
Abstract
A growing number of studies investigate brain anatomy in migraine using voxel- (VBM) and surface-based morphometry (SBM), as well as diffusion tensor imaging (DTI). The purpose of this article is to identify consistent patterns of anatomical alterations associated with migraine. First, 19 migraineurs without aura and 19 healthy participants were included in a brain imaging study. T1-weighted MRIs and DTI sequences were acquired and analyzed using VBM, SBM and tract-based spatial statistics. No significant alterations of gray matter (GM) volume, cortical thickness, cortical gyrification, sulcus depth and white-matter tract integrity could be observed. However, migraineurs displayed decreased white matter (WM) volume in the left superior longitudinal fasciculus. Second, a systematic review of the literature employing VBM, SBM and DTI was conducted to investigate brain anatomy in migraine. Meta-analysis was performed using Activation Likelihood Estimation (ALE) on GM volume data. Alterations of GM volume, WM volume, cortical thickness or white-matter tract integrity were reported in 72%, 50%, 56% and 33% of published studies respectively. Spatial distribution and direction of the disclosed effects were highly inconsistent across studies. The ALE analysis revealed no significant decrease of GM volume in migraine. A significant increase of GM volume in the left superior temporal and angular gyri was detected in migraine, a result however based on a small number of studies. Overall there is to this day no strong evidence of specific brain anatomical alterations reliably associated to migraine. Possible explanations of this conflicting literature are discussed.
1. Introduction
Migraine is the most common neurological disorder in the adult population with a prevalence comprised between 8% and 17% [1]. Migraine attacks are characterized by acute, moderate to severe, recurrent headaches lasting between four to 72 hours, accompanied with nausea and/or hypersensitivity to visual (photophobia), auditory (phonophobia), olfactory (osmophobia) and/or tactile (allodynia) environmental stimulations [2]. Several migraine subtypes (not necessarily exclusive) have been defined based on migraine attack frequency (episodic and chronic migraine), presence of aura preceding the attack (migraine with and without aura), or even secondary symptoms such as vertigo/head dizziness (vestibular migraine).
A rich and still growing literature report brain structural alterations in migraine [3–6]. Identifying brain abnormalities associated with migraine is indeed expected to provide new insights into the migraine pathophysiology. Neuroimaging methods have widely improved since the last two decades, especially through the popularization of automated whole-brain morphometric techniques such as voxel- (VBM) and surface-based morphometry (SBM). However, despite numerous studies applying these techniques, no consensus has yet emerged identifying certain alterations as markers of the disease. It is still unclear whether recurrent headaches lead to systematic long-term changes of brain anatomy or even damage.
In this study we first aim to identify gray (GM) and white matter (WM) abnormalities in subjects with migraine during the interictal period using several hypothesis-free whole-brain morphometric analyses: VBM and SBM and tract-based spatial statistics (TBSS). Second, a systematical review of the literature was performed on whole-brain studies of GM and WM abnormalities in migraine in order to try to make sense of the conflicting results. To this end a meta-analysis of the literature was run with an Activation Likelihood Estimation (ALE) which determined the convergence of foci reported from different experiments [7].
2. New data
2.1. Methods
2.1.1. Participants
Twenty-five subjects were identified and diagnosed as migraineurs without aura by a neurologist specialized in cephalgia (GD, Hospices Civils de Lyon). Patients between 18 to 60 years old and reporting a migraine frequency between two to five attacks per month were included in this study. Exclusion criteria comprised migraine with aura, chronic migraine, a medical history of psychiatric or neurological disorders, ongoing background medical treatment other than contraceptive medication, and pregnancy. Patients who suffered from a migraine attack 72 hours prior to the scheduled MRI examination, were rescheduled at a later time, whereas those who suffered from a migraine attack within 72 hours post-MRI (n=6) were discarded from further analyses. Data from 19 migraineurs were thus retained for analyses (13 females, 6 males, mean age ± SD: 32.7 ± 8.7 years, all right-handed). Migraine patients filled out the Hospital Depression and Anxiety scale [8], the Headache Impact Test (HIT-6), a short questionnaire aiming to evaluate headache impact on everyday life [9] and the Migraine Disability Assessment Questionnaire (MIDAS) [10] (Table 1).
New Data. Demographics and headache profile of the control and migraine groups. HIT-6 scores are comprised between 36 (negligible impact of migraine on daily life) and 78. MIDAS scores between 0 and 5 correspond to little to no disability due to migraine, while scores higher than 21 correspond to a severe disability. Mean and standard deviation are provided when relevant. Group differences are tested using non-parametric Mann-Whitney U tests. NA: not applicable.
