Article Text

Abstract
Background In 2010, the European Society of Cardiology (ESC) released recommendations for the interpretation of the 12-lead ECG in athletes, dividing changes into group 1 (training related) and group 2 (training unrelated). Recently, the ‘Seattle Criteria’, a series of revisions to these recommendations, was published, with the aim of improving the specificity of ECG screening in athletes.
Objectives First, to assess the prevalence of ECG abnormalities in a cohort of elite Australian athletes using the 2010 ESC recommendations and determine how often group 2 ECG changes correlate with the evidence of significant cardiac pathology on further investigation. Second, to assess the impact of the ‘Seattle Criteria’ in reducing the number of athletes with ECG abnormalities in whom further cardiac testing is unremarkable (‘false positives’).
Design 1197 elite athletes underwent cardiovascular screening between 2011 and 2012, of whom 1078 aged 16–35 years volunteered and were eligible to participate.
Results 186 (17.3%) had an abnormal ECG according to ESC recommendations and a further 30 (2.8)% had unclassified changes. Three athletes (0.3%) were found to have a cardiac abnormality on further investigation. Using the Seattle Criteria, the number of athletes classified as abnormal fell to 48 (4.5%, p<0.0001) and the three with an underlying cardiac abnormality were still identified. The improved specificity was due to reclassification of 71 athletes (6.6%) with an equivocal QTc interval, 42 (3.9%) with T wave inversion isolated to V1–2 and 22 (2%) with either isolated right axis deviation or right ventricular hypertrophy on voltage criteria.
Conclusions The ‘Seattle Criteria’ reduced the false-positive rate of ECG screening from 17% to 4.2%, while still identifying the 0.3% of athletes with a cardiac abnormality.
- Cardiology
Statistics from Altmetric.com
Background
On the basis of research showing a reduction in the incidence of sudden cardiac death (SCD) in young athletes in the Veneto region of Italy over 30 years after introduction of mandatory preparticipation screening (PPS) inclusive of an ECG, the European Society of Cardiology (ESC) and major sporting organisations including the International Olympic Committee and the Federation Internationale de Football Association now endorse PPS inclusive of an ECG for their athletes.1 ,2
While the addition of an ECG to PPS can improve the detection of cardiomyopathies and primary electrical diseases of the heart, which together account for at least one half of the cases of SCD in young competitive athletes,3–5 physiological cardiac adaptations to exercise, reflected in the athlete's ECG, can mimic pathological changes. Thus, the false-positive rate of ECG screening in an athletic population is not negligible, and resultant secondary testing comes with a significant financial and psychological cost.
In 2010, the ESC released updated guidelines for ECG interpretation in athletes, dividing ECG changes into group 1 changes (those which are common and training related) and group 2 (training unrelated, prompting further investigation to exclude disease), the main change from the 2005 guidelines being the inclusion of left ventricular hypertrophy (LVH) on voltage criteria as a group 1 change. Persistent false-positive rates of 10% in a subelite athletic population6 and the questionable relevance of criteria such as isolated axis deviations have led to calls for further refinement of such guidelines.7 ,8 A recent transcontinental collaboration aimed at achieving this has led to the release of a series of three papers categorising ECG changes as suggestive of either normal physiological adaptations,9 cardiomyopathy (including changes suggestive of pulmonary hypertension)10 or primary electrical disease,11 summarised as the ‘Seattle Criteria’.12
The accuracy of the 2010 ESC recommendations or Seattle Criteria is yet to be assessed in a large cohort of elite professional athletes despite the fact that professional sporting organisations were the first to mandate PPS inclusive of a 12-lead ECG. Given that the extent of cardiac remodelling is associated with training hours and fitness,13 it may be expected that the overlap between ECG changes associated with training and those associated with pathology may be greatest in elite athletes. Furthermore, regional differences in the prevalence of ECG changes may be important and yet current experience is based largely on European populations of Caucasian origin, which may not be applicable to an Australian population of elite athletes, including indigenous Australian/Torres Strait Islander and Pacific Islander/Maori athletes, who are very well represented in elite sport, but in whom we have no data on cardiac adaptation to exercise.
