
Abstract
Background There is scant information regarding risk for COVID-19 among migrants or ethnic minorities in Europe.
Methods Population-based cohort analysis of the cumulative incidence of PCR-confirmed COVID-19 cases until April 25 (2020) among 152018 residents at the city of Alcorcón (Spain) attended at the only public hospital serving this city. Crude incident rates for Spaniards and migrants from different areas of the world were estimated. Age and sex-adjusted relative risks for COVID19 were estimated by negative polynomial regression.
Findings PCR confirmed COVID-19 cumulative incidence was 6·81 cases per 1000 inhabitants among residents of Alcorcón. The crude incidence among migrants (n=20419) was higher than among Spaniards (n=131599): 8·81 and 6·51 and per 1000 inhabitants respectively (p<0·001). By regions of the world, crude cumulative COVID-19 incidences were Asia 2·1, European Union 2·4, Northern Africa 3·6, Russia & East Europe 4·4, Sub-Saharan Africa 11·2, Caribbean 18·3 and Latin-America 20·8 per 1000 inhabitants. By negative polynomial logistic regression, adjusted for age and sex, relative risks (RR) for COVID-19 were not significantly different from Spaniards for individuals from Europe, Asia or Northern Africa. In contrast, there was an increased risk for Sub-Saharan Africa (RR 3·66, 95% confidence interval (CI) 1·42-9·41, p=0·007), Caribbean (RR 6·35, 95% CI 3·83-10·55, p<0·001) and Latin-America (RR 6·92, 95% CI 4·49-10·67, p <0·001).
Interpretation There was a marked increased risk for COVID-19 among migrants from Sub-Saharan Africa, Caribbean and Latin-America residing in Spain. Our data suggest a heretofore unreported increased risk in these populations that may deserve special attention.
Evidence before this study Preliminary reports suggest an increased burden of COVID-19 among migrant or ethnic minorities in Western countries, particularly regarding mortality. Reports have failed to dissociate clinical outcomes from differences in access to medical care or pre-existing medical conditions.
Added value of this study We report a population-based approach estimation of COVID-19 risks for migrants residing in Spain. Our data show a significant increased COVID-19 risk for migrants from Sub-Saharan Africa, and even higher for Caribbean and Latin-America migrants that cannot be attributed to unequal access to medical care.
Implications of all the available evidence Migrants, particularly from some regions of the world deserve a closer attention.
The increased risk may be of relevance for the evolution of the epidemics in Africa, the Caribbean and Latin-America. An underlying potential role of genetic / ethnic background deserves further research
Background
COVID-19 pandemic is imposing a tremendous challenge to the humankind with dramatic direct health consequences and dire secondary economic perspectives 1,2 Most of our information related to COVID-19 epidemiology and clinical evolution relates to the findings from China3. As the epidemic spreads out to different countries, with different social, economic and health systems, as well as different societal and political responses, the spectrum of COVID-19 is acquiring a variety of shapes 4. Nonetheless, little is known regarding potential different effects in people from different countries and diverse ethnic background5–7.
Recent reports have described a disproportionate burden of COVID-19 among migrants as well as ethnical minorities in Western countries 8-10. However, the clinical outcomes (in particular mortality) associated to ethnic minorities are inextricably connected to different socioeconomic backgrounds, pre-existing medical conditions, and unequal access to medical services10,11. Studies in countries with a universal health care coverage may help to attenuate the contribution of unequal access to medical services from other factors associated to differential COVID-19 incidence and clinical outcomes in migrants.
We sought to describe the incidence of COVID-19 among migrants from different areas of the world as compared to Spaniards, both of them living in Alcorcón, a city in the suburbs of Madrid (Spain) with a substantial proportion of foreign residents. The Spanish Health System provides universal free access to medical care for all inhabitants through the Madrid’s Health Service (SERMAS).
Methods
Case-population cohort study conducted at Alcorcón (Madrid), with a total population of about 17000 inhabitants. The population at risk was defined as all adults included in the official municipal live registry of population of the City Council of Alcorcón (last updated March 14, 2020)12 Distribution of the population by nationality and country of origin stratified by age and sex was obtained from this registry.