Nineteen control subjects with no medical history of psychological or neurological disorders were identified from a cohort of sixty-three healthy participants for whom MRI scan were available and acquired with a procedure strictly identical to the migraine group. The MatchIt R package [11] was used to select subjects matched for age, sex and total intracranial volume (TIV), as those three covariates are known to have distinct contribution to GM volume [12]. Propensity score matching was conducted using the nearest neighbor method [13] in order to minimize bias due to confounding factors. Additional demographic details are presented in Table 1. All persons gave their informed consent prior to their inclusion in the study.
2.1.2. MRI acquisition
MRI examinations for all participants were performed on a Magnetom Prisma Siemens 3T MRI scanner equipped with a 64-channel head/neck coil. A T1-weighted sagittal magnetization-prepared-rapid acquisition with gradient echo (MPRAGE) image (repetition time (TR) = 3500 ms, echo time (TE) = 2.25 ms, inversion time (TI) = 1000 ms, field of view (FOV) = 250×250 mm, matrix size = 288×288, spatial resolution: 0.9×0.9×0.9 mm), and a diffusion tensor imaging (DTI) sequence with 64 gradient directions and 38 continuous slices (b = 0 and 1000 s/mm2, TR = 10000 ms, TE = 72 ms, FOV = 240×240 mm, matrix size = 132×132, spatial resolution: 1.8×1.8×1.8 mm) were acquired.
2.1.3. Voxel-based and surface-based morphometry
The VBM and SBM analysis were conducted using the Computational Anatomy Toolbox (CAT12, dbm.neuro.uni-jena.de/cat/), an extension toolbox of Statistical Parametric Mapping software (SPM12, www.fil.ion.ucl.ac.uk/spm/software/spm12/). Default settings as detailed in the CAT12 manual (http://dbm.neuro.uni-jena.de/cat12/CAT12-Manual.pdf) were applied.
For the VBM analysis, GM, WM and cerebrospinal fluid (CSF) tissue segmentation was first performed. The resulting GM and WM masks were then aligned to the SPM12 tissue probability maps (DARTEL template in the MNI space), co-registered using DARTEL [14] and smoothed with a Full-Width at Half-Maximum (FWHM) kernel of 10 mm [15]. TIV was finally estimated for each participant.
For the SBM analysis, the automated workflow from the CAT12 toolbox which measures cortical thickness and reconstructs the central surface was used. Based on the central surface data, we estimated the gyrification index and sulcus depth [16]. Cortical thickness, gyrification index, and sulcus depth data were smoothed using a Gaussian filter with a FWHM kernel of 15 mm (default parameter).
2.1.4. Statistical analyses (VBM and SBM)
Statistical designs were prepared using SPM12. A two-sample t-test was performed at each voxel to evaluate differences between migraineurs and control participants in regional GM and WM volumes, cortical thickness, gyrification index and sulcus depth data. For volumetric data, TIV, age and sex were considered as nuisance parameters and consequently entered in the design matrix as covariates as recommended in [12, 15]. For surface data, only age and sex were entered as covariates. An implicit mask and a threshold masking (value=0.1) were applied to the images to remove voxels of the background from the analyses. Two contrasts were investigated: control > migraine, and migraine > control. Statistical inferences were made using non-parametric permutations and a Threshold-Free Cluster Enhancement (TFCE) correction was applied to the t-stats map produced (TFCE toolbox by Christian Gaser, http://dbm.neuro.uni-jena.de/tfce) to increase sensitivity (5000 permutations) [17] along with a family-wise error (FWE) correction to address multiple testing. Clusters were considered significant with p<0.05.
2.1.5. DTI analysis
DTI analysis was conducted using tools from the FMRIB software library (FSL v5.0, fsl.fmrib.ox.ac.uk/fsl/fslwiki) and the Nipype pipelines [18]. DTI images were first corrected for any susceptibility induced distortions [19], eddy currents, and head movements [20]. Fractional anisotropy (FA), mean diffusivity (MD), axial (AD) and radial diffusivity (RD) maps were calculated by fitting a tensor model at each voxel of the diffusion data. Tract-based spatial statistics (TBSS) was then performed on all participants’ FA images. TBSS analysis consisted first on non-linearly co-registering all FA images to the FMRIB58-FA standard-space template. A mean FA image was then created along with a skeleton of the major WM fiber tracts. Next, all participants FA images were projected onto this skeleton which will be fed into the voxelwise statistical analysis. This process was similarly applied to the MD, AD, and RD maps.
2.1.6. Statistical analyses (DTI)
The voxel-level non-parametric permutation test (randomise function in FSL) was used to investigate the following contrasts on FA, MD, AD and RD maps: control > migraine and migraine > control. A TFCE correction was applied to the produced t-stats images to increase sensitivity (5000 permutations) along with a FWE correction to address multiple testing. Surviving clusters are reported with p<0.05.
