
Abstract
Aim and Background We aimed at identifying vaccination strategies that minimize loss of life in the Covid-19 pandemic. Covid-19 mainly kills the elderly, but the pandemic is driven by social contacts that are more frequent in the young. Vaccines elicit stronger immune responses per dose in younger persons. As vaccine production is a bottleneck, many countries have adopted a strategy of first vaccinating the elderly and vulnerable, while postponing vaccination of the young.
Methods Based on published age-stratified immunogenicity data of the Moderna mRNA-1273 vaccine, we compared the established “one dose fits all” approach with tailored strategies: The known differential immunogenicity of vaccine doses in different age groups is exploited to vaccinate the elderly at full dose, while the young receive a reduced dose, amplifying the number of individuals receiving the vaccine early. A modeling approach at European Union scale with population structure, Covid-19 case and death rates similar to Europe in late January 2021 is used.
Results When the elderly were vaccinated preferentially, the pandemic initially continued essentially unchecked, as it was dominantly driven by social contacts in other age groups. Tailored strategies, including regular dosing in the elderly but reduced dose vaccination in the young, multiplied early vaccination counts, and even with some loss in protection degree for the individual person, the protective effect towards stopping the pandemic and protecting lives was enhanced, even for the elderly. In the European Union, pandemic duration (threshold >100’000 cases/day) was shortened from 53 to 18-24 days; cumulative death count over 100 days was reduced by >30’000. Data suggest that the findings may be relevant to both, the Moderna and the Pfizer-BioNTech mRNA vaccines.
Conclusion Protecting the vulnerable, minimizing overall deaths and stopping the pandemic is best achieved by an adaptive vaccination strategy using an age-tailored vaccine dose, in this model parameterized to European demographics, coronavirus transmission observations and vaccine characteristics.
Introduction
Faced with the Covid-19 pandemic, vaccines against SARS-Cov2 have been developed in unprecedented speed, and mRNA vaccines like the Pfizer BNT162b2 vaccine1(Tozinameran) and the Moderna mRNA-1273 vaccine2 have shown excellent immunogenicity, safety and protection against disease, and data indicating that they protect against virus transmission are accumulating. While vaccines development was rapid, vaccine production capacities are now the key bottleneck for national and global deployment. During development, dose optimization of the Moderna vaccine has been performed towards optimal protection of the elderly, exploring doses of 25, 50, 100 and 250ug, as the elderly show reduced immune response on vacccination3. Laboratory-assessed immunity levels typically exceeded those seen in the plasma of reconvalescent patients who have a protection of 83% for at least 5 months4. Immunogenicity in the young is even higher than in the elderly. Certain Covid-19 vaccination study populations have 76% protection against infection for at least four months5 despite some decline of the measured immunity parameter in the elderly, indicating that vaccination can protect against infection as well as against symptomatic disease, rendering vaccination a rational approach for stopping the pandemic. We noted that in the young, a 25µg dose of the Moderna vaccine elicited an immune response level at day 57 that was comparable to the immune response seen in patients older than 71 years at day 119 (Table), a group in which the vaccine achieves >86% protection. Likewise, published data for the Pfizer Tozinameran vaccine show strong immunogenicity6 at threefold reduced dose in the young. The interpretation that good immunogenicity translates into good protection is very plausible7,8,9, implying that in the young, having a stronger immune response, a lower vaccine dose may suffice to achieve sufficient protection. We therefore hypothesized that exploiting age-tailored vaccination dosing may allow multiplying the proportion of persons early and thereby may lead to improved pandemic control.
Note that the 25µg dose in the <55 year old elicits a similar or stronger immune response compared to the >71 years old at 119 days, and compares favorably with the immune levels found in convalescent plasma.
S-2P is the antigen encoded by the vaccine. RBD ELISA measures receptor-binding domain binding antibodies. PsVNA50 is the pseudovirus neutralization assay’s 50% inhibitory dilution. PRNT80 is the live-virus plaque-reduction neutralization testing assay’s 80% inhibitory dilution.