Case was defined as a patient with a COVID-19 diagnosis at Hospital Universitario Fundación Alcorcón confirmed by Polymerase Chain Reaction (PCR) for SARS-CoV2 for adults residing in Alcorcón. Incident cases of COVID-19 were obtained from the Electronic Patient Record (Selene ©) that is used for all medical and administrative interactions with patients. COVID-19 clinical diagnosis was established by the attending clinicians at the Emergency Room according to European Center for Disease Control and Prevention (ECDCP)-World Health Organization Criteria (WHO) 13.
For molecular diagnosis of SARS-CoV-2 infection, nasopharyngeal swabs, sputum, or bronchopulmonary aspirates were processed by automatized extraction using the MagNaPureLc instrument (Roche Applied Science, Mannheim, Germany) and real time reverse-transcription PCR using the SARS-Cov-2 nucleic acid detection Viasure kit (CerTestBiotec S·L·), following the manufacturer’s instructions. For this rRT-PCR, we used Bio-Rad CFX96™ Real-Time PCR Detection System. We amplified two different viral regions: ORF1ab gene (FAM channel), N gene (ROX channel), and the internal (HEX channel). Cycle threshold values ≤40 were considered positive. Positive and negative controls were included in each run for every assay.
An anonymized set of data was extracted on April 25 from the electronic patient record containing the following parameters: age, sex, nationality, country of birth, city of residence, date of COVID-19 diagnosis (clinical), date and results of SARS-CoV2 PCR, clinical evolution / outcomes (hospital admission, critical care admission, hospital discharge, length of hospital stay, and in-hospital death). For the present study, patients whose residence was outside the city of Alcorcón were excluded. Patients were classified according to their country of origin into one the following groups: a) Spain; b) European Union (including Switzerland and Norway); c). Russia & Eastern Europe; d) Asia, e).
Australia & New Zealand; f) Northern Africa; g) Sub Saharan Africa; h) Latin America (Mexico and continental Latin-American countries); i) Caribbean; j) United States of America & Canada.
Statistics. Results are described as means (± standard deviation), medians (interquartile range) or percentages as appropriate. Quantitative variables were compared by the student’s t test, ANOVA, or U Mann-Whitney ‘s test, as appropriate. Qualitative variables were compared by the Chi2 test or the Fisher’s exact test as appropriate.
Aggregated data by world zone (or country), sex and age group (<30, 30-39, 40-49, 50-59, 60-69, 70-79, 80-89 and >=90) were analyzed. Incidence rates and 95% exact Poisson confidence intervals were calculated by zone. Multivariate negative binomial regression model with robust variance was used to estimate the incidence rate by world zone adjusted for sex and age. These models are appropriate to analyse over-dispersed count data 14 Statistical significance was assumed for p values <0·05. All statistical analyses were conducted with Stata 14 (StataCorp LLC, Texas, USA).
The protocol received the approval of the local Institutional Review Board / CEIm (Medicines Research Ethical Committee).
Results
Alcorcon city registry (last updated on March 14) comprised 152,018 individuals 17 years of age or older. Among them, 20,419 (13·4%) residents had a nationality different from Spain. Their countries of origin (and associated areas of the world) are summarised in Table 1. Different areas of the world were chosen because of geographical, socioeconomic and ethnic background reasons provided there was a minimum of 500 individuals per area. In this regard, Switzerland and Norway were included within the European Union group. Interestingly, the highest proportion of migrants from EU were from Romania (61·4%), followed by Poland (10·1%). Eastern Europe was vastly dominated by Ukraine (90·4%). China was predominant in Asia (60·4%), followed by Pakistan (15·4%). Equatorial Guinea (39,1%) and Nigeria (21·5%) were predominant among sub-Saharan Africa, while Northern Africa was essentially represented by Morocco (96·5%). Major contributors for continental Latin America were Colombia (20·2%), Peru (18·0%), and Venezuela (17·3%). Predominant Caribbean countries were Dominican Republic (71·3%) and Cuba (26·8%). Finally, the regional group ‘others’ (including the USA, Canada, Australia and New Zealand) provided < 200 inhabitants. Given its residual nature, this group was removed for further analysis.
Male sex was more frequent in Spaniards (58·6%) than migrants (52·5%), although the difference did not reach statistical significance (p=0·15). In contrast, Spaniards were substantially older than migrants (median age 73 vs 52 years, p<0·001) (Supplemental Figure 1). Similarly, age distribution pyramids in the reference population were strikingly different for Spaniards and migrants (Supplemental Figure 2).