2.1.7. Power analysis
We ran a sensitivity power analysis using the G*Power software [21], using a power of 0.8 and an α error of 0.05 for our group comparisons. The required effect size given our sample size equals 0.82, suggesting an adequate sensitivity to large effects [22]. Please note that it is challenging to perform power calculations for statistical analyses that involve high-dimensional data [23], here power analysis was calculated as if we performed a simple one-tailed t-test.
2.2. Results
2.2.1. VBM results
Neither significant decreases nor significant increases of GM volume in migraine were detected. Compared to controls, WM volume was significantly decreased in migraine (corrected p=0.042, η2 = 0.78) in the left hemisphere which intersected the superior longitudinal fasciculus and the superior corona radiata (MNI coordinates of cluster peaks: [-30,-30,39], [-33,-26,26] and [-20,-38,39]), close to the superior temporal areas and the postcentral gyrus (Fig. 1). The reported effect size of this test is close to the required effect size of 0.82 as calculated by the G*Power software. No significant increases of WM volume in migraine were detected.
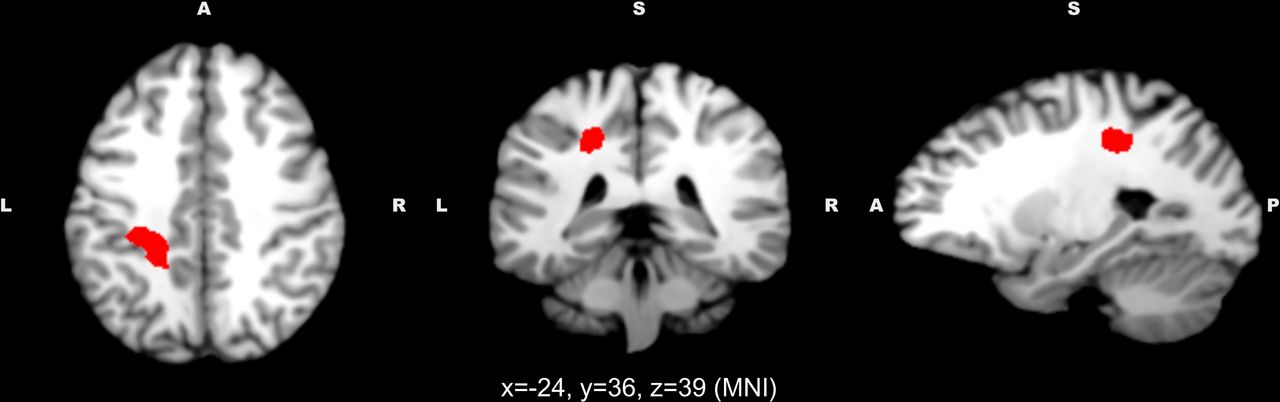
Voxels with a significant decrease of white matter volume in migraine participants (n=19) compared to healthy controls (n=19). From left to right, sagittal, coronal and axial views, MNI coordinates of the views are reported on the figure.
2.2.2. SBM results
No significant differences in cortical thickness, gyrification index, and sulcus depth were detected between the control and migraine participants.
2.2.3. DTI results
No significant differences in FA, MD, AD, or RD were detected between the control and migraine participants.
2.3. Discussion
With the present dataset, no brain anatomical differences could be detected in migraine regarding GM volume as assessed with VBM, cortical surface (thickness, gyrification and sulcus depth) as assessed with SBM, and in the integrity of WM as assessed with TBSS.
However, WM volume appeared to be decreased in migraine in the left superior longitudinal fasciculus (SLF). Only three studies (from the same research team) have yet reported WM volume decreases in migraine but none of them pinpointed such an alteration in the left superior longitudinal fasciculus [24–26] Moreover, no DTI study including the present one has reported altered WM integrity in this particular tract.
The SLF is an association tract which connects occipital and temporal areas to the frontal lobe. This pathway is involved in various cognitive processes [27], however the left SLF has been consistently linked to language processing (e.g. [28–31] as it connects Broca’s and Wernicke’s area [32]. To our knowledge, migraine is not associated to major language defects, however some neuropsychological studies have reported that migraineurs performed worse than healthy participants in verbal memory and verbal skills tasks (for a systematic review, see [33]). The SLF might also be involved in the control of the vestibular function [34]: an alteration of its integrity could underlie the vestibular symptoms observed in migraine as migraineurs are much more prone to vertigo and dizziness episodes than the general population [35, 36].
