Article Text

Abstract
Objective Due to the burden of coronary heart disease (CHD), the monitoring of CHD trends is required. This study sought to examine the acute myocardial infarction (AMI) trends in attack and mortality rates, and in 28-day case-fatality, in six European populations during 1985–2010.
Methods Data consisted of 78 128 AMI events included in eight population-based registries from Finland (several populations), Italy (Brianza and Varese), Germany (Augsburg), France (Haute-Garonne), Spain (Girona) and Estonia (Tallinn). AMI event rates and case-fatality trends were analysed using the annual percentage change (APC) obtained by negative binomial and joinpoint regression.
Results AMI attack and mortality rates decreased in most populations. Finland experienced the steepest decline in attack rates (APC=−4.4% (95% CI −5.1 to −2.9) in men; −4.0% (−5.1 to −2.8), in women). Total-hospital and inhospital case-fatality decreased in all populations except in Tallinn. The steepest decline in total case-fatality occurred in Spain (−3.8% (−5.3 to −2.4) in men; −5.1% (−6.9 to −3.3) in women). Prehospital case-fatality trends differed significantly by population and sex. The trends for all included populations showed a significant decline in AMI event rates and case-fatality, in both sexes and all age groups. However, in women aged 65–74 years, a significant increase in total case-fatality occurred in 2005–2010 (4.7% (0.7 to 8.8)).
Conclusions AMI event rates and inhospital case-fatality declined in 1985–2010 in almost all populations analysed. Prehospital case-fatality declined only in certain population groups, showing differences by sex. These results highlight the need of specific strategies in AMI prevention for certain groups and populations.
Statistics from Altmetric.com
Introduction
Despite reductions in the prevalence of cardiovascular (CV) risk factors and improvements in therapeutic management, coronary heart disease (CHD) remains the leading cause of death worldwide. In Europe, CHD causes almost 1.8 million deaths yearly and is a major contributor to morbidity.1 ,2 Given the burden of CHD and the variation in CV risk factor prevalence and in patient management in Europe,1–4 it is essential to monitor CHD mortality and morbidity trends in this region to reduce disparities between populations.
CHD mortality trends are regularly released in Europe.1 ,2 However, CHD morbidity trends are mostly limited to the results from independent registries.1 When analysing CHD trends, it is of critical importance to perform multinational studies to ensure that the same methods are used, yielding comparable estimates.
The last multinational comparison of long-term CHD trends in different European populations was published by the WHO-MONICA (WHO-Multinational MONItoring of trends and determinants in CArdiovascular disease) investigators in 1999.5 Recently, short-term trends of acute myocardial infarction (AMI) inhospital case-fatality were published for a number of European countries,2 but these trends were not stratified by sex or age group. In addition, data on CHD attack rates, on long-term trends of case-fatality, and the separate analysis of out-of-hospital and inhospital case-fatality are lacking in Europe.
To fill this gap, investigators who have maintained population-based AMI registries following the WHO-MONICA methodology designed the AMITIE (Acute Myocardial Infarction Trends In Europe) Study. The AMITIE Study aims at analysing the trends on AMI attack and mortality rates and on 28-day case-fatality in six European populations during 1985–2010. This study also aims at comparing trend estimates by population, sex and age groups.
Methods
Study population
AMI data from 1985 to 2010 were gathered from the following population-based registries: FINAMI6 (population-based MI registry in Finland), FINMONICA (MONICA registry in Finland),7 MONICA-Brianza and CAMUNI (CArdiovascular Monitoring Unit in Northern Italy; Brianza area/Varese province, Italy),8 MONICA-KORA (KOoperative Gesundheitsforschung in der Region Augsburg, Cooperative Health Research in the Augsburg Region; Augsburg, Germany),9 MONICA-Toulouse (Haute-Garonne department, France),10 REGICOR (REgistre GIroní del COR, Girona Heart Registry; Girona province, Spain)11 and Tallinn AMI Registry (Tallinn, Estonia).12 All registries contributed at least 20 years of data from the 1985–2010 period, except MONICA-Brianza and CAMUNI that contributed 16 years, and Tallinn that contributed 10 years. The exact years of data collection in each registry are presented in the online supplementary table S1, together with the main characteristics of the registries. Each component registry was approved by its local ethics committee.
