
Abstract
Background N-of-1 trials are single patient, multiple crossover, comparative effectiveness experiments. Despite their rating as “level 1” evidence, they are not routinely used in clinical medicine to evaluate the effectiveness of treatments.
Objective We explored the potential for implementing a mobile app-based n-of-1 trial platform for collaborative use by clinicians and patients to support data-driven decisions around the treatment of insomnia.
Methods A survey assessing awareness and utilization of n-of-1 trials was administered to healthcare professionals that frequently treat patients with insomnia at the Icahn School of Medicine at Mount Sinai in New York City. 1M electronic health records were analyzed to evaluate evidence for a comorbid relationship between insomnia and dementia or Alzheimer’s disease among a patient population that may benefit from n-of-1 trials for the selection of optimal sleep treatments.
Results A total of 45 healthcare professionals completed the survey and were included in the analysis. We found that 64% of healthcare professionals surveyed had not heard of n-of-1 trials. After a brief description of these methods, 75% of healthcare professionals reported that they are likely or highly likely to use an app-based n-of-1 trial at least once in the next year if the service were free and easy to offer to their patients.
Conclusions An app-based n-of-1 trials platform might be a valuable tool for clinicians and patients to identify the best treatments for insomnia. Educational interventions that raise awareness and provide training are also likely necessary. The electronic health record (EHR) may help identify eligible patients.
1 Introduction
Healthcare professionals routinely practice individualized care. They design treatment plans based on unique patient characteristics and clinical presentation, consider various levels of evidence for treatment efficacy, and help patients weigh the risks of side effects and other potential treatment burdens and trade-offs. While there is widespread agreement that we should not expect most treatments to work uniformly across most populations, the systematic evaluation of treatment effect remains a challenge for healthcare professionals and patients [1]. Healthcare professionals who practice “evidence-based medicine” generally use comparisons of means and proportions between large groups of patients (e.g. from clinical trials), but are intuitively aware that there exists large heterogeneity of effects for many disease processes and interventions.(possible references). N-of-1 trials create an opportunity in some contexts for healthcare professionals and patients to individualized treatment selection in a more systematic way. They are designed to help both parties make objective, data-driven treatment choices.
1.1 What are n-of-1 trials?
In clinical medicine, N-of-1 trials are used as a decision support tool to inform individualized treatment selection [2]. The Oxford Centre for Evidence-Based Medicine ranks n-of-1 trials as “level 1” evidence for determining whether a treatment benefits a patient [3]. N-of-1 trials are also viewed as a tool to enhance patient-centered care, insofar as the patient may be involved in the selection of treatments to compare, the selection of outcomes to measure, and the selection of the treatment to continue at the end of the trial [4]. Typically in an n-of-1 trial, a single patient completes a baseline period without any treatments, then alternates between two treatments in a sequence (i.e. “multiple crossover”) [5,6]. Where feasible, treatments may be blinded or placebo-controlled. Outcomes are measured during baseline and each treatment period. At the end of the trial, outcome measurements for each treatment are compared and a treatment is selected. N-of-1 trials may also be deployed to answer other common treatment investigations, such as whether to begin a treatment, proper dosing [7], disease-related nutrition recommendations [8–10], assessing treatment response in people with characteristics (e.g. rare genetic variants) not studied in randomized controlled trials of approved medications [11–13], and deprescribing [14], among others.
To be sure, n-of-1 trials are not useful in every context. They work best in patients with chronic or stable conditions. Non-curative treatments with rapid onset and rapid washout are ideal candidates for n-of-1 trials, whereas treatments with cumulative effectiveness (e.g. some antidepressants) or treatments that disrupt the nature of the underlying condition (e.g. surgery) are not. N-of-1 trials are particularly relevant in contexts where evidence for treatment efficacy is weak or where treatment effects are known to be heterogeneous across populations and among individuals [5].
1.2 Chronic insomnia: a testbed for implementation of n-of-1 trials
There are many therapeutic contexts where n-of-1 trials are able to serve unmet patient needs. Chronic insomnia is a good target disorder because there is a high prevalence of affected individuals in the general population and also across distinct clinical populations, including Alzheimer’s disease (AD), Parkinson’s disease (PD), attention deficit hyperactivity disorder (ADHD), pregnancy, post-treatment cancer patients, and many others.