Overall we found little evidence for brain anatomical alterations in migraine, we now consider these negative results in light of a systematic review and a meta-analysis of the relevant literature.
3. Meta-analysis
3.1. Material and methods
3.1.1. Data sources and study selection
Systematic searches were performed on January 2019 in PubMed database without any publishing time restriction. For VBM studies, we used the combination of keywords migraine AND ((voxel based morphometry) OR VBM); for SBM studies, we used the combination of keywords migraine AND ((surface based morphometry) OR (cortical thickness) OR (gyrification)); for DTI studies, we used the combination of keywords migraine AND ((diffusion tensor imaging) OR DTI). Additional studies were also searched from reference lists of the included articles. Inclusion criteria were: (1) the article was an experimental article; (2) it was published in an English-speaking peer-reviewed journal, (3) it included a VBM (gray and/or white matter), SBM, or DTI comparison of adult patients with migraine vs. healthy controls. If patient group overlapped with another study, the study with the larger sample size was retained. A paper was excluded if the patient group was not afflicted with migraine as defined by the International Headache Society [2] (presence of cluster headache, medication-overuse headache, tension headache, etc.). Furthermore, studies performing whole-brain analysis and reporting results coordinates in a standard stereotactic space (MNI or Talairach) were separated from studies performing ROI analysis or that failed to include stereotactic coordinates of the results. For DTI studies, we did not exclude articles which did not report stereotactic coordinates of the results as it did not appear to be a common practice. For each paper, demographics and headache profile of the sample and analysis methods were extracted.
3.1.2. ALE meta-analysis
Regarding VBM or SBM studies, if a sufficient number of studies (>10 studies) reported a significant increase or decrease of a certain metric (ex. GM volume) in the patient group, results of those studies were combined with Anatomic Likelihood Estimation methods [7, 37, 38] to identify brain structures that were consistently affected in migraine. Coordinates of the peaks of significant clusters were extracted and if necessary, transformed to MNI coordinates using the conversion tool from the BrainMap toolbox (http://brainmap.org). All coordinates were then pooled and analyzed using the GingerALE software (brainmap.org). GingerALE blurred the included coordinates using a Gaussian filter with a FWHM value computed based on the sample size of the study. Then, the ALE statistic was computed for every voxel. We used a cluster-level FWE thresholding of p<0.05 with a cluster forming threshold of p<0.005 with 1000 permutations [39].
3.2. Results
3.2.1. VBM – Gray matter
The search strategy resulted in 61 relevant documents among which only 23 were retained. As displayed in Fig. 2, 18 were rejected for not being an experimental article, two for not using voxel-based morphometry, thirteen for not comparing adult participants with migraine with healthy controls, four for not presenting a whole-brain analysis and stereotactic coordinates of significant clusters and one for using the same sample as a previous article. Three articles from other sources were added, as well as the results from the present article, resulting in a total of 27 articles used for the meta-analysis (Table 2). Some articles investigated more than one subtype of migraine: results are then considered separately for the meta-analysis elevating the number of “actual” studies to 32. They involved a total of 1172 healthy participants and 1071 migraineurs.

Search strategy used for the inclusion of the studies considered in the present meta-analysis.
Summary of the voxel-based morphometry (VBM) studies included in the meta-analysis. N.T. = not tested, MwA = migraine with aura, MwoA = migraine without aura, FWE = family-wise error, FDR = false detection rate, TFCE = threshold-free cluster enhancement, vox = voxels, FWHM = full-width height maximum.
Out of 32 studies, 23 (72%) found differences in GM volume in migraine, including eight studies (25%) reporting both GM volume increases and decreases in migraine.
Gray matter volume decreases
Out of 32 studies, 18 (56%) observed a decrease of GM volume in the brain, these studies involved 527 healthy participants and 629 migraineurs. One hundred and twelve foci were considered for the ALE meta-analysis (Fig. 3). No brain regions revealed a significant decrease in GM volume in this meta-analysis.

Here are reported on a standard T1-weighted image all loci from the literature in which a significant difference in grey matter volume, white matter volume and cortical thickness in migraine has been detected (respectively n=32, n=10 and n=16 studies). Foci are blurred using a Gaussian filter with a Full-Width Height Maximum value computed based on the sample size of the study. The green gradient corresponds to an increase in migraine, the red gradient corresponds to a decrease in migraine. Please note that some studies have reported only the peak of significant clusters while others also reported also local maxima inside the significant cluster: a relatively high concentration of foci may not necessarily reflect convergence between studies.