Methods
The pandemic was modeled using a discrete-time10,11, extended model inspired by the SEIR (“susceptible-exposed-infected-recovered”) approach with daily stepping, as shown in figure 1 and described in more detail in the supplement, incorporating separate, interacting age groups with age-specific immune levels triggered by vaccination or natural infection, and age-specific fatality rates. The model was initialized with population size and age structure according to the European Union with a population of 447’706’200, split into a cohort > 64 years “old” of 90’436’652 and 357’269’547 “young” persons ≤64, as reported in the EU Eurostat respository12. European Covid-19 case numbers were from the Johns Hopkins University CSSE dataset and were used to initialize the model to 195’000 per day as per mid January 2021. The infectious window after Covid-19 infection was assumed to be day one to day 7 days after infection. The model was run for 100 days.
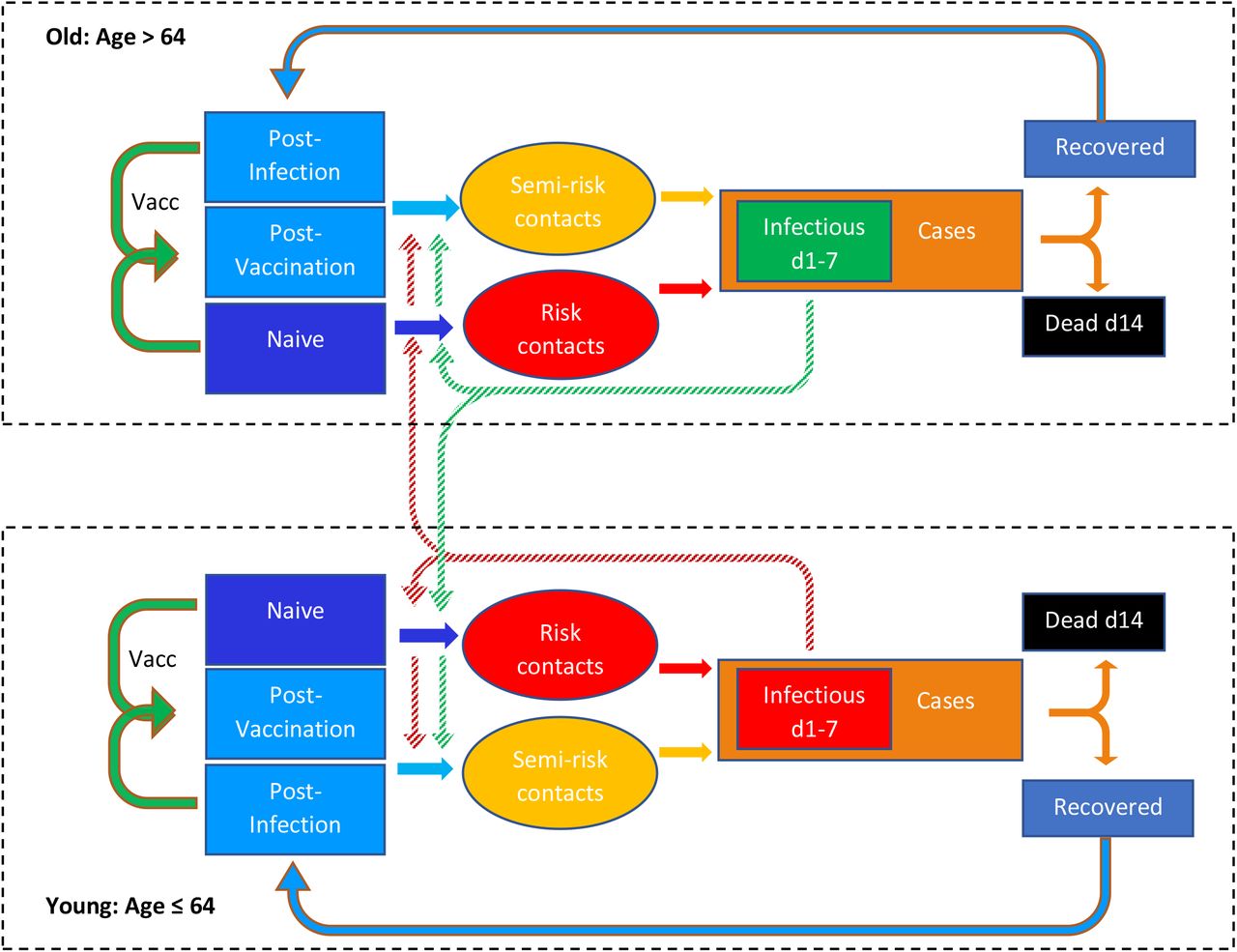
An extended, time-discrete version of the SEIR modeling approach. It incorporates 2 age strata and a tailorable degree of susceptibility in infection-naïve, vaccinated, and post-infection individuals. Protective efficacy of vaccination can be adapted to the age group and the vaccine dose, and vaccination campaigns can be modeled by daily setting the number of new vaccinations. Time lag and time window of infectivity after a risk contact is incorporated, and the time lag of deaths relative to diagnosis of new cases is incorporated. Social interaction within and between the age strata with cross-infection uses information on vaccination count and degree of susceptibility in each group. As protection by vaccination or prior infection is not 100%, the “semi-risk contacts” contribute to new cases. “Cases” rather than “infections” are used because this better allows parameterization of the model with real-world data. d1 and d14 indicate day 1 and day 14, respectively.
