 580 patients with FCD, lesions were non-uniformly distributed across the cerebral cortex, with predominance in the superior frontal sulcus, frontal pole and temporal pole. Vertex-specific lesion location was significantly associated with age of epilepsy onset and duration of epilepsy. Likelihood of seizure freedom post-operatively varied considerably according to lesion location, with lesions in visual, motor and premotor areas associated with much lower rates of seizure freedom than elsewhere, likely attributable to neurosurgical caution in resecting lesions around eloquent cortex.
The map of FCD lesion locations highlights a non-uniform distribution across and between cortical lobes. It substantiates previous studies finding that FCDs were more common in frontal (particularly FCD Type II) and temporal (FCD Types I & III) lobes.3,4 Additionally, these maps extend previous understanding, demonstrating “hot-spots” in the superior frontal sulcus driven by FCD Type IIB, and a cluster of temporal pole lesions in all FCD subtypes. Surface and volumetric atlases of FCD lesion locations offer a resource for guiding the clinical search for FCDs and research into the underlying neurobiology of malformations of cortical development. Our unique dataset linking individual clinical and demographic data with lesion location uncovered relationships between age of epilepsy onset, duration of epilepsy and lesion location. Lesions in primary sensory, motor and visual areas were associated with younger epilepsy onset, while lesions in higher-order association cortex were associated with later epilepsy onset. This relationship may reflect differing developmental trajectories of these areas,22,23 with seizures initiating as a result of the development of particular cortical properties. However, differing seizure semiologies may be a contributing factor, where more subtle seizure symptoms are not attributed to a diagnosis of epilepsy for longer.
Most patients had epilepsy onset during childhood (median onset = 6·0 years), but the median age at preoperative scan was 19·0 years (Table 1), indicating many patients had long delays between epilepsy onset and potentially curative epilepsy surgery (Figure 4C, median duration = 10·4 years). Longer duration of epilepsy is associated with increased morbidity, mortality and with worse postsurgical outcome (Figure 3B & 4A).4,24 In our cohort, patients with a longer duration of epilepsy were more likely to have lesions in the frontal cortex, particularly around the central sulcus. Factors contributing to longer duration of epilepsy might include diagnostic and surgical challenges such as lesion conspicuity, MRI scanning protocol and whether a lesion is in eloquent cortex. Other reasons might include trials of anti-epileptic drugs, alongside under and delayed referral to specialist epilepsy centres.25
Consistent with a recent study,4 69% of patients with FCD in the MELD cohort were seizure free post-surgically. We found that a longer duration of epilepsy was significantly associated with a reduced chance of seizure freedom (Figure 4A), but the impact of duration was small, with a 3% decrease in likelihood of seizure freedom for every 10 year increase in duration of epilepsy (Figure 3B). By contrast, differences in lesion location were associated with large shifts in mean seizure freedom, from 30% in visual, motor and premotor areas to 80% in temporopolar regions. These findings support the incorporation of precise, i.e., per vertex or sub gyral, lesion locations into pre-operative seizure freedom scores.26
Lesions in visual, motor and premotor areas were associated with low likelihoods of seizure freedom. The most likely reason is that these lesions were in eloquent cortex or close to white matter tracts such as the optic radiation or corticospinal tracts, and as such neurosurgeons may have been intentionally cautious with their resections to minimise the risk of deficits such as hemiparesis or hemianopia.27 Additionally, the medial occipital and cingulate areas are located on the medial wall of the cortex, restricting ease of surgical access. Both factors could contribute to higher rates of incomplete resections of the dysplastic tissue known to be associated with worse postsurgical outcome.11
One strength of our study is the inclusion of operated and non-operated patients. This helped to minimise ascertainment bias in the dataset, as the lesional distribution of non-operated patients captured more lesions in eloquent cortex (e.g. left inferior frontal gyrus) or cortex which is more surgically challenging to resect (e.g. insula, Supplementary Figure 2), while purely post-surgical cohorts may miss these lesions. However, it is important to note that our cohort primarily consisted of patients with epileptogenic, drug-resistant FCDs. Future work is needed to establish the distributions of non-epileptogenic or drug-responsive FCDs which may not present to epilepsy surgery centres.