Gray matter volume increases
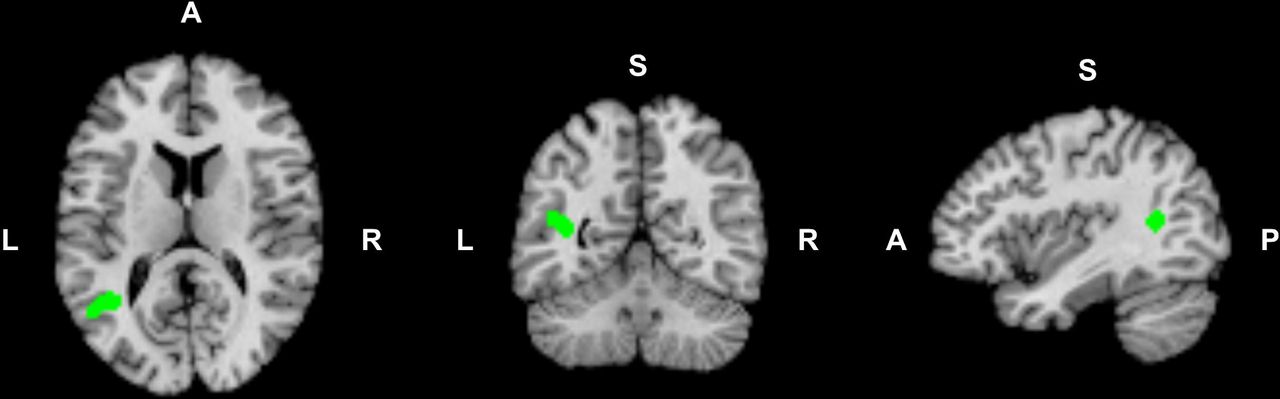
Out of 32 studies, thirteen (41%) observed an increase of GM volume in the brain, these studies involved 454 healthy participants and 541 migraineurs. Forty-three foci were considered for the ALE meta-analysis (Fig. 3). The analysis reported one significant cluster of increased GM volume (1160 mm3) (Fig. 4). It included the left superior temporal gyrus (extremum at −40, −54, 12: Brodmann area 22, p=0.01) and the left angular gyrus (extremum at −50, −60, 16: Brodmann area 39, p=0.01); Three out of thirteen studies contributed to this cluster [25, 40, 41].

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Results of the Activation Likelihood Estimation analysis combining 27 VBM studies of gray matter volume in migraine. In green, voxels with a significant increase of gray matter volume in migraine. From left to right, sagittal, coronal and axial views, MNI coordinates of the views are reported on the figure.
3.2.2. VBM – White matter
Out of the 27 articles retained for the meta-analysis of GM volume, only eight analyzed WM volume. Two of these eight investigated two subtypes of migraine elevating the number of “actual” studies to ten (Table 2). They involved a total of 249 healthy participants and 269 migraineurs.
Out of ten studies, five (50%) found differences in WM volume in migraine, including one study (10%) reporting both WM volume increases and decreases in migraine. This number of studies was insufficient for an ALE meta-analysis.
White matter volume decreases
Five of those studies (50%) observed a decrease of WM volume in the brain, these studies involved 162 healthy participants and 176 migraineurs. Nineteen significant foci were reported (Fig. 3). Visual inspection showed that six foci out of 19 were localized in the occipital lobe, others were dispersed in the rest of the brain.
White matter volume increases
Only one study (10%) reported an increase of WM volume in the superior frontal lobe, with one significant focus reported (Fig. 3).
3.2.3. SBM – Cortical thickness
The search strategy resulted in 42 relevant documents among which only 12 were retained. As displayed in Fig. 2, four were rejected for not being an experimental article, six for not using surface-based morphometry, thirteen for not comparing adult participants with migraine with healthy controls, four for not presenting a whole-brain analysis and stereotactic coordinates of significant clusters and two for using the same sample than a previous article. The results from the present article were added and an article was excluded for using a rather lax statistical threshold (uncorrected p-values with a 0.05 significance threshold), resulting in a total of thirteen articles used for the meta-analysis. Some articles investigated two subtypes of migraine: results are then considered separately for the meta-analysis elevating the number of “actual” studies to 16 (Table 3). They involved a total of 848 healthy participants and 776 migraineurs.
Summary of the surface-based morphometry (SBM) studies included in the meta-analysis. N.T. = not tested, MwA = migraine with aura, MwoA = migraine without aura, FWE = family-wise error, FDR = false detection rate, TFCE = threshold-free cluster enhancement, vox = voxels, FWHM = full-width height maximum.
Out of 16 studies, nine studies (56%) found differences in cortical thickness in migraine, including one study (10%) reporting both increases and decreases of cortical thickness in migraine. This number of studies was insufficient for an ALE meta-analysis.