Young persons were set to have 80% of their social contacts with the “young” and 20% with the “old”13, while for the old, contacts to other elderly and the young were each assumed to be 50%. Daily transmissions for each age group were derived from the daily propensity of “risk contacts”, i.e., encounters of non-immune with infectious persons of either age group, plus, weighted by vaccine protection level, of “semi-risk contacts”, i.e., encounters of a vaccinated or previously infected with an infectious person. Deaths were based on the case fatality rate in the Europe in December 2020/January 2021, approximately 2·5% during a quasi-steady state in case numbers implying an R number near one. The age distribution of Covid-19 deaths was computed from age-dependent mortality taken from the European Center for Disease Prevention and Control situation dashboard14.
Four vaccination strategies were compared:
“one dose fits all”, using the standard vaccine dose, and starting with the old
Standard dose, starting with the young
“Adaptive”: half of vaccine supply for standard dose for vaccination of the old, plus half of the vaccine supply for vaccination of the young at quarter dose (thereby reaching more young persons early)
“quarter dose vaccination, only to the young”, a strategy that maximizes the number of vaccination in the young, i.e. the “frequent transmitters”, allowing for potential reduced vaccine efficacy in the individual person.
Vaccine stock is available for 1 million full dose vaccinations (Moderna, 2×100 µg) per day. Vaccination efficacy was parameterized with data reported by Moderna on phase I15,16,17,18,19 II and III20 studies. The interval from vaccination to protection was 10 days. Protective efficacy for the 100µg vaccine dose was 95·6% in the young and 86·2% in the elderly as reported; in one analysis, the vaccine efficacy for avoidance of transmission of a 25µg dose in the young was set to 86·2% based on the levels of immunogenicity achieved in the young compared to the immune response in the elderly vaccinated with 100µg; then, transmission blocking efficacies were varied between 30% and 90% for the 25µg dose in the young to explore the impact of blocking efficacy on strategy preference.
Ethics
According to a written statement from the relevant Ethical Kommittee Nordwestschweiz EKNW, computer modeling studies not including subjects do not fall under their ethical committee jurisdiction.