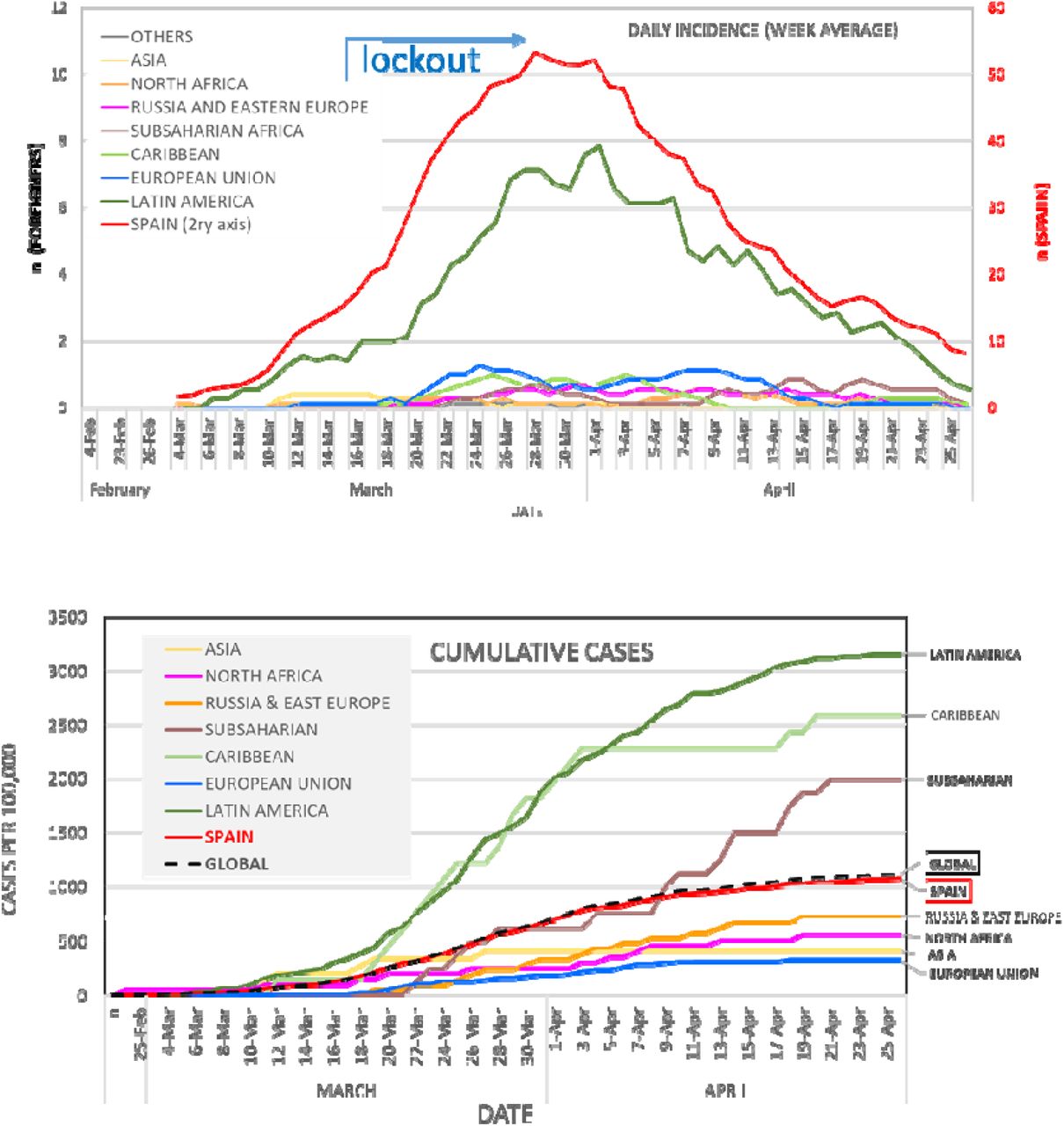
A total of 1691 residents in Alcorcon were diagnosed as having COVID-19 following ECDCP-WHO clinical criteria13 from February 1 until April 25 at our hospital (Figure 1). The number of cases increased steadily until the end of March and declined thereafter (figure 1), roughly 2 weeks after the lockout Decree of the Spanish Government (March 14, 2020)15. In order to avoid potential misdiagnosis, we restricted our analysis to the remaining 1036 cases with a positive CRP for SARS-CoV2 sample (hereafter COVID-A-PCR+ cases). Median age of COVID-A-PCR+ patients was 71 years (IQ range 54-79), and 57·2 % were male. The global accumulated COVID-A-PCR+ incidence was 6·81 per 1000 inhabitants. By origin, the global accumulated COVID-A-PCR+ incidence in Spaniards was 6·50 cases per 1000 inhabitants as compared to 8·82 per 1000 for non-Spaniards (p<0·001; Table 2, Figure 1B). The global cumulative incidence increased dramatically with age for both Spaniards and migrants (Supplemental Figure 3A).
