Article Text

Abstract
In the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic, pathologists can be exposed to infection handling surgical specimens. Guidelines related to safety procedures in the laboratory have been released. However, there is a lack of studies performed on biopsy and surgical resection specimens. Here we report the detection of SARS-CoV-2 in formalin-fixed paraffin-embedded samples from surgical resection of tongue squamous cell carcinoma of a patient who developed COVID-19 postsurgery. RNA of SARS-CoV-2 strain was detected in the tumour and the normal submandibular gland samples using real-time PCR-based assay. No viral RNA was found in metastatic and reactive lymph nodes. We demonstrated that SARS-CoV-2 RNA can be detected in routine histopathological samples even before COVID-19 disease development. These findings may give important information on the possible sites of infection or virus reservoir, and highlight the necessity of proper handling and fixation before sample processing.
- viruses
- pathology, oral
- pathology, molecular
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) pandemic is locking down the entire world. This pandemic started a few months ago in Wuhan, People’s Republic of China and has dramatically spread worldwide to other countries.1 2 The outbreak in Northern Italy has been particularly serious for the high number of deaths caused by COVID-19 and the high number of people requiring intensive care treatment. In this situation, it is imperative to reduce the risk of in-hospital transmission of virus among other patients and healthcare workers.3 Protective procedure and personal protective equipment have been recommended to healthcare workers, in some situation belatedly.
Different scientific societies of pathologists proposed recommendations and guidelines to address the problem of safety in the laboratories that deal with SARS-CoV-2-positive samples.4 However, handling of fresh samples especially during intraoperative consultations is routinely requested, and it may occur for samples from patients with unknown SARS-CoV-2 status or before the appearance of COVID-19 signs and symptoms.
SARS-CoV-2 detection in surgical tissue specimens has not been described so far. Indeed, clinical features, chest CT scan appearance and their association with rapid viral testing on pharyngeal swab offer a prompt diagnosis.5 Most available SARS-CoV-2 tests rely on rapid real-time PCR (RT-PCR) assays and have been developed to analyse fresh samples from lower respiratory tract, sputum and upper respiratory tract.
Here we performed SARS-CoV-2 test on formalin-fixed paraffin-embedded (FFPE) tissue specimens from a patient with tongue squamous cell carcinoma who underwent surgical resection before knowing the SARS-CoV-2 status and the onset of COVID-19 symptoms. We sought to (1) show the feasibility of SARS-CoV-2 testing in FFPE tissue specimens using rapid RT-PCR assay; (2) investigate the presence of COVID-19 virus in different anatomical sites; and (3) emphasise the potential risk for pathologists handling samples from patients with unknown SARS-CoV-2 status.
Case presentation
On 9 March 2020, a 50-year-old non-smoker and non-drinker man with a diagnosis of squamous cell carcinoma of the right side of mobile tongue, clinically staged as cT2N1M0, was admitted to the Division of Otolaryngology and Head-Neck Surgery of the European Institute of Oncology (IEO) to undergo surgical resection of the tumour. Presurgical general conditions were good with no fever or respiratory symptoms. Chest X-ray and laboratory tests were normal. On 10 March the patient underwent a major surgery: type IIIb glossectomy6 with an ‘en bloc’ resection of the ipsilateral cervical lymph nodes (levels 1–4) and reconstruction of the surgical defect with forearm free flap. An intraoperative consultation was requested on the surgical margin of the base of the tongue that was performed on frozen section and reported as negative. The entire specimen was fixed in 10% neutral buffered formalin for 24 hours before gross examination and sampling. Macroscopically there was a greyish, hard, ulcerated, deeply infiltrating tumour of 2.3 cm (major axis) and deep of invasion of 10 mm on the right margin of the tongue. A sampling of the neoplasia, salivary gland and lymph nodes was made according to standard procedures. Histologically, non-keratinizing, poorly differentiated squamous cell carcinoma infiltrating the extrinsic tongue muscles was seen. A single metastasis with extranodal spread was found in level IIA of the right cervical lymph nodes. Final tumour pathological staging according to TNM 8 ed.7 was pT2N3b cM0, stage IVb.