Thus, the aim of our study was to characterise the ECG findings in a group of elite Australian athletes undergoing cardiovascular screening, determine the prevalence of group 2 ECG abnormalities using current ESC guidelines and how often these abnormal findings correlated with significant cardiac pathology on further investigation. Finally, the impact of applying the refined Seattle Criteria on the accuracy of these screening results was to be determined.
Methods
Setting
In Australia, cardiovascular PPS is not mandatory and there are currently no published national screening guidelines. However, a number of professional sporting organisations recommend PPS, in line with European recommendations. In 2011, the authors contacted a variety of sporting organisations Australia wide, currently undertaking, or wishing to undertake ECG screening and invited them to allow their athletes to participate in this study.
Subjects
From June 2011 to December 2012, 1197 elite athletes underwent cardiovascular screening inclusive of a resting 12-lead ECG, personal and family history and physical examination, incorporating each of the 12 items in the Bethesda guidelines for screening. We also enquired about a personal history of palpations or irregular heart beat as per the ESC guidelines,2 and morphometric and demographic data (ethnic background, sport and hours spent in athletic training per week) were collected. Exclusion criteria were age less than 16 or over 35 years, known cardiac disease or multiple screenings (only the first screening episode was included). An age cut-off of 16 was selected to improve the likelihood of identifying athletes with phenotypic expression of diseases such as cardiomyopathies, and reduce the number of false-positive tests due to juvenile ECG patterns of right precordial T wave inversion. One hundred and nineteen athletes were excluded; 94 were aged less than 16 or over 35, 23 had already been screened in the study, 1 had a known diagnosis of cardiac disease and 1 athlete refused consent.
Wherever possible, a cardiologist (MB) attended organised screening days, collected the resting 12-lead ECG and completed the cardiac questionnaire. In a minority of cases, practical constraints mandated that the ECG and questionnaires be performed remotely. Collection of these ECGs was performed under instruction from the study investigators and the ECG was forwarded for reporting and clinical interpretation.
Definitions
Elite athletes were defined as professional athletes whose main source of income was derived from their sport, athletes competing at an international level, for example, Olympic Games, World Championships and/or nationally competitive athletes.
Resting 12-lead ECG
A standard 12-lead ECG was recorded at 25 mm/s and 10 mm/mV in all participants. All ECGs were interpreted by two experienced cardiologists, using the 2010 ESC recommendations14 and classified as having group 1 or 2 changes, in which case further investigation, most commonly an echocardiogram (TTE) was recommended. A cardiac electrophysiologist (JK) was consulted for cases in which the classification was unclear. Wherever possible, any abnormal ECG was repeated with careful lead placement before any further investigation was suggested.
Sinus bradycardia was defined as a resting heart rate <60 bpm; first-degree heart block (first degree atrioventricular (AV) block) as a PR interval >200 ms; incomplete right bundle branch block (iRBBB) as an rsR’ pattern in V1 with QRS duration <120 ms and LVH on voltage criteria as the sum of the S wave in V1 and the R wave in V5 or V6 of >35 mm. Early repolarisation (ERP) was defined as elevation of the J point (offset of QRS complex) of at least 0.1 mV in ≥2 leads. Rohmilt-Estes score for LVH was also calculated. QTc was calculated by hand, using the ‘teach the tangent’ method. The QT interval was measured in lead II or V5 (whichever provided best delineation of the T wave), the preceding RR interval was measured and Bazett's formula was used to calculate QTc. In cases of significant sinus arrhythmia (SA), the average of 3 × QT and RR intervals was calculated.
