
Abstract
Background Reports suggest that asymptomatic individuals (those with no symptoms at all throughout the infection) with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are infectious, but the extent of asymptomatic transmission requires further understanding.
Purpose This living review aims to critically appraise available data about secondary attack rates from people with asymptomatic and pre-symptomatic SARS-CoV-2 infection.
Data sources Medline, EMBASE, China Academic Journals full-text database (CNKI), and preprint servers were searched from 30 December 2019 to 3 July 2020 using relevant MESH terms.
Study selection Studies that report on contact tracing of index cases with asymptomatic or pre-symptomatic SARS-CoV-2 infection, in either English or Chinese were included.
Data extraction Two authors independently extracted data and assessed study quality and risk of bias. We calculated the secondary attack rate as the number of contacts with SARS-CoV-2, divided by the number of contacts tested.
Data synthesis Of 928 studies identified, 19 were included. Secondary attack rates from asymptomatic index cases ranged from 0% to 2.8% (9 studies). Pre-symptomatic secondary attack rates ranged from 0.7% to 31.8% (10 studies). The highest secondary attack rates were found in contacts who lived in the same household as the index case. Other activities associated with transmission were group activities such as sharing meals or playing board games with the index case.
Limitations We excluded some studies because the index case or number of contacts were unclear. Owing to the anticipated heterogeneity, we did not produce a summary estimate of the included studies.
Conclusion Asymptomatic patients can transmit SARS-CoV-2 to others, but our findings indicate that such individuals are responsible for fewer secondary infections than people with symptoms in the same studies.
Systematic review registration PROSPERO CRD42020188168
Funding No funding was received
Introduction
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) demonstrates efficient transmission in populations without effective public health interventions; basic reproduction numbers (R0) values range between 2-3 (1). While asymptomatic transmission has been described as the “Achilles’ heel” of control efforts during this pandemic, the extent to which transmission of SARS-CoV-2 by people without symptoms drives this pandemic remains uncertain (2). SARS-CoV-2 infection that is asymptomatic at the time of laboratory testing is widely reported (3); however, studies that follow infected people over time suggest that many infections are not asymptomatic throughout the entire disease course, and a large proportion of these individuals ultimately develop a diverse range of symptoms (4-7). A living systematic review of studies published up to 10 June 2020, estimated that 20% (95% CI 17 to 25%) of people who become infected with SARS-CoV-2 remain asymptomatic throughout infection (7).
One of the barriers to understanding the role of asymptomatic transmission is the lack of consistency in case definitions. While symptom severity exists on a spectrum, individuals infected with SARS-CoV-2 can be miscategorized as asymptomatic, when they are paucisymptomatic. For instance, Gudbjartsson et al. reported that approximately half of the participants in their population screening in Iceland had symptoms despite asking symptomatic patients not to participate (3). Additionally, studies that define symptomatic disease narrowly as fever, cough, or shortness of breath might overestimate the proportion without symptoms (3, 8). It is increasingly clear that some individuals experience more diverse symptoms, including taste and smell disturbance or myalgia, either for the entire course of illness or preceding respiratory symptoms. These symptoms can be so mild and insidious that they do not limit patients’ daily activities (4, 9). The situation is further complicated by subjective patient perception and differences between studies in the elicitation and reporting of symptoms.
There are reports describing asymptomatic individuals with SARS-CoV-2 who are infectious (10) and who have infected one or more contacts (11), but the extent and significance of asymptomatic transmission requires further understanding. The aim of this review is to summarize the available evidence about secondary attack rates (defined as the probability that an infected individual will transmit the disease to a susceptible individual) amongst the contacts of asymptomatic or pre-symptomatic individuals with SARS-CoV-2 to provide information about how contagious they are, and their role in driving the pandemic.
Methods
Systematic review was registered in PROSPERO on 8 June 2020 (CRD42020188168) and will be updated three times a year as a living systematic review (12). The larger review aims to answer transmission dynamics of SARS-CoV-2. The analysis in this report addresses one of the review questions; to identify asymptomatic and pre-symptomatic secondary attack rate.
Definitions
We defined “asymptomatic” as an individual with laboratory-confirmed SARS-CoV-2 infection who does not demonstrate symptoms throughout their entire course of infection, or after 14 days of follow up; “paucisymptomatic” as an individual with laboratory-confirmed SARS-CoV-2 infection with mild symptoms, and “pre-symptomatic” as an individual who reports no symptoms at the time of the initial positive test result, but who goes on to develop recognised COVID-19 symptoms. We used these definitions to categorize the index cases. Secondary attack rate was defined as the number of new SARS-CoV-2 infection cases among susceptible contacts of primary cases divided by the total number of susceptible contacts.
