
Abstract
To broadly explore the extent that COVID-19 has initially impacted medical learners around the world and examine global trends and patterns across geographic regions and levels of training, a cross-sectional survey of medical learners was conducted between March 25-June 14th, 2020, shortly after the World Health Organization declared concurrent COVID-19 a pandemic. 6492 medical learners completed the survey from 140 countries, Students were concerned about the quality of their learning, training progression, and milestone fulfillment. Most trainees felt under-utilized and wanted to be engaged clinically in meaningful ways; however, some trainees felt that contributing to healthcare during a pandemic was beyond the scope of a medical learner. Statistically significant differences were detected between levels of training and geographic regions for satisfaction with organizational responses, the impact of COVID-19 on wellness, and state-trait anxiety. Overall, the initial disruption to medical training has been perceived by learners across all levels and geographic regions to have negatively affected their training and well-being, particularly amongst postgraduate trainees. These results provide initial insights into the areas that warrant future research as well as consideration for current and future policy planning, such as the policies for clinical utilization of medical learners during public health emergencies.
Introduction
The coronavirus pandemic (COVID-19) represents the first global interruption to medical education since World War II. This public health emergency has required undergraduate and postgraduate medical training programs around the world to rapidly respond, including re-deploying learners to other clinical spaces or removing them entirely, and moving education online to promote physical distancing (Association of American Medical Colleges 2020; Harvey 2020; Rose 2020). The current COVID-19 pandemic has changed the status quo of medical training as we know it – whether for better or for worse remains unclear and may have profound implications.
Prior localized disruptions to medical training have negatively affected trainees, such as pandemics and climate emergencies. The severe acute respiratory syndrome (SARS) pandemic in 2003 revealed the tension between embracing learning opportunities that a public health emergency offers and protecting the needs and well-being of learners (Rieder et al. 2004; Sherbino & Atzema 2004; Rambaldini et al. 2005). The SARS pandemic adversely affected the mental health of learners and healthcare professionals, and heightened anxiety amongst learners was associated with a perceived negative educational experience (Maunder et al. 2003; Bai et al. 2004; Landis & Bradley 2005; Rambaldini et al. 2005). In 2005, the rapid restructuring of the medical school curriculum in response to Hurricane Katrina resulted in a decline in academic performance (Crawford et al. 2008). Lessons from both SARS and Hurricane Katrina highlighted the importance of support networks and attention to learner wellness, recognizing the additional stressors that these disruptions can place on medical trainees (Landis & Bradley 2005; Rambaldini et al. 2005; DiCarlo et al. 2007; Crawford et al. 2008). These emergencies led to significant and rapid innovation in curriculum structure and content (DiCarlo et al. 2007). While disruptions to medical education can provide an impetus to reconsider ethical and practical implications of training during emergencies, training models may remain stagnant (Landis & Bradley 2005; DiCarlo et al. 2007). Despite a heightened awareness fifteen years ago of the potential implications of interruptions to medical education, many organizations and systems entered the current pandemic relatively unprepared.
Medical education’s understanding of the impact of global emergencies and disruptions to medical training remains limited to SARS and localized emergencies, yet the current pandemic remains the single most substantial disruption to contemporary medical training with global impact. The extent to which COVID-19 has impacted medical training remains speculative and anecdotal, and the consequences and implications may be profound. The research question for this exploratory study was: How have medical learners been impacted by the COVID-19 pandemic around the world?
Methods
Data Collection
We administered a cross-sectional survey between March 25 and June 14, 2020, shortly after the World Health Organization declared COVID-19 a pandemic. Criterion and snowball sampling techniques were used to collect data from undergraduate (e.g., medical students) and postgraduate (e.g., interns, house staff, resident physicians) medical learners at any medical school around the world. This study explicitly focused on medical learners given that they provide a significant proportion of patient care yet are still considered learners.
Our decision to use a survey was based on the ability of this method to efficiently collect empirical data from a large population (Kelley et al. 2003) The survey instrument was designed to include both quantitative and qualitative questions in order to later compare variables across groups, allow participants to provide insight into how they have been impacted using their own words, and use the qualitative data to potentially expand upon the results of the quantitative data (Appendix A). All participants completed demographic questions followed by questions specific to their level of training. Next, shared questions explored the effect of the pandemic on learner wellbeing and their communications with others. Open-ended questions collected qualitative data surrounding the impacts of the pandemic on training, utilization of residents, and strategies used in response to the pandemic. All questions were developed de novo, except the 6-item State-Trait Anxiety Inventory (STAI-6) (Marteau & Bekker 1992). One question exploring the impact of the pandemic on five domains of wellness was informed by a holistic framework for learner wellness (Kassam & Ellaway 2020).