A Brugada type 1 ECG pattern was defined as high take-off and downsloping ST segment elevation followed by a negative T wave in ≥2 leads in V1–3. The remainder of group 2 ECG definitions is outlined in table 3. ECG changes not classified in the ESC recommendations were documented as indeterminate findings, with further investigation undertaken as felt clinically appropriate.
Subsequently, using the Seattle Criteria, ECG changes were recategorised as normal (training related) or abnormal and representative of cardiomyopathy, pulmonary hypertension or primary electrical disturbance (see table 3 for differences in definitions between criteria).
Statistical analysis
Statistical analysis was performed using SPSS software. Continuous variables were tested for normality of distribution using the Komogorov-Smirnov test. All descriptive variables are expressed as mean±SD or percentages as appropriate. A χ2 test was used to compare the number of ECGs categorised as normal or abnormal using the ESC and Seattle Criteria, with p<0.05 considered significant.
Results
Athletes
In total 1078 athletes, 82% men, with a mean age of 20±4 years (median 19, range 16–35) were screened during the study period of July 2011 to December 2012 (table 1). Of these, 926 athletes (86%) were Caucasian, 76 (7%) were of indigenous Australian or Torres Strait Islander descent, 48 (4.5%) were of Pacific Islander or Maori descent, 11 (1%) African, 10 Asian (0.9%) and 7 (0.7%) South American. All but three female athletes (Asian) were Caucasian. They competed in a range of endurance and non-endurance sports (figure 1) and 64% had represented Australia at the Olympics or World Championships.
Demographic and morphometric information on 1078 elite athletes undergoing screening

Sports participation in 1078 athletes undergoing ECG screening. AFL, Australian Rules Football; ATS/PI, indigenous Australian/Torres Strait Islander or Pacific Islander/Maori athletes; Rugby, Rugby League and Rugby Union. Other: athletics n=5, cricket n=5, equestrian n=2, lawn bowls, shooting, snow board, weightlifting, sailing, rowing Cox n=1 each.
ECG findings
Group 1, training-related changes
In total, 86.7% of all athletes had at least one group1 ECG change (table 2). Multiple group 1 changes were common, with 57% of all athletes demonstrating two or more group 1 changes. The most common changes were sinus bradycardia, ERP, iRBBB, LVH and SA. First degree AV block was seen in 7.5% of the athletes; however, higher degrees of AV block were very uncommon with Mobitz type 1 second degree AV block seen in one athlete.
Prevalence of training-related ECG changes as per 2010 ESC criteria and the Seattle Criteria in 1078 elite athletes
Group 2, uncommon, training-unrelated ECG changes
One hundred and eighty-six athletes (17.3%) had at least one group 2 ECG abnormality and 73 (6.8%) demonstrated two or more group 2 ECG abnormalities (table 3). Of those with abnormal ECGs, 82 (7.6%) had findings suggestive of cardiomyopathy, including 69 (6.4%) with deep T wave inversions. 7.5% of the cohort had findings suggestive of a primary electrical disturbance, with long (>440 ms men or >460 ms women; 2.3%) and short QTc (<360 ms; 4.3%) accounting for most; however, no athlete had a QTC >470 ms or <340 ms (figure 2). Group 2 abnormalities suggestive of pulmonary hypertension, namely RVH, RAD and RAA, often occurred in combination (eg, RVH with RAD) and were seen in 3.1%. Only 3/124 (2.4%) indigenous Australian/Torres Strait Islander or Pacific Islander/Maori athletes had group 2 ECG abnormalities, and none demonstrated T wave inversion beyond V3.
Comparison of the prevalence of abnormal ECG findings representative of cardiomyopathy, pulmonary hypertension or primary electrical disturbance in 1078 elite athletes using the 2010 ESC criteria versus the Seattle Criteria

Distribution of Bazett QTc intervals and the impact of revised QTc cut-offs recommended in the Seattle Criteria. No athlete was classified as abnormal using the Seattle Criteria, compared with 71 (red bars) using the European Society of Cardiology criteria.