Search Strategy
We retrieved articles about transmission of SARS-CoV-2 infection through systematic searches of eight databases: Medline, EMBASE, Europe PMC, Web of Science, SCOPUS, Chinese database (CNKI), and preprint servers (MedRxiv, BioRxiv) using relevant Medical Subject Headings (MeSH) terms (Supplementary material). The initial search was completed from 30 December 2019 to 21 May 2020, searches were repeated on 8 June 2020 and 3 July 2020, owing to the rapidly increasing numbers of studies.
Study Selection
Studies were eligible if they met the inclusion criteria: (1) report on Coronavirus disease 2019 (COVID-19) or SARS-CoV-2 infection and (2) report an outbreak investigation or contact tracing study. Exclusion criteria were: (1) review articles; (2) observational studies providing only the proportion of individuals infected; (3) studies that do not indicate the number of contacts or secondary infections; and (4) reports in media sources. We also manually screened the references of the included original studies and reviews to identify additional eligible studies.
Data Extraction
Two authors (XQ and AIN) independently reviewed reports by title and abstract for relevance, with at least 20% of all reports being screened in duplicate to ensure consistency. Two authors then independently read the full text report of all studies not excluded by title and abstract, to consider eligibility for inclusion. Any disagreements regarding study inclusion were resolved through discussion with a third author (MC). Data were extracted onto a standardized form. From each study, the following variables were extracted: the name of the first author, year of publication, country, sample size, details of index cases (categorised as asymptomatic, pre-symptomatic and symptomatic); event details such as environment, transmission details; number of contacts, number of secondary cases. If these data were not reported, we contacted authors to request them.
Risk of bias in included studies
Two authors (XQ and AIN) independently assessed completeness of reporting and risks of bias, using an adapted version of the Joanna Briggs Institute Critical Appraisal Checklist for Case Series (Supplementary material). Any disagreements were resolved through discussion with a third author (MC).
Data synthesis and statistical analysis
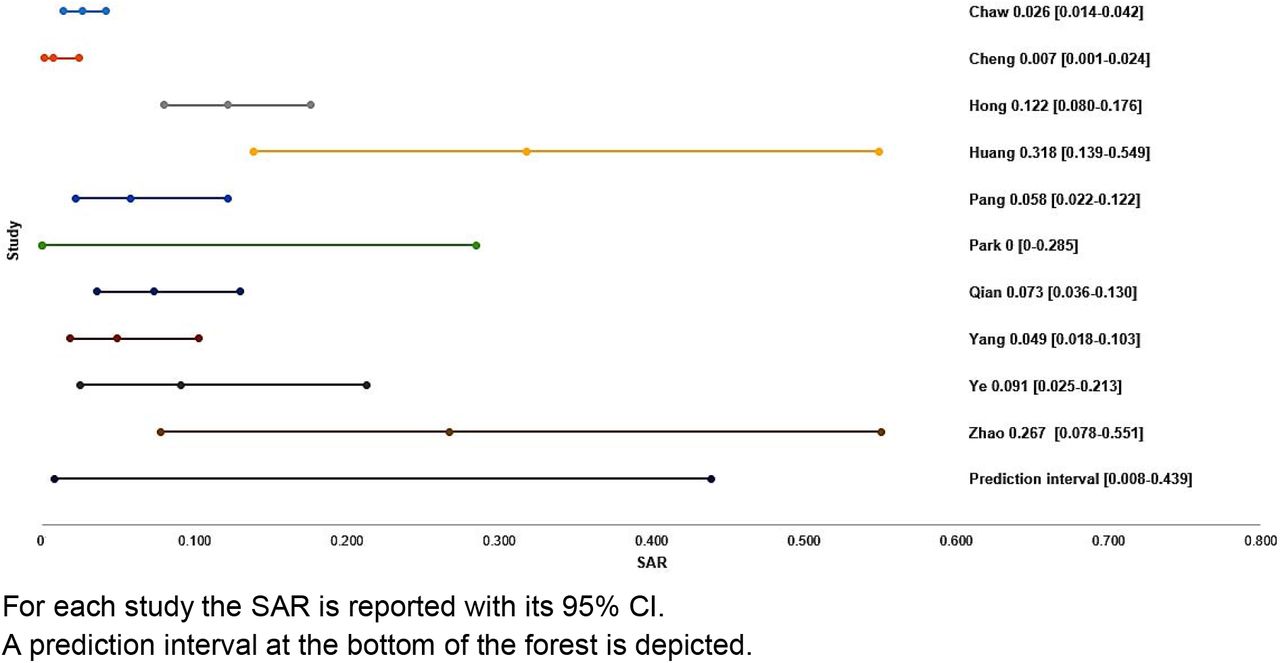
The studies are summarized in text and table form, descriptive statistics were completed for key outcome measures. Secondary attack rates were computed from raw data in each study, dividing the number of infected contacts of primary cases by the total number of susceptible exposed contacts. A 95% confidence interval [CI] was calculated by using the Clopper-Pearson method (13, 14). Secondary attack rates are presented as a proportion along with 95% CIs in forest plots, stratified according to the features of index cases: truly asymptomatic or pre-symptomatic. A 95% prediction interval is shown, but a pooled estimate was suppressed due to the expected high methodological and clinical heterogeneity among the studies. A prediction interval is an index of dispersion, providing information on how widely the true effect size varies. It is an estimate of the range of values in which a future observation will fall (15). Analyses were carried out through the Comprehensive Meta-analysis (CMA) software program (Version 3, Biostat, Englewood, NJ, USA) and forest plots were created by means of Excel from Office 2019 (Microsoft, Redmond, WA, USA).
Results