N-of-1 trials have been implemented or are currently underway in several populations with insomnia. Coxeter et al. reported the effectiveness of valerian versus placebo in 24 patients with chronic insomnia [15]. Punja et al. have described a protocol to assess the effectiveness of melatonin in children (ages 6-17) taking medications for ADHD [16]. Nikles et al. have described a protocol to assess the effectiveness of melatonin in patients with PD [17].
Many patient populations have insomnia. It is one of the most common mental disorders [18]. Patients with insomnia have significant interest in finding the most effective treatment due to the negative impact on quality-of-life for patients, family and caregivers [19,20]. Poor sleep may also interact with recovery or progression of some diseases, including cardiovascular disease, depression, diabetes, AD, among others [21–25]. Estimates of the prevalence of insomnia in the general population vary in part due to the definition of insomnia used. The American Academy of Sleep Medicine (AASM) estimates that 33-50% of adults experience symptoms of insomnia and 10-15% of adults experience insomnia disorders that disrupt daily functioning [26].
The International Classification of Sleep Disorders, 3rd Edition (ICSD-3) includes seven categories of sleep disorders, including insomnia. The category of insomnia has three sub-types: chronic insomnia disorder, short-term insomnia disorder, and other insomnia disorder. The criteria for diagnosing chronic insomnia specify that a person must report a problem with sleep initiation or maintenance while having an adequate opportunity and environment to sleep. Symptoms must also cause clinically significant functional distress during the daytime; be present for at least three nights per week for at least three months. Chronic insomnia is likely a heterogeneous disorder [27]. Brain imaging studies, for example, have not found consistent patterns across patients with chronic insomnia [28].
There is limited efficacy data available for insomnia treatments in many patient populations, so decisional conflict is common. The American Academy of Physicians recommends cognitive behavioral therapy for insomnia (CBT-I) as the first line therapy in adults with chronic insomnia [29]. In a systematic review of randomized controlled trials (RCTs) that compared CBT-I and medications for the treatment of insomnia, evidence supports the notion that CBT-I is better than medications in some contexts [30]. However, among patients that choose to pursue CBT-I, around 20-30% fail to respond [31]. Furthermore, many people do not choose CBT-I because of several treatment-related burdens, including limited access to trained healthcare professionals, weekly therapy appointments, and out-of-pocket costs [32,33]. There is widespread use of pharmacological interventions and over-the-counter sleep aids. Around 20% of U.S. adults use prescribed or over-the-counter (OTC) sleeping medications each month [34]. While commonly used, many OTC sleep treatments have limited efficacy and safety data [35]. Furthermore, some sleep medications that are commonly used in younger populations for sleep problems are, for example, potentially inappropriate for use in older populations (e.g. hypnotics or Z drugs) [36].
For n-of-1 trials to be an effective tool for patients and healthcare professionals, the design of these trials should incorporate the precise needs of the populations they intend to serve. Next, we describe one patient population where chronic sleep disturbance is a salient issue: individuals at risk for AD with chronic sleep problems.
1.3 Alzheimer’s and sleep disturbance
AD is a critical public health concern with an estimated 131 million people worldwide predicted to be affected by the year 2050 [37]. More than six million older Americans have AD [38,39] and the annual incidence of the disease is estimated to rise to one million cases by 2050, which is more than double the current incidence [40]. Research into possible preventive measures is an urgent need, especially for people at risk due to family history or genetic predisposition. Primary prevention of AD is currently seen as the most effective strategy at reducing the prevalence of AD over the next several decades [39]. In recent years, sleep has been identified as a potential modifiable risk factor for prevention or delay of AD [41].
The connection between poor sleep and negative outcomes among the elderly population has long been established. In the 1990s, a prospective study of elderly people living in New York City found that insomnia among males was the strongest predictor of mortality and placement in a nursing home, exceeding many other factors analyzed, including age, income, health, and activities of daily living (ADL) [42]. Another prospective study found that older women with sleep disturbance were more likely to get dementia or mild cognitive impairment (MCI) [43,44].
