
Abstract
SARS-CoV-2, the virus responsible for the COVID-19 pandemic, is perceived to be primarily transmitted via person-to-person contact, through droplets produced while talking, coughing, and sneezing. Transmission may also occur through other routes, including contaminated surfaces; nevertheless, the role that surfaces have on the spread of the disease remains contested. Here we use the Quantitative Microbial Risk Assessment framework to examine the risks of community transmission of SARS-CoV-2 through contaminated surfaces and to evaluate the effectiveness of hand and surface disinfection as potential interventions. The risks posed by contacting surfaces in communities are low (average of the median risks 1.6×10−4 - 5.6×10−9) for community infection prevalence rates ranging from 0.2-5%. Hand disinfection substantially reduces relative risks of transmission independently of the disease’s prevalence and the frequency of contact, even with low (25% of people) or moderate (50% of people) compliance. In contrast, the effectiveness of surface disinfection is highly dependent on the prevalence and the frequency of contacts. The work supports the current perception that contaminated surfaces are not a primary mode of transmission of SARS-CoV-2 and affirms the benefits of making hand disinfectants widely available.
Introduction
SARS-CoV-2, the virus responsible for the COVID-19 pandemic, is transmitted primarily via person-to-person pathways such as prolonged exposures to respiratory droplets produced while talking, coughing, and sneezing 1,2. Based on the assumption of respiratory-droplet transmission, infection control recommendations include maintaining social/physical distances, wearing masks, case isolation, contact tracing, and quarantine 3. Due to the possibility of transmission through other routes, including airborne and surface-mediated transmission, the WHO recommends taking airborne precautions for particular settings where aerosols are generated and emphasizes the importance of hand hygiene2. Nevertheless, the role that airborne and surface-mediated transmission have on the spread of the disease remains contested 1,2,4–7.
Indirect transmission via fomites (contaminated surfaces) contributes to the spread of common respiratory pathogens 8–10 and evidence-to-date suggests fomite transmission is possible for SARS-CoV-2. People infected with SARS-CoV-2 shed the virus into the environment, as evidenced by extensive SARS-CoV-2 RNA detected on surfaces in cruise ships, hospitals, and public spaces in urban areas such as bus stations and public squares 11–15. Infective coronavirus persists in the environment, with experimental evidence of persistence on surfaces ranging from 3 hours to 28 days, depending on environmental factors such as surface material and temperature 16–18. Viruses readily transfer from contaminated surfaces to the hand upon contact 19–21 and from hands to the mucous membranes on the face 21–23. People touch their faces frequently, with studies reporting average hand-to-face contacts ranging from 16 to 37 times an hour 24–26. Taken together, this suggests surface contamination could pose a risk for indirect SARS-CoV-2 transmission, similar to other respiratory viruses8.
Despite the potential importance of indirect transmission, it is difficult to estimate its role relative to direct transmission. Quantitative Microbial Risk Analysis (QMRA) provides a framework for understanding health risks from indirect transmission and provides insights into potential impacts of infection control recommendations. Mechanistic models of transmission events within the context of QMRA frameworks have been used to identify risks for a number of scenarios including children playing with fomites 27, sanitation workers collecting and processing urine for nutrient recovery 28, and people sharing a houseboat.29 Within the context of the current COVID-19 pandemic, QMRA has been adapted to evaluate and compare transmission risks for MERS-CoV and SARS-CoV-2 through droplets, aerosolized particles, and doffing personal protective equipment in hospitals 30–32 and to evaluate the effectiveness masks at reducing the risk of SARS-CoV-2 infection 33.
In this study, two mechanistic models of indirect transmission within the QMRA framework are used to estimate the risk of infection for SARS-CoV-2 in community settings and inform guidance on potential intervention strategies. Specifically, a model is developed to estimate the risk of infection for single contacts with contaminated surfaces, with the concentrations of SARS-CoV-2 RNA on the surfaces informed by literature investigating surface contamination in public spaces (bus stations, gas stations, stores, playgrounds). A second model is used to estimate risks from surface-mediated community transmission as a function of the prevalence of COVID-19 cases in the community and to test the efficacy of feasible intervention strategies of hand disinfection and surface disinfection.