The systematic search identified 928 potentially relevant articles and 790 records were screened after removal of duplicates. Of 188 articles retrieved for full-text review and assessed for eligibility, 83 studies were included in the overall systematic review, and among those we identified 19 studies that indicated contact tracing of asymptomatic or pre-symptomatic index cases. The remaining studies are not reported in this systematic review. The number of selected papers at each step of the screening and eligibility are reported in the flow diagram (Figure 1).

Flowchart describing the study design process
Of these 19 studies that indicated contact tracing of asymptomatic or pre-symptomatic index cases, after reviewing the details and contacting the authors, we re-classified three studies from asymptomatic to pre-symptomatic as the index cases developed symptoms later during the disease course (16-18).
Summary of secondary attack rates of asymptomatic index cases
Of the 19 studies included, contact tracing of index patients who were identified as asymptomatic cases, according to our definition, was reported in nine (Table 1, Figure 1) (6, 11, 19-25). All except one tested all close contacts for SARS-CoV-2, regardless of symptoms (23). Cheng et al. only tested symptomatic cases, but they also tested high risk populations regardless of symptoms including the household and hospital contacts (23). Six studies reported on household contacts, two studies included hospital contacts and two studies included non-household close contacts.
Three studies identified no secondary cases after following up 17, 91 and 455 close contacts of asymptomatic index cases (asymptomatic secondary attack rate of 0%) (21-23). Of those, two studies demonstrated higher symptomatic secondary attack rates; Cheng et al. demonstrated that mild cases had a secondary attack rate of 3.8% (95% CI 1.1, 12.8%) and severe cases had 4% (95% CI 1.0, 15.8%) secondary attack rate (23), while Park et al. showing household symptomatic secondary attack rate of 16.2% (95% CI 11.6, 22.0%) (21). In another study, 305 contacts of 8 asymptomatic cases were followed up, identifying one secondary case (secondary attack rate 0.3% (95% CI 0.0, 1.8%) (25). In the same study, mild, moderate and severe attack rates were 3.3%, 5.6% and 6.2%, respectively. Zhang et al. followed up 119 close contacts of 12 asymptomatic index cases and identified one secondary case, an asymptomatic secondary attack rate of 0.8% (95% CI 0.0, 4.6). In the same study, the secondary attack rate was 3.5% (95% CI 1.5-8.0) for those with mild, 5.7% (95% CI 2.5, 12.8%) for those with moderate, and 4.5% (95% CI 0.8, 21.8%) for those with severe symptoms (6). In this study, close contacts that lived with an index case had 12 times the risk of infection as those who did not live with the index case (RR 12.5 - 95% CI 1.6, 100.8) and those who had frequent contact with an index case-patient, and those who had more than 5 contacts had 29 times the risk of infection as those with fewer contacts (RR 29.0 - 95% CI 3.6, 232.3). Two studies indicated an asymptomatic secondary attack rate of 1% and 1.9% (19, 20). Chaw et al. reported asymptomatic and pre-symptomatic contacts together. The authors clarified that 3 asymptomatic index cases and their 106 close contacts were followed up, leading to 3 secondary cases, a secondary attack rate of 2.8% (95% CI 0.06, 8.0%). In this study, the overall secondary attack rate was 10.6% in the household setting, which was higher for symptomatic cases (14.4%, 95% CI 8·8, 19·9%) than that of asymptomatic cases and for non-household contacts 0.7 (95% CI 0.1, 1,3) (11). Zeng et al. conducted the largest contact tracing study, following up 753 close contacts of asymptomatic index cases and identified one secondary case, an asymptomatic secondary attack rate of 0.13% (95% CI 0.0, 0.7%). In the same study, the secondary attack rate for all contacts was 2.0% (95% CI 1.8, 2.3%) for confirmed symptomatic index cases (24).