An initial survey underwent pilot testing to refine comprehension and functionality. The final survey was translated to 19 additional languages to increase the inclusion of learners from around the world. The survey was administered online using Qualtrics software by distributing an anonymous, re-usable link over social media and through snowball sampling.
Data Analysis
Quantitative data were imported into SPSS Version 26 (IBM Corp., New York) for analysis. Countries were coded to the geographic regions defined by the World Bank to explore geographic differences (World Bank) Descriptive statistics were calculated for each item. Total scores were computed for scaled questions, with positively worded items reverse coded in the calculation. Independent t-tests were used to compare total scores between medical students and residents, and an Analysis of Variance test was used to compare data across geographic regions using a post-hoc correction to account for multiple comparisons. To examine the psychometric properties of the survey, Cronbach’s alpha was computed for scaled items to assess reliability evidence and an exploratory factor analysis was used to examine construct validity.
Qualitative data were back translated to English and analyzed in NVivo Version 12 (QSR International, Melbourne). Three investigators read through the data to identify emerging themes, which were then organized into a coding framework for deductive thematic and content analysis to similarly examine trends between levels and across geographic regions (Miles et al. 2014). Two investigators (KB, MM) independently coded 100 responses to refine the initial coding framework and assess inter-rater agreement. After an additional 400 responses were analyzed and the Kappa statistic continued to suggest acceptable inter-rater agreement, and a decision was made to divide to improve efficiency given the volume of data. Upon completion of the coding for all responses, themes in the coding framework were divided amongst the research team. Each member analyzed the data coded to their assigned themes and summarized the trends and patterns in the data. Theme summaries were compiled for interpretation by the study team, who then compared and contrasted the results of the qualitative data with the quantitative data to examine how these findings converge or diverge from, and ultimately expand upon, the quantitative results.
The University of Calgary Conjoint Health Research Ethics Board reviewed and approved this study (File #20-0484). Participation in this study was voluntary. Implied consent was obtained from all participants. Participants had the option to either skip individual questions or select “prefer not to answer.”
Results
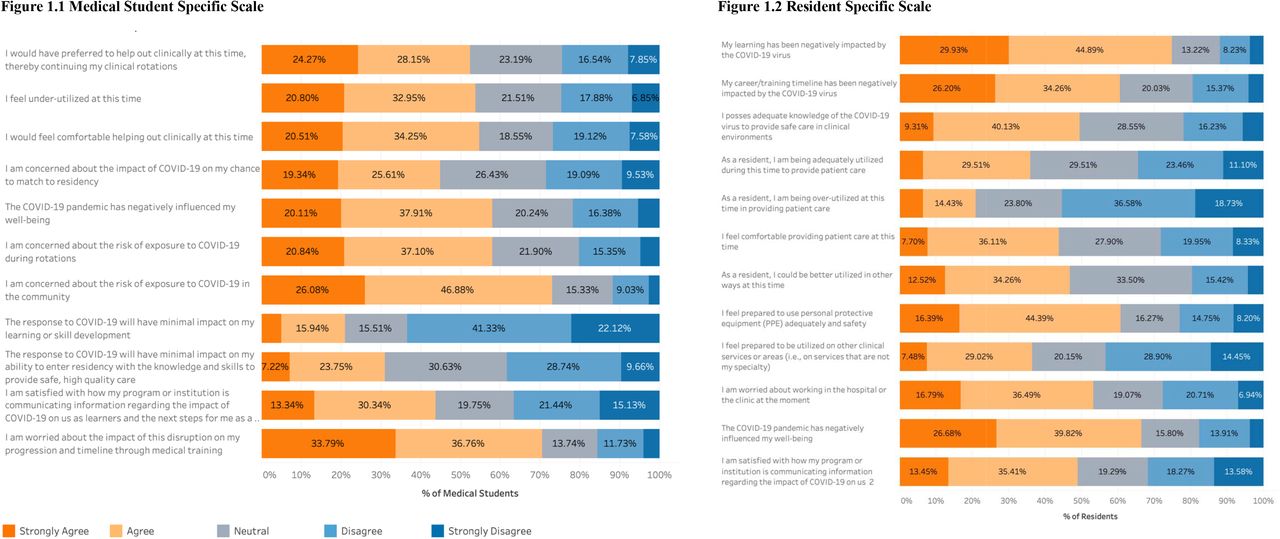
A total of 6492 learners from 140 countries completed the survey. The majority of participants were medical students (81.0%) and from Europe and Central Asia (43.4%) (Table 1). The results for both medical student-specific and resident-specific questions are summarized in Table 2. Figure 1 visualizes the responses to the scaled questions for both levels (see Appendix B for additional visualizations of the data by level of training and geographic region).