Indeterminate ECG changes
Functional AV-dissociation was seen in 16 athletes (1.5%; isorhythmic dissociation in 12 (1%) and junctional escape rhythm in 4 (0.4%); figures 3 and 4). A further 12 athletes (1.1%) had a low atrial rhythm. One athlete demonstrated tightly coupled atrial bigeminy (figure 5), and another had three premature ventricular contractions (PVCs) in one ECG tracing of 10 s duration.

ECG of an asymptomatic 18-year-old football player, demonstrating isorhythmic dissociation. Arrows indicate P waves.
ECG of an asymptomatic 20-year-old Rugby player, demonstrating sinus bradycardia with junctional escape beats.

ECG of an asymptomatic 21-year-old endurance athlete, demonstrating marked sinus bradycardia (HR 38 bpm) and tightly coupled atrial bigeminy. Arrows indicate blocked premature atrial complexes.
Results of follow-up
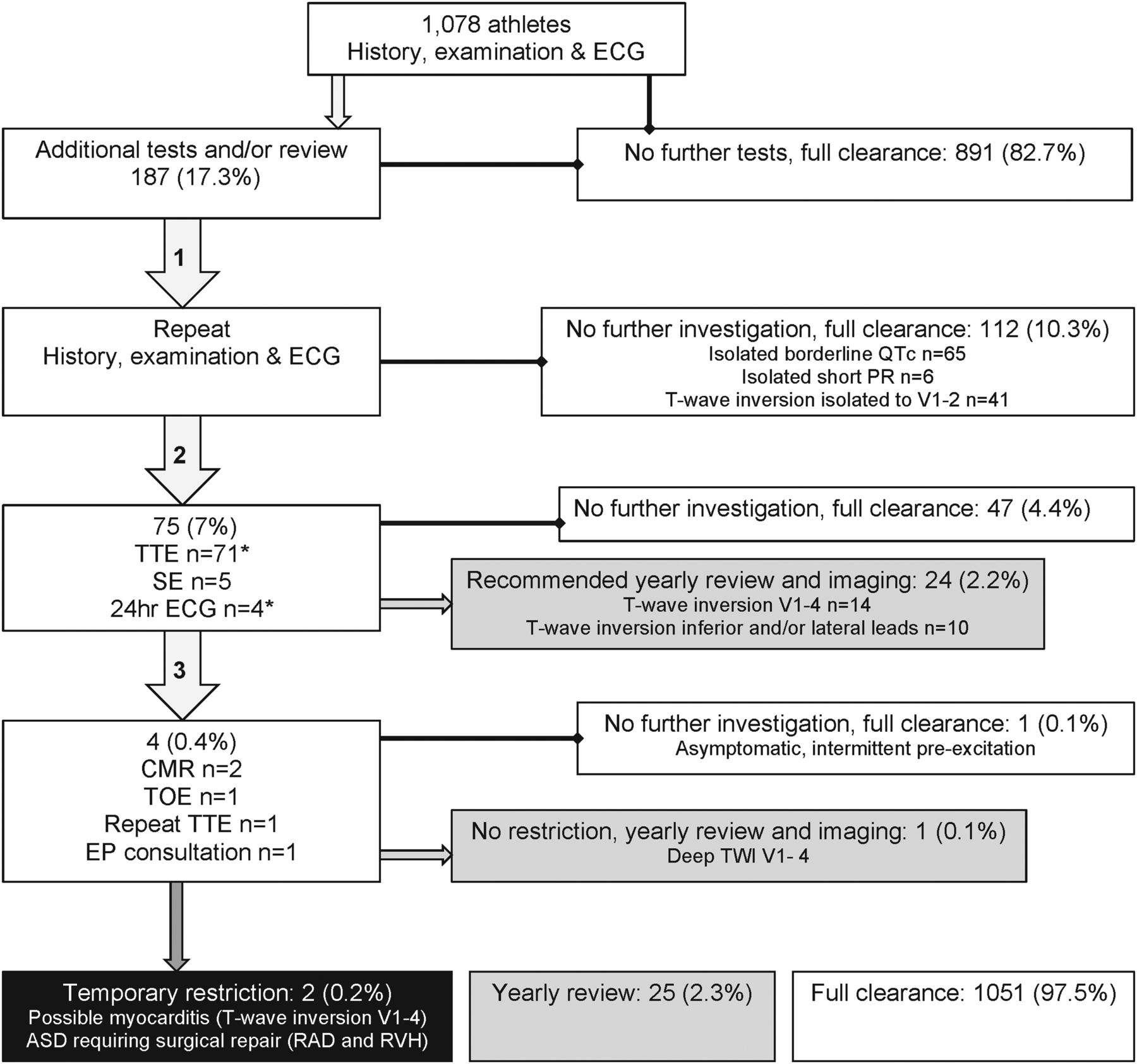
A detailed outline of screening results and follow-up is shown in figure 6. Only one athlete underwent further investigation based solely on history or examination: a male athlete whose mother was presumed to have suffered SCD in her 30s.