Summary of pre-symptomatic secondary attack rates
Thirteen papers reported either outbreak investigations or contact tracing studies reporting transmission from an index case during the pre-symptomatic period (11, 16, 18, 23, 26-33) (Table 2). Of those, ten studies followed up 22 to 585 close contacts whose initial exposure occurred before symptom onset of the index case (Figure 3). These studies reported secondary attack rates ranging from 0% to 31.8%. Even in studies that followed up large numbers of people, including community contacts, the majority of secondary cases identified were from the same household or among friend gatherings. In these studies, having meals together, or playing cards with the index case were exposure activities associated with transmission. Hong et al. demonstrated lower secondary attack rates in those wearing masks (8.1% vs. 19.0%; p < 0.001) (27). The remaining three studies exclusively reported family cluster outbreaks (26, 28, 29); these investigations did not test contacts outside the household and it is challenging to truly differentiate transmission during the pre-symptomatic period from symptomatic transmission in the household setting (Supplementary Figure 1).


{kind=link}
{kind=link}
{kind=link}
Quality assessment
All but 3 studies were contact tracing studies. All papers included a clear definition of symptomatic and asymptomatic cases, number of secondary cases and number of contacts. The majority of studies identified index cases with a clear diagnosis, had an acceptable case definition and sufficiently followed up close contacts (for a minimum of 14 days). However, in some studies the definition of close contact and setting of transmission was not provided. In addition, it was unclear in four reports whether all potential close contacts were included, which could result in an underestimation of the secondary attack rate. (Supplementary Table 1)
Discussion
This systematic review provides comprehensive data on secondary attack rates arising from people with asymptomatic and pre-symptomatic SARS-CoV-2 infection. While asymptomatic patients can transmit the virus to others (34), the findings from nine studies in this review found secondary attack rates of zero to 2.8%, compared with secondary attack rates of 0.7% to 16.2% in symptomatic cases in the same studies. These findings suggest that individuals who are asymptomatic throughout the disease course are responsible for fewer secondary infections than symptomatic and pre-symptomatic cases. For contacts whose exposure occurred before symptom onset of the index case, transmission events were associated with living with the index case or group activities such as sharing meals and playing board games.
The findings of our study raise the question about whether the low secondary attack rates from asymptomatic individuals result from low infectiousness or a shorter duration of infectiousness. In another living systematic review, of studies published up to 6 June 2020, we found that cases with asymptomatic infection have a shorter duration of RNA shedding than symptomatic individuals (35). Asymptomatic patients may therefore be contagious but for a shorter duration, limiting the duration they could transmit to their contacts. However, there remain limited data on the shedding of infectious virus in asymptomatic individuals to quantify their transmission potential, which would be needed to inform policy on quarantine duration in the absence of testing. Low likelihood of transmission from asymptomatic index cases combined with high symptomatic secondary attack rates emphasises that, especially in the context of limited resources, approaches should be targeted predominantly on identifying and immediately isolating patients with prodromal or mild symptoms and their contacts, which may avert a significant number of community transmission clusters (36). These findings are in line with previous contact tracing and outbreak investigations suggesting that many SARS-CoV-2-infected people either do not contribute to an onward transmission or have minimal potential to do so (37, 38), and a large number of cases are often caused by a small number of infected patients. Clusters have become a prominent characteristic of SARS-CoV-2 which distinguishes it from seasonal influenza, although a similar pattern was also observed in SARS-CoV and MERS-CoV.
