Article Text

Abstract
Cardiovascular screening in young athletes is widely recommended and routinely performed prior to participation in competitive sports. While there is general agreement that early detection of cardiac conditions at risk for sudden cardiac arrest and death (SCA/D) is an important objective, the optimal strategy for cardiovascular screening in athletes remains an issue of considerable debate. At the centre of the controversy is the addition of a resting ECG to the standard preparticipation evaluation using history and physical examination. The American Medical Society for Sports Medicine (AMSSM) formed a task force to address the current evidence and knowledge gaps regarding preparticipation cardiovascular screening in athletes from the perspective of a primary care sports medicine physician. The absence of definitive outcome-based evidence at this time precludes AMSSM from endorsing any single or universal cardiovascular screening strategy for all athletes, including legislative mandates. This statement presents a new paradigm to assist the individual physician in assessing the most appropriate cardiovascular screening strategy unique to their athlete population, community needs and resources. The decision to implement a cardiovascular screening programme, with or without the addition of ECG, necessitates careful consideration of the risk of SCA/D in the targeted population and the availability of cardiology resources and infrastructure. Importantly, it is the individual physician's assessment in the context of an emerging evidence base that the chosen model for early detection of cardiac disorders in the specific population provides greater benefit than harm. AMSSM is committed to advancing evidenced-based research and educational initiatives that will validate and promote the most efficacious strategies to foster safe sport participation and reduce SCA/D in athletes.
- Prevention
Statistics from Altmetric.com
Background
Cardiovascular screening in competitive athletes is recommended by most major medical organisations and sports governing bodies;1–6 however, agreement on the most appropriate screening protocol remains a topic of considerable controversy. Within the primary care sports medicine and sports cardiology communities, this topic has created a highly charged debate specifically regarding the addition of a resting 12-lead ECG to the preparticipation history and physical examination. This polarised environment has limited a productive discussion of the current evidence, the identification of knowledge gaps and the development of research and educational priorities to improve the cardiovascular care of athletes.
AMSSM charge
The AMSSM Board of Directors appointed a task force to address the issues surrounding the cardiovascular screening of young competitive athletes (age 12–35) in the USA. The objective of the task force was to examine the current evidence and knowledge gaps relevant to cardiovascular screening in athletes and provide a framework for the AMSSM membership to assess screening recommendations and future research directions. This statement is unique in providing an assessment of cardiovascular screening from the perspective of a primary care sports medicine physician. While it may assist other healthcare professionals with cardiovascular screening in athletes, conclusions may not necessarily apply to physicians from other disciplines.
Writing group selection and process
The AMSSM President appointed cochairs (JAD and FGO) to assemble a task force to address the topic of cardiovascular preparticipation screening. The task force was carefully selected to include a balanced panel of primary care sports medicine physicians with demonstrated leadership and expertise in athlete cardiovascular screening to represent the different perspectives of cardiovascular preparticipation screening. This panel focused specifically on issues relevant to the potential addition of ECG to the preparticipation physical evaluation (PPE) and did not address the utility of other potential screening modalities, such as echocardiography.
A survey of the task force members was used to identify key discussion areas and generate an initial outline. The panel subsequently engaged in a series of conference calls, literature review and written communications to discuss and analyse specific areas relevant to cardiovascular screening in athletes, followed by an inperson meeting in Atlanta, Georgia, USA, on 21–22 February 2016. An Executive Summary from this panel is presented in box 1.
Executive summary
The overall role of the preparticipation physical evaluation (PPE) is to evaluate the health of the athlete to optimize safe sports participation.
Early detection of athletes at risk for sudden cardiac arrest and death (SCA/D) is an important objective of the PPE for athletes.
The primary goal of cardiovascular screening of athletes is to identify underlying cardiac disorders predisposing to SCA/D with the intent to reduce morbidity and mortality by mitigating risk through individualized, patient-centered, and disease-specific medical management.
The natural history and absolute risk of conditions associated with SCA/D in athletes identified with a cardiac disorder during screening is largely unknown with limited outcomes-based evidence.
Exercise is a known trigger and can unmask occult cardiac disease to precipitate SCA/D.
The differential risk of SCA/D between athletes and non-athletes is not fully understood based on current epidemiologic evidence.
Athletes display a differential risk for SCA/D based on age, sex, race, sport, and level of play.
The current PPE history and physical examination, while pragmatic and widely practiced, is limited in its ability to identify athletes with conditions at risk for SCA/D.
The electrocardiogram (ECG) increases early detection of some cardiac disorders associated with SCA/D.
ECG interpretation accuracy and reliability are challenges with the principal concern of adding false-positive results to the PPE screening process.
Results from centers with considerable experience in athlete ECG screening have demonstrated improved detection of cardiac conditions with potential risk for SCA/D and decreased false-positive rates.
While there is general agreement that early detection of cardiovascular conditions associated with SCA/D in athletes is important, the absence of clear outcomes-based research at this time precludes AMSSM from endorsing a single or universal cardiovascular screening strategy for all athletes.
AMSSM supports individual physician autonomy to assess the current evidence and implement the most appropriate cardiovascular screening strategy unique to their athlete population and community resources.
Considerations for implementing a cardiovascular screening strategy in a targeted athlete population should include the risk of SCA/D, the available infrastructure and cardiology resources, and the physician assessment that screening for early detection of cardiac disorders has a favorable risk-benefit ratio that will improve athlete outcomes with limited harm.