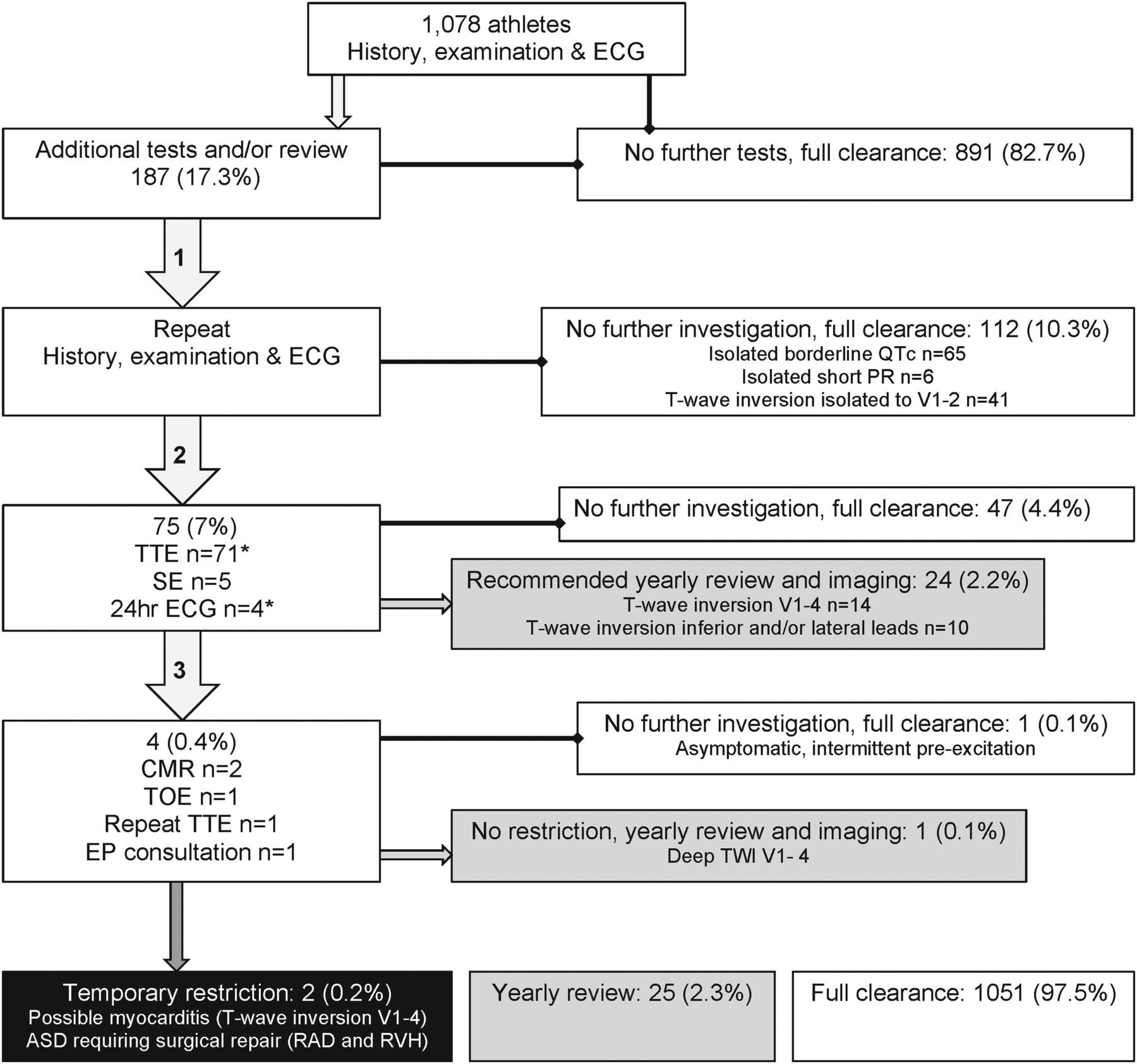
Results of screening inclusive of an ECG, interpreted as per the 2010 European Society of Cardiology recommendations. Arrows 1, 2 and 3 represent subsequent stages of investigation. SE, stress echocardiogram; CMR, cardiac MRI; TOE, transoesophageal echocardiogram; EP, electrophysiology; ASD, atrial septal defect. *One athlete with asymptomatic atrial bigeminy declined follow-up with TTE and 24 h ECG.
Three asymptomatic athletes had positive findings after ECG screening. A 31-year-old man with RAD and RVH on ECG and a subtle cardiac murmur, which was missed at initial screening, was diagnosed with a large atrial septal defect and referred for open surgical repair. An 18-year-old man with deep T wave inversion to V4 who demonstrated a mild segmental abnormality on TTE, was diagnosed with possible acute myocarditis and advised to temporarily refrain from athletic activity. Repeat imaging 3 months later showed resolution of these changes and he has resumed competitive sport, with planned ongoing follow-up. A 21-year-old man with short PR and delta wave diagnosed with intermittent, asymptomatic pre-excitation, with intervention deemed unnecessary after non-invasive investigation and review by an experienced cardiac electrophysiologist.
Despite several athletes having markedly abnormal ECGs, none had structural or functional abnormalities on follow-up imaging consistent with a cardiomyopathy. In those athletes with a markedly abnormal ECG, but no current evidence of structural