Methods
Model 1. Risks from contaminated surfaces
A stochastic-mechanistic model was developed to estimate the infection risk for a single hand-to-surface followed by hand-to-face contact (Figure S1). The concentration of SARS-CoV-2 RNA on public surfaces [gene copy number (gc) cm-2] was obtained from literature13,15. Conversion of SARS-CoV-2 RNA to infective virus was assumed to follow a uniform distribution with range 100 and 1000 (gc per infective virus, with infective virus measured using Plaque Forming Units (PFU)). The gc:PFU ratio is based on the sparsely available information of SARS-CoV-2 found in literature 18,34,35, data from enveloped respiratory RNA viruses36 (seasonal influenza A(H1N1), A(H3N2), and influenza B have mean ratios of 708, 547, and 185 gene copies per TCID50 respectively), and a ratio of 0.7 to convert TCID50 to PFU37. The transfer of virus from surface-to-hand and from hand-to-mucous membranes was assumed to be proportional to the concentration of virus on the surface and the transfer efficiency of virus at both interfaces38. An exponential dose-response model39 was used to estimate the probability of infection for a given dose. This model is based on the pooled data of studies of SARS-CoV40 and Murine hepatitis virus (MHV-1)41 infection in mice. The upper bounds of the dose-response curve are consistent with the infectivity of two different variants of SARS-CoV-2 in mice, hamsters, and ferrets42. Monte Carlo simulations were used to incorporate the uncertainty and variability of the input parameters. The model was simulated 50,000 times. Results are presented as the median risk values with 5th and 95th percentiles. The equations used, the probability distributions for the input parameters, and a diagram of the model can be found in the Supporting Information (Figure S1-S3, Table S1).
Model 2. Risks from surface-mediated community transmission
Contamination of SARS-CoV-2 on surfaces in public spaces (e.g., traffic light buttons, train buttons) was modeled as a function of disease prevalence in the community and frequency of contact with the surface. Estimates obtained in the model describe the probability of infection for people contacting the surface across a period of seven days. In the model, surface inoculation happens when infected individuals use their hand to cover their mouth while coughing and subsequently touching a surface. Viral loads [gc mL-1] in the saliva or sputum of symptomatic COVID-19 patients within the first 14 days of symptom onset were used as input to the model35,43–45. The concentrations of SARS-CoV-2 in saliva and sputum samples measured in genome copies35,43–45, align with concentrations of samples measured in TCID50 34 once they are adjusted by the previously mentioned genome copies to infectivity ratio.
The frequency of surface contamination was determined by the prevalence of the disease in the population46–50. A cough was assumed to spread particles conically51. Therefore, virus inoculation on hands was modeled as a function of the concentration of virus in the saliva, the volume of saliva expelled per cough, the distance between the mouth and the hand, and the right circular cone angle of the ejected particles, a (Figure S2, Table S1). Transfer from surface-to-hand and from hand-to-mucous membranes was assumed proportional to the concentration of virus on the surface and the transfer efficiency of virus at both interfaces38 (Figure S1). The concentration of virus in the contaminated surface was assumed to decay exponentially 52. Decay rate was obtained from research on SARS-CoV-2 survival on various surfaces 18. An exponential dose-response model39 was used to estimate the probability of infection for a given dose. The concentration on the contaminated surface and on the hand was reduced according to the log10 reduction values for the scenarios of surface and hand disinfection. Alcohol-based hand sanitizer was selected as hand disinfection strategy due to the widespread availability and portability of hand-sanitizers. Although hand-washing was not considered, based on the log reductions of enveloped viruses achieved by handwashing53, we assume effectiveness of handwashing is similar to hand sanitizer for the reduction of SARS-CoV-2 on hands.
Monte Carlo simulations were used to incorporate uncertainty and variability of the input parameters in the risk characterization. Convergence was tested for the baseline scenario by running five times 5 000, 10 000, 20 000, 50 000, and 100 000 simulations. There was minimal variation after 50 000 simulations (Supplementary Figure 2). Based on the results, all the models were simulated 50,000 times. For each of the 50,000 simulations, the risks were calculated across time, for a period of seven days. Therefore, each simulation has a time profile of contaminations and risks. The median, 25th and 75th quartiles of the seven day simulations were recorded for each of the 50,000 simulations and the average values of the median, 25th and 75th quartiles are reported (Figure 2). A sensitivity analysis was performed to investigate how the variability and uncertainty of the parameters in the model influenced the estimated risks. The sensitivity was estimated using the Spearman’s correlation coefficients between the inputs and outputs of the model. A detailed description of the model and model parameters are found in the Supporting Information (Figure S1, Table S1).