In 2017, a meta-analysis of 27 observational studies found that poor sleep might explain around ∼15% of cases of cognitive impairment or AD [45]. They observed that people with sleep problems had a 1.55, 1.65, and 3.78 times higher risk for AD, cognitive impairment, and preclinical AD than individuals without sleep problems, respectively [45]. They also examined the relative risks related to specific sleep problems, including short and long sleep duration (1.86), poor sleep quality (1.62), circadian rhythm abnormality (1.38), and insomnia (1.38) [45].
The conventional wisdom is that changes in the brain due to AD causes sleep disturbance. Indeed, the prevalence of sleep problems among patients with AD range from 25-50% [46]. Recent evidence suggests causality might also work in the other direction: sleep disturbance as a risk factor for developing AD [24,41,47,48]. Several recent studies provide evidence of a plausible mechanism: increased amyloid-β production during periods of sleep deprivation. A single night of sleep deprivation leads to elevated amyloid-β-42 (Aβ42) in the cerebrospinal fluid of healthy middle-aged men [49]. In a small, 3-arm, crossover RCT researchers found that sleep deprivation increased overnight amyloid-β (−38, −40, −42) levels by 25–30%, while regular sleep or sedated sleep showed no change in Aβ levels [50]. The connection between sleep disturbance and risk for AD remains unproven and other plausible mechanisms have been proposed [51].
With the emerging evidence around the importance of sleep, people with a family history of Alzheimer’s disease and those with genetic risk factors (e.g. APOE-e4) are likely to be motivated to find the most effective interventions to address chronic sleep problems. Indeed, the REVEAL Study observed healthy behavior change among patients that received genetic risk information for Alzheimer’s disease, even in the absence of any proven approaches to prevention [52]. This group of individuals are likely to meet many of the criteria identified by clinicians in qualitative interviews about ideal patients for n-of-1 trials: “proactive, cognitively intact, reliable, motivated, and engaged in a trusting physician–patient relationship” [53].
1.4 Key questions for the current study
The purpose of this study is to collect preliminary evidence to inform potential routes for the implementation of an app-based n-of-1 trial platform, called the N1 app. While this platform may be adapted to inform the optimal selection of treatments for a variety of disorders and wellness-related goals, patients with insomnia have been identified as a potential population to target due to the prevalence of the condition, limited evidence for efficacy of treatments across some patient populations, the possibility to incorporate wearable devices for the passive collection of outcome measures [54], among others.
In this study we aim to assess the familiarity and experience with n-of-1 trials in a sample of healthcare workers that frequently care for patients with insomnia. Further, we examine the characteristics of a hospital patient population that may stand to benefit from n-of-1 trials for the selection of optimal sleep treatments. One hypothesis is that healthcare professionals are currently familiar with, but do not regularly use n-of-1 trials. A second hypothesis is that data mining of Electronic Health Records (EHR) in a hospital, health system, or health plan could be a viable route for n-of-1 trial patient recruitment, which we explore through the assessment of the comorbidity relationship between insomnia and dementia.
2 METHODS
2.1 Survey
2.1.1 Instrument
The Office for the Protection of Human Subjects at Mount Sinai approved a protocol to administer a voluntary, anonymous survey to healthcare professionals. The exploratory, cross-sectional survey administered has three sections (a) sociodemographics (b) experience and satisfaction with the treatment of patients with insomnia and (c) awareness and utilization of n-of-1 trials (see Datasheet S1).The survey was administered online through REDCap (Research Electronic Data Capture) hosted by the Icahn School of Medicine at Mount Sinai [55].
2.1.2 Sample and recruitment
We chose to recruit a sample of clinicians and nurse practitioners through the Department of Psychiatry due to the regularity with which these healthcare professionals treat patients with insomnia. We sent messages through the department mailing list and advertised at bimonthly Grand Rounds events during October and November of 2019.
2.1.3 Statistical analysis
We primarily use standard descriptive statistics to summarize the survey results. We further assessed differences of participants awareness of n-of-1 using two-sided Chi-squared test for categorical variables and a t-test for continuous variables. Using the same methods, we also assessed associations for willingness to use a n-of-1 digital service, which we binarized due to low sample size and imbalanced responses into “More likely” (consisting of “Strongly agree” and “Agree” responses) and “Less likely” (consisting of “Neutral”, “Disagree”, and Strongly disagree” responses).