Demographic Characteristics of Participants
Medical Student and Resident Specific Questions

Scaled Questions Exploring the Impact of COVID on Learners
Undergraduate Medical Learners
The majority (84.3%) of clinical-level medical students were excused from clinical duties; however, some worked clinically in some capacity (9.0%). Most spent their time in online learning coordinated by their medical school (68.2%), pursuing self-directed learning (44.1%), resting (36.4%), and engaging in more wellness activities than normal (31.4%). Most (80.9%) had online learning coordinated by their school but 66.5% felt their education would be of lower quality as a result. Some had difficulties learning from home (21.0%) and accessing the internet (11.0%).
Students reported that their core electives (23.5%) and visiting electives (19.5%) were cancelled or postponed. The qualitative data highlighted how reduced clinical exposure limited opportunities to explore specialties, decreased career interests, and created anxiety about implications for future milestones (e.g., examinations, residency match). While the majority of medical students did not report the pandemic influenced their career interests, 11.4% of medical students reported increased interests in both Public Health and Infectious Disease as a result of the pandemic, as well as other clinical specialties (e.g., Emergency Medicine, Critical Care, Internal Medicine) and new interests in incorporating epidemiology into their future careers. Decreased interest in clinical careers and concerns about the impact of the pandemic on job prospects in their country were noted qualitatively.
Over half of medical students reported feeling under-utilized (53.8%); 52.4% wanted to assist clinically (52.4%) and felt comfortable doing so (54.8%). While 57.9% worried about the risk of exposure to the virus during rotations, 73.0% worried about the risk of exposure in the community. Over two thirds (70.6%) reported feeling worried about the disruption to their progression through medical training, with 45.0% worrying about their chances to match to residency. Only 21.0% thought the pandemic would have a minimal impact on their learning or skill development, and only 31.0% felt that it would have a minimal impact on their ability to enter residency with sufficient knowledge and skill to provide safe, high-quality care. The majority of students (58.0%) felt that the pandemic negatively affected their wellbeing.
Postgraduate Resident Learners
Residents were from a variety of specialties, mostly in urban settings. Three-quarters of residents agreed their learning was negatively impacted by COVID-19 and 60% felt it disrupted their career progression and timeline. Only 16% reported working more than normal during the pandemic and 36.7% working less than normal. Some residents felt adequately utilized (35.9%) or over-utilized (20.9%); however, 46.8% reported they could be better utilized. Over one-third felt comfortable providing patient care at this time, and 60.8% felt prepared to use personal protective equipment (PPE). Half of residents reported adequate knowledge of COVID-19 to provide care, 36.5% were prepared to be redeployed to other clinical services, and only 53% were worried about working in the hospital. 66.5% agreed that COVID-19 had negatively impacted their wellbeing. The qualitative data provided further evidence that residents felt under-utilized - but highlighted how they saw their re-deployment in a clinical setting as being in conflict with their educational goals.
Shared Questions
All scaled items had acceptable internal consistency (α>.7) and factor loadings, suggesting reliability and validity evidence. Statistically significant differences were detected between levels of training (p<.05) and geographic regions (p<.007) for the items examining satisfaction with organizational responses [t=7.517, p<.000; [F(6,5258) = 73.85, p<.007]], the impact of COVID-19 on wellness [t =-7.774, p<.000 [F(6,5165)= 11.81, p<.007]], and state-trait anxiety [t=-4.710, p<.000;[F(6, 5131)=10.48, p<.007]] (Appendix C). In general, residents reported lower satisfaction with organizational responses (x=15.67, 95% CI = 15.36-159.98) as well as a greater negative impact on their wellbeing (x=18.52, 95% CI 18.24-18.80,) and anxiety (x=15.13, 95% CI 14.83-15.42). Learners from the East Asia and Pacific region were most satisfied with organizational responses, whereas learners from Sub-Saharan Africa and Latin America and Caribbean were least satisfied (Figure 2.1). Medical students from the Latin America and Caribbean region as well as residents from North America reported the largest negative impact of COVID-19 on their wellness (Figure 2.2). Residents from South Asia, Latin America and Caribbean reported the highest state-trait anxiety (Figure 2.3).