Results
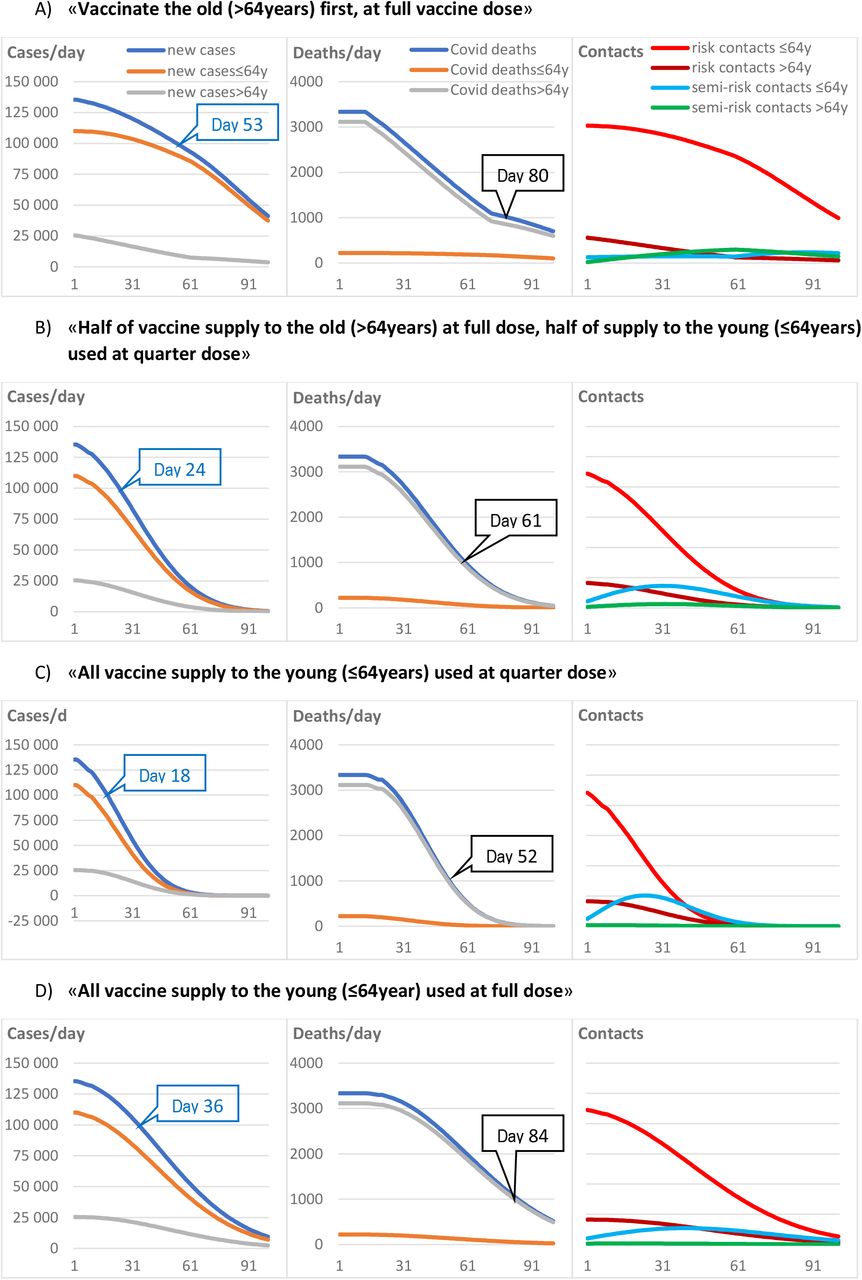
Results are summarized in the Figure 2.

Impact of different vaccination strategies on Covid-19 cases, deaths and the propensity of “risk contacts”. Panel A) vaccinating the elderly first leaves large population segments unprotected. Note that the prolonged spread of infection in the non-vaccinated young spills over to high case and death counts in the elderly that are not yet vaccinated or only partly protected by the vaccine.
Panel B) using half of the vaccine supply to vaccinate the elderly at full dose, and using the other half of the supply to vaccinate the young with a quarter dose, leads to a faster decline in cases and fewer deaths, even in the elderly.
Panel C) Using all vaccines for vaccinating the young with a quarter dose leads to faster reduction of overall case numbers, and thereby, indirectly, also protect the elderly after a sufficient overall vaccination rate is achieved, yielding low overall deaths.
Panel D) Compared to the best scenarios, using the full vaccine dose for vaccinating only the young (“the frequent transmitters”) is slower compared to the quarter dose strategies in stopping the pandemic despite being more protective for the individual person, and is associated with substantial death counts in the elderly.
“Risk contact” designates an encounter of a non-immune with an infectious person, and “semi-risk contact” designates an encounter of a vaccinated person with an infectious person, taking into account that vaccine protection is less than 100%. X-axes are days. Blue labels show the day when case numbers fall below 100’000. Black labels show the day death numbers fall below 1000.