Physicians incorporating ECG in the cardiovascular screening process should optimize strategies to assure accurate ECG interpretation and adequate cardiology resources to conduct the secondary evaluation of ECG abnormalities.
No screening program provides absolute protection against SCA/D; an emergency action plan and access to an automated external defibrillator (AED) are essential to improve outcomes from SCA in athletes.
AMSSM is committed to evidenced-based research, education, and policy initiatives that will validate and promote the most efficacious strategies to foster safe sport participation and reduce SCA/D in athletes.
The PPE and cardiovascular screening
The role and objectives of the PPE
The overall role of the PPE is to evaluate the health of the athlete to optimise safe sports participation and provide an opportunity to assess current and future health risks and quality of life matters.1 ,5 ,6 Although studies have not shown the PPE to prevent morbidity or mortality in athletes, there is general agreement and acceptance that the primary objective of the PPE is to detect conditions that predispose athletes to serious injury, illness or sudden death.1 The current PPE model employs a comprehensive history questionnaire and physical examination. While pragmatic and widely practiced, this model has shown limited effectiveness in screening for conditions associated with sudden death or catastrophic injury. In 2004, an evidence-based review questioned the PPE format as an effective method for health risk screening prior to participation in exercise and sport.7 As currently practiced, the PPE may have fallen short of achieving its desired purpose, and its primary goals may need to be re-evaluated and refocused.
Ideally, the PPE is performed in the primary care setting (ie, physician's office) as part of the continuous care of the athlete, creating an entry point for young athletes into the healthcare system and affording opportunities to provide education, counseling and intervention for general wellness and injury prevention. Within this context, screening questionnaires serve as an expanded checklist to guide the physician during the preparticipation evaluation of a young athlete. This panel supports the PPE as a mechanism for the general health assessment of the athlete and to establish a minimum standard to evaluate multiple organ systems that may impact safe sports participation. This panel also supports the development of additional strategies to promote the overall and cardiovascular well-being of young athletes and non-athletes.6
The role and objectives of cardiovascular screening
The primary goal of cardiovascular screening in competitive athletes is to identify underlying cardiac disorders predisposing to sudden cardiac arrest and death (SCA/D) with the intent to reduce morbidity and mortality by mitigating risk through individualised, patient-centred and disease-specific medical management.2 ,8 Cardiovascular screening is one component of a comprehensive PPE, although cardiovascular screening can also be performed independently.
Cardiovascular screening in young athletes is challenging, and all potential screening tools have limitations. This panel proposes that a ‘one size fits all’ model of cardiovascular screening is not warranted or justified. It is important that the goals and expectations of cardiovascular screening based on history and physical examination alone be re-evaluated and that considerations for more intensive cardiovascular screening be defined. Factors to consider in selecting a cardiovascular screening strategy include: estimates of risk for SCA/D in the individual or athlete population; available sports cardiology resources and expertise; the potential benefits and harms of the screening process and existing sport association directives.
Considerations for the team physician
Team physicians maintain a unique role and often function as the primary care provider for many of the athletes under their care. Team physicians also recognise that many athletes have a primary care provider, independent of the team, who performs the required PPE and is integral in managing acute and chronic problems that confront the individual athlete. In these circumstances, the team physician has the additional challenge and responsibility for shared decision-making, and open communication between the primary care provider, team physician and athlete is essential for optimising care. Furthermore, the PPE and cardiovascular screening protocol implemented by team physicians may be driven by institutional standards or sport governing body requirements.
Incidence of SCA/D in young athletes
Current evidence
Estimates of the rate of SCA/D in athletes vary widely and are affected by study methodology, the means for case identification, age range, the inclusion or exclusion of cardiac arrest with survival and cases occurring at rest or outside of exercise9–21 (table 1). Based on available US studies and a systematic review of the literature, a generally accepted annual incidence of all SCA/D is ∼1 in 80 000 in high school athletes and 1 in 50 000 in college athletes.22 Studies indicate that 56–80% of SCA/D in young athletes occurs during exercise with the remainder considered non-exertional (ie, at rest or during sleep).12 ,17 ,21
Incidence studies of sudden cardiac arrest and death in US competitive atheltes, military personnel and the young general population
Evidence supports that athletes display a differential risk for SCA/D based on age, sex, race, sport and level of play.9 ,10 ,14–21 Incident rates are consistently higher in male and African-American athletes. Male college basketball players have the highest reported overall risk of sudden cardiac death (SCD) at 1 in 9000 per year, and male African-American college athletes have a reported SCD risk of 1 in 16 000 per year.21 In addition, studies consistently report that two sports alone, male basketball and football, account for 50–61% of all identified cases of SCA/D.12 ,17 ,21 Studies with mandatory reporting systems in other active young adult populations, such as military personnel and firefighters, have demonstrated comparable rates of SCA/D as in college male athletes.23–25
Knowledge gaps
Without a mandatory reporting system for SCA/D in athletes, cases may go undetected and current incidence estimates may not represent the true risk. In addition, current epidemiological studies do not provide a complete understanding of the comparative risk of SCA/D in athletes versus non-athletes as the estimated incidence range of SCA/D in the general population of adolescents and young adults overlaps with that of SCA/D in adolescent and young adult athletes18 ,25–29 (table 1). In a prospective study monitoring SCA in US high schools, student athletes were 3.6 times more likely to suffer SCA while on school campus than non-athlete peers.18 However, this study did not account for activities off campus and did not allow an absolute risk comparison between the groups. In contrast, a recent retrospective study comparing the risk of SCD in adolescent and young adult athletes versus non-athletes from Hennepin County, Minnesota, found a higher incidence of sudden cardiovascular-related death in non-athletes.30 This study was limited by estimates of the athlete and non-athlete populations at risk and by unclear methodology to confirm if cases participated in an organised sport.
