Article Text

Abstract
Aims Hospitalised patients with COVID-19 have a variable incidence of acute kidney injury (AKI) according to studies from different nationalities. The present systematic review and meta-analysis describes the incidence of AKI, need for renal replacement therapy (RRT) and mortality among patients with COVID-19-associated AKI.
Methods We systematically searched electronic database PubMed, SCOPUS and Web of Science to identify English articles published until 25 May 2020. In case of significant heterogeneity, the meta-analyses were conducted assuming a random-effects model.
Results From 746 screened publications, we selected 21 observational studies with 15 536 patients with COVID-19 for random-effects model meta-analyses. The overall incidence of AKI was 12.3% (95% CI 7.3% to 20.0%) and 77% of patients with AKI were critically ill (95% CI 58.9% to 89.0%). The mortality among patients with AKI was 67% (95% CI 39.8% to 86.2%) and the risk of death was 13 times higher compared with patients without AKI (OR=13.3; 95% CI 6.1 to 29.2). Patients with COVID-19-associated AKI needed for RRT in 23.4% of cases (95% CI 12.6% to 39.4%) and those cases had high mortality (89%–100%).
Conclusion The present study evidenced an incidence of COVID-19-associated AKI higher than previous meta-analysis. The majority of patients affected by AKI were critically ill and mortality rate among AKI cases was high. Thus, it is extremely important for health systems to be aware about the impact of AKI on patients’ outcomes in order to establish proper screening, prevention of additional damage to the kidneys and adequate renal support when needed.
- kidney
- viruses
- death
- epidemiology
Data availability statement
All data relevant to the study are included in the article.
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
Introduction
Seven months after the first reported case of COVID-19 in Wuhan, China in December 2019, we face >10 million cases and a half million deaths worldwide in 216 countries.1 SARS-CoV-2 causes an interstitial and alveolar pneumonia, but in nearly 26% of patients it can lead to a severe disease, with multiple organ failure.2–5
It has been shown that nucleocapsid protein antigen, virions and virus-like particles were present in proximal tubular cells cytoplasm of postmortem patients.6 7 Nevertheless, recent studies of native kidney biopsy in patients with acute kidney injury (AKI) with or without proteinuria and/or haematuria failed to identify viral presence in the kidney tissue by immunohistochemistry and electron microscopy.8 9 Light microscopy of patients with COVID-19 showed mainly acute diffuse tubular injury, associated with a lower frequency of other findings such as erythrocyte aggregates obstructing peritubular capillary lumens and endothelium injury.6 7
The incidence of AKI varies according to studies among different populations ranging from 0.9% to 29.0% and it is associated with a high mortality, especially if in combination of respiratory failure.10–13 Besides the direct impact of SARS-CoV2 virulence, other renal insults such as volume depletion, hypoxia, cytokine storm, drug nephrotoxicity and co-infection with other pathogens might play a role in the AKI of critically ill patients. This has posed pressure to healthcare systems due to a shortage of dialysis staff, equipment and consumables throughout the world.
This study aims to systematically review the incidence of COVID-19-associated AKI, its related risks factors, need for renal replacement therapy (RRT) among patients with AKI and mortality according to current illness severity. Awareness of the real numbers is paramount because it will help prevent avoidable AKI cases, promote prompt recognition if it already occurred and provide adequate management of the burden or escalation of care.
Materials and methods
Study protocol and eligibility criteria
This study was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses and Meta-analysis Of Observational Studies in Epidemiology guidelines.14 15 PICOS criteria were defined for frequency analysis studies: patients—adult patients diagnosed with COVID-19; outcomes—disease severity, survival, death and RRT; studies—observational studies, published until 25 May 2020. For mortality analysis studies: patients—adult patients diagnosed with COVID-19; intervention/exposure—hospitalisation for COVID-19; controls—adult patients who did not present AKI; outcomes—disease severity, survival, death and RRT; studies—observational studies, published until 25 May 2020.