A “one dose fits all” vaccination strategy starting with the elderly allows an initially unchecked propagation of the virus in younger population segments with high “risk contact” numbers, as shown in figure 2, panel A; a large number of infections in the young inevitably spreads to some degree to the elderly (who are not 100% protected by the vaccine), with case numbers above 100’000 per day up to day 53, 199’000 cumulative deaths over 100 days and death rates of >1000 deaths per day until day 80.
In contrast, a strategy initially vaccinating the young only, at full vaccine dose, shown in panel D, stops the pandemic earlier with case numbers falling below 100’000 on day 36, but lacking protection for the vulnerable leads to 226’000 deaths, with death rates falling below 1000 on day 84.
Remarkably, an adaptive strategy using half the available vaccine stock for vaccinating the elderly at full vaccine dose and using the other half at a reduced dose (figure 2, panel B) to immunize a much larger number of younger people, even at the price of a somewhat reduced vaccine efficacy per individual person, is much more effective in reducing case numbers and deaths in each age group. Using a quarter dose for the young (25µg), assuming 86·4% protection, allows shortening the time to <100’000 cases to 24 days and reducing deaths to 165’000 at 100 days. This scenario also reaches the milestone of <1000 deaths per day significantly faster, in 61 days.
Distributing a quarter dose (25µg) only to the young (i.e., not vaccinating the elderly; figure 2, panel C), also assuming 86·4% protection, reduced deaths to 148’000, protecting the elderly indirectly by shortening the pandemic, with< 100’000 cases per day reached on day 18 and <1000 deaths per day reached on day 52.
Results proved to be robust against varying input parameters, in particular when varying the transmission blocking efficacy of a vaccine: The adaptive strategy combining quarter dose vaccination to the young and full dosing in the old remained preferable to the “one dose fits all” approach starting with the old, down to a transmission blocking vaccine efficacy of 30% (Figure 3).

Sensitivity of choice of strategy to different efficacies for transmission blocking or vaccine- and infection-mediated immunity. Transmission blocking efficacy for vaccine and infection-mediated immunity is varied between 30 and 90% for the young. For the old, a transmission blocking efficacy is kept at 86.4%, potentially biasing the results in favor of the “one dose fits all” strategy starting with the old. Nevertheless, the adaptive strategy, reaching large numbers of young persons early, is more effective in reducing the Covid-19 case load at all transmission blocking efficacies tested, down to 30%.
Discussion
Combining demographic and recent epidemiologic data from Europe with published immunity responses of vaccinated persons from different age groups, we find that vaccination strategies tailored to the characteristics of the existing vaccines have a large potential for saving more lives and shortening the duration of the pandemic, compared to the current “one dose fits all” approach and the current strategy of prioritizing the elderly.
The different pattern of social contacts in the young21, the strong immunogenicity of the Moderna vaccine in the young and its excellent protective effect at full dose in the elderly inspire an adaptive strategy that uses the established dose in the elderly, but in parallel, applies a reduced vaccine dose to a much larger number of younger people, exploiting its extremely good efficacy in this population segment. In this model, this approach allows an acceleration of the vaccination campaigns, resulting in fewer deaths and shorter duration of the pandemic emergency.
The significant effectiveness of the Moderna vaccine already at moderate immune response level, evident by its effectiveness in preventing disease already at 10 days after vaccination with a single standard dose in the pivotal trial, before the full immune response is reached, supports biological benefit already before reaching full titers. Emerging data confirm a protective effect of mRNA Covid-19 vaccines for blocking transmission22; as this effect is manifest in elderly patients already after a single dose, we infer that those patients have not yet reached full immunity titers but are already protected, supporting our line of thought. Likewise, 83% protection against reinfection is documented after natural infection23, where average immune titers are lower than after vaccination. Experiences with “fractional” dose vaccination in other viral diseases24,25 further lend credibility to the results.
Notably, “protecting the vulnerable” is achieved best, when not only the vulnerable, but all population segments are immunized, in particular those that contribute more to drive the pandemic than the elderly26,27,28. A large number of infected young people combined with the imperfect protection achievable by vaccination in the elderly still represents a relevant threat to the vulnerable, rendering the strategy focusing on the elderly-first inferior to stopping the pandemic through a comprehensive approach.