{kind=link}
{kind=link}
Comparison of Shared Scaled Items Between Levels and Geographic Regions
Seventy-four percent of residents and 57% of medical students reported being more anxious than usual (Table 3; Figure B.4). Common concerns were the health and wellbeing of family members, the impact of the pandemic on their learning, the health of the public, their personal health, the financial situation of others, and their personal financial situation (Figure B.3). One-quarter of participants identifying as Asian reported an increase in racist comments or behaviors in the clinical setting during COVID-19. Over half (54.7%) of learners living with a disability felt their school’s response to the pandemic would further disadvantage them due to their disability.
Shared Questions
Some learners reported having to be in quarantine or isolation at the time of the survey. Nearly all learners were practicing physical and social distancing.
The qualitative data highlighted how normal education and training processes were severely disrupted by the pandemic (Appendix D). Learners identified a need for institutions to adapt and innovate in order to mitigate these impacts and continue education. Learners also desired to have input into their institutions’ pandemic response. Strategies such as town halls, surveys, and learner representation on decision-making committees helped ensure their circumstances were accurately understood and enabled them to raise concerns overlooked by decision-makers.
Clear and effective communication during the pandemic was essential for learners, while poor or absent communication left learners uncertain of what was happening and contributed to their anxiety. Effective communication provided clarity and reassurance about the pandemic’s impacts and the institutional response. Learners wished to be informed about impacts on their programs, details of the pandemic response, their role (including how to help), and resources they could access. Effective communications about these topics were clear, specific, decisive, concise, and reassuring. Irregular (sporadic) communication created an “information vacuum” that was filled by speculation, rumors, and misinformation. Overly frequent communication was overwhelming and led students to ignore institutional communications.
Numerous interventions were implemented in response to COVID-19, including virtual teaching strategies (e.g., Zoom, Microsoft Teams), office hours and town halls, and clinical strategies (e.g., patient handover via teleconference, alternating call schedules to minimize exposure). When done effectively, online learning maintained educational momentum and provided learners with motivation, a routine, and a sense of purpose. Self-directed learning was frequently used to augment online learning, and when provided with support and guidance, this motivated learners and provided them with a sense of progress. Programs with too much content overwhelmed them, whereas programs that provided minimal guidance left learners feeling aimless. Some participants stated that their program or school had done nothing in response to the pandemic, and that either their education had continued as usual or, in some instances, students were told to stay at home and self-direct their learning without any guidance from their program.
Discussion
This study provides empirical data about the impact of COVID-19 on medical education around the world, notably the effects on learning and wellbeing. Taken together, our findings highlight how learners have been impacted regardless of their program’s response to the pandemic and whether or not they were removed from the clinical environment. However, the extent that COVID-19 has impacted learners differs significantly between levels of training and geographic regions.
COVID-19 has disrupted the traditional format and process of medical training for the vast majority of medical students and residents around the world. The rapid adoption of online learning by most schools may raise concerns about the quality of education (Mian & Khan 2020). Despite these concerns, equivalent educational outcomes between online and offline methods have been reported in the literature.(Pei & Wu 2019) The removal of learners from the clinical setting may diminish training (particularly for residents in time-based models of training), influencing clinical competence acquisition and career-decision making – all of which may affect patient care and health system outcomes (Goldhamer et al. 2020). While COVID-19 has required programs to adapt their curricula, this may be an opportunity to reconceptualize, innovate, and improve the current models of medical training, and ultimately catalyze broader educational transformation (Goldhamer et al. 2020; Sklar 2020).