Studies were included if they reported (1) COVID-19 diagnostic method, and (2) AKI identification and classification. The exclusion criteria included: (1) studies with pregnant and postpartum patients; (2) studies with end-stage renal disease and/or kidney transplant patients; (3) case reports; (4) studies without AKI diagnostic according to Kidney Disease Improving Global Outcomes (KDIGO) clinical guidelines for AKI or KDIGO expanded criteria16 17 and (5) studies written in languages other than English.
Search strategy and data selection
We systematically searched PubMed, SCOPUS and Web of Science databases with the search terms ‘COVID-19’ OR ‘SARS-CoV-2’ OR ‘Coronavirus 2019’ OR ‘2019-nCoV’ AND ‘Acute Kidney Injury’ OR ‘Kidney’ OR ‘Nephrology’ OR ‘Renal Disease’ OR ‘Clinical Characteristics’ OR ‘Clinical Features’. Two investigators worked independently to select which studies should be included, and the disagreement was resolved by consensus or by a third investigator.
Data were extracted from the following information from each study: (1) population characteristics (age, sex, comorbidities and number of patients with and without AKI), (2) study characteristics (type of study design, countries where studies were conducted, number of patients, definition and method of AKI ascertainment) and (3) outcomes (severe cases, critically ill patients, need for RRT and no-survivors patients).
Quality assessment
The studies were qualitatively evaluated according to the National Institutes of Health criteria by two investigators who worked independently.18 The choice was based on (1) clear specification and definition of study population; (2) uniform application of prespecified inclusion and exclusion criteria for to all participants and (3) outcome measures clearly defined, valid, reliable and implemented consistently across all study participants. Again, any disagreements were resolved by consensus or by a third investigator mediation.
Meta-analysis and meta-regression
We analysed the following outcomes: (1) incidence of AKI among patients with COVID-19; (2) critically ill cases among all AKI cases; (3) mortality among AKI cases; (4) incidence of RRT among patients with AKI and (5) risk of death of patients with AKI compared with patients without AKI. We considered severe cases, all patents requiring ICU support or patients who were classified as critical or severe in selected studies.
The heterogeneity between studies sample sizes was expressed through I2 measure and τ2 statistic (estimated via maximum-likelihood). A Cochran’s Q test with k–1 df (in which k is the number of studies included) and with significance level α=0.10 (exclusively for this test) was conducted to assess if heterogeneity was significantly different from zero. If so, the heterogeneity was classified according to the observed I2 measure: ≤25%, between 25% and 50%, between 50% and 75% and between 75% and 100% were considered as low, moderate, high and very high heterogeneity, respectively. In case of significant heterogeneity, the meta-analyses were conducted assuming a random-effects model with the Hartung-Knapp adjustment.19 20
Sensitivity analysis was performed by repeating prevalence estimation following the detection and removal of outliers (studies with extreme—too low or too high—sample sizes in relation to the remaining studies) or studies with potential overlapping of participants. The percentage difference of the estimations before and after outliers being removed were calculated to assess if our estimations were robust.
Meta-regressions were performed, each one corresponding to one meta-analysis. The independent variables were: study location (China, Poland or the USA), study design (case series, prospective or retrospective cohorts), study setting (single or multicentre), median age of patients in years, proportion of males patients in the sample size and proportion of patients with certain comorbidities, namely hypertension, other cardiovascular diseases, diabetes, chronic pulmonary disease, chronic kidney disease (CKD) and cancer. These comorbidities were analysed because they were reported in at least 30% of the selected studies.
The meta-analysis, outlier detections, sensitivity analysis and meta-regressions were performed using meta for R software, V.4.0.1 (R Core Team, Vienna, Austria).21 22
Results
Screening and selection of articles for this systematic review are represented as a flow diagram (figure 1). The main characteristics and outcomes of the 21 included studies (15 536 patients) are summarised in tables 1 and 2.

Flow diagram of the selection process to identify the studies included in the meta-analysis. AKI, acute kidney injury.