Included events
First and recurrent AMI cases were included, classified according to the WHO-MONICA Project (http://www.thl.fi/publications/monica/manual/index.htm) and to American Heart Association/European Society of Cardiology (AHA/ESC) algorithm.13 Using the WHO-MONICA definition, AMI total events included non-fatal and fatal definite AMI (NF1+F1), fatal possible AMI or coronary death (F2) and unclassifiable deaths (F9).
AMI indicators
Event rates (attack and mortality rates) and case-fatality (total, inhospital and prehospital) were calculated for each population, for the age group 35–64 years, by year and sex. Event rates and case-fatality were also calculated for all populations together, for the age groups 35–64, 35–74 and 65–74 years, by aggregating AMI events and population estimates from all included populations. All-population event rates and case-fatality were calculated as unweighted estimates. Sensitivity analysis with weighted event rates, adjusting each population's event rate for the country's population, showed similar trends (table 1 and see online supplementary table S2).
Annual percentage change (APC) in AMI attack and mortality rates and in 28-day case-fatality, in 1985–2010, by population and age group
Event rates were age standardised using the 1976 European Standard Population (ESP). The 1976 ESP was preferred to allow direct comparison with previous publications and because the data used in this study predate 2013 ESP. Case-fatality was standardised using weights derived from the distribution of AMI events by age group (4, 13, 30 and 53 for the age groups 35–44, 45–54, 55–64 and 65–74 years, respectively). These estimates were similar to the weights derived from the age distribution of patients with AMI and stroke in the WHO-MONICA Project,5 as shown in sensitivity analysis (see online supplementary table S3).
Age-standardised event rates and case-fatality were calculated for the WHO-MONICA definition. In Finland and in Haute-Garonne-France, where AMI cases were classified according to the AHA/ESC definition only from the late 1990s onwards, the number of events was weighted with sex-specific correction coefficients.14 For Finland, coefficients were obtained from the literature: 0.913 for men and 0.821 for women.14 As in Haute-Garonne-France, both definitions were not used simultaneously at any time period, coefficients were computed using data from Girona-Spain, which has a similar AMI incidence rate. Coefficients were obtained as the ratio of events diagnosed with the WHO-MONICA definition to the number of events diagnosed with the AHA/ESC definition as described.14 The coefficients observed in Girona-Spain were 0.890 for men and 0.833 women. Correction was not applied to mortality rates and case-fatality, as the effect of the AHA/ESC definition in these AMI indicators is negligible.14
Statistical analysis
Trends in event rates and case-fatality were analysed using negative binomial regression, because the restriction implicit in the Poisson regression (conditional mean=conditional variance) did not hold for most of the populations. Year was the continuous predictor variable. The annual percentage change (APC) was calculated as (regression coefficient of year)×100. The 95% CI of the APC was calculated using the SE of the regression coefficient of year.
Trends were further analysed by joinpoint regression to detect significant changes in trend, using the Joinpoint Regression Program (National Cancer Institute Bethesda, Maryland, USA, V.4.0.4). A maximum of two joinpoints was allowed for estimation, and the Bayesian Information Criterion was used to select the model that best fitted the data with the smallest number of joinpoints. The year of the joinpoints and the APCs with 95% CIs were obtained for each trend period.
All-population trends were represented with smoothed curves obtained by nonparametric regression using the LOESS function from R (LOcally wEighted Scatterplot Smoothing). Sex and age group differences in all-population trends were examined using the test for parallelism.
Statistical analysis, except for the joinpoint regression, was performed with R Statistical Package V.3.0.3.15 p values <0.05 were considered significant.
Results
Attack rate trends
In the population aged 35–64 years, the highest AMI attack rates were observed in Finland and in Tallinn-Estonia, and the lowest in Girona-Spain and in Haute-Garonne-France (figure 1A). Attack rates decreased significantly in 1985–2010 in all populations aged 35–64 years, except for men in Tallinn-Estonia and in Girona-Spain. In men from Girona-Spain, however, attack rates decreased significantly during 2001–2009 (see online supplementary table S4). The steepest annual declines were observed in Finland (APC=−4.4% in men and −4.0% in women), the population showing the highest absolute attack rates at the beginning of the analysed period (table 1 and figure 1A).