Consistent with early reports, medical students feel under-utilized and have a strong desire to help out clinically during times of need (Lauren et al.; Herman et al. 2007; Gallagher & Schleyer 2020; Kalet et al. 2020; Li & Bailey 2020). However, not all learners may share these views. In addition to concerns about physical safety, some participants in our study believed the role of trainees is to be educated and that any deviation from that role is inappropriate. Others felt personally invested in contributing to care and viewed it as their personal calling and professional obligation. The optimal role of trainees during pandemics is complicated given their dual role as learners and healthcare providers – the extent to which each role is prioritized during emergencies remains debated. On one hand, it has been argued that medical students specifically, as an unpaid workforce, are not essential workers, and may increase disease transmission and waste scarce supplies of PPE (Menon et al. 2020). In contrast, it can also be argued that medical students are a semi-skilled workforce that can alleviate the burden on residents and staff, and should gain experience in preparation for future pandemics when they will no longer be trainees. In one study, hospital leaders viewed medical students who graduated early to help during COVID-19 as “game changers” (Flotte et al. 2020). It has also been argued that medical education is equally important to patient care during a pandemic (Klasen et al. 2020). This may be a unique opportunity to cultivate leadership skills if learners are well-supported (Brand 2020). For learners in the clinical environment, supervision, feedback, and evaluation as well as access to adequate wellness supports remain crucial (Brand 2020; Klasen et al. 2020). The ethical and practical considerations of utilizing medical learners during a pandemic remains an ongoing point of discussion and needs to be weighed against potential benefits of learning and implications to patient care (Simonds & Sokol 2008; Bauchner & Sharfstein 2020).
COVID-19 is expected to affect the mental health of the public(Venkatesh & Edirappuli 2020) as well as that of healthcare professionals (Lai et al. 2020). Previous health emergencies and disruptions to training, such as SARS and Hurricane Katrina, have been shown to diminish the mental health of trainees and healthcare professionals (Kisely et al. 2020). Our study provides similar evidence but from a global perspective that the wellbeing of medical learners has been negatively impacted by COVID-19 across all levels of training and geographic regions. This is concerning given the existing evidence on the alarming prevalence of burnout and psychiatric morbidities in learners, as COVID-19 may amplify these pre-existing issues (Puthran et al. 2016; Frajerman et al. 2019; Quek et al. 2019; Hartzband & Groopman 2020). Pandemic responses have superimposed new stressors while exacerbating existing stressors for learners. The “anticipatory loss” associated with the disruption of traditional processes and milestones (e.g., electives, residency match, licensing exams) appears associated with anxiety, and front-line learners (e.g., residents) may be particularly prone to wellness stressors (Gallagher & Schleyer 2020; Li & Bailey 2020). Suggestions for mitigating the psychological consequences of COVID-19 on front-line care providers include clear communication, education, and psychological support, among others (Kisely et al. 2020).
This pandemic remains an ongoing challenge for medical education. While the uncertainty of COVID-19 required organizations to adopt a “worst-case scenario” approach, medical schools not only continue to react to the needs of the health system, but proactively plan for the future. While some participants in this study applauded their program’s response, it is important to learn from this experience and improve planning and policies for current and future emergencies that may disrupt medical education (O’Byrne 2020). Recommendations are increasingly being discussed in the literature (The Coalition for Physician’s Accountability Work Group on Medical Students in the Class of 2021; Kachra & Brown 2020; Klasen et al. 2020; O’Byrne 2020; The Association of Faculties of Medicine of Canada 2020). Considerations for medical educators synthesized from our results and existing recommendations are summarized in Table 4. We must continue to share innovations and key lessons amongst the global medical education community. Future research is warranted to understand the long-term impact and potential consequences of the COVID-19 on education, patient care, and health system outcomes.
Considerations for Medical Education During COVID-19
Limitations
We acknowledge that this study has several limitations, including the response and selection bias. The response rates from residents are low, potentially because they continued working clinically and the disruptions to their training were less extreme than for medical students who were completely removed from their training environments. Further, this study excluded participants who did not speak any of the 20 languages of the survey and there may be inconsistencies across the survey translations despite our best attempts to ensure questions and constructs translated accurately. Due to the public circulation of the survey, participants could not be validated as medical learners. A small fraction (3.5%) of participants did not specify their level of training and were excluded from the comparisons across levels of training. The geographic comparisons remain limited, as other classification systems (e.g., the World Health Organization regions) may have generated different results and there may be more pronounced differences between countries within similar regions (e.g., the United States vs. Canada). Finally, the variable responses to COVID-19 across countries and time is worth noting. Numerous qualitative comments highlighted how national responses informed the responses of professional organizations and training programs. Future research could examine potential associations between temporality and the political and health system responses to examine how these factors may extend to influence medical learners (Pablos-Méndez et al. 2020).