Characteristics of the 21 included studies with patients with COVID-19
Outcomes of the 21 included studies with patients with COVID-19
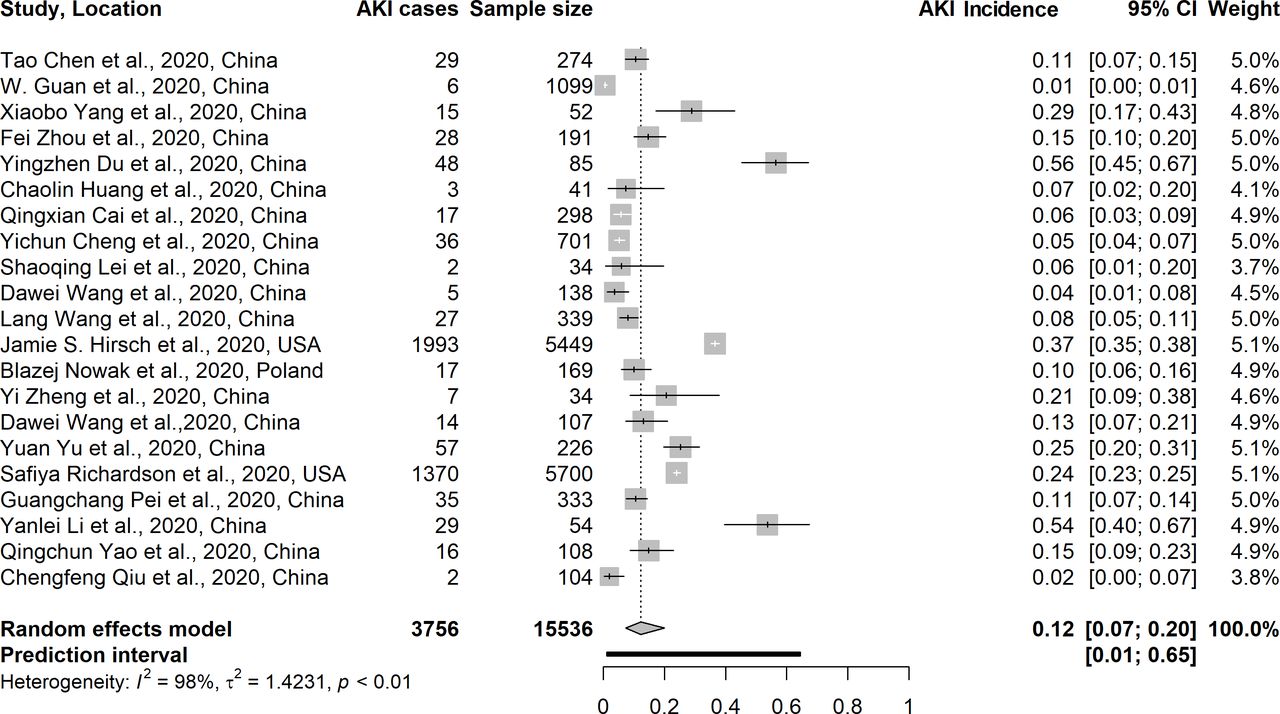
The meta-analysis showed an incidence of AKI associated with COVID-19 of 12.3% (95% CI=7.3% to 20.0%; Cochran’s Q=839.6 with 20 df, p<0.001; I2=97.6% and τ2=1.42). This meta-analysis included all selected studies (k=21) (figure 2).13 17 23–41 We detected six outliers among those: Guan et al 36; Du et al 39; Cheng et al 24; Hirsch et al 13; Richardson et al 32 and Li et al.33 Repeating the meta-analysis without those, we obtained an estimation of 11.0% (95% CI=7.6% to 15.7%; Cochran’s Q=86.0 with 14 df; p<0.001; I2=83.7% and τ2=0.35), resulting in a percentage variation of about 10%, which indicates that our meta-analysis was deemed robust against outliers or potential overlapping of individual participants.

Forest plot for the incidence of acute kidney injury (AKI) cases in patients with COVID-19.
Among all AKI cases, we found that 77.3% were critically ill patients (95% CI 58.9% to 89.0%; Cochran’s Q=32.7 with 9 df; p=0.002; I2=72.5% and τ2=0.80) (figure 3). We detected a single outlier in this subset: Hirsch et al.13 Repeating the meta-analysis without this study, we obtained an estimation of 80.6% (95% CI 63.1% to 90.9%; Cochran’s Q=13.5 with 8 df; p=0.096; I2=40.6% and τ2=0.45), resulting in a low percentual variation of about 4%. Thus, the analysis remained with all studies included.