Trends in age-standardised acute myocardial infarction attack and mortality rates in six European populations during 1985–2010. (A) Attack rates in the included populations, 35–64 years; (B) mortality rates in the included populations, 35–64 years; (C) all-population attack and mortality rates, 35–64 years. (D) All-population attack and mortality rates, 65–74 years. Results are presented separately for men (left) and for women (right). Available period for each population: Finland (1985–2007), Tallinn-Estonia (1991–1997, 2003–2005), Augsburg-Germany (1985–2010), Haute-Garonne-France (1985–1993, 1997–2010), Brianza/Varese-Italy (1985–1994, 1997–1998, 2003–2004, 2007–2008) and Girona-Spain (1990–2009).
When all included populations were analysed together, attack rates were three times higher in the older age group (65–74 years) than in the younger age group (35–64 years; figure 1). Similarly, attack rates were almost 10 times higher in men than in women. The decline in attack rates was observed in both the younger and the older age groups being steeper in the latter (p<0.01; table 1). In the population aged 35–64 years, a constant decrease in attack rates was observed in men, while in women, two trend changes were detected and only the period 1998–2010 showed a significant decrease (tables 1 and 2, analysis by sex p<0.01).
Joinpoint analysis of all-populations trends on AMI attack and mortality rates and 28-day case-fatality in 1985–2010
Mortality rate trends
The highest absolute mortality rates were observed in Finland, in Tallinn-Estonia and in Augsburg-Germany, while the lowest were recorded in Girona-Spain and in Haute-Garonne-France (figure 1B). Mortality rates decreased significantly in 1985–2010 in all populations aged 35–64 years, except for men in Tallinn-Estonia. The steepest annual declines were observed in Finland (APC=−6.3%) and in Girona-Spain (APC=−7.3%), for men and women, respectively (table 1). In all populations except in men from Tallinn-Estonia and in women from Brianza/Varese-Italy, the decline in mortality rates was significant during the last 10 years analysed (table 1 and see online supplementary table S4).
Trends including the events from all populations showed that absolute mortality rates were much higher in the population aged 65–74 years than in the younger population, and that this difference was twice as high in women compared with that in men (figure 1). Regarding the mortality trends, a significant annual decrease in mortality rates was found in men and women, and in all age groups, especially in the population aged 65–74 years (APC=−6.3% in men and −6.9% in women; table 1 and figure 1). The steepest declines in mortality rates were observed after 1995 in all sex and age groups (table 2). In the population aged 65–74 years, AMI mortality trends differed by sex (p<0.05). While in men there was a decrease over time, in women, mortality rates decreased until 2004 to stabilise thereafter (table 2). In women, AMI mortality trends differed by age group (p<0.05). In women aged 35–64 years mortality rates only decreased in 1999–2010, while in women aged 65–74 years the pattern was the opposite (table 2).
Total 28-day case-fatality trends
In men, the highest case-fatality was recorded in Tallinn-Estonia, and the lowest in Girona-Spain and in Haute-Garonne-France (see online supplementary figure S1A). In women, case-fatality rates showed high year-to-year variability and the lowest case-fatality was recorded in Finland and in Girona-Spain. All populations aged 35–64 years showed significantly decreasing trends in total 28-day case-fatality in 1985–2010, except for Tallinn-Estonia (table 1). In addition, total case-fatality decreased during the last 5 years analysed in all populations (table 1 and see online supplementary table S4). The steepest annual declines for the whole period were observed in Girona-Spain in both men and women (APC=−3.8% and −5.1%, respectively; table 1).