More effective vaccination strategies may also have profound repercussions on preserving functionality of healthcare systems and on economies. Hopefully, they will also accelerate access to vaccination in poorer countries in a time when nations risk to quarrel over this precious resource, although Covid-19 can only be overcome by global collaboration.
The benefit of a reduced-dose approach results from a non-linear dose-efficacy relationship of a given vaccine, where the fractional loss of protection for the individual person is less than the gain in additional vaccine doses. We note that antibody responses and T-cell responses observed29 in the Pfizer Tozinameran (BNT162b2) vaccine show a similar nonlinear dose-response relationship, in that at most a marginal reduction in immune titers is observed when dose is reduced from 30 to 10ug (with an antibody and T-cell response even observable at 1ug). These findings suggest that also for the Pfizer vaccine used in the young, a dose reduction of at least 3-fold, and thus an increase in early vaccinations of 3-fold, could be considered for implementing a similar strategy as quantitatively analyzed here for the Moderna vaccine.
While the Moderna vaccine appears to retain full activity for the mutant of concern B.1.1.7 that currently spreads rapidly30, thereby rendering the proposed strategy rational also with this new threat, other coronavirus mutations that might evade the immune response imparted by prior infection or by the current vaccines are feared to arise soon31 and may require additional shots with modified vaccines, and thereby will put further strain on production lines, adding considerable urgency to optimizing vaccine strategies now. The risk of mutants developing after reduced dose vaccination does not appear high32 because virus infection after coronavirus vaccination typically induces a strong immunity boost33.
The study is limited because it is based on reinterpretation and extrapolation of existing data and includes the assumption of a degree of clinical efficacy of transmission blocking of a reduced vaccine dose based on laboratory surrogate parameters, while safety has already been documented for these doses. Protection from transmission has been shown for the Astra Zeneca vaccine but detailed data are not yet available for the vaccines used here. The proof of benefit of such an approach for society is amenable to straight-forward study designs that are immediately implementable: Allocate entire cities or countries to this approach, and count the cases, death rates and outbreak duration. The approach described here focuses on high-efficacy mRNA vaccines; generalizations to other vaccines will require examining specific dose-response relationships per vaccine.
As this approach is an “off-label” use of a registered drug, applying it in patients will require specific permits from relevant ethics committees and regulatory bodies.
Conclusion
Adaptive vaccination strategies, namely fully dosing a vaccine in the elderly, vulnerable, and concomitantly applying a highly effective mRNA vaccine at a reduced dose in the remainder of the population, or even a reduced dose strategy focused on the young only, will multiply the number of persons receiving the vaccine early, may contribute to stopping the pandemic faster and have the potential to save many lives, as predicted by this model parameterized for European demographics, Covid-19 transmission patterns and vaccine characteristics.
Evidently, the vulnerable are best protected by protecting society as a whole.
Data Availability
A spreadsheet with daily data will be available, starting with publication in a scientific journal, for 6 months, by email request from the author, for non-commercial, scientific purposes by academic institutions and government agencies, with mandatory source attribution when used. For use of the statistical model and for other uses, contact the author directly.
Data sharing statement
A spreadsheet with daily data will be available, starting with publication, for 6 months, by email request from the author, for non-commercial, scientific purposes by academic institutions and government agencies, with mandatory source attribution when used. For use of the statistical model and for other uses, contact the author directly.
Research in Context
Evidence before this study
As source of demographics of Europe, we used the official EU Eurostat repository. For epidemiology of the Covid-19 pandemic, the Johns Hopkins University CSSE dataset and the European Center for Disease Prevention and Control situation dashboard were used. For immunogenicity of the Moderna vaccine, PubMed was used to identify the published data related to “mRNA-1273”; a Bing search retrieved an additional presentation slide set from Moderna about its testing pipeline. Vaccine supply limitations are amply referred to in official statements published by the media outlets. Efficacy for the Moderna vaccine at regular dose is 95·6% (95% CI, 90·6-97·9) for those up to 64 years and 86·4% (95% CI, 61·4-95·2%) for those above, as reported in the pivotal phase 3 publication. Immunogenicity data are given in the table.