Forest plot for the incidence of severe cases among patients with acute kidney injury (AKI) associated with COVID-19.
RRT was needed in 23.4% of AKI cases (95% CI 12.6% to 39.4%; Cochran’s Q=140.6 with 13 df; p<0.001; I2=90.8% and τ2=1.01) (figure 4). We detected a single outlier among this subset: Richardson et al.32 Repeating the meta-analysis without this study, we obtained an estimation of 26.4% (95% CI 14.7% to 42.8%; Cochran’s Q=66.6 with 12 df; p<0.001; I2=82% and τ2=0.72), resulting in a percentage variation of 13%. As it was not significant, our original meta-analysis was deemed robust.
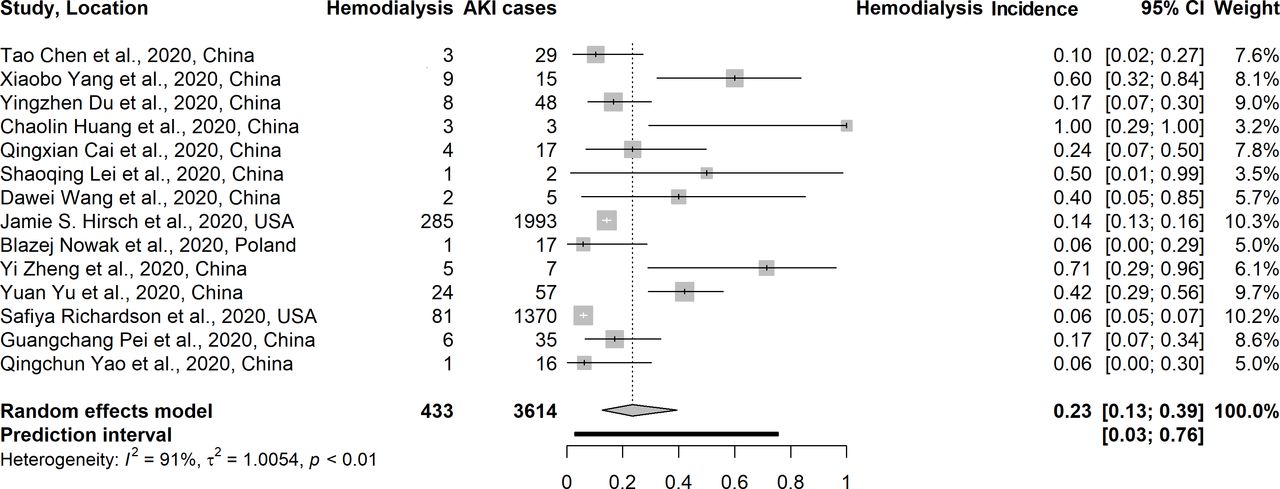
Forest plot for the incidence of renal replacement therapy among patients with acute kidney injury (AKI) associated with COVID-19.
The overall mortality among AKI cases was 67.0% (95% CI 39.8% to 86.2%, Cochran’s Q=111.8 with 9 df; p<0.001; I2=91.9% and τ2=1.55) (figure 5). We detected two outliers among this subset: Hirsch et al and Richardson et al.13 32 Repeating the meta-analysis without those, we obtained an estimation of 75.7% (95% CI 49.1% to 91.0%; Cochran’s Q=23.3 with 7 df; p=0.002; I2=70.0% and τ2=0.98), resulting in a percentage variation of 13%. Again, the variation was considered small and these studies were included in the meta-analysis.

Forest plot for mortality associated with acute kidney injury (AKI) in patients with COVID-19.
The meta-analysis of AKI-associated mortality risk showed that patients with AKI had 13 times more risk of dying when compared with patients without AKI (OR=13.3. 95% CI 6.1 to 29.2; Cochran’s Q=21.2 with 7 df; p=0.004; I2=66.9% and τ2=0.27) (figure 6). No outliers were detected in this analysis.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot for mortality risk among patients with acute kidney injury (AKI) associated with COVID-19.