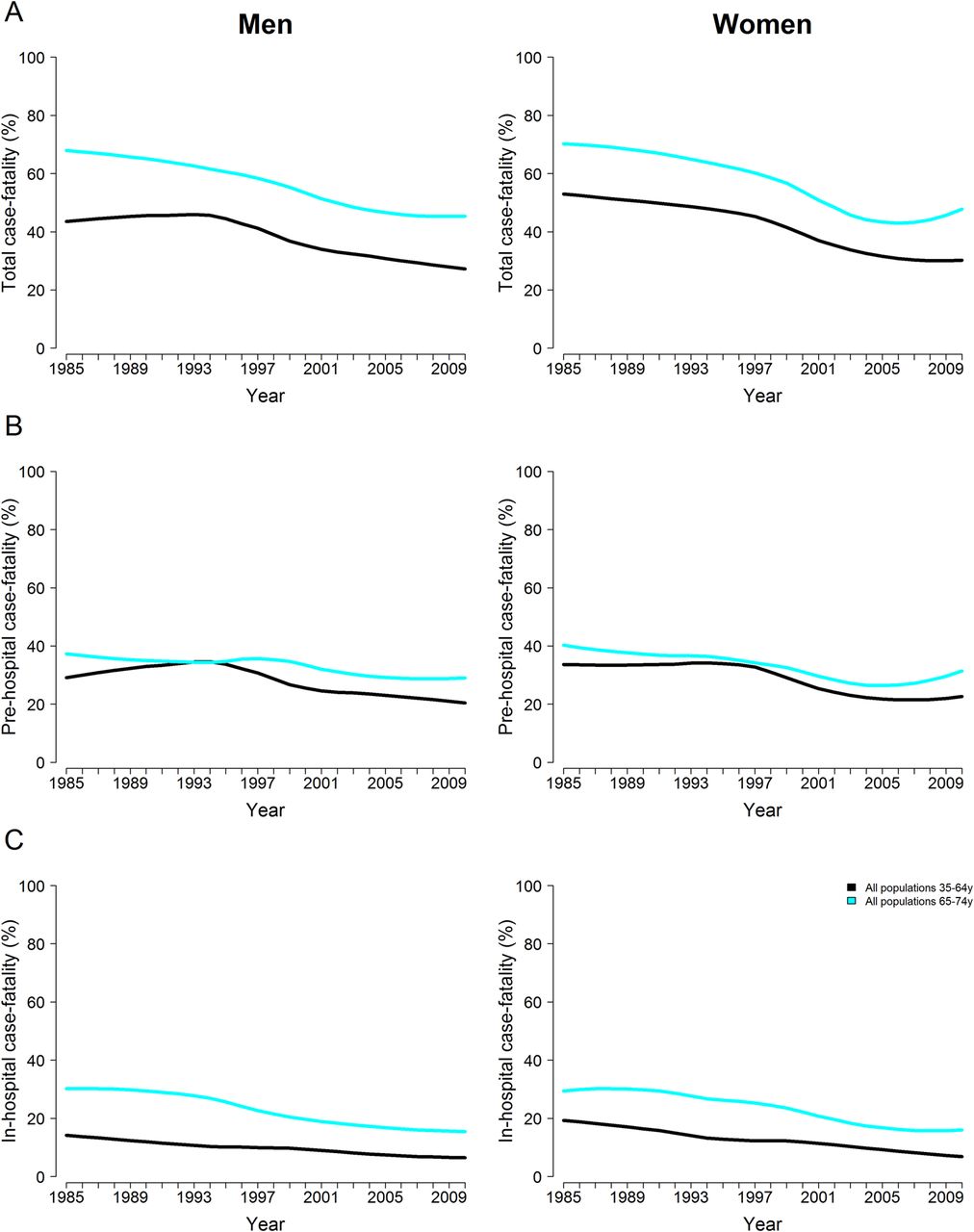
When all included populations were analysed together, it was observed that total case-fatality was 20% higher in the population aged 65–74 years than in the younger population, and 10% higher in men than in women (figure 2A). A decline in total case-fatality was observed in both sexes and in all age groups (table 1) during 1985–2010. Total case-fatality trends differed by sex in the population aged 65–74 years (p<0.01). While in men total case-fatality decreased continuously, in women, it decreased until 2005 but increased in 2005–2010 (APC=4.7%; table 2 and figure 2A).
{kind=link}
{kind=link}
All-population trends in age-standardised acute myocardial infarction total (A), prehospital (B) and inhospital 28-day case-fatality (C) during 1985–2010. Results are presented separately for men (left) and for women (right). Individual trends of the included populations are presented in the online supplementary figure S1.
Prehospital 28-day case-fatality trends
The lowest prehospital case-fatality was recorded in Girona-Spain and in Haute-Garonne-France in men and in Finland and in Girona-Spain in women (see online supplementary figure S1B). The highest prehospital case-fatality was observed in Tallinn-Estonia. Prehospital case-fatality trends differed by sex in the individual populations aged 35–64 years. In men, only Finland, Haute-Garonne-France and Girona-Spain showed significantly decreasing trends in 1985–2010, with the steepest annual decline occurring in Haute-Garonne-France (APC=−3.5%). In women, all populations except Tallinn-Estonia and Finland showed significantly decreasing trends, and the steepest annual decline was observed in Girona-Spain (APC=−5.6%; table 1). Although prehospital case-fatality did not decrease across the whole study period in a number of populations, it is noteworthy that at least in the last 5 years analysed a significant decrease occurred in all populations except in men from Augsburg-Germany and Brianza/Varese-Italy and in women from Tallinn-Estonia (table 1 and see online supplementary table S4).