Two days after surgery the patient developed hyperpyrexia (39.2°C); laboratory test revealed leucocytosis with increased neutrophils count and decreased lymphocytes. On day 3 dry cough and mild dyspnoea appeared. Chest X-ray performed in intensive care (figure 1) raised the suspicion of a viral pneumonia. Rapid SARS-CoV-2 testing performed on nasopharyngeal swab was positive. The patient was isolated and properly cared for in a dedicated IEO-COVID-19 department where he gradually recovered.

Chest X-ray of the patient performed in the intensive care unit showed an ill-defined ground-glass opacity (arrows) involving the right lung. AP, anteroposterior.
Materials and methods
Representative FFPE tissue blocks of tongue carcinoma, nodal metastasis, histologically non-metastatic lymph nodes and normal submandibular salivary gland from this case were selected for the analysis. Moreover, 10 FFPE samples from patients with lung cancer who underwent surgical procedures in our institution during the last month and six bronchoalveolar lavages obtained from endobronchial ultrasound-transbronchial needle aspiration- procedures were also included to assess SARS-CoV-2 test performance on different specimen types. All the patients gave informed consent regarding the storage and the use of these samples for research purpose.
RNA was extracted automatically with the RSC RNA FFPE KIT by Promega Maxwell instrument (Promega, Madison, Wisconsin, USA) and quantified with the Quantus fluorometer (Promega).
SARS-CoV-2 test was performed using the CE-IVD Logix Smart COVID-19 kit (Co-Diagnostics, Salt Lake City, Utah, USA), an in vitro diagnostic test based on RT-PCR technology that analyses the presence of RNA SARS-CoV-2 strain. Two synthetic RNA molecules carrying sequences homologous to COVID-19 virus and provided with the kit were used as positive control. Positive and negative controls were included in each run. Internal control was also evaluated for each sample to identify possible quantitative PCR inhibition, confirm the integrity of the reagents and verify the quality of sample extraction. A positive result was considered with positive internal control and an amplification curve or cycle threshold value for COVID-19 at or below 45 cycles.
Results
H&E-stained slides of squamous cell carcinoma, submandibular gland and lymph nodes selected for RNA extraction and SARS-CoV-2 test are shown in figure 2. RNA SARS-CoV-2 strain was detected in the sample from squamous cell carcinoma of the tongue (table 1 and figure 3). Viral RNA was also found in the histologically normal submandibular gland; lymph nodes were negative, including metastatic and non-metastatic samples (table 2, figure 4). No SARS-CoV-2 RNA was identified in specimens from patients with lung cancer and bronchoalveolar lavages (tables 1 and 2, figures 3 and 4).