Results and discussion
Risks from contaminated surfaces
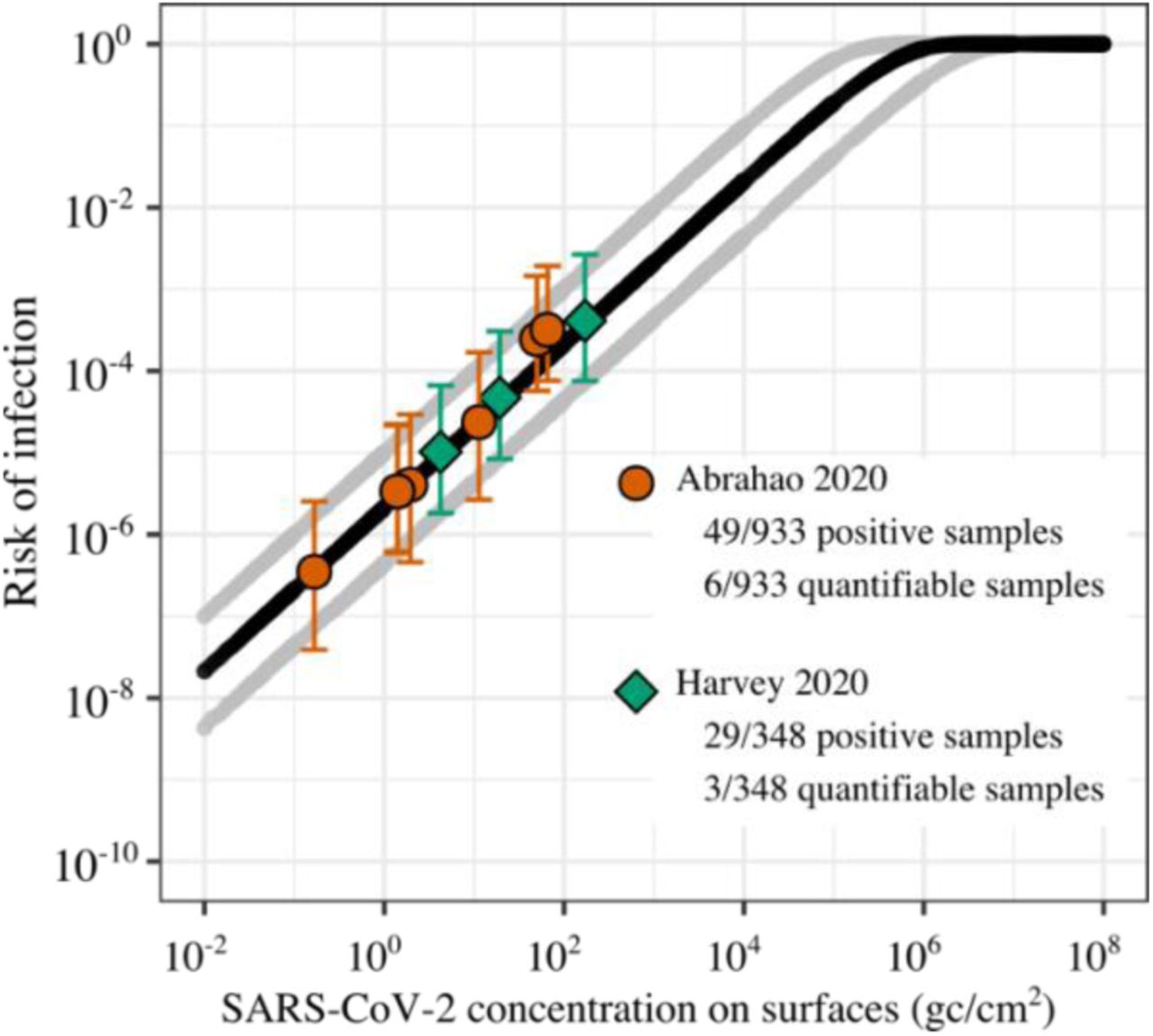
Risks of SARS-CoV-2 infection from contact with a fomite in community settings are estimated to be low (Figure 1) and influenced by both infection prevalence rate in the community and the frequency with which the fomite is contacted (Figure 2). Median risk of infection from interaction with a contaminated fomite is linearly related to surface contamination, ranging from 2×10−8 for a surface with 0.01 RNA genome copies (gc) cm-2 to approximately 1 for a surface with ≥106 RNA gc cm-2 (Figure 1). Previous studies of surface contamination on public spaces have detected 0.1 to 102 SARS-CoV-2 gc cm-2 13,15. In the two studies only 3 of 1281 (0.2%) surfaces sampled were associated with risks of infection greater than 1 in 10,000. The average risk of infection for the sampled surfaces was of 8.5×10−7, assuming negligible risks for samples with SARS-CoV-2 RNA below the LOD (1203 out of 1281 surfaces).