Added value of this study
Using an epidemic model initialized with EU-wide population, Covid-19 case and death data from mid-January 2021, alternative, up to now unexplored vaccination strategies were defined and compared to the currently preferred approach that consists of initially focusing vaccination on the elderly because vaccine supplies are insufficient for a broader initial use. The study addressed several alternative vaccination strategy scenarios, in particular the use of a reduced vaccine dose in the group that showed the strongest immune response to vaccination, namely those < 65 years.
Implications of all the available evidence
Vaccination, combined with societal measures up to lock down, will be the mainstay of mastering the SARS-CoV2 pandemic. The available evidence, including the findings reported here, imply that tailored vaccination schemes adapted to the specific characteristics of the vaccine, the demographics and the immune response of population subgroups have a large potential for reducing case numbers and deaths in Europe.
Supplementary material
Model construction
The model is inspired by the SEIR approach but is performed in discrete-time steps and uses difference equations instead of continuous time and differential equations. This approach allows parameterizing the model in a straightforward way by daily statistical data available from the various data sources. The model has discrete structure with a time step of ône for 100 consecutive days.
Two age strata are modeled, allowing to use age-group adapted immunity, fatality, and social interaction propensity. The model is initialized with the population size of the European Union split in two age segments, ≤ 64 years (“young”) and 64 years(“old”), using the daily infection rate and the cumulative number of cases documented in mid-January 2021.
In each age stratum, a infection-naïve, a vaccinated and a postinfective group is modeled, with transitions between groups upon infection or vaccination. Susceptibility to transition to “infection” is 1.0 for the naïve group and parameterizable for the other groups to allow for modeling of various vaccine efficacies.
Contact modelling between persons assumes that a “young” person has 80% of its social encounters with the “young” and 20% with the “old”, while “old” persons have 50% of its social encounters with the “old”. “Risk contacts” are defined as the proportion of encounters (relative to day 1) of noninfected persons with persons newly infected within the past 7 days, and “Semi-Risk contacts” are defined as the proportion of encounters of immune (natural or post vaccination) persons with newly infected persons, using separate computation for each age group. Daily contact frequency is conservatively chosen as equal in both groups. Selecting larger contact numbers in the young would further underline the key findings of the study.
During December 2020/January 2021, number of cases, deaths and tests in stagnated at a high level in Europe, allowing to estimate an approximate case fatality rate, and initialize an initial contact propensity by multiplying the number of infectious persons with susceptible persons (weighted for the degree of immunity). We couple the pandemic modeling to the documented (though imprecise) case count rather than on “infection” count because testing rates are currently high and true infection rates (including asymptomatic individuals) across Europe are currently at best very coarse estimates. In reality, asymptomatic infections will also make persons transition from “naïve” to “post-infection”, a cause of bias that is minor early in a pandemic but becomes more important when large proportions of a population have been infected.
The number of new cases for is computed as proportional to the risk contacts, plus the semi-risk contacts scaled by the degree of immunity (i.e., effectivity of the vaccination for this group, or natural immunity). The infectious window is on day 1 to 7 after infection.
The number of deaths was modeled as proportional to the number of new cases, with a time lag of 14 days.
1 million vaccine full vaccine sets (2*100 µg) per day are used. In the different scenarios, they are either applied as 1 million full vaccinations of the >64 year old person per day in the standard vaccination strategy until day 65% of the elderly population is vaccinated, followed by 1 million full vaccinations per day in the young. In the other scenarios, daily 500’000 vaccinations are performed in the elderly and 2 million vaccinations at quarter dose in the young in the adaptive scheme, or 4 million vaccinations at quarter dose limited to the young, or 1 million vaccinations at full dose limited to the young, respectively. Vaccinated persons became protected against infection on day 10, to a degree corresponding to the level of immunity conferred by the given vaccine dose and age group as described in the methods paragraph.
Counts of population, newly infected, infectious, immune, susceptible, vaccinated persons and deaths were updated daily.