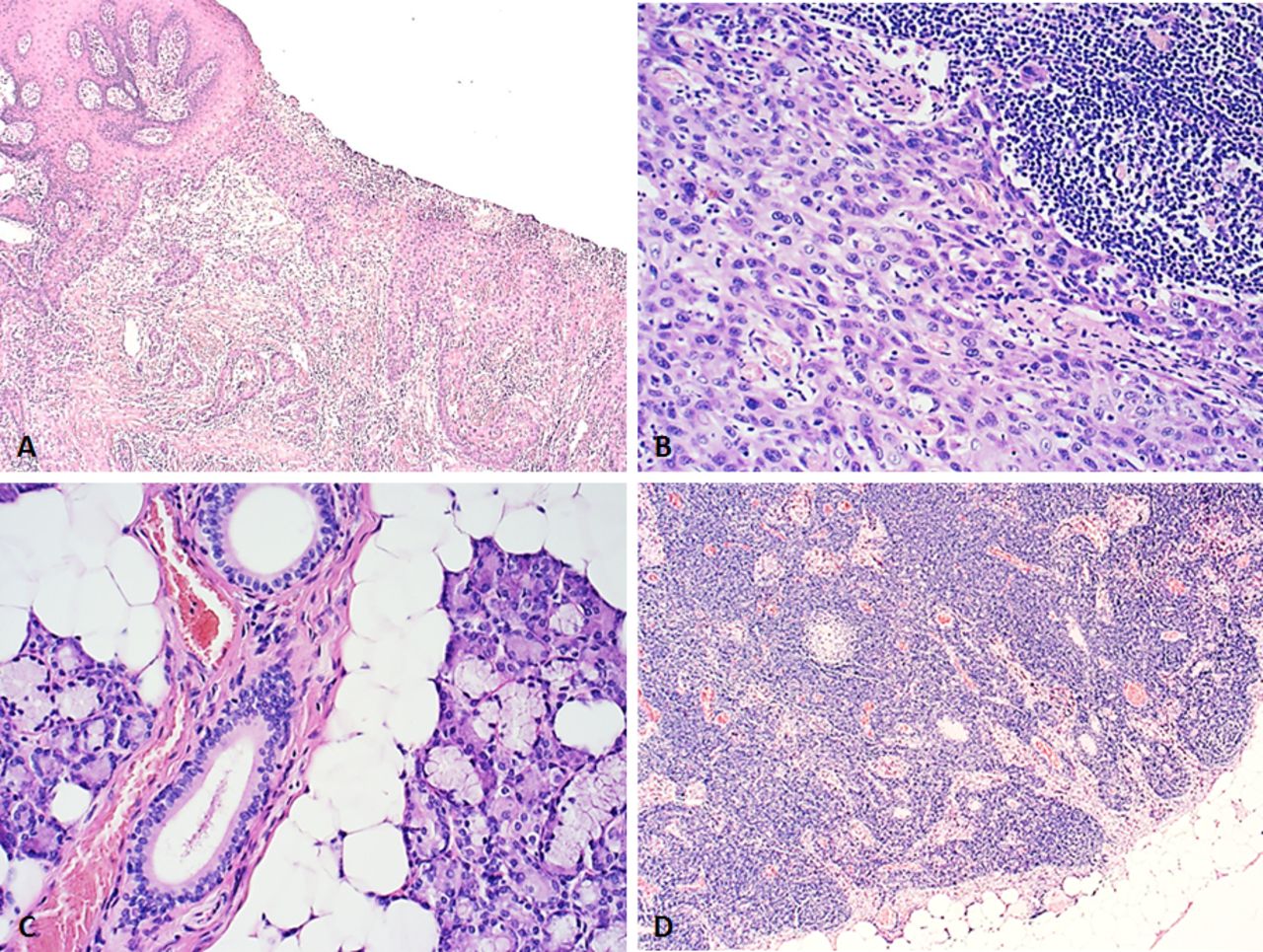
H&E-stained slides (micrographs) of surgical resection specimens selected for SARS-CoV-2 test analysis: ulcerated, poorly differentiated squamous cell carcinoma of the tongue (A, original magnification 100×); lymph node metastasis of squamous cell carcinoma (B, original magnification 250×); submandibular salivary gland with no signs of inflammation (C, original magnification 250×); and cervical lymph node with sinus histiocytosis (D, original magnification 100×). SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.

Real-time PCR curves from SARS-CoV-2 test run 1. Only sample 5 (tongue squamous cell carcinoma, pink) and positive control (pos, black) showed an amplification curve or cycle threshold value for COVID-19 below 45 cycles (left panel). All samples had positive internal control but one bronchoalveolar lavage (sample 8, orange; right panel). SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Real-time PCR curves from SARS-CoV-2 test run 2. Only sample 10 (submandibular gland, red) and positive control (pc, black) showed an amplification curve or cycle threshold value for COVID-19 below 45 cycles (left panel). All samples had positive internal control (right panel). SARS-CoV-2, severe acute respiratory syndrome coronavirus 2.