Prehospital case-fatality including the events from all populations showed that the difference in the crude rate between age groups and sexes was only around 5%, being higher in the population aged 65–74 years and in women (figure 2B). Long-term trends showed a significant decrease in 1985–2010, especially in the population aged 35–64 years (APC=−1.8% in men and −2.2% in women; table 1).
Inhospital 28-day case-fatality trends
The highest inhospital case-fatality was recorded in Augsburg-Germany and the lowest in Tallinn-Estonia and in South-European populations (see online supplementary figure S1C). All populations aged 35–64 years except for Tallinn-Estonia showed significantly decreasing trends of inhospital case-fatality in 1985–2010. The steepest annual decline was observed in Brianza/Varese-Italy (APC=−8.1% in men and −8.3% in women; table 1). During the last 10 years analysed, inhospital case-fatality declined significantly in all populations except in men from Haute-Garonne-France and Girona-Spain and in women from Tallinn-Estonia (table 1 and see online supplementary table S4).
Inhospital case-fatality including the events from all populations showed similar rates in men and women but 10% higher in the older age group (figure 2C). Long-term trends decreased significantly in men and women and in all age groups (table 1).
Discussion
A consistent decrease in AMI attack and mortality rates, and total and inhospital case-fatality occurred in most European populations analysed over the last 25 years. Prehospital case-fatality trends were less clear and differed by population and sex. Trends combining all populations showed that the decline in AMI event rates and case-fatality occurred in men and women, and that case-fatality increased in women aged 65–74 years during 2005–2010.
Attack rate trends
The observed decrease in AMI attack rates in most of the studied populations is consistent with studies from other European regions.16–19 This decrease probably reflects the primary and secondary prevention efforts in Europe. Within the WHO-MONICA Study, it was estimated that trends in major risk factors, such as systolic blood pressure, smoking and cholesterol, explained 40% and 15% of the variability in coronary event rates, in men and women, respectively.20 The prevalence and control of hypertension, hypercholesterolaemia and smoking have greatly improved in recent decades in the analysed populations1 ,21 (see online supplementary table S5). The WHO-MONICA Study also described that treatment changes explained 52% and 30% of the variability in coronary event rates, in men and women, respectively.22 Since 1995 there has been a dramatic increase in the proportion of CHD patients receiving proven-efficacy drugs in secondary prevention in most of the analysed populations.1
Absolute AMI attack rates differed among the included populations. Rates in Finland and in Tallinn-Estonia were the highest throughout the study, while rates in Southern-European populations were the lowest in both men and women. Attack rates decreased in 1985–2010 in all populations except in men from Girona-Spain and Tallinn-Estonia. Regions with the lowest attack rates in men (eg, Girona-Spain) during the whole study period showed the more modest decreases as expected. The dramatic increase in obesity observed in men from Girona-Spain in 1995–2000 may have contributed to the lack of decrease in event rates in this group until 2001.21 As for Tallinn-Estonia, the number of years available cannot entirely clarify the long-term trends in this population. However, the differences in risk factor prevalence in the last decades could provide a plausible explanation for the difference observed between sexes1 (see online supplementary table S5).
The trends including all populations showed that the decline in attack rates was larger in population aged 65–74 years than in the younger population (35–64 years). This difference could be due to the inclusion of first and recurrent events. As the decline in 28-day case-fatality was less steep in population aged 65–74 years, this would decrease the recurrences in this age group. On the other hand, it has been suggested that younger people may show less favourable trends in CV risk factors.16
Mortality rate trends
Absolute mortality rates varied largely between the included populations. The highest rates were recorded in Tallinn-Estonia, Finland and Augsburg-Germany, while mortality rates recorded in Southern-European populations were the lowest throughout the studied period.