Overall, definitive evidence that US athletes as a whole are at higher risk of SCA/D than the general population of similar age is lacking. This uncertainty has generated ethical concerns about limiting a screening programme for unsuspected genetic and/or congenital heart disorders to only competitive athletes.30 ,31 However, systematic preparticipation screening is currently required by sports governing bodies for high school, college and professional athletes in the USA, and there is substantial evidence that some athlete groups, especially in the college age range, have higher rates of SCA/D than estimates for the general population. A standardised approach to the evaluation and reporting of SCA/D in athletes has been proposed and may lead to more precise data moving forward.32
Prevalence of disorders associated with SCD
Current evidence
Exercise is a known trigger and can unmask occult cardiac disease to precipitate SCA/D.33 The prevalence of cardiac conditions associated with SCA/D in young athletes is ∼0.3%.2 This estimate is supported by multiple studies using non-invasive cardiac evaluation tools to identify cardiac disorders at potential risk of SCA/D in young athletes.34–41 The most commonly reported causes of SCA/D in athletes include hypertrophic cardiomyopathy, anomalous coronary arteries, idiopathic left ventricular hypertrophy, arrhythmogenic right ventricular cardiomyopathy, dilated cardiomyopathy, myocarditis, long QT syndrome, ventricular pre-excitation/Wolff-Parkinson-White, aortic dissection and atherosclerotic coronary artery disease.12 ,21 ,42–45 Notably, up to 44% of athletes with SCD have no structural cardiac abnormalities identified on postmortem examination.21 ,43–47 These cases, known as autopsy-negative sudden unexplained death, may be due to primary electrical diseases and inherited arrhythmia syndromes. Structurally normal hearts are also reported in up to 41% of active military personnel with non-traumatic sudden death23 ,24 (table 2).
Causes of sudden cardiac death in athletes, military personnel and the young general population
Hypertrophic cardiomyopathy represents 8–36% of cases in US athletes depending on the study.12 ,21 While the reported prevalence of hypertrophic cardiomyopathy in the general adult population is 1 in 500 or possibly higher,48–50 studies in young athletes have not identified a similar prevalence. This is perhaps due to variable morphological expression of hypertrophic cardiomyopathy during adolescence and young adulthood or functional limitations leading to self-selection out of competitive sports. Based on existing studies, the detected prevalence of hypertrophic cardiomyopathy in a young athletic population is ∼1 in 800 to 1 in 2600.38 ,41 ,51–54 Atherosclerotic coronary artery disease as a cause of SCA/D in athletes increases with age and is also the most common identified cause of SCD in studies of the general population under age 35.29 ,55–59
Knowledge gaps
The lack of standardised autopsy protocols and wider expertise in forensic cardiovascular pathology present challenges to a more precise understanding of the aetiology of SCA/D in athletes. However, even with such protocols, many of these conditions remain challenging to diagnose at autopsy. Current data sets largely involve review of autopsy results that may be limited by inadequate quality or information. In cases with negative or borderline autopsy findings, postmortem genetic testing for cardiovascular conditions with known genetic mutations may provide additional insights into the causes of SCA/D.60 ,61
A better understanding of the prevalence and natural history of conditions leading to SCA/D in different athlete populations will help predict the frequency of screening abnormalities and the potential value of different screening modalities. In addition, while high-risk features for some cardiovascular disorders have been defined, a number of detectable conditions present an uncertain risk of SCA/D in athletes. More information is needed to fully understand which conditions or subsets of conditions will most likely lead to SCA/D.
Cardiovascular screening in athletes
Current assessment
History and physical examination has been the traditional standard for cardiovascular preparticipation screening in the USA.1 ,2 ,62 ,63 The addition of a screening ECG has potential benefits and potential risks. Regardless of the screening strategy, the optimal age and frequency to conduct cardiovascular screening in athletes is uncertain, but generally begun between the ages of 12 and 14 and repeated every 1–3 years. Ideally, preparticipation cardiovascular screening should take place with adequate time prior to the start of a sports season to perform secondary testing of screening abnormalities.
History and physical examination for the cardiovascular screening of athletes
Benefits
Identifying athletes with potential cardiovascular symptoms (ie, exertional syncope) or a family history of juvenile/young adult SCA/D or inheritable cardiac conditions are important elements of screening. The history and physical examination is a core skill routinely practised by medical providers and a fundamental component of the PPE. Based on existing studies, the sensitivity of history and physical examination for the detection of cardiac disorders with elevated risk for SCA/D is ∼20%,54 representing a small but important group of athletes potentially identifiable by the customary screening model. A screening examination also can identify previously unrecognised hypertension in adolescent and young adult athletes, which is important in the prevention of long-term cardiovascular morbidity.64–66
Limitations
Approximately 80% of athletes who suffer SCA/D have no documented warning symptoms at the time of PPE screening and may be missed by an evaluation focused primarily on signs and symptoms.47 ,67–69 Standardised symptom and family history questionnaires, such as the PPE Monograph and American Heart Association questions, also demonstrate a high positive response rate in high school (15–31%) and college (27–37%) athletes,40 ,41 ,70–72 requiring the medical provider to understand the purpose of the questions and the requisite pursuit of additional history to determine the need for secondary testing. Variable understanding of the PPE questions and process can create wide variation in provider follow-up and limit the effectiveness of standardised history questionnaires as a screening tool.