Median risk of infection is shown in a continuous black line; Gray lines display the 5th and 95th percentiles. Orange circles13 and green diamonds15 represent the median risk estimates for point values of surface contamination in public spaces with whiskers from the 5th to the 95th percentiles. Data from Abrahao et al., orange circles, shows the risk for the 6 quantifiable samples out of the 49 RNA positive samples. Data from Harvey et al., green diamonds, shows the risk of 3 quantifiable samples out of the 29 RNA positive samples.
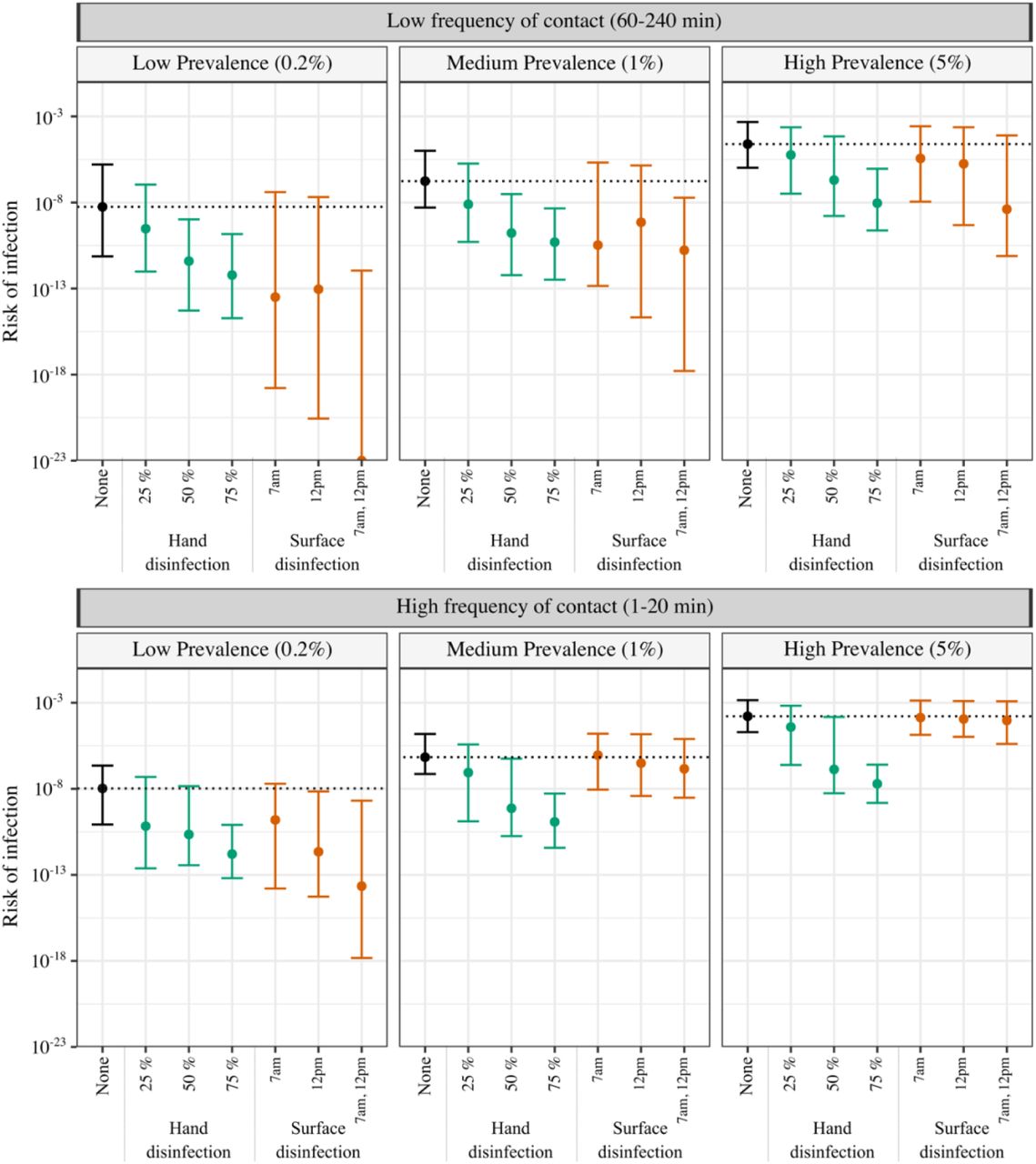
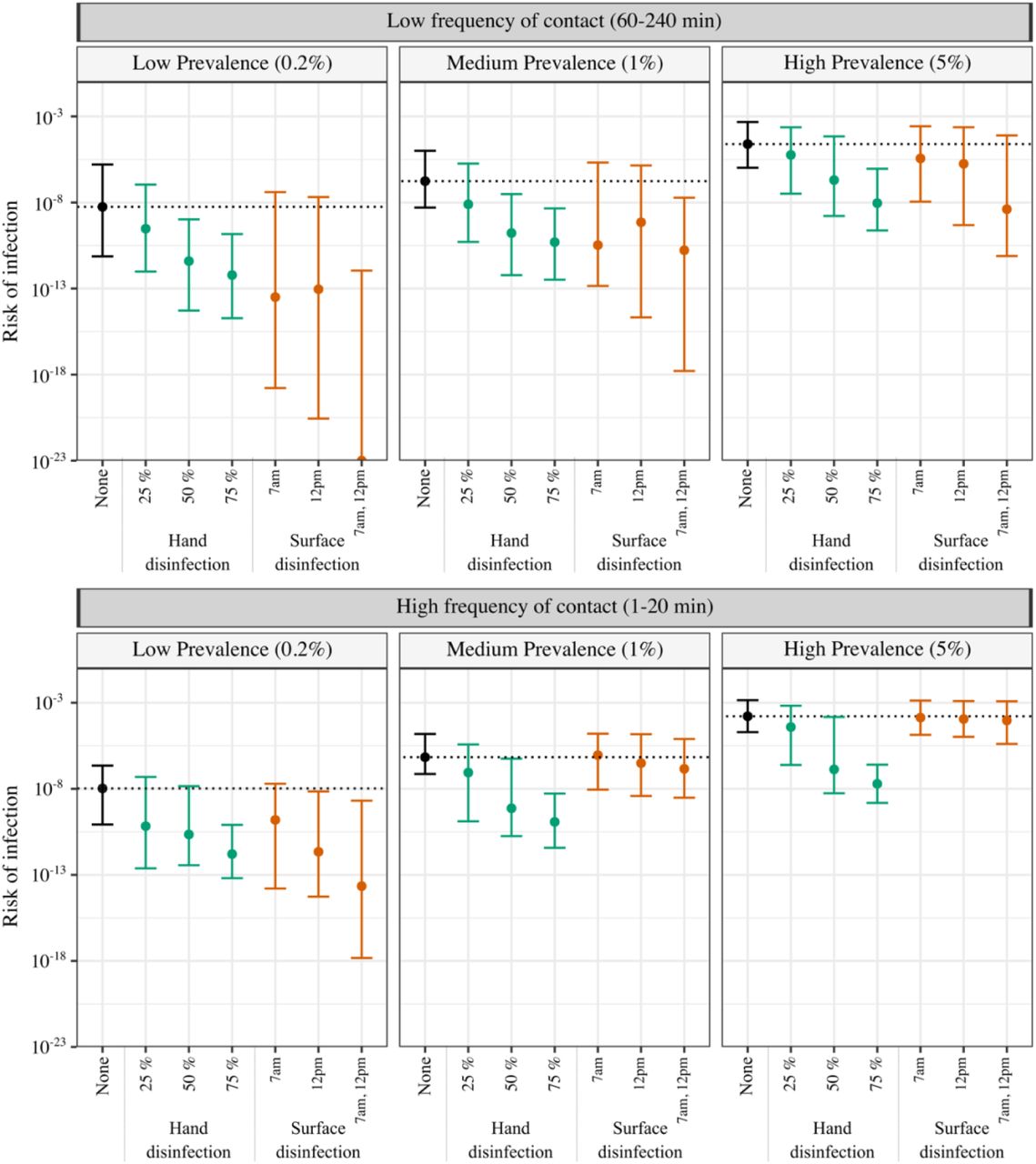
The plot shows the average median risk of infection, with whiskers from the 25th to the 75th percentiles. Two interventions were tested (hand disinfection [green] and surface disinfection [orange]) in parallel to no intervention control [black]. Compliance for hand disinfection was set to 25, 50, and 75% of the population. Surface disinfection regimes were: every day at 7am, 12pm, or 7am and 12pm. The horizontal black dotted line illustrates the median risk of infection without intervention. Two contact frequencies and three prevalence levels (percentage of the population sick at any given time) were modeled: high contact frequency [1-20 min] and low contact frequency [60-240 min] and low [0.2%], medium [1%], and high [5%] prevalence. The risk of infection of 10−6 is equivalent to one person sick as a result of hand-to-mouth contact every million people touching the surface.
Risks from surface-mediated community transmission