In accordance with previous studies,23 ,24 our all-population trends showed a significant annual decline in AMI mortality in both sexes and all age groups, especially in the female older population.17 Our results showed that AMI mortality rates decreased in 1985–2010 in all populations except in men from Tallinn-Estonia. The mortality trend in men from Tallinn-Estonia is heavily influenced by the mortality rates recorded in the last available years (2003–2005), which are much higher than in the other populations. Due to this fact the extrapolation of the whole 1985–2010 trend in men from Tallinn-Estonia and its comparison with the trend in women has to be made with caution. In this regard, the differences in CV risk factors between sexes could explain, at least in part, the difference in AMI mortality rate trends among men and women from Tallinn-Estonia.1
28-day case-fatality trends
In men, the highest total case-fatality was recorded in Tallinn-Estonia and the lowest was recorded in Girona-Spain and in Haute-Garonne-France. In women, four populations showed the highest case-fatality during the study period, while Girona-Spain and in Finland showed the lowest.
A significant decrease in total, prehospital and inhospital case-fatality was observed in 1985–2010 when all populations were combined. The APC was steeper for inhospital case-fatality than for prehospital case-fatality, as described previously.6 While the overall trends in total case-fatality decreased, a significant increase occurred in older women in 2005–2010, which seemed mainly driven by the non-significant increase in prehospital case-fatality in this group in 2005–2010 and by stabilised inhospital case-fatality trends in 2004–2010. The increase in total case-fatality may reflect more atypical symptoms, longer time from symptom onset to hospital presentation or lower prescription of evidence-based medication in older women.
Prehospital case-fatality trends differed by population and sex. Significant declines for the whole period analysed were only found in Haute-Garonne-France and in Girona-Spain, along with declines in men from Finland and in women from Augsburg-Germany and Brianza/Varese-Italy. In Finland, there was a decrease in prehospital case-fatality in men and women in 2001–2007. However, in Augsburg-Germany and Brianza/Varese-Italy, the decline was only present in women. This difference by sex may be related to the higher prehospital case-fatality described in men.25 Because men have a lower 28-day case-fatality than women, this difference disappears when the prehospital and inhospital periods are combined,26 as observed in our analysis. Differences in prehospital case-fatality by population and sex may also be the result of different trends in CV risk factors, awareness of early symptoms and emergency transport times.
Regarding inhospital case-fatality, we found a significant decrease in all populations analysed except for Tallinn-Estonia. Interestingly, in most years with data from Tallinn-Estonia, the lowest inhospital case-fatality was recorded in this region, showing that a further decline in inhospital case-fatality in Tallinn-Estonia may not be realistic from a clinical point of view. The inhospital case-fatality trends including all populations showed a significant decrease in both sexes and all age groups, concurring with previous studies.16 ,17 ,27–30 The inhospital case-fatality decrease may be attributable to the progressive increase in the use of proven-efficacy drugs and invasive procedures, such as percutaneous coronary intervention (PCI) during the AMI acute phase. In line with this plausible explanation, a recent study comparing short-term survival in patients with AMI from Sweden and UK found that earlier and more extensive primary PCI and more frequent use of β-blockers at discharge accounted, in part, for a lower 30-day mortality in Swedish patients.31
The main differences between populations were observed in comparing Tallinn-Estonia to the rest. However, this comparison has to be made with caution due to the shorter period available in Tallinn-Estonia. While Tallinn-Estonia showed the less steep declines in AMI trends, Finland experienced the steepest declines in AMI attack and mortality rates. This difference could be explained, in part, by changes in major risk factors. While in Finland the prevalence of all CV risk factors, except for body mass index, has decreased in the last 40 years, in women from Tallinn only smoking has shown a tendency to reduction in the last decade.32 ,33 In addition, differences in acute care, including PCI and evidence-based drug use, and in socioeconomic factors have probably affected AMI trends. These differences between populations, as well as the described differences by sex in certain populations, highlight the importance of continued monitoring of AMI cases through standardised population-based registries to reduce the inequalities between European populations.
Except in Tallinn-Estonia, AMI event rates and 28-day case-fatality declined in 1985–2010 in all populations analysed. However, not all the populations showing a significant decrease in the overall period also showed a significant decrease in the last 5–10 years analysed. On the contrary, Tallinn-Estonia showed a significant decline in 28-day case-fatality during the last 5 years analysed. These results warrant further analysis to obtain the long-term trends in Tallinn-Estonia and in other European populations and to identify the underlying mechanisms of the reported changes in trend and the short-term differences between the analysed populations.