To be effective, PPE questionnaires require an honest patient and thus may fail to elicit a positive response to symptoms that are present but not volunteered. In addition, cardiovascular symptoms may be present in athletes with occult disorders, but misinterpreted as a normal response to vigorous exertion. Some athletes also may develop symptoms subsequent to the PPE, and thus a cardiac disorder could be missed by an evaluation performed at a single time point. Part of the PPE process should include athlete and family education on cardiovascular signs and symptoms that may develop after the examination and warrant re-evaluation.
Several studies indicate that the PPE is not implemented adequately or uniformly.7 ,73–76 This incomplete compliance and awareness of expert guidelines complicates our understanding of the potential benefit and overall feasibility of implementing systematic questionnaires as a primary screening strategy. Recent studies suggest that less than half of primary care physicians are aware of the cardiovascular screening recommendations from the American Heart Association or the PPE Monograph.73 ,74 In a survey of cardiovascular screening practices at National Collegiate Athletic Association Division I universities, 92% of responding universities did not use PPE forms that fully meet the American Heart Association recommendations for cardiovascular screening,75 and, in 2014, only 43% of state high school athletic associations require forms that fully address all of the PPE Monograph (4th edition) personal and family history cardiovascular screening recommendations.76
Physical examination also presents challenges as a screening tool for the identification of cardiovascular disorders. Clinical agreement during cardiac auscultation can vary widely among medical providers, and the ability to distinguish physiological from pathological murmurs is difficult even among experts.77–81 In one pilot study evaluating auscultation clinical agreement during a preparticipation assessment of 101 consecutive athletes, two board certified family physicians each identified six individuals requiring further investigation, but only agreed on one, demonstrating limited agreement with a κ of 0.114 (95% CI −0.182 to 0.411).81 Identification and clinical agreement of the physical stigmata of Marfan's syndrome and related connective tissue disorders is also challenging for primary care providers and experts.82
Knowledge gaps
Despite its use and existence for over two decades, the immediate-term and long-term outcomes of the customary PPE are largely unknown. In fact, no study, to date, has tested the ability of modern recommendations for cardiovascular screening by history and physical examination alone to detect cardiovascular conditions that pose potential risk of SCA/D in athletes. Current estimates of the sensitivity of the history and physical examination are extrapolated from studies that also use other screening modalities such as ECG, and thus interpretation of history or physical examination findings may be confounded when viewed in the context of a normal or abnormal ECG. Thus, the extent to which a screening evaluation using only history and physical examination can identify athletes with conditions associated with elevated risk of SCA/D is yet to be clearly established.
The potential benefit of education, continuity and repeat assessments using a cardiac history and physical examination also requires additional investigation. Further research is needed to improve the sensitivity, specificity, positive predictive value and reliability of screening questions and the physical examination for the identification of athletes with at risk disorders. The physician response to positive history questions remains relatively uninvestigated and non-uniform, and more research is needed to determine the clinical features and pathways for additional evaluation in athletes. Electronic PPE formats may provide a platform to better understand the current PPE process and improve question sets. Whether a PPE performs more effectively than an annual health examination with the patient's primary care physician is also unknown.
ECG for the cardiovascular screening of athletes
Benefits
The addition of a screening ECG to the history and physical examination increases the detection of cardiac disorders potentially at risk of SCA/D in athletes.39–41 ,54 ,68 ,70 ,72 ,83 An estimated 60% of the disorders associated with SCA/D in young individuals may have detectable ECG abnormalities.17 In studies conducted by centres with considerable experience in ECG screening, adding an ECG demonstrates improved sensitivity compared to history and physical examination in detecting previously undiagnosed and unsuspected cardiac disorders.34–41 ,51 ,70 ,83 ,84
ECG is an objective test, but subject to variable interpretation. The use of modern ECG interpretation guidelines that account for physiological adaptations in athletes have reduced the false-positive burden without a demonstrable change in sensitivity.84–87 False-positive rates have declined, ranging from 2.5% to 6.6%, when ECG review is conducted by clinicians experienced in applying modern interpretation standards.40 ,41 ,70 ,72 ,83–88
An ECG deemed to be abnormal is typically an actionable finding in the screening evaluation of athletes. An abnormal ECG also may raise awareness to vague symptoms or relevant family history that previously went unreported or uninvestigated, or initiate a more indepth assessment of questionable physical examination findings.
Limitations
ECG interpretation in athletes is challenging even when using modern criteria, and clinical agreement and reproducibility between physicians can be limited. Some studies have demonstrated that systematic evaluation of an athlete's ECG using standardised criteria improves interpretation accuracy.89 ,90 However, interobserver variability and the reliability of ECG standards even among experienced physicians remains a major concern.91 ,92 In one study, paediatric cardiologists, without the use of a standardised criteria set, achieved a sensitivity of 68% and a specificity of 70% for recognition of abnormal ECG patterns that occur infrequently, but may represent conditions predisposing to SCD.93
The false-positive rate for ECG screening is strongly associated with the criteria used to guide interpretation and the experience of the interpreting physician.83–87 A false-positive ECG leads to additional testing that increases the total cost and may pose other risks to the athlete depending on the nature and timing of the test. ECG is not 100% sensitive for ECG detectable disorders (false-negatives), and the age at which some cardiac disorders manifest ECG abnormalities is variable, raising concerns about the timing of testing and requirements for repeat testing. In addition, some conditions at risk for SCA/D do not manifest ECG abnormalities and thus would not be detectable through ECG screening. Finally, like history and physical examination, some conditions that create an increased risk for SCA/D are sporadic and not present at the time the ECG is obtained.