When modeling risks of surface contamination within communities, average median value [IQR] risks range from approximately 1.6×10−4 [2.0×10−5, 1.4×10−3] for the highest risk scenario (5% infection prevalence rate, object contacted once every 1-20 minutes) to 5.6×10−9 [7.4×10−12, 1.6×10−6] in the lowest risk scenario (0.2% prevalence rate, object contacted once every 1-4 hours) (Figure 2). The overwhelming majority of interactions with fomites modeled were associated with risks < 10−4 (Table S2). The low risks of community transmission of SARS-CoV-2 via fomites is in accordance with previous studies and opinions of fomite-mediated transmission in hospitals4–7.
According to the sensitivity analysis, the model parameters most influencing estimated infection risks within a community are transfer efficiency between the surface and the hand, TEsh, and concentration of SARS-CoV-2 in sputum or saliva, Csp (Table S1, Figure S4). TEsh was inversely correlated with risk (Spearman’s rank correlation, ρ = −0.58) and Csp was directly correlated (ρ = 0.29). Correlation was low with all other modeled parameters (ρ < 0.05).
Effectiveness of hand and surface disinfection
Hand hygiene was consistently the most effective intervention. Alcohol-based hand disinfectants are portable, widely available, and effective at inactivating coronavirus 54,55. Even with low compliance, representative of only 1 in 4 people disinfecting hands after surface contact, median infection risks from fomite contact were reduced by 0.6-2.2 log10. Under high compliance, representing 3 of every 4 people disinfecting, median risks decreased by 3.8-4.3 log10. Importantly, the impact of hand hygiene also appears to be independent of surface contact frequency and prevalence rates, suggesting a strategy of hand disinfection promotion in community settings is universally applicable. Our findings re-affirm the existing strategies of promoting hand hygiene and making hand disinfect products widely available in shared community settings56.
Although the risks of SARS-CoV-2 transmission via fomites are estimated to be low, they are possible and may contribute a small number of new cases during outbreaks. For both surfaces with quantified contamination and modeled surfaces within a community, infection risk estimates are very low when people interact with a single fomite. However, a person’s infection risk increases when accounting for the hundreds of objects contacted every hour, and the thousands of frequently contacted objects (crosswalk buttons, public transportation buttons, ATMs, and railings) within a city. Each interaction provides an opportunity for SARS-CoV-2 transmission. Risk of infection from multiple contacts with fomites – as compared to a single contact with a fomite – is substantially higher. Nevertheless, in our models the risk of infection from a fomite is orders of magnitude lower than the prevalence rates, suggesting the relative contribution of fomite-mediated transmission might be small compared to other transmission routes.