One limitation is the number of clinical variables collected. Future work including more detailed clinical information, such as seizure types, seizure burden, electrophysiology, medication, genetics and extent of lesion resection might further our understanding of FCD and enable the development of predictive models for seizure freedom. Additionally, the clinical variable “ever reported MRI-negative” is imperfect, depending on MRI protocols and the expertise of radiological review. Nevertheless over a large sample size, it does indicate that some lesions were more subtle. From our data FCD Type IIB was less likely to be MRI-negative, and therefore there may be an ascertainment bias in our dataset, with an overrepresentation of FCD Type IIB.
As a subtle pathology on MRI, manual masking of FCD lesions is challenging. There is likely to be some heterogeneity in the masking process. At each site lesions were delineated by different individuals. Additionally, for some lesions that were difficult to detect on MRI delineation of the lesion boundaries was guided by post-surgical resection cavities. By contrast, other lesions might extend beyond what was visible. Future studies using automated lesion detection and masking7 may yield more observer-independent and consistent lesion masks. Nevertheless, the stability of the lesional overall cohort pattern (Figure 1C) indicates that the core findings of this study are robust to idiosyncrasies of particular lesion masks.
Large collaborative initiatives have shown the power of big data to answer clinically relevant questions.9,28,29 Here open-science practices enabled mapping of the topographic distribution of epileptogenic FCDs across the cerebral cortex, a departure from the coarse, lobar annotations usually described. We have demonstrated the utility of this map along with clinical variables for mechanistic research and to identify factors impacting the likelihood of post-surgical freedom.
Data Availability
Code to reproduce all analyses and figures in this manuscript is available to download from github.com/MELDproject. Requests can be made for access to the full MELD dataset.
Data sharing statement
Lesion maps for the whole cohort are freely available to download from the UCL data repository. Code to reproduce all analyses and figures in this manuscript is available to download from github.com/MELDproject. Requests can be made for access to the full MELD dataset.
Author contributions
KSW and SA verified the data and contributed to the literature search, study design, data collection, data analysis, data interpretation, and writing. KJW, AR, JS, PEV, JHC and TB contributed to the study design, analysis strategy, data interpretation and writing. All other authors contributed to data collection, data preprocessing, data interpretation and provided feedback on the manuscript.
Funding and acknowledgements
The MELD project is supported by the Rosetrees Trust (A2665). We are grateful to ENIGMA-Epilepsy for paving the way for collaborative neuroimaging cohorts in epilepsy and open protocols. This work is supported by the NIHR GOSH BRC. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health. KSW is supported by the Wellcome Trust (215901/Z/19/Z). XY, NYC & WDG were supported by the Hess Foundation. FC and CY were supported by the São Paulo Research Foundation (FAPESP), Grant # 2013/07559-3 (BRAINN - Brazilian Institute of Neuroscience and Neurotechnology). JOM is supported by a Sir Henry Dale Fellowship jointly funded by the Wellcome Trust and the Royal Society (Grant Number 206675/Z/17/Z) and received support from the Medical Research Council Centre for Neurodevelopmental Disorders, King’s College London (grant MR/N026063/1). PEV is a Fellow of MQ: Transforming Mental Health (MQF17_24) and of the Alan Turing Institute funded by EPSRC grant EP/N510129/1. JJM and KZ are funded by the National Natural Science Foundation of China (No. 82071457). PS acknowledges the DINOGMI Department of Excellence of MIUR 2018-2022 (legge 232 del 2016). GW is supported by the MRC (G0802012, MR/MR00841X/1). KJW is supported by The Alan Turing Institute under the EPSRC grant EP/N510129/1.
References