Physician training and experience are linked to accurate ECG interpretation and limit the ability of many physicians to add ECG to the current screening process. In addition, technical standards need to be adhered to as the use of poor quality, low-resolution ECG instruments or improper recording techniques can also produce misleading results.94 Physician infrastructure and resources remain major obstacles to considering quality application of ECG in the cardiovascular preparticipation evaluation of athletes.95
Knowledge gaps
Education in ECG interpretation is a critical step that should be accomplished before including an ECG in the athlete cardiovascular screening process. While educational modules have been developed, the impact and effectiveness of ECG interpretation training programmes requires additional study. The secondary evaluation of athletes with ECG abnormalities can vary by physician experience,72 and the recommended evaluation of specific ECG abnormalities should be more clearly defined. Finally, the extent to which technology advances and computerised ECG interpretation algorithms using modern athlete-specific standards will improve physician ECG interpretation accuracy is unknown and requires investigation.
Outcomes for early detection of cardiovascular disease
Current assessment and knowledge gaps
Outcome studies of cardiovascular screening in athletes are limited and present conflicting evidence regarding the potential benefit to prevent SCA/D.35 ,51 ,96 In addition, the natural history and absolute risk of conditions associated with SCA/D in athletes identified with a cardiac disorder during preparticipation screening is largely unknown with limited outcome-based evidence.
However, cardiovascular screening is supported based on the premise that early detection of pathological cardiac disorders is important and could make a positive difference, and disease-specific data suggest that individualised risk stratification and management lowers mortality for some conditions. For example, large cohort studies using current management strategies and therapeutic measures have demonstrated improved survival with a low hypertrophic cardiomyopathy-related mortality in children and young adults with hypertrophic cardiomyopathy.97 ,98 A prospective study from Italy found a 73% mortality reduction in athletes from early detection of hypertrophic cardiomyopathy compared to unscreened non-athletes.51 In addition, individualised management and indepth counseling of children diagnosed with long QT syndrome have shown low cardiac event rates and no deaths in two separate cohorts of young recreational and competitive athletes.99 ,100 Expert consensus guidelines for risk stratification and management of asymptomatic athletes identified with a Wolff-Parkinson-White pattern also were developed in partnership between the Pediatric and Congenital Electrophysiology Society and the Heart Rhythm Society.101 ,102 In addition, the American Heart Association and American College of Cardiology recently updated their “Eligibility and Disqualification Recommendations for Competitive Athletes with Cardiovascular Abnormalities.”103 The language and content in these guidelines affirms from cardiology experts that early detection of conditions at risk has the potential for individual benefit.103 Finally, the accurate diagnosis of an inherited cardiac condition in an individual athlete, and the appropriate guidance for participation and treatment, may benefit not only the individual athlete, but also the entire family and possibly future generations through appropriate genetic testing and counseling.
The question of whether early detection provides more benefit than harm applies to cardiovascular screening by any means and the potential risks associated with the early detection and therapeutic process. The detection of a cardiac condition associated with SCA/D statistically places an athlete in a higher risk category than an athlete without a cardiac condition detected by screening. However, data to quantify and predict individual risk are limited, and the potential harms of secondary testing of screening abnormalities must be considered.
Overdiagnosis refers to a disorder detected through screening that does not lead to symptoms or a major event.104–106 The potential for overdiagnosis can be a product of any cardiovascular screening strategy (ie, history and physical examination with or without ECG), but will increase when using modalities with a higher sensitivity. The number of athletes detected with conditions at potential risk needed to identify one athlete that will go on to have SCA/D is affected by the accuracy of the screening procedures, the predicted prevalence of disorders at elevated risk and the estimated incidence of SCA/D (table 3). The lack of definitive outcome data and the uncertainty surrounding overdiagnosis complicate our understanding of whether the potential benefits of adding ECG to cardiovascular screening in athletes will outweigh the potential risks.
The impact of differential risk: number of athletes with detectable cardiac disorders needed to prevent one death*
Physician resources and infrastructure
Current assessment
An ECG screening programme requires physicians knowledgeable in current athlete-specific ECG interpretation standards and adequate cardiology resources to guide the secondary investigation of ECG abnormalities. The absence of a physician workforce capable of accurate ECG interpretation in athletes and the secondary evaluation of ECG abnormalities is a major obstacle to wider application of ECG screening, even among US universities and colleges.6 ,107
Sports medicine physicians conducting or considering ECG screening as a part of a PPE are strongly encouraged to establish a close and collaborative relationship with local cardiology resources as part of a cardiovascular care team approach. Some considerations when identifying appropriate cardiology resources include: specialist availability with practice models that facilitate rapid turn around times; access to timely diagnostic testing; familiarity with contemporary athlete-specific ECG interpretation criteria and a commitment to work in partnership following the establishment of an exercise or competition-limiting diagnosis. The development of regional referral centres has also been proposed to assist in ECG interpretation and the evaluation of athletes with a suspected or known cardiovascular disorder when local expertise is not available.6
Likewise, cardiovascular screening strategies using a standard history and physical examination recommended for over two decades are still not uniformly implemented or practised.73–76 Additional education and implementation strategies regarding best practices for history and physical examination need to be pursued.