The data used to quantify risks from measured concentrations of SARS-CoV-2 RNA on surfaces in public spaces were obtained from two locations: Somerville, Massachusetts, USA15, and Belo Horizonte, Minas Gerais State, Brazil13. The sampling collection for both studies occurred throughout a COVID-19 outbreak from March-June 2020. Both places had control measures when the collection took place, including mandatory use of masks in public spaces. The mask use requirement may have influenced surface contamination, with the measured SARS-CoV-2 RNA concentrations lower than what could be observed without a mask requirement. Our modeled interventions included hand disinfection and surface disinfection, but given the widespread use of masks within a community, masks may also help to curb fomite-mediated transmission. Masks are repeatedly shown to be effective at reducing transmission of SARS-CoV-257 through the proposed mechanism of limiting both production of and exposure to aerosolized droplets. Masks may also influence fomite-mediated transmission by reducing hand or surface contamination from droplets and/or reducing hand-to-mouth contact frequency. As there is currently insufficient data on the effectiveness of masks against droplet production and on the frequency of hand-to-mouth contacts, mask use could not be considered as an intervention here.
The model findings are influenced by the model implementation and assumptions, and changes in assumptions may shift some of our conclusions. First, absolute infection risks from QMRA may be unreliable due to the uncertainty and/or variability in the estimates of the parameters58. The exponential dose-response model in particular suffers from a number of limitations: the model is based on data of SARS-CoV and Murine hepatitis virus (MHV-1) infection in mice by intranasal administration40,41. Extrapolating the model from mice to people and from MHV-1 and SARS-CoV to SARS-CoV-2, introduces uncertainty in infection risk estimates, but – in accordance with current best practice 59 – we did not consider this here. Nevertheless, dose-response relationships derived from animal studies tend to be more conservative60. An additional limitation is that the dose-response relationship was determined using virus as measured in units of Plaque Forming Units (PFU) and therefore a ratio of genome copies to PFU is needed. The assumed range of ratios of 1:100 to 1:1000 for genome copies to viable virus is based on Influenza, along with the sparse data currently available for SARS-CoV-2. Data quantifying viable virus on fomites in communities would be the “gold standard”, but detection of viable virus is unlikely given previously observed concentrations of SARS-CoV-2 RNA align with estimates of viable virus of <1 / 100 cm2. Because of the uncertainties in parameter estimates, QMRA estimates of relative risk reduction from interventions are viewed as more reliable because potential biases in data are incorporated into both the intervention and control risk estimates58.
Additional model characteristics likely influence risk estimates. Model parameters used for virus transfer and decay rates are determined experimentally in laboratory conditions and could be different in environmental conditions. Also, prevalence rates modeled here are assumed to correspond directly with the percent of people who are infected and contact the surface with a hand contaminated by coughing. In reality, an unknown fraction of infected people would likely either: 1) stay at home (i.e., quarantine and/or isolation), or 2) not cough directly on their hand. In this regard, the modeled infection risks are likely higher (more conservative) than would be expected at the stated community infection prevalence rates.
Despite the limitations of the underlying model, Quantitative Microbial Risk Assessment remains a valuable tool to understand and characterize risks of surface-mediated transmission of SARS-CoV-2 within communities and test the effectiveness of different interventions. Epidemiological investigations and/or structured experimental designs (i.e., randomized controlled trials) are infeasible given that fomite-mediated transmission is likely a rare event and is difficult to decouple from other – more likely – transmission routes. The results presented here add to the evidence supporting the relatively low contribution of fomites in the transmission of SARS-CoV-215, and can inform guidance on potential intervention strategies.
Author contributions
T.R.J. and A.K.P designed the study. A.K.P. performed the modeling. T.R.J. and A.K.P wrote the manuscript.
Competing interests
We have no competing interests to declare.

{kind=link}
{kind=link}
{kind=link}
Acknowledgements
We thank Danilo Cuccato, Emmanuel Froustey for their inputs on the model, and Diego Marcos, Sunil K. Dogga, Gabriele Micali, Esther Greenwood, Sital Uprety and Elyse Stachler for reviewing the manuscript. A.K.P. was supported by Swiss National Science Foundation – SNSF.
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
1
Blogs/Media
Author Videos