All multivariate meta-regression analyses did not reveal association between any of the evaluated variables, namely hypertension, chronic cardiovascular disease, diabetes, chronic pulmonary disease, CKD and cancer with the outcomes (table 3). However, older age was associated with increased prevalence of AKI cases among coronavirus-infected patients only in the univariate meta-regression analysis (p=0.005).
Meta-regression modelling risk of COVID-19-associated AKI
Discussion
Our meta-analysis analysed 21 observational studies about clinical characteristics and outcomes of 15 739 patients with COVID-19. We found an AKI incidence of 12.3% in hospitalised patients, higher than the incidence calculated in previous meta-analysis.42–44 Conversely, other studies have shown a lower incidence of AKI. Ng et al evaluated nine studies with a total of 2702 patients and evidenced a pooled incidence rate of AKI of 3% (95% CI 1.0 to 7.0).44 Similarly, Yang et al found an AKI incidence of 4.5% (95% CI 3.0 to 6.0) in a meta-analysis of 17 studies with 3968 patients.42 Another meta-analysis including 20 studies and 6945 patients from China, Italy, the UK and the USA showed an AKI incidence of 8.9% (95% CI 4.6 to 14.5).43
The higher incidence of AKI in our meta-analysis can be explained by the heterogeneity of the evaluated populations. In previous meta-analysis, >95% of patients were Chinese42 44; whereas in the present study <30% of patients were from China and around 70% of patients were from the USA, with similar proportion of black, white and other races. Studies from the USA had higher rates of AKI risk factors, such as hypertension, diabetes, older age and more severe cases with respiratory failure and need of vasopressors, when compared with Chinese studies.13 32 Moreover, it has been shown that there is some variability in genetic expression of the ACE2 that may partially explain the differences in susceptibility or severity to COVID-19 among races (eg, between Chinese and white Americans), but not between sex.45 The ACE2 is mostly expressed in the kidneys and in the gut, and to a lesser extent in the pneumocytes 2, in the lungs and in the peripheral blood; it cleaves peptides and the ACE2 receptor is used by SARS-CoV2 to enter the cells.46 The SARS-CoV2 also targets the ACE2 receptor in the CD4 +and CD8+ T cells, leading to interleukins release, cell death and lymphopenia, which is a marker of aggressive disease.46
Severity of COVID-19 is closely associated with AKI.24 42 In our meta-analysis, 77% of patients with AKI were critically ill and the incidence of AKI among critically ill patients ranged from 8% to 76% among the studies. Yang et al showed an AKI incidence in critically ill cases of 36% (95% CI 14.6% to 58.5%), higher than an AKI incidence of 2.8% (95% CI 1.4 to 4.2) in severe cases and 1.3% (95% CI 0.2% to 2.4%) in mild to moderate cases. In addition, the risk of AKI was 1.8 times greater in severe patients, compared with non-severe patients (95% CI 1.21 to 2.41, p<0.010).42 Temporally, severe COVID-19-associated AKI usually occurs close to respiratory failure and mechanic ventilation. The majority of patients under RRT are mechanically ventilated, which denotes the important cross-talking between these organs.13 The cytokine storm observed in severe cases is also in a temporal proximity to the respiratory failure and contributes to the prothrombotic milieu that reduces vital organs perfusion.