Educational initiatives
Consensus standards for ECG interpretation in athletes have evolved considerably over the past decade with each revised criteria set improving specificity.84–87 Online training modules are available at no cost to physicians to foster a common understanding of modern ECG interpretation standards (http://learning.bmj.com/ECGathlete). This may serve as a starting point for physicians, although accurate ECG interpretation will be enhanced by additional clinical experience and ongoing education.
The PPE Monograph is available to guide a standardised preparticipation history and physical examination.1 Additional resources are also available to aid in Marfan's syndrome recognition and diagnosis (http://www.marfan.org/dx/home) and cardiac auscultation skills (http://www.easyauscultation.com/heart-sounds).
Recommendations
Moving forward: a new paradigm for cardiovascular screening in athletes
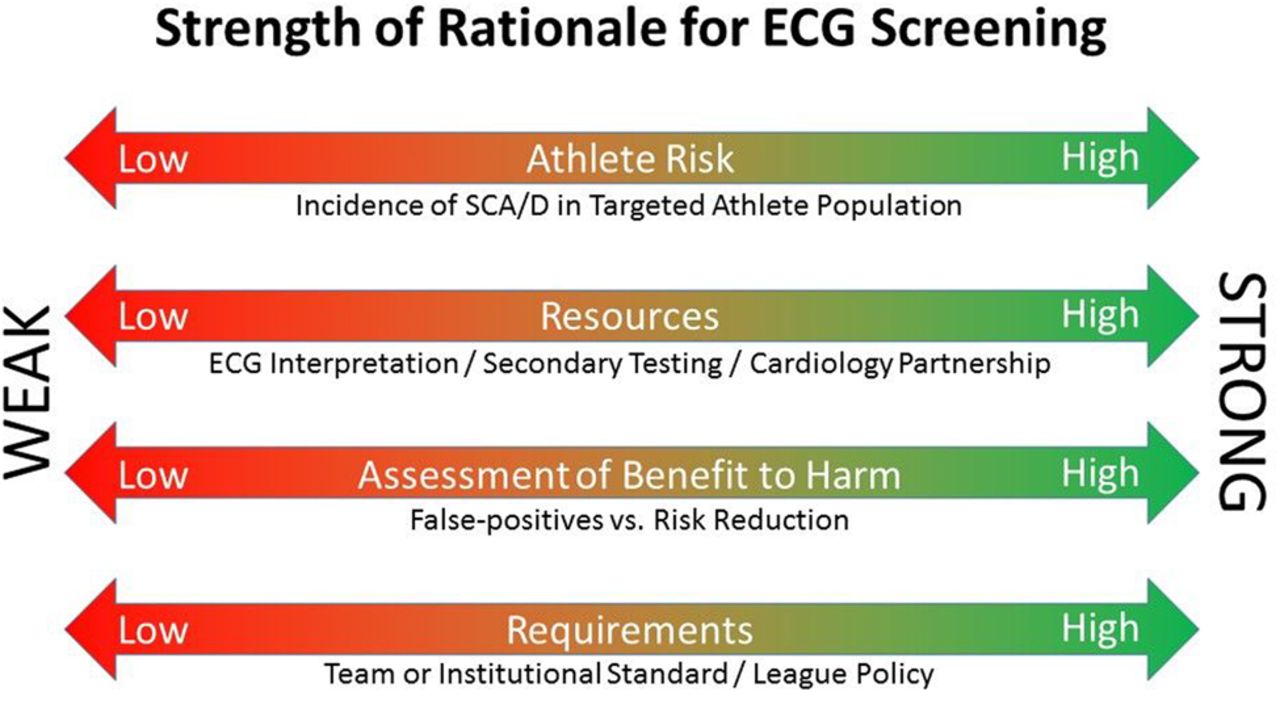
While knowledge gaps exist between the available evidence and the evidence needed to precisely quantify and balance the potential benefits versus the potential harms associated with different models of cardiovascular screening, the lack of definitive data should not discourage reassessment of our current practices. The ECG screening debate is often framed as a choice between universal, mandatory screening or no screening at all.108 These polarised options provide little guidance to explore alternative strategies for the individual physician who recognises the limitations of the current PPE model, understands that adding an ECG has potential benefits and risks and recognises a lack of clear patient-oriented outcome evidence. The primary care sports medicine physician, however, is still responsible for the cardiovascular screening of the individual athlete and in many cases may guide decision-making for at risk populations. A new framework to guide sports medicine physicians in choosing how they perform cardiovascular screening is warranted (figure 1).

{kind=link}
Major considerations and strength of rationale for electrocardiogram screening. SCA/D, sudden cardiac arrest/death.
This AMSSM task force, in moving forward with this position statement and new paradigm, reviewed and reflected on guiding ethical principles and core concepts as applied to evidence-based medicine. The group acknowledged two key ethical principles that guide medical decision-making: beneficence and non-maleficence. Ultimately, the benefit of any intervention must exceed the risks for the intervention to be ethical. In addition, while the physician functions as an educator in informing patients about benefits and risks, in the end it is the patient who assigns them weight. The task force additionally recognised that evidence-based medicine is “the conscientious, explicit and judicious use of current best evidence in making decisions about the care of the individual patient. It means integrating individual clinical expertise with the best available external clinical evidence from systematic research.”109 ,110 Thus, a context for clinical decision-making for cardiovascular screening must be developed that accounts for the individual skills and expertise of the physician, as well as the individual characteristics of the patient or patient population.