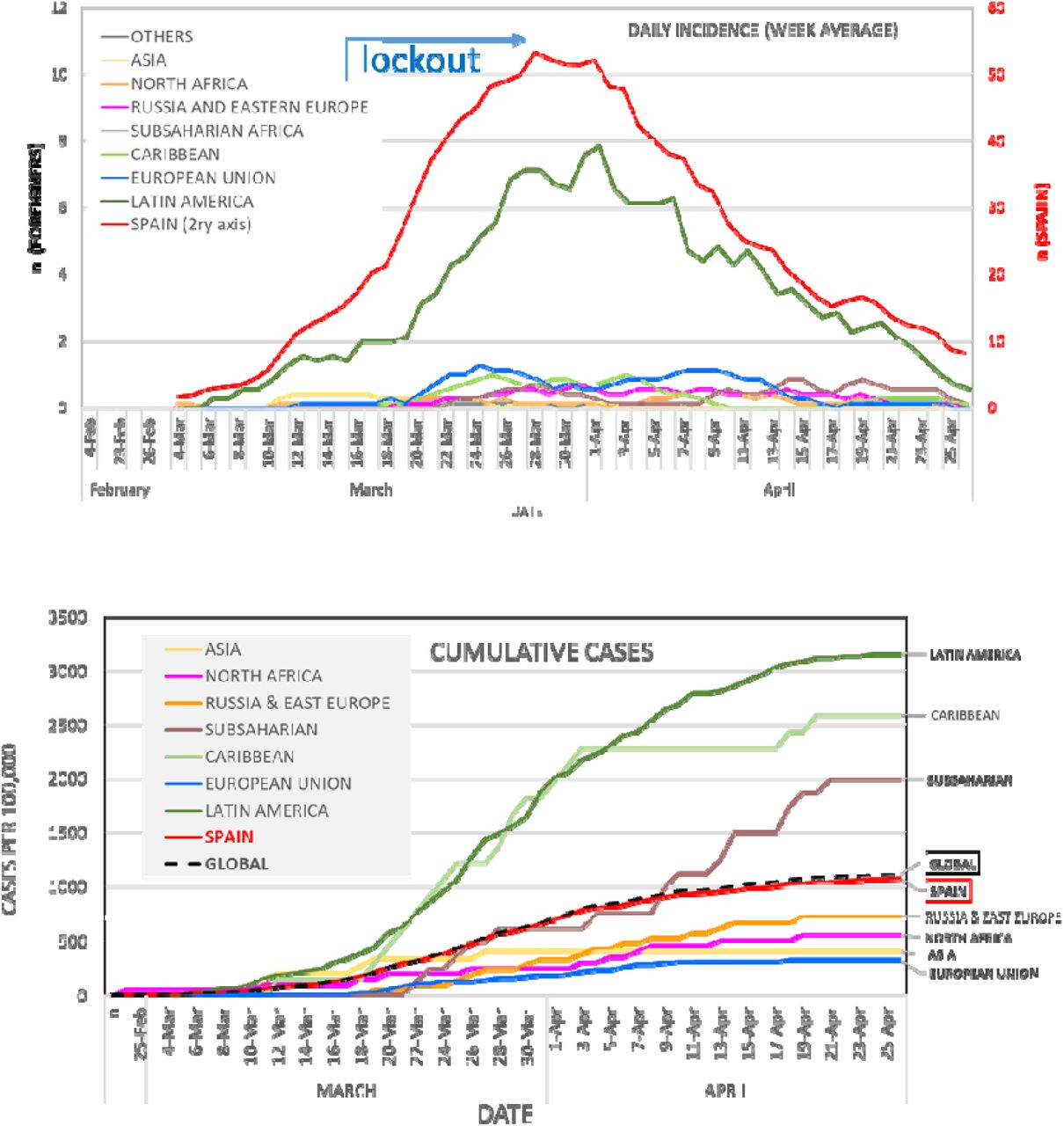
Evolution of clinical diagnosis of COVID-19 at Alcorcón. Panel A: daily diagnosis (graph represents for everyday the average number of daily diagnosis of the preceding week). Panel B Cumulative incidence rate of new diagnosis per region of the world.