SARS-CoV-2 test run 1 showing positive result in the sample of tongue squamous cell carcinoma
SARS-CoV-2 test run 2 showing positive result in the sample of submandibular gland
Discussion
Here, we demonstrated that SARS-CoV-2 strain RNA can be detected in FFPE samples using rapid RT-PCR-based assays. To our knowledge, this is the first report of COVID-19 virus identification in routine histopathological specimens. Recently, Tian et al 8 described the pathological characteristics of COVID-19 pneumonia. At that time the lack of robust test for FFPE samples prevented the authors from confirming the presence of virus in lung specimens. In this study, we used an in vitro diagnostic qualitative SARS-CoV-2 test, based on RT-PCR technology. Indeed, the use of RT-PCR for virus detection in FFPE samples has a long history. Viral RNA has been detected on histological samples during the epidemics of the Rift Valley fever virus,9 Marburg and Ebola virus,10 and Zika virus.11 In 1997 using RT-PCR technologies, Taubenberger and colleagues12 were able to identify influenza genes in lung specimens from autopsies of individuals who died during the 1918 H1N1 virus influenza pandemic (‘Spanish flu’).13 The effort of these archeovirology studies was fundamental to understanding the past (and the new) pandemics. Moreover, they highlighted the robustness of RT-PCR methods for the detection of viral RNA even in old FFPE samples. In this study, RT-PCR technologies provided a robust and rapid method of detecting SARS-CoV-2 strain RNA in FFPE surgical resection specimens.
SARS-CoV-2 strain RNA was identified in the ulcerated squamous cell lesion of the tongue. Oral cavity mucosae are well-known sources of droplets and aerosols containing micro-organisms from infected individuals.14 SARS-CoV-2 strain RNA was also found in histologically normal submandibular gland with no evidence of inflammation. As recently reported, the virus was consistently detected in saliva from patients with COVID-19 infection.15 However, it is still unknown whether salivary glands represent passive reservoirs of the virus or are actively colonised from the oral cavity. Salivary glands are target of other RNA virus, including mumps and rabies. Moreover, an influenza virus-related non-mumps parotitis was also reported in USA and Argentina.16 Although we analysed a specimen resected during the incubation period of the disease, our preliminary findings may be a source of new information about the COVID-19 pathology. Unfortunately, we were unable to demonstrate whether the virus is able to colonise neoplastic cells or which cell type in the salivary gland. Moreover, we could not quantify the tissue viral load and sequence viral RNA. The implementation of ad hoc in situ assay and the improvement in the quantitative high-throughput SARS-CoV-2 RNA sequencing will be important to clarify these points.
The absence of SARS-CoV-2 RNA in cervical lymph node sample and in samples from patients without COVID-19 was consistent with the known virus transmission and body spread. Nevertheless, pathologists, laboratory technicians and molecular biologists need to be aware and properly equipped while handling potentially infective fresh or frozen material, particularly specimens from the oral cavity, respiratory tract and intestine. In this pandemic situation, reduction of intraoperative consultation frozen section, proper formalin fixation, reduction of diagnostic procedures according to priority criteria and the implementation of digital pathology for remote working may represent effective strategies to reduce the risk among healthcare workers in a pathology laboratory.17–20
Emerging and re-emerging infectious diseases need an interlaboratory collaboration. Diagnosis of COVID-19 infection relies on clinical, radiological and virology parameters. Pathologists may provide important information about the pathogenesis of this new and protean infection: SARS-CoV-2.
Acknowledgments
We thank the patient/s and all colleagues and healthcare workers fighting COVID-19. We acknowledge the laboratory technicians of the Division of Pathology (European Institute of Oncology IRCCS, Milan, Italy) for sample collection and processing. This work was partially supported by the Italian Ministry of Health with Ricerca Corrente and 5x1000 funds.
Footnotes
Handling editor Runjan Chetty.
Contributors All authors made substantial contributions to this study and this manuscript. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Obtained.
Ethics approval The study was conducted in accordance with the 1964 Helsinki Declaration and later amendments.
Provenance and peer review Not commissioned; internally peer reviewed.