At this time, this task force recognises that there is not conclusive evidence to make a universal recommendation for or against the incorporation of ECG screening during the preparticipation evaluation. However, this task force additionally recognises that the current PPE has substantial limitations for detecting occult cardiac disorders, the ECG provides increased sensitivity for detecting some cardiac disorders, a discordance exists between the prevalence of cardiac disorders and the rate of SCA/D and evolving data support that some athletes are at considerably higher risk of SCA/D than others. Accordingly, the cornerstone of this document's recommendations is respect for the autonomy of individual physicians to assess the current evidence, evaluate their unique clinical situation and decide what they believe to be the best decision for their patient or patient population. In this scenario, it is understood that some physicians may decide to implement a strategy for cardiovascular screening that incorporates an ECG, while others may not. Any ECG screening programme if implemented, however, should have a strong infrastructure, high quality control, and consider informed consent that outlines the potential benefits and risks with the athlete (and/or parent/guardian). Optimally, the decision to incorporate or exclude an ECG from the preparticipation evaluation is one of shared decision-making between a patient and a provider.
Risk, resources and opinion on early detection
Where does the risk/benefit ratio change so that adding an ECG is beneficial to the athlete? The primary considerations to add ECG include: (1) individual risk based on age, sex, race, sport and level of play; (2) physician expertise and available cardiology resources to conduct an ECG screening programme with high quality and (3) physician assessment that the utilisation of ECG for the individual athlete provides more benefit than harm (figure 1). Recognition of the differential risk in athletes may lead to an approach that more closely reflects individualised risk. For example, a physician may not add ECG for high school female athletes, but choose to use ECG screening in male, African-American college basketball players. Given the uncertainty and the desire to balance potential harms with the potential benefit of early detection, differential risk, as well as the availability of cardiology resources, may have a substantial impact on the risk/benefit ratio and thus the choice of screening strategy.
In centres where ECG screening is conducted by clinicians trained in athlete ECG interpretation using modern standards and with adequate cardiology resources for secondary investigations of ECG abnormalities, ECG screening can increase the detection of athletes potentially at risk for SCA/D with lower false-positive rates. However, this may not apply to sites with less experience or those without adequate cardiology infrastructure and support. A major challenge to adding ECG is improved training in athlete ECG interpretation and the presence of cardiology expertise for the secondary evaluation of ECG abnormalities.
The foundation of cardiovascular screening relies on the premise that early detection is important and prioritised. If one determines that early detection of occult cardiac disorders is of questionable benefit or outweighed by the potential risks of a particular screening strategy and the lack of definitive outcome data, then this stance argues for less screening or perhaps no screening. Some countries endorse a paradigm with no preparticipation cardiovascular screening of any sort.44 ,111
Weighing the risks versus the benefits
All screening risks the identification of disorders that may not become symptomatic or cause significant morbidity or mortality (overdiagnosis). If the threat (or evidence) of harms from early detection with potential overdiagnosis using a specific screening strategy is large, then screening by that means should be questioned.
The use of ECG will lead to increased detection and thus potentially a greater risk for overdiagnosis, misdiagnosis, unnecessary disqualification or even adverse events or outcomes from activity restrictions, medical management or evaluation and/or treatment procedures. In accepting an additional test to enhance the sensitivity of the PPE, one must also accept that the test layers on additional risk of harm through a greater number of false-positives, costly secondary investigations and the potential for unnecessary interventions, including temporary sports restriction and prohibiting exercise when not indicated. This added layer of risk may be magnified as the incidence of SCA/D declines.
Identification of cardiovascular abnormalities also leads to opportunities for risk assessment and disease management. Published studies of ECG screening in relatively small US athlete cohorts have not reported major adverse events/harm or death as a result of screening.34 ,39–41 ,53 ,70 ,72 ,83 Nonetheless, the potential risks and complications from invasive cardiovascular procedures and therapeutic interventions remain a valid concern.112 ,113 More outcome data are needed to define the procedural risk in athletes with conditions detected through screening. Screening by history and physical examination alone also has potential risks, such as false-positive responses requiring unnecessary investigations, a higher false-negative rate and perhaps false reassurance regarding cardiac safety.
Physician autonomy
The lack of clear outcome data at this time precludes an algorithmic or universal approach to the decision of adding an ECG to preparticipation screening. In addition, while this panel strongly supports the goals of the PPE and cardiovascular screening, in the absence of clear outcome-based evidence, legislative mandates requiring any particular cardiovascular screening strategy as obligatory, including history and physical examination with or without ECG, are unwarranted at this time. In the context of a developing evidence base, this panel respects the autonomy of physicians to choose the best strategy for the athlete population under their care. Physicians should be guided by the previously discussed considerations and their assessment of relevant and emerging research.
Sports medicine physicians responsible for the cardiovascular care of athletes they deem high risk for SCA/D should thoughtfully consider more intensive screening strategies, such as ECG screening. Until more definitive outcome data are available, maintaining the current standard of cardiovascular screening, without adding the ECG, is a reasonable choice for physicians caring for athletes. Some physicians, however, may favour the potential to prevent SCA/D in targeted risk groups and chose to add ECG screening in higher risk athlete populations. Some physicians interested in ECG screening may be limited by the lack of local cardiology resources and are unable to employ ECG screening programmes with sufficient quality control. And finally, physicians with extensive experience in ECG screening and robust cardiology resources may choose to include ECG for all of their athletes. A standardised questionnaire should be considered during the PPE and during well childcare visits that serve as the PPE to guide a comprehensive cardiac symptom and family history evaluation. Additional screening with an ECG should be considered if (and only if) accurate interpretation and proper cardiology resources can be developed or are currently available.