2.2 Electronic Health Records Analysis
2.2.1 Clinical Cohort
We utilize clinical data from the EHRs of the Mount Sinai Hospital (MSH). MSH is an urban, tertiary care hospital located on the Upper East Side of Manhattan in New York City. The clinical data contained within the EHRs consists of structured data of patient information such as encounters, disease diagnoses, lab test results, vital signs, medication prescriptions, and procedures among others.
2.2.2 Phenotyping process and cohort breakdown
For the current study, we restrict our research cohort to individuals with at least one recorded clinical feature, who were at least 70 years old, with a minimum of five years of medical history in our system, and ICD codes for both insomnia and AD or dementia (See Datasheet S2), leaving 2632 unique patients for subsequent analyses (see Figure S1). This filtering procedure allowed for more robust phenotyping by prioritizing individuals 65 and older that are more likely to be regular patients in the MSH system (i.e., currently 70 years or older with at least five years of prior history and at least one diagnostic code). Due to HIPAA requirements, the ages of patients within the research cohort are right-censored at age 90. The mean age of the cohort is 84.3 ± 12.5 (std). The self-reported sex breakdown of the cohort is 71.1% female, 28.8% male, and 0.04% not available. The self-reported race breakdown of the cohort is: 50.8% Caucasian (White), 30.4% African American (Black), 12.8% Other, 6.6% Unknown, and 2.7% Asian. The self-reported ethnicity breakdown of the cohort is: 43.9% Hispanic/Latino, 25.5% non-Hispanic/Latino, and 31.9% Unknown.
2.2.3 Enrichment analysis
We used a chi-squared test to evaluate the relationship between insomnia and AD or dementia. Our null hypothesis is that the diseases are independent and they have no significant comorbidity relationship. Specifically, we tabulated the number of individuals that pass the above filtering criteria that have both AD or dementia diagnosis and an insomnia diagnosis, compared to those with one or the other, and to those with neither.
2.3 Ethics approval
This study has been approved by the Institutional Review Board at the Icahn School of Medicine at Mount Sinai (IRB-18-00789 & IRB-19-02369)
3 RESULTS
3.1 Survey Results
3.1.1 Sample characteristics
A total of 66 participants consented to the survey, 49 participants completed the survey and the responses from 45 participants were included in the analysis (see Figure S2). This sample of 45 healthcare professionals from a large, urban hospital are mostly practicing clinicians (88.9%), affiliated with the Department of Psychiatry (88.9%), in their first or second decade of clinical practice (64.4%), with a primary specialty of Psychiatry and Neurology (93.3%) (see Table 1).
Sociodemographics of the sample of healthcare professionals surveyed
3.1.2 Experience and satisfaction of sample with current treatments for patients with insomnia
Most healthcare professionals surveyed frequently see patients with insomnia in their clinical practice with 88.9% reporting daily or weekly encounters. A majority of participants also expressed their dissatisfaction with available treatment options for their patients with insomnia, with 55.6% disagreeing or strongly disagreeing with the statement: “I am satisfied with the available treatment options for my patients with insomnia.” Participants also perceived their patients as being dissatisfied with available treatment options, with 62.2% disagreeing or strongly disagreeing with the statement: “My patients are satisfied with available treatment options for insomnia” (see Table 2).
Summary of survey results from a sample of healthcare professionals on their experience and satisfaction with current treatments for insomnia
3.1.3 Awareness and use of n-of-1 trials
Most participants surveyed were unfamiliar with the concept of n-of-1 trials, with 64.4% reporting that they had never heard of them before. Following this survey question, participants were presented with a short description of n-of-1 trials that also included a screenshot of the N1 app, a smartphone based n-of-1 trial platform developed at the Icahn School of Medicine (see Data sheet S1) [56,57]. They were asked to consider the scenario that “a free service [existed] that made it easy for you to offer n-of-1 trials to select patients in your practice with insomnia. The patient would conduct the mobile app-based trial at home. At the conclusion of the trial, the analyzed results would be available to you and the patient to review together.” Excluding 5 participants that did not respond to this question, 75% of participants (i.e. 30 of 40) reported that they were either “likely” or “highly likely” to “use a service like this to make data-driven treatment choices at least once in the next year.”