The modelling studies suggest that it isn’t possible to have epidemics of this size without substantial pre-symptomatic transmission. Viral load dynamics of SARS-CoV-2 derived from confirmed cases suggest that peak viral loads are detected at the start of symptom onset up to day 5 of illness, suggesting highest infectiousness potential in just before or within the first few days after symptom onset (35). So far several contact tracing studies emphasize that the highest risk of transmission occurs during the prodromal phase or early in the disease course (39, 40). For instance, in a prospective contact tracing study of 100 confirmed cases of COVID-19 and 2761 close contacts no secondary cases were identified when the exposure occurred more than 5 days after the symptom onset (23). Our findings therefore have important implications from a public health perspective. In settings such as nursing homes, homeless shelters, prisons, cruise ships and meat-packing plants in which many people spend prolong period of time together in the same environment including sleeping, dining and sharing common facilities, and where several outbreaks have been documented, pre-symptomatic transmission may contribute substantially to transmission (38, 41). In these settings, when infection develops, most patients are already inside the facility with high viral loads that increase the risk of onward transmission. This highlights the importance of mitigation measures and surveillance in these settings to identify those patients early in the disease course to prevent onward transmission inside the facility.
This systematic review has several strengths. Firstly, this is a living systematic review examining the transmission of SARS-CoV-2 through contact tracing and outbreak investigation studies. Secondly, we only included studies with clear case definitions, which indicated the number of contacts and secondary cases. The most important study limitation relates to the limitations of the evidence itself. We excluded studies in which the index case was unclear, or the numbers of contacts were not provided. Owing to anticipated heterogeneity, we did not produce a summary estimate of the included studies. The estimates from individual studies are also subject to limitations, such as imprecision resulting from small study size, and sources of bias in the estimation of the true secondary attack rate.
We identified two systematic reviews that investigated asymptomatic transmission, with different research questions and search terms. One review included studies published up to 10 June 2020 and identified five studies that directly compared secondary attack rates between asymptomatic and symptomatic index cases; all were included in our review (7). The summary risk ratios for asymptomatic versus symptomatic (0.35, 95% CI 0.10, 1.27) and pre-symptomatic versus symptomatic (0.63, 95% CI 0.18, 2.26) are consistent with our findings. The second review estimated only household secondary attack rates and included studies published up to 29 July 2020 (42). Of three studies that included asymptomatic index cases, two were included in our review. We excluded one of the studies because the number of contacts of asymptomatic index cases was not specified; we have not yet received details of the study after contacting the authors. Advantages of our review over these two studies are inclusion of studies published in Chinese, search terms that aimed to capture studies specifically estimating secondary attack rates in different settings and clarification about symptomatology of index cases through direct contact with the authors.
Important barriers to more accurate quantification of the contribution of asymptomatic and pre-symptomatic SARS-CoV-2 transmission relate to the different definitions used to estimate the asymptomatic fraction of infections, not taking into account mild or atypical symptoms, or the use of estimates from cross-sectional studies without follow up (43). Therefore, in order to understand the extend of asymptomatic infections and transmission, a clear and comprehensive case definition, which assesses the presence or absence of a defined list of major and minor or atypical symptoms is required in future studies.
In summary, whilst asymptomatic transmission is a major concern for SARS-CoV-2 community spread, secondary attack rates from those who remain asymptomatic throughout their course of infection are low suggesting limited infectiousness. Although it is difficult to estimate the proportion of pre-symptomatic transmission, these patients are likely to be highly infectious around the time of symptom onset and appear to transmit efficiently, especially within households. Those with mild symptoms, who feel otherwise well, still carry large amounts of virus in the upper respiratory tract, which might contribute to easy and rapid spread of SARS-CoV-2 (20). Future clinical studies should incorporate clear definitions and assess a broad range of symptoms associated with COVID-19, should include longitudinal follow up of patients, and calculate secondary attack rates for a wider range of settings and populations.
Conflict of Interest
The authors declare that there is no conflict of interest
Funding
No funding was received
Contribution statement
X Qiu: investigation, data curation, writing – original draft; A Nergiz: investigation, data curation, writing – review and editing; A. E. Maraolo: methodology, formal analysis, writing – original draft; I. Bogoch and N. Low: interpretation, writing – review and editing; M. Cevik: conceptualisation, methodology, investigation, writing – original draft, supervision.
Acknowledgements
We would like to thank the authors of Chau et al. (Dr Tan Le Van), Mandić-Rajčević et al. (Dr Stefan Mandić-Rajčević), Chaw et al. (Dr Liling Chaw) for providing further details about asymptomatic cases in their reports also Prof Stephen Gillespie for his comments on the first draft of this manuscript. We would like to acknowledge Dr. Shuang Jin for searching and downloading Chinese database for this review.
References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
6
Blogs/Media
Author Videos