Urinalysis in early AKI cases showed that around 40% of cases had ≥2+ proteinuria and >5 red blood cells per high-power field, denoting parenchymal damage rather than a reversible acute kidney dysfunction.13 Analysis of kidney specimens from autopsy of patients with COVID-19-associated AKI showed predominant tubular lesion, with vacuole degeneration, loss of luminal brush border and severe acute tubular necrosis, associated with a prominent expression of ACE2 in proximal tubular cell. In addition, immunohistochemistry detected SARS-COV-2 antigen in kidney tubules and virus particles were detected in the renal tubular epithelium and podocytes by transmission electronic microscopy.6 7 In contrast to these findings, subsequent studies evaluated kidney biopsies of patients with COVID-19-associated AKI with or without proteinuria and/or haematuria and found no evidence of SARS-COV-2 by immunohistochemical staining and electronmicroscopy ultrastructural examination.8 9 Rossi et al also evaluated viral genetic material in renal tissue, urine and serum by real-time PCR and did not find SARS-COV-2 RNA.47
In addition to the tubular lesion, erythrocyte aggregates obstructing peritubular capillary lumens and endothelium activation were described in optic microscopy revealing the prothrombotic status that is often observed in severe cases of COVID-19.6 The COVID-19-related immunothrombosis is due to the macrophage activation and cytokine storm leading to elevated C reactive protein, ferritin and D-dimer levels, which are correlated to worse outcomes.48 49 Thus, the probable mechanisms of COVID-19-associated AKI is the tubular lesion caused by hypoxia, hypotension, cytokine storm and hypercoagulable state usually seen in critically ill patients with concomitant multiple organs failure.
Besides age, our meta-regression could not identify significant risk factors for AKI. Most of the selected studies were descriptive, did not focus AKI as a main outcome or did not have multivariable analysis in this regard. However, the second largest study from the meta-analysis, with >5000 patients, found that older age, black ethnicity, hypertension, diabetes and cardiovascular disease were risk factors for AKI in the adjusted analysis.13
Patients with AKI associated with COVID-19 had higher risk of death compared with non-AKI.24 42 In our meta-analysis, the overall mortality among patients with AKI was 67%. Moreover, patients with AKI had 13 times higher risk of dying when compared with patients without AKI associated with COVID-19. Similarly, it has been shown that the risk increases according to AKI severity (AKI stage 1=1.90; AKI stage 2=3.51; AKI stage 3=4.38).24 Moreover, all AKI stages were independent risk factors for in-hospital death, even after adjusting for age, sex, disease severity, comorbidity and leucocyte count.24 A meta-analysis comparing non-survivors with survivors showed a higher incidence of AKI (52.9% vs 0.7%) and RRT (15.6% vs 0.4%) among non-survivors. In addition, RRT was indicated in 5.6% of severe patients and 0.4% of non-severe patients.42 In our study, RRT was required in 23% of patients with AKI and mortality among RRT patients ranged from 89% to 100% between selected studies.17 28 32 35 37 39
The main limitation of this study is the retrospective design of most selected studies. Some studies did not analyse covariates or risk factors for AKI; and the majority had no data about patients’ baseline glomerular filtration rate or CKD history, which are important predictors of AKI occurrence. Additionally, most patients were from the USA and China, and a small amount from Poland, which does not preclude a global sample. The heterogeneity between studies was high, therefore, all analyses were interpreted according to a random-effects model.
In conclusion, despite SARS-CoV-2 being a predominantly respiratory virus, it can often damage the kidneys, probably by hypoxia, hypotension, cytokine storm and hypercoagulable state found in critically ill patients. Our findings showed a higher incidence of AKI in hospitalised patients with COVID-19 compared with previous meta-analysis; a close association of AKI with disease severity and high mortality among all patients with AKI, especially for patients on RRT. Thus, healthcare systems should be aware of kidney impairment in COVID-19 by screening and monitoring the cases and be prepared to deliver prompt renal care for those who need it.
Take home messages
Meta-analysis of 21 studies with 15 536 patients with COVID-19.
Incidence of COVID-19-associated acute kidney injury (AKI) was 12.3% and 77% of patients with AKI were critically ill.
The risk of death was 13 times higher in patients with COVID-19-associated AKI compared with patients without AKI.
High mortality among renal replacement therapy patients (89%–100%).
Data availability statement
All data relevant to the study are included in the article.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to thank the LIKA-UFPE team for their scientific contribution.
References
Footnotes
Handling editor Tahir S Pillay.
CBO and CADL contributed equally.
Contributors CBO and CADL contributed equally to this study. CBO, CADL, GV and PSG designed the study, had full access to all results and take responsibility for the accuracy of the data analysis. CBO and CADL performed the articles search and selection. CBO, CADL and GV interpreted the data and drafted the manuscript. AVCC did the statics analysis. PSG and AVCC revised the manuscript. PSG conceived the idea and supervised the study. All authors read and approved the final manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.