Cortical thickness decreases
Six studies out of fifteen (40%) observed a decrease of cortical thickness, these studies involved 183 healthy participants and 243 migraineurs. Twenty-two significant foci were reported (Fig. 3).
Cortical thickness increases
Four studies out of fifteen (27%) observed an increase of cortical thickness, these studies involved 249 healthy participants and 300 migraineurs. Ten significant foci were reported (Fig. 3). Visual inspection did not reveal any pattern in the spatial distribution of the foci, all lobes present at least one focus and they are present in the two hemispheres.
Others surface metrics
Only two studies (including the present one) have investigated cortical gyrification. Zhang and colleagues found an increased gyrification index in left postcentral gyrus, superior parietal lobule and right lateral occipital cortex, and decreased gyrification index in the left rostral middle frontal gyrus in migraine [42], while our study did not observe any group difference. Only two studies (including the present one) have investigated sulcus depth and none of them detected a significant difference between migraine and control groups.
3.2.4. DTI
The search strategy resulted in 57 relevant documents among which only 7 were retained. As displayed in Fig. 2, six were rejected for not being an experimental article, seven for not using diffusion tensor imaging, 16 for not comparing adult participants with migraine with healthy controls, 19 for not presenting a whole-brain analysis (mainly articles providing ROI analyses) and two for using the same sample than a previous article. The results from the present article were added and an article found from personal sources, resulting in a total of nine articles used for the meta-analysis. Some articles investigated two subtypes of migraine: results are then considered separately for the meta-analysis elevating the number of “actual” studies to twelve (Table 4). They involved a total of 252 healthy participants and 352 migraineurs.
Summary of the diffusion tensor imaging studies (DTI) included in the meta-analysis. N.T. = not tested, MwA = migraine with aura, MwoA = migraine without aura, TBSS = tract-based spatial statistics.
In the following, we will consider decreased FA or AD and increased MD or RD as a sign of altered WM integrity. Out of twelve studies, four (33%) found differences in WM integrity. Decreased WM integrity in migraine was detected in three studies (25%), which involved 86 healthy participants and 91 migraineurs, in different fiber tracts depending on the studies. Only one study (8%) reported increased WM integrity in migraine. Further information is available in Table 4.
3.3. Discussion
All studies considered here investigated brain structures during the interictal period, for obvious practical considerations and also because the interictal alterations are more likely to reflect long-term changes in brain anatomy. It is noteworthy that migraine symptoms are not exclusive to the ictal period. If sensory disturbances clearly climax during the attacks, alterations of sensory processing extend beyond the ictal state [43–46]. Migraine may be associated to minor cognitive dysfunctions interictally [33, 47–49] and to vertigo and dizziness episodes [35, 36].
The systematic review of the literature resulted in a sufficient number of studies for an ALE analysis only for GM volume increases and decreases, not for changes of WM volume or of cortical thickness. The ALE analysis did not reveal any significant decrease of GM volume in migraine despite the fact that more than half of the studies did report at least one locus with a GM volume decrease. This result is explained by the scattering of the loci reported in the literature across the whole brain; no discernible cluster of loci could be observed (Fig. 3). However, the ALE analysis revealed a significant increase of GM volume in the left temporal lobe, around the angular gyrus. Despite a quite conservative statistical analysis, this result should be considered with caution as only three studies contributed to this significant cluster. The left angular gyrus has been associated to various cognitive processes including social cognition, spatial cognition, arithmetic, and reading [50]. While keeping in mind that the left and right angular gyri have distinct functional roles, it is worth noting that the right angular gyrus (as part of the right temporo-parietal junction) has been reported to be dysfunctional in migraine in several studies [51–54]Regarding WM volume, the low number of studies makes any conclusion uncertain. It appears that there is a tendency of WM loss on migraine as half of the studies reported WM volume decrease while only one reported WM volume increase. However, reported loci of WM volume decrease are relatively scattered across the brain. The situation is even more obscure concerning cortical thickness, since a similar number of studies reported cortical thickness increase and decrease which affected cortical areas dispersed across the cortical surface.
Finally, regarding DTI, a minority of studies reported alteration of white matter tracts in migraine. When they did, reported anatomical alterations were generally widespread but did not necessarily intersected across studies. In studies only investigating regions of interest (not presenting whole-brain analyses), alterations of white matter integrity in migraine were reported in regions as diverse as the thalamus [55], the brainstem [56, 57], the corpus callosum [58, 59], visual processing networks [60, 61] or fronto-insular tracts [62, 63].
In conclusion, for these three metrics of brain anatomical integrity, there is no emerging pattern of anatomical alteration in migraine.