Of the 16 healthcare professionals that reported that they were aware of n-of-1 trials, 3 reported that they had previously used an n-of-1 trial in the treatment of their patients. For the remaining 11 participants that were aware of n-of-1 trials, had never used them in their clinical practice, and reported a primary reason for the lack of adoption, 45.4% cited inadequate training in n-of-1 trial design.
We further assessed the relationship between various questionnaire features and having heard of n-of-1 trials (n=45). We found no significant relationship between having heard of n-of-1 trials and age (p = 0.54, t = −0.61), sex (p = 0.09, X-squared = 2.91), race (p = 0.10, X-squared = 7.92), ethnicity (p = 0.75, X-squared = 0.58), clinical degree (p = 0.84, X-squared = 0.04; one individual with both degrees not included), number of years practiced (p = 0.29, X-squared = 5.02), frequency of seeing patients with insomnia (p = 0.50, X-squared = 2.36), satisfaction of current treatments for insomnia (p = 0.23, X-squared = 5.65), or perceived patient satisfaction of current treatments for insomnia (p = 0.80, X-squared = 0.99).
We also assessed the relationship between various questionnaire features and willingness to use a n-of-1 digital service app (n=40; binarized response). We found no significant relationship between willingness to use a digital app service and age (p = 0.22, t = −1.27), sex (p =0.23, X-squared =1.45), race (p =0.54, X-squared = 3.13), ethnicity (p = 0.20, X-squared = 3.26), clinical degree (p = 0.81, X-squared = 0.06; one individual with both degrees not included), number of years practiced (p = 0.67, X-squared = 2.36), frequency of seeing patients with insomnia (p = 0.64, X-squared = 1.68), satisfaction of current treatments for insomnia (p = 0.21, X-squared = 5.87), or perceived patient satisfaction of current treatments for insomnia (p = 0.82, X-squared = 0.93).
3.2 Electronic Health Records clinical comorbidity analysis
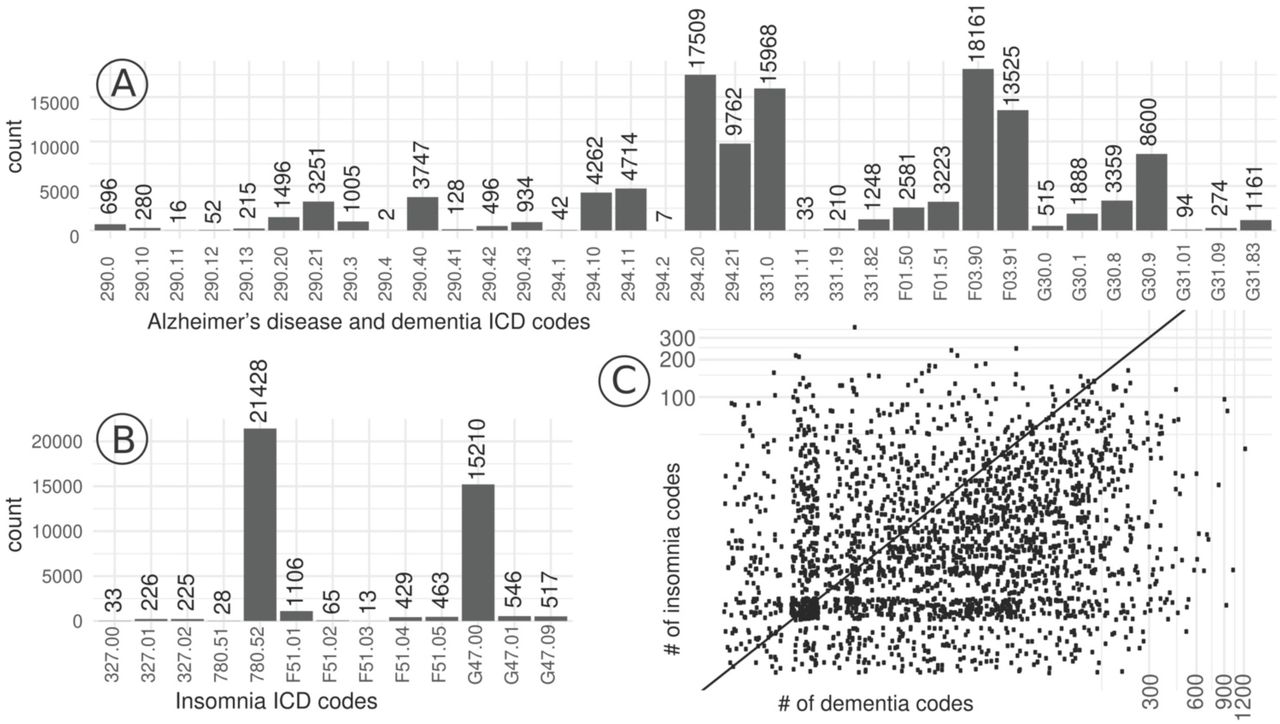
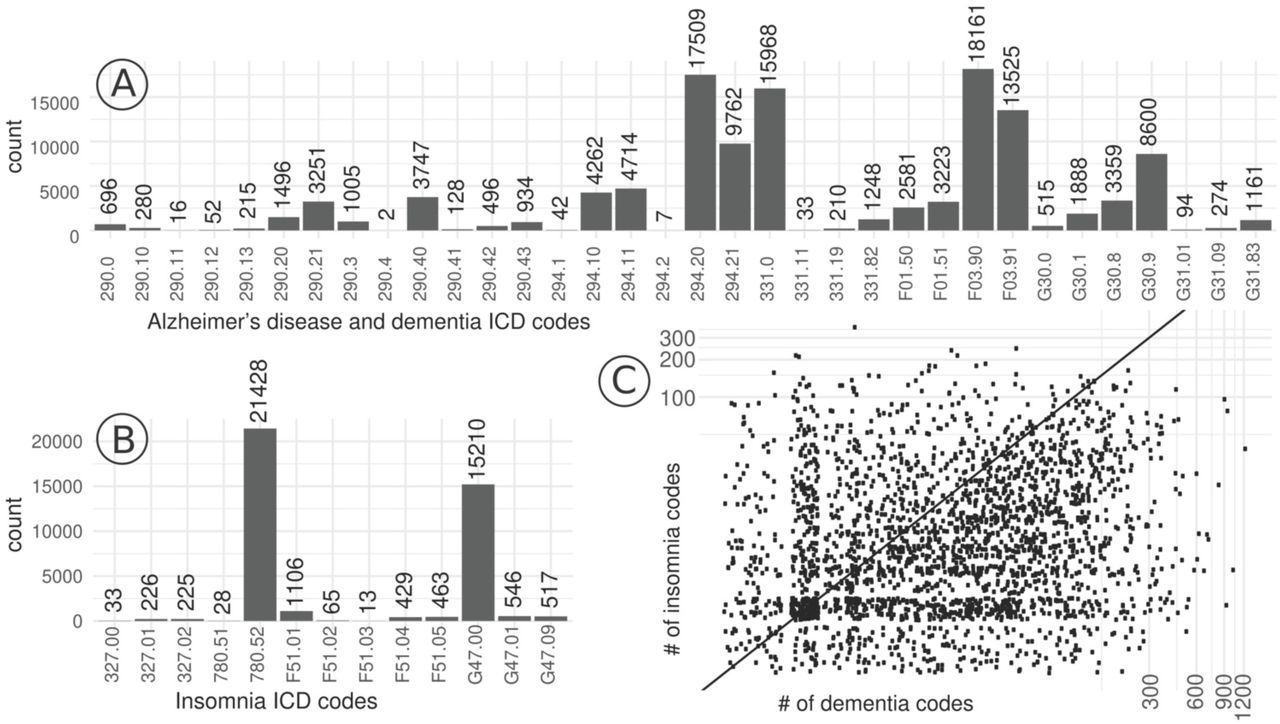
In the EHR analysis, our goal was to discern whether an enriched comorbidity relationship between AD or dementia and insomnia was present in the MSH patient population. We present the breakdown of patients by ICD code for each disease category in Figure 1 (A and B). We further visualize the distribution and frequency of ICD codes between both disease categories in Figure 1C.
{kind=link}
The breakdown of patients by each ICD-9-CM and ICD-10-CM code of each category, specifically for A) Alzheimer’s disease or dementia and B) insomnia. Note that there might be patients that have more than one associated code. C) a scatter plot visualizing the distribution and frequency of patients by number of ICD codes of each disease category. Here, we display the number of ICD codes associated for each patient for insomnia codes on the y-axis and AD or dementia codes on the x-axis.