Relative risks for age intervals (reference age < 30 years), sex (Panel A), as well as areas of the world (reference Spain) were calculated by negative binomial regression analysis (Panel B).
We next evaluated cumulative incidence rates of COVID-A-PCR+ for natives from different regions of the world as compared to Spaniards (Table2, Figure 1B,). Unadjusted incident rates for individuals from Europe, Asia and North Africa and Spain were lower than average, while for Sub-Saharan Africa, Caribbean and Latin-America were higher.
In order to have a better understanding of risks for migrants as compared to the local Spanish population we conducted a multivariate negative binomial regression analysis 16 adjusting for age and sex. The adjusted relative risks for COVID-PCR+ among migrants from Asia, European Union and Eastern Europe did not significantly differ from Spain (table 3). In contrast, the relative risk for Latin-America migrants was about 7-fold higher than that for Spaniards (RR 6·92; 95% CI 4·49-10·67, p <0·001). In addition, the adjusted risk was also increased for Sub-Saharan Africa (RR 3·66 95% 1·42-9·41, p=0 007) as well as Caribbean (RR 6·35 95% CI 3·83-10·55, p<0·001) in a highly clinical and statistically significant manner.
As a sensitive analysis (Table 3), we repeated our estimation with wider criteria (clinical diagnosis regardless of PCR results; n=1,691) and stricter criteria (patients requiring hospital admission because of moderate-to-severe COVID-19, n=877). In both cases, results remained essentially unchanged. Adjusted relative risks for the spectrum of COVID-19 among migrants from Europe, Asia or Northern African (essentially Morocco) did not differ from Spaniards.
In addition, adjusted risk for Sub-Saharan Africans, Caribbeans and Latinos was about 3, 6 and 7 fold higher in all clinical scenario (Table 3). As an exploratory evaluation, we performed a similar analysis for countries that had at least 800 inhabitants in Alcorcón (Table 1). Citizens from Romania, Ukraine, China, or Morocco did not exhibit increased rates for COVID-19 cumulative incidence (Supplemental Figure 4). In agreement with regional data, all Latin American countries showed a consistent increased risk for COVID-19.
Severe COVID-19, defined as death, critical care admission or hospital stay longer than 7 days occurred in 63% of the Spaniards as compared to 33% for migrants. Similarly, unadjusted mortality was higher for Spaniards (25% of admissions) than for migrants (6%). Most likely this mirrors the advanced age of patients with severe disease (median 76 years IQR 69·82 years) or death (median 79 years IQR 74-85), an age range virtually absent in migrants (Supplemental Figures 1, 2). Our data do not support a more severe disease among migrants residing in Spain.
Discussion
Our study describes for the first time that the incidence of COVID-19 varies for citizens of national versus migrants with a population-based approach in a Western European country. We used the best available updated registry of citizens residing in the reference population. This is also likely the case for migrants, since a number of social services rely upon the actual place of residence, even in the case of citizens in an irregular administrative position for the immigration authorities 12
Our estimation of the incidence of COVID-19 is a reasonable approach since the population primarily attended by our hospital is precisely the city of Alcorcón and there is no other public hospital in the city17. In case of an emergency such as COVID-19, it is likely that citizens rely even more into their local facilities. In any event, it is almost certain that a number, albeit small, of Alcorcón residents have been attended because of COVID-19 in hospitals different from ours and thus our data are likely an underestimation of the real incidence. We have excluded from our analysis 16% of COVID-19 cases attended in our hospital whose residence was not Alcorcón. Official data from the Community of Madrid indicates that our hospital receives a slightly higher number of patients from other areas than viceversa17. Accordingly, our underestimation of COVID-19 incidence in Alcorcón may be somewhere between 10-15%. We do not believe that these data modify substantially the relative incidence for migrants, since the proportion of COVID-19 migrants excluded from our study because of residence outside Alcorcon was essentially identical (17%) as that for Spaniards (16%).
Another critical issue relates to the actual access to medical care for migrants. Since July 2018 all individuals resident in Spain have access to free medical care in conditions virtually identical to Spaniards 18. In addition, the hospital is close to the city centre and serves a single urban area, with an easy access either by foot or public transportation. It thus seems likely that the request for free and accessible medical care reflects actual incidence and severity of the disease for both Spaniards and migrants.