4. General discussion
The question which underlies this whole study was quite simple: are there chronic anatomical alterations of the brain associated to migraine? In spite of a rich and growing literature, we are still far from a consensus on whether migraineurs present such alterations and which brain areas are potentially affected. Previous studies reported highly heterogeneous results, either in terms of the presence of a group effect or in terms of the direction and the localization of a potential effect. Can we make sense of this conflicting literature?
4.1. Heterogeneity of protocols, heterogeneity of results?
As illustrated in the tables 2 to 4, there exists quite a heterogeneity in the protocols chosen in previous studies in the literature.
First, numerous studies have favored investigating one subtype of migraine (migraine with/without aura, episodic/chronic migraine, vestibular migraine), in an attempt to reduce the variability in the migraine group. Previous results suggest that migraineurs with aura may differ anatomically from migraineurs without aura in terms of GM volume [41], of cortical thickness [64], and white matter integrity [65, 66], highlighting the importance of considering the two groups separately. Vestibular migraine differed from other types of migraine in terms of GM volume [41]. Finally, GM damage appears to be increased in chronic compared to episodic migraine [67, 68] and it correlates with attack frequency [26, 40, 68–70]. In conclusion, based on the literature, it is probable that each subtype of migraine presents a specific anatomical signature. More studies are needed for this hypothesis to be tested in a meta-analysis.
Second, all the studies considered here are not necessarily homogenous in terms of demographic characteristics. The mean age of the migraine sample ranges from under 30 to over 70 years old while there are suspicions that anatomical alterations evolve with age [26, 40, 68, 71, 72]. Gender seems to interact with the pathology [4], yet some studies chose to only include women and other (including the present study) opted for a sex-ratio closer to the migraine sex-ratio in the general population. Other variables such as comorbidities, education level or medication overuse may interact with the pathology and affect the patterns of anatomical alterations.
Finally, if voxel-based and surface-based morphometry analyses are based on standardized, streamlined workflows, slight deviations in the parameters can affect results in a major way. As illustrated in the tables 2 to 4, there are discrepancies on the statistical thresholds applied in such analyses: some studies have opted for uncorrected p-values, which is often an overly lax statistical strategy, or for a cluster-level control of FWE (implemented by default in SPM12 statistics) which is unlikely to be appropriate for VBM as it assumes stationary smoothness [73]. Inappropriate or lax statistical strategies may have led to a disproportionate rate of false positives, accounting for some of the heterogeneity in previous results. However, if we presume that there is a major anatomical alteration in migraine (i.e. with a large effect size), it should have been detected consistently, irrespective of the statistical strategy and therefore it should have been revealed through this meta-analysis.
4.2. A lack of statistical power?
Small sample sizes can be appropriate for exploratory studies as trivial effects are very unlikely to reach significance which ensures that only large-sized effects with actual scientific importance will be detected [74]. However, low statistical power reduces the reproducibility of the results and increase the probability of false positives [75]. Moreover, if subtle effects are to be expected, scrupulous matching of the control participants is crucial in order to avoid the detection of spurious effects [6].
Statistical power is usually relatively satisfactory in the studies considered in this meta-analysis. Most studies presented a sample size superior to 20 participants (in each group), especially in SBM and DTI studies. Some of them presented a sample size superior to 60 participants, ensuring the detection of even small effects and a limited probability of a false positive [74]. Interestingly, out of the three VBM studies with a large sample size (>60), only one of them detected an effect on GM volume. Out of the three SBM studies with a large sample size (>60), two of them detected an effect on cortical thickness, but not in the same direction. Such observations do not support the hypothesis of the presence of brain anatomical alterations in migraine.
4.3. The issue of publication bias
Publication bias is a widespread concern which is known to distort the results of meta-analyses as positive results are more likely to be published than negative results [76]. This risk is consubstantial to any attempt of performing a meta-analysis, however there are serious signs that this bias might be particularly exacerbated in the present situation. First, anatomical images (especially T1-weighted MRI images) are routinely acquired in numerous studies, notably in functional studies using fMRI. It is very likely that many scientific teams have usable datasets available for morphometry analyses. Second, voxel- and surface-based morphometry are fairly simple to use and widely available techniques, as streamlined workflows exist in two common free analysis toolboxes (SPM and FSL). They do not necessitate much of computing power nor are they too time-consuming.
It is reasonable to assume that numerous researchers in the field of migraine have attempted to analyze their anatomical data but that a large part of these analyses have never got published due to unconvincing results. Regarding VBM and SBM studies, even in the available literature, between one third and half of the articles did not report any significant difference between the control and migraine participants. It is probable that this proportion of negative results would be much higher if unpublished analyses were to be taken into account. Such proportions do not reassure on the actual presence of anatomical alterations in migraine.