The null hypothesis was that the two diseases were independent from one another. We performed a chi-square assessment for the rates of individuals that passed our eligibility criteria (see Figure 1) had instances of both diseases compared to one or the other against a background of those with neither (see Table 3). From this analysis, we obtained a chi-squared test statistic of 2978 which corresponds to a statistically significant p-value of < 2.2 e-16. Odds ratio was used to quantify the strength of the relationship between insomnia and Alzheimer’s/dementia. We obtained a relative risk of 3.01 and an odds ratio of 3.57, with a 95% confidence interval of 3.40-3.75.
A contingency table tabulating the number of patients in the Mount Sinai Hospital Electronic Health Records that pass our filtering criteria with Alzheimer’s disease (AD) or dementia and insomnia.
4 DISCUSSION
The N1 app aims to facilitate the design, administration, and analysis of n-of-1 trials [56–58]. Individuals with insomnia or other chronic sleep disturbance issues are a population that may benefit from access to n-of-1 trials for data-driven treatment selection. While these multi-crossover, comparative effectiveness trials have been in use for decades, awareness and adoption by healthcare professionals continues to face challenges, as our survey further indicates. Yet, we are encouraged that the healthcare professionals sampled did also report substantial receptivity to future use of app-based n-of-1 trials to inform the treatment of patients with insomnia provided there were a service that made such trials free and easy to implement. The lack of awareness of n-of-1 trials coupled with receptivity to their use suggests that educational interventions may address at a current barrier to wider utilization of n-of-1 trials.
Historically, several centers have been established to support the implementation of these trials for local clinicians as a service [7,53,59]. One center currently operates at the University of Queensland in Australia with a focus on sleep [60]. While these centers have documented many cases where patients and clinicians were aided in the selection of treatments, the centers are often experiments themselves that last as long as funding permits their operation, for example. For a time in the United States, there was a Current Procedural Terminology (CPT) code for “personalized medicine tests” that suggested a route to reimbursement for the effort required to design, administer and analyze an n-of-1 trial [4]. Writing in 2008, Kravitz et al. suggested that one alternative to the model where n-of-1 trials take root and gain traction primarily through academic clinical centers is the possibility that they “cast off some of their academic trappings and focus on appealing to what patients want and need” [4].
One of the major challenges with prospective studies, including n-of-1 trials, is cohort identification and recruitment. A benefit of working within a health system is the possibility of accessing retrospective patient data within the EHR. Of course, there are plenty of challenges of working with such data (e.g., bias and missingness) but the EHR also offers countless opportunities for research and a promising resource for patient engagement [61]. For instance, study recruitment via EHRs and patient portals are an emerging trend for pragmatic trials [62]. In our EHR analysis, we found a significant comorbidity enrichment between sleep disturbances, specifically insomnia, and AD or dementia. This finding is encouraging as it replicates a previously established association and reinforces the notion of using the EHR to aid in the construction of cohorts with specific features for research and recruitment.
While healthcare practitioners take into consideration each patient’s unique characteristics and strive to use the most up-to-date information to make informed therapeutic recommendations, there will always be some variability and uncertainty in outcomes. Leveraging n-of-1 trials as self-contained experiments can quantify individual outcomes and can better optimize treatment selection in some contexts. We believe growth in the adoption of n-of-1 trials will enhance the precision of treatment selection for many individuals. App-based platforms offer the potential to reduce some barriers, but other challenges still remain.
6 Author contributions
All authors listed have made a substantial, direct and intellectual contribution to the work, and approved it for publication.
7 Data availability
The survey and electronic health record datasets for this manuscript are not publicly available because of privacy considerations of patients and clinical practitioners.
5 Acknowledgments
This study is funded by the Icahn School of Medicine at Mount Sinai and a generous gift from Julian Salisbury. Thanks to Drs. Richard Kravitz MD (UC Davis) and Andrew Avins MD (Kaiser Permanente) for providing feedback on the survey instrument and the manuscript, and also thanks to Alex Charney MD PhD (Mount Sinai) for providing feedback on the survey instrument. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
8 References




Subject Area
Reviews and Context
0
Comment
0
TRIP Peer Reviews
0
Community Reviews
0
Automated Services
0
Blogs/Media
Author Videos