Of note, there is a striking difference between diverse areas of the world and their relative risk for COVID-19. First, there seems to be an unadjusted relative lower COVID-19 risk for other European citizens as compared to Spaniards. This may be related to a younger age connected to the so-called ‘healthy migrant effect’ 19–22 Indeed, healthier and younger individuals are more likely to migrate in search for better economic conditions. It is also noteworthy that most European migrants come from countries such as Romania and Bulgaria with a lower economic per capita income 23. Most migrants from these countries also have jobs with a low qualification and salary 24 In spite of this socioeconomic handicap, the age-adjusted relative incidence of COVID-19 among migrants from Romania or Ukraine does not differ Spain. This argument may be even more outstanding when applied to migrants from Northern Africa, most of them from Morocco. Indeed, age adjusted COVID-19 incidence for Moroccans did not differ from Spaniards.
Our data cannot offer any clue regarding the situation for the Chinese community. Whether a potential higher risk related to a direct communication with people coming from China has been buffered by stricter isolation measures within the Chinese community or in their relationship with other local residents remains purely speculative.
The other major finding of our work is an apparent higher risk for COVID-19 for individuals from Sub-Saharan, Caribbean or Latin-American origin. All of them have equal access to the virtually universal health coverage available for Spaniards or migrants from other areas of the world. Migrants from these 3 areas of the world are younger than Spaniards, and as opposed to Latinos or African Americans in the USA, the do not exhibit higher prevalence of obesity, hypertension, diabetes or cardiovascular disorders10,20–22. On the other hand, they are usually employed for low-income jobs and pertain to a low socioeconomic status that may not be very different from Moroccans or Romanians 24 In spite of this, a higher risk is consistently detected when it is estimated globally for their regions of origin or for particular countries. Furthermore, the risk is clearly enhanced when adjusted for age and gender.
It might be argued that some migrants may rely less on primary care physicians and thus show a disproportionate use of hospital services 21,25. However, our sensitive analysis, restricted to more severe COVID-19 requiring hospital admission does not support this potential overuse of hospital resources.
Some limitations of our study must be addressed. First, we did not collect information regarding mobility or social interactions that may well differ for different migrant populations. Second, we did not have local data regarding socioeconomic status, education or health conditions for migrants. However, on aggregate, migrants from Romania, Ukraine or Morocco belong to a relatively lower socioeconomic stratum all along Spain24 and do not exhibit an increased risk for COVID-19 as opposed to migrants from Sub-Saharan Africa or Latin-America. There is no reason to consider that migrants residing in Alcorcón are on average particularly different from those residing in other cities in Madrid or Spain.
Once the above-mentioned factors do not seem to adequately explain this increased incidence, we should pay attention to the ethnic background of the populations. Our results suggest a gradual increased risk for Sub-Saharan and Latin-American with an intermediate value for Caribbeans consistent with their mixed ethnic background. Our findings may be of particular relevance since the focus of COVID-19 has shifted from China to Europe, then to the United States and now is unfortunately emerging in Africa and Latin America.
There are limited data regarding different susceptibility to respiratory viruses from different ethnic backgrounds. Some studies have suggested a greater susceptibility of racial minorities to influenza26,27. However, many studies have failed to dissociate clinical outcomes from socioeconomic issues, particularly unequal access to health care 6-9 Different susceptibilities to COVID-19 with a genetic background with unequal world distribution are just beginning to be explored28,29.
In summary, we report a selective increased risk for COVID-19 among certain migrant populations in Spain: Sub-Saharan, Caribbean and Latin-America that is not related to unequal access to health care. These groups may deserve a particular attention, particularly when our country, as well as others, is beginning a de-escalation of social distancing measures. In addition, our data are compatible with different genetic susceptibility to COVID-19 among diverse ethnic backgrounds that warrants further studies.
Data Availability
No individual patient data are avaiulable
Supplemental Figures

Age group distribution for Spaniards and Migrants residing in Alcorcon

Population age pyramids from different regions of the world among residents at Alcorcón.

Age group distribution of the global population and COVID-19 cases among al inhabitants (upper panel)Spaniards (middle panel) and migrants (lower panel)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Exploratory analysis. Crude and age and sex adjusted incidence of PCR-confirmed COVID-19 among Spaniards and migrants from different countries
References