This reasoning is not as appropriate for DTI studies as diffusion sequences are not routinely acquired in functional studies and as DTI analysis workflows are less common and streamlined than their VBM counterparts.
5. Conclusions and future directions
Previous studies reporting anatomical alterations in migraine do not converge neither on the direction nor on the spatial localization of the effect. Negative results are quite prevalent, especially in the context of a potentially strong publication bias. Based on current knowledge, there is to this day no strong evidence for the presence of systematic brain anatomical abnormalities associated to migraine. However, this study alone is not sufficient to rule out the existence of subtle anatomical alterations in migraine nor the existence of alterations specific to some migraine subtypes. Also, the number of studies on WM integrity and cortical surface in migraine is still quite low leading to weak conclusions. Further research is needed to produce a better picture.
What could be the next steps in researching brain anatomy alterations in migraine?
Small-sized, exploratory studies do not appear to be sufficient to shed light on possible anatomical alterations in migraine, especially regarding GM alterations. If a large-size effect existed, it should have been consistently reported by these studies. However, it remains scientifically crucial to keep on reporting morphometry analyses results, even if the statistical power is low, in order to provide information for future meta-analyses.
One of the major future developments could be longitudinal studies at different timescales. Migraine has been postulated to be a progressive disease with brain damage accumulating over the years, even if this proposition is controversial [6]. To our knowledge, at least two studies have attempted to study long-term effects of migraine (after a one-year or a four-year follow-up evaluation) with promising results [40, 72]. Further research is needed to confirm those results. It would be particularly interesting to investigate through longitudinal studies if spontaneous migraine remission with age is associated to a receding of anatomical alterations. On a different timescale, it has been suggested that anatomical alterations evolve along the migraine cycle [77]. All but one study in this article reported structural images during the interictal period. Deeper understanding of the dynamics of brain plasticity during the migraine cycle through short-term longitudinal studies would be of great interest.
Data Availability
Data that support the findings are not publically available because participants included in this study did not consent to sharing their personal data with other parties.
Conflict of interest
The authors declare that there is no conflict of interest regarding this article.
Ethical standards
The ethical approval of this work was obtained through the Hospices Civils de Lyon, approved by the local ethical committee (Comité de Protection des Personnes SUD EST III) and registered under the ID number NCT02791997. Therefore, this work has been performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
6. Acknowledgments
This work was supported by the French National Research Agency (ANR) Grant ANR-14-CE30-0001-01 (to Aurélie Bidet-Caulet and Anne Caclin). This work was performed within the framework of the LABEX CORTEX (ANR-11-LABX-0042) and the LABEX CeLyA (ANR-10-LABX-0060) of Université de Lyon, within the program “Investissements d’Avenir” (ANR-16-IDEX-0005) operated by the French ANR. The acquisition of imaging data was performed at the CERMEP imaging center in Lyon, we thank Frank Lamberton for his technical assistance. We thank Hesham ElShafei and Lesly Fornoni for their help in recruiting the participants.
7. References
- 1.↵
- 2.↵
- 3.↵
- 4.↵
- 5.
- 6.↵
- 7.↵
- 8.↵
- 9.↵
- 10.↵
- 11.↵
- 12.↵
- 13.↵
- 14.↵
- 15.↵
- 16.↵
- 17.↵
- 18.↵
- 19.↵
- 20.↵
- 21.↵
- 22.↵
- 23.↵
- 24.↵
- 25.↵
- 26.↵
- 27.↵
- 28.↵
- 29.
- 30.
- 31.↵
- 32.↵
- 33.↵
- 34.↵
- 35.↵
- 36.↵
- 37.↵
- 38.↵
- 39.↵
- 40.↵
- 41.↵
- 42.↵
- 43.↵
- 44.
- 45.
- 46.↵
- 47.↵
- 48.
- 49.↵
- 50.↵
- 51.↵
- 52.
- 53.
- 54.↵
- 55.↵
- 56.↵
- 57.↵
- 58.↵
- 59.↵
- 60.↵
- 61.↵
- 62.↵
- 63.↵
- 64.↵
- 65.↵
- 66.↵
- 67.↵
- 68.↵
- 69.
- 70.↵
- 71.↵
- 72.↵
- 73.↵
- 74.↵
- 75.↵
- 76.↵
- 77.↵
- 78.
- 79.
- 80.
- 81.
- 82.
- 83.
- 84.
- 85.
- 86.
- 87.
- 88.
- 89.
- 90.
- 91.
- 92.
- 93.
- 94.
- 95.
- 96.
- 97.
- 98.
- 99.
- 100.
- 101.
- 102.