Limitations
The main limitation of this study is that the number of years available was not the same for all populations. However, at least 20 years were available in all populations except for Brianza/Varese-Italy (16 years) and Tallinn-Estonia (10 years), ensuring comparability of rates and trends. In this regard, long-term trends in Tallinn-Estonia have to be taken as a robust approximation pending further studies. A second limitation is that standardisation between registries was discontinued after the mid-1990s, which may have affected the division of 28-day case-fatality into prehospital and inhospital case-fatality. However, internal standardisation of procedures is regularly conducted in the registries. As all included registries are based on the WHO-MONICA methodology, data quality is warranted and there are no reasons to assume that the standardisation process would be different among registries. A third limitation is the generalisation of the all-population trends. We analysed six European populations, meaning that the reported all-populations trends are not representative of the whole European region but an average of the included populations. On the other hand, the location of the populations and the applied statistical methods provide robust trends as an approximation to European trends.
Conclusions
AMI attack and mortality rates, as well as total and inhospital case-fatality, declined in 1985–2010 in all analysed European populations except for Tallinn-Estonia. However, not all populations showed decreasing AMI trends in the last 5–10 years analysed. In addition, the prehospital case-fatality decline was population and sex dependent, showing that specific actions must be designed and implemented in the identified populations to reduce this major public health burden.
Key messages
What is already known on this subject?
Acute myocardial infarction (AMI) mortality rates, and inhospital case-fatality, are declining in Europe, except in some populations from the former Soviet Union.
European comparative data on AMI incidence and case-fatality trends are lacking since 1999.
What might this study add?
AMI attack and mortality rates, and in inhospital case-fatality, may be stabilising in certain European populations in the last decade.
The AMI prehospital case-fatality decline seems to be population and sex dependent.
The steepest declines in AMI total, prehospital and inhospital case-fatality were observed in Southern-European populations.
Total case-fatality decreased in 1985–2005 in women aged 65–74 years, but increased in 2005–2010.
How might this impact on clinical practice?
Our results suggest that strategies to reduce AMI prehospital case-fatality should be tailored to each population.
The increase in AMI total case-fatality in women aged 65–74 years during 2005–2010 demands attention to the preventive and clinical management of these patients.
Acknowledgments
The authors are grateful to the full roster of AMITIE contributors (http://www.regicor.org/amitie_inv/) for data acquisition and to Elaine Lilly, PhD, of Writer's First Aid, for revision of the English text.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
- Data supplement 2 - Online Appendix
Footnotes
Collaborators The list of all AMITIE Study investigators can be found in the online supplementary appendix.
Contributors Conception of the study: JM. Study design and data acquisition: all authors. Data analysis: IRD. Interpretation of results and preparation of the manuscript: IRD, RE and JM. All authors are responsible for critically reviewing the manuscript and for approving its final version.
Funding This work was supported by the Finnish Foundation for Cardiovascular Research (FINAMI register); the Health Administration of Regione Lombardia (grant numbers 9783/1986, 41795/1993, 31737/1997, 17155/2004 and 10800/2009; Monica-Brianza and the CAMUNI coronary event registries); the Helmholtz Zentrum München (MONICA/KORA Infarction Registry); the German Federal Ministry of Health (MONICA/KORA Infarction Registry); the InVS (MONICA-Toulouse register); INSERM (MONICA-Toulouse register); the Health Institute Carlos III-FEDER (grant numbers RD06/0009, RD12/0042, FIS-90/0672, FIS-93/0568, FIS 94/0539, FIS96/0026-01, FIS99/0655, FIS99/0013-01, FIS 99/9342, PI081327, and CP12/03287; REGICOR register); the Catalan Agency for Management of University and Research Grants (grant numbers 2005SGR00577, 2009SGR1195, 2014SGR240 and 2011BP-B00169 postdoctoral contract to IRD–Beatriu de Pinós Program co-financed by the European Commission; REGICOR register); Fundació La Marató TV3 (grant number ID#081630) (REGICOR register); Agència d'Informació, avaluació i qualitat en salut (grant number AATRM 034/33/02; REGICOR register); the Estonian Science Foundation (Tallinn AMI registry) and the Estonian Academy of Sciences (Tallinn AMI registry).
Competing interests None.
Ethics approval Each registry was approved by its own regional Ethics Committee/Institutional Review Board.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Heartbeat
- Miscellaneous