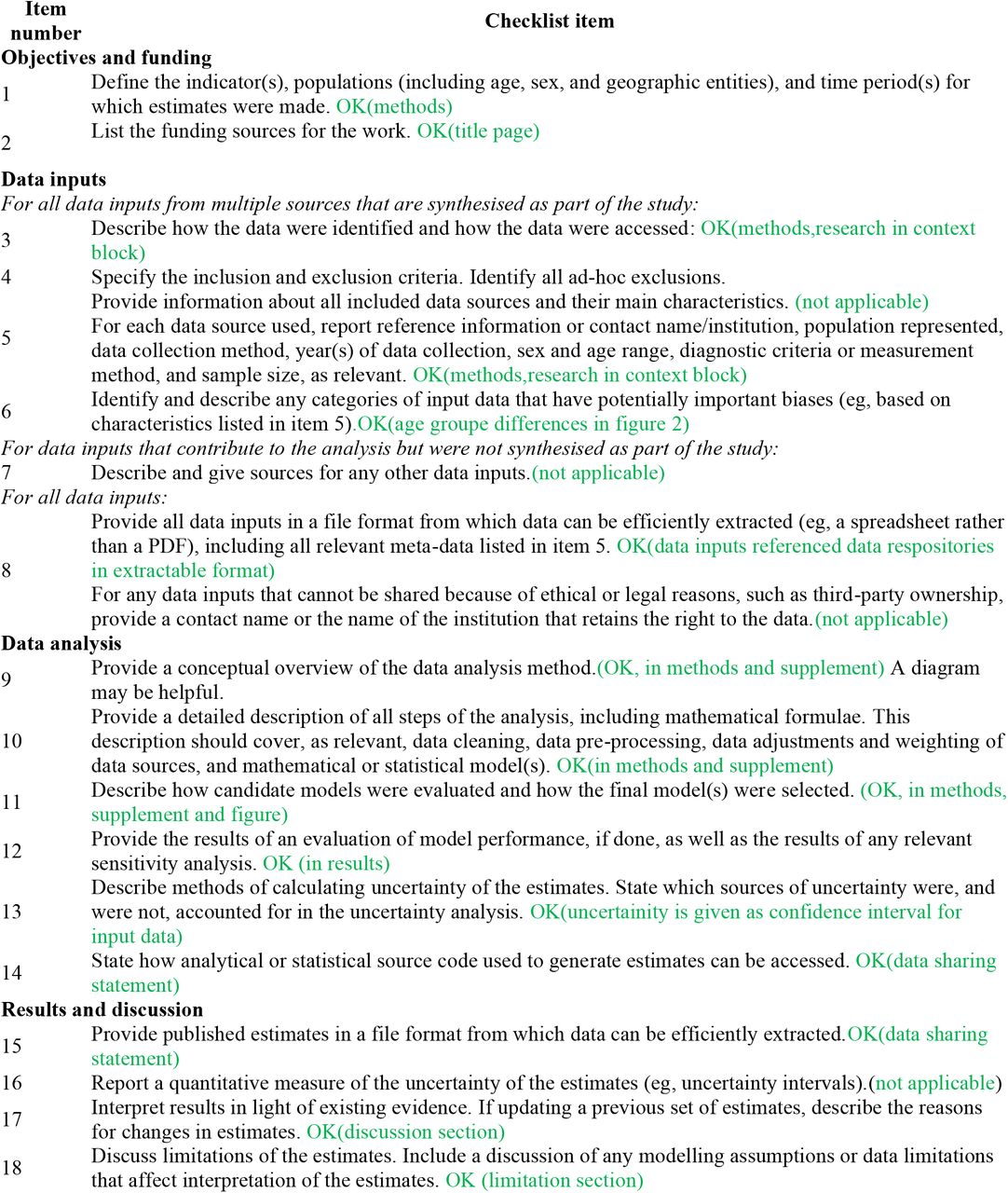
GATHER checklist of information that should be included in reports of global health estimates
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Footnotes
Funding: Self-funded
Conflicts of interest: None
Ethics committee approval: Not subject to ethical committee requirements
sharpened conclusion and abstract
References