Conclusions
This global study provides empirical data surrounding the profound impact that COVID-19 has had on medical learners, which can inform responses to the current pandemic, future disruptions to training, and future research. The results highlight the differences and similarities between levels of training and geographic regions. Despite the global shift toward online education, all education may not be created or perceived equally, as the results of this study suggest medical students fear their education will be of lower quality at this time. Both medical students and residents report their under-utilization, yet the role of the medical learner during a pandemic remains controversial. A delicate balance remains between medical training and the acute needs of the health system to ensure that both education and patient care remain safe. Finally, this study highlights how the COVID-19 pandemic has negatively impacted the wellbeing of medical learners globally, particularly those at the postgraduate level of training, which may be associated with their anxiety relating to the anticipatory losses of their educational experience. While the goal of this study was to broadly examine the impacts of COVID-19 on medical education, it highlights several areas for further exploration. Future research is warranted to better understand the implications of COVID-19 on learner outcomes and to generate evidence-based strategies surrounding how best to teach, engage, and support medical learners during similar events.
Practice Points
The rapid reorganization of medical training in response to COVID-19 has been substantial across all levels of training and geographic regions
Medical learners are concerned that the disruption will negatively influence their learning, training trajectory, and career outcomes.
The majority of medical learners feel under-utilized and are motivated to help out during times of need
The mental health and wellbeing of learners may be further diminished at this time
Medical schools should ideally learn from this experience and improve planning and policies for current and future disruptions or emergencies
Data Availability
Data referred to in the manuscript is not publicly available at this time.
Acknowledgments and Declaration of Interest
Notes on Contributors:
Allison Brown, PhD is an Assistant Professor in the Department of Medicine and Department of Community Health Sciences at the University of Calgary Cumming School of Medicine.
Aliya Kassam, PhD is an Assistant Professor in the Office of Postgraduate Medical Education and the Department of Community Health Sciences at the University of Calgary Cumming School of Medicine.
Mike Paget, BFA is a Manager of Academic Technologies in Undergraduate Medical Education at the University of Calgary Cumming School of Medicine.
Kenneth Blades, MA is a research analyst at the University of Calgary Cumming School of Medicine. Megan Mercia is a baccalaureate student in the Faculty of Science at the University of Calgary.
Rahim Kachra, MD EdM is an Associate Clinical Professor in the Department of Medicine and the Director of Teaching Innovations in Undergraduate Medical Education at the University of Calgary Cumming School of Medicine.
Declaration of Interest
This study was funded by the O’Brien Institute for Public Health through a Catalyst Grant to support the timely back-translation and analysis of the qualitative data. O’Brien Institute for Public Health did not influence the design, conduct, collection, analysis, or interpretation of data, or the writing of the manuscript for publication. The authors have no conflicts of interest to declare for this research.
Ethical Approval
This study was reviewed and approved by the University of Calgary Conjoint Research Ethics Board (File 20-0484) and follows the ethical conduct of the Tri-Council Policy Statement required by the Government of Canada and complies with the World Medical Association’s Declaration of Helsinki on Ethical Principles for Medical Research Involving Human Subjects. Participation in this study was voluntary and implied consent was obtained from all participants. Participants had the option to not answer any question or select “I prefer not to answer” if they wished to skip a question.
Acknowledgements
The authors wish to acknowledge the O’Brien Institute for Public Health for funding this research, members of the University of Calgary medical education community for their support in conducting this study, as well as the Conjoint Health Research Ethics Board (Ashley Krecsy) for reviewing this study in a timely manner. Thanks to Kayla Atchison, Kyle Lafreniere, Suhair Bandeali, Krista Reich, Matthew Mancusco, Tefani Perera, and Nadiya Goswami for pilot testing the initial survey and providing feedback to help improve the survey items and functionality. We also wish to acknowledge Erika Tan and the Immigration Services Centre of Calgary and the assistance of numerous individuals who helped with the translation of the survey into additional languages: Philippe Pepin (French), Yusuf Yilmaz (Turkish), Dinesh Chavda (Hindi), Tayebah Chaudhry (Urdu), Giuliana and Salvatore Guarna (Italian), Michael Ji (Korean), Joska Eelsingh (Dutch), Laura Massignani (Spanish), Shenghao Huang (Chinese), Elzbieta Raniszewska (Polish), Florentino Guerra Filho (Portuguese), Tomoka Tsuhara and Lea Mezger (German), Hengameh Kheirkhah (Farsi), Atipong Pathanasethpong (Thai), Thi Hong An Do (Vietnamese), Vesta Seibel (Ukrainian), Alena Yakimenka (Russian), and Aito Ueno (Japanese). Next, our study team wishes to acknowledge all who amplified this study over social media or other forms of snowball sampling, including the Association for Medical Education in Europe (AMEE), AMOpportunities. Finally, our study team wishes to acknowledge the patient partners who reviewed the results of this research and the draft manuscript.
References