The essential role of automated external defibrillators and emergency action plans
No screening programme provides absolute protection against SCA/D. A proper emergency action plan and access to an automated external defibrillator (AED) are essential to improving outcomes from SCA in athletes.6 ,13 ,114–116 Every school, club and organisation that sponsors athletic activities should be prepared to respond to a collapsed athlete with an acute cardiac emergency. An emergency action plan for SCA with written policies and procedures is recommended to ensure an efficient and structured response to a cardiac emergency. An emergency action plan for SCA including access to an AED increases the likelihood of bystander cardiopulmonary resuscitation, reduces the time to defibrillation and improves survival from SCA. Successful programmes require an organised and practiced response, an established communication method to activate the emergency medical services system and rescuers trained and equipped to provide cardiopulmonary resuscitation and defibrillation.
Prompt recognition of SCA is the first step to an efficient emergency response. Resuscitation can be delayed because SCA is mistaken for a seizure or the rescuer misinterprets agonal gasping for normal breathing.13 ,115 Coaches, sports medicine professionals and other anticipated first responders to SCA in an athlete must maintain a high index of suspicion for SCA in any collapsed and unresponsive athlete. The treatment of SCA involves immediate recognition and activation of the local emergency medical services system (ie, call 9-1-1), early cardiopulmonary resuscitation (starting with chest compressions) and prompt retrieval of an AED for defibrillation. AEDs should be strategically placed within schools and sporting facilities to achieve a collapse to first shock time of <3 min (although immediate availability of AEDs is ideal).116 ,117
Future research directions
This panel has identified many knowledge gaps that would benefit from further investigation. However, the following research priorities are suggested:
Higher quality data on the aetiology of SCA/D in athletes to guide screening strategies. This requires standardised autopsies, wider application of postmortem genetic testing and review of the diagnosis in cases of SCA with survival.
The downstream impact of any screening programme requires more research, a better understanding of the natural history of cardiac disorders and more complete outcome data. The outcomes and clinical course of athletes identified with cardiovascular disorders at risk for SCA/D should be monitored inclusive of adverse events from diagnostic or therapeutic procedures, continued participation in sports and exercise as well as the occurrence of major cardiovascular events or other cardiovascular morbidity.
Potential avenues to refine the history and physical examination as a screening tool for cardiac disorders that place an athlete at elevated risk for SCA/D remain largely unexplored. Research efforts to improve the sensitivity, specificity and reliability of the history and physical examination are needed.
A potential gap exists between the quality and results of ECG screening at expert centres compared to the results of screening at more novice sites with less experience. More data addressing implementation research are needed to address the potential risks and benefits of ECG screening more broadly, and the potential impact of technology advances to assist accurate ECG interpretation results.
Conclusions
The primary goal of cardiovascular screening in competitive athletes is to detect cardiac disorders early in their natural history to more effectively mitigate the risk of SCA/D through improved risk stratification, targeted management and evidence-driven activity recommendations. Acknowledging the gaps and limitations of the history and physical examination, as well as those associated with the potential addition of ECG, to accomplish the goal of cardiovascular screening does not in itself endorse a particular strategy, but is fair to the current state of the science. ECG screening does offer enhanced detection of cardiac disorders at potential risk of SCA/D, but also increases the potential for false-positive results and the associated downstream consequences. In choosing a screening strategy, sports medicine physicians should consider and assess the differential risk of the athlete, the individual needs of their specific athlete population and community, their experience and available cardiology infrastructure as well as their evaluation of the risks and benefits of early detection as a means of reducing cardiovascular morbidity and mortality in athletes.118 No screening strategy provides absolute protection from SCA/D; therefore, proper emergency planning and prompt availability of AEDs during training and competition are critical. Widely practised and accepted screening standards are not perfect and should undergo continual revision as new data emerge. Accordingly, in the absence of a clear evidence-based strategy, AMSSM supports continued research in this area to validate the optimal strategies for reducing SCA/D in athletes. Finally, AMSSM respects and supports the autonomy of an individual sports medicine physician to assess the needs of their athlete population and the assets of their community to implement an appropriate screening strategy.
Supplementary appendix
Acknowledgments
The authors thank the AMSSM Board of Directors and the following individuals for their review of the statement prior to publication: Aaron Baggish, MD, Mats Borjesson, MD, PhD, Benjamin Levine, MD, Brian Hainline, MD, Richard Kovacs, MD, and Willem Meeuwisse, MD, PhD.
References
Footnotes
JAD and FGO cochairs.
This article has been co-published in the Clinical Journal of Sport Medicine, and Current Sports Medicine Reports.
Twitter Follow Robert Dimeff at @Robert @dimeff
Disclaimer The opinions and assertions contained here are private views and are not to be construed as official or as reflecting the views of the Uniformed Services University of the Health Sciences, the US Army Medical Department or the Department of Defense at large.
Competing interests None declared. Please see online supplementary appendix 1 for a list of volunteer positions, board and other paffiliations.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Editorial
- Infographics
- Warm up