heart disease, we have recommended repeat clinical evaluation on an annual basis, including repeat ECG and TTE, to ensure that subclinical disease will not be missed. Worthy of mention are the cases of two asymptomatic professional athletes, who after releasing results of screening to their health insurance company were charged a 5% premium for a training-related ECG finding and a 50% premium on the basis of a ‘diagnosis’ of athlete's heart on echocardiogram.
ECG screening results using the ‘Seattle Criteria’
Using the Seattle Criteria, the number of athletes who would have been classified as abnormal and recommended to undergo further follow-up was reduced by 74%, from 186 (17.3%) to 48 (4.5%), p<0.0001 (table 3). Seventy-one (6.6%) with borderline QTc, 42 (3.9%) with deep T wave inversion isolated to V1–2, 22 (2%) with RAD or RVH in isolation, 7 (0.6%) with PR <120 ms, 5 with RBBB and 2 with IVCD <140 ms (0.6%) were reclassified as normal. A further 28 (2.6%) with indeterminate ECG changes were classified as having only training-related changes, and one with three PVCs classified as abnormal. While the sensitivity of ECG screening cannot be formally assessed without imaging all athletes, the three cardiac abnormalities identified with ECG-prompted investigations were identified with both the ESC and Seattle Criteria (figure 7). On the other hand, there were no athletes referred for further cardiac investigation on the basis of the Seattle Criteria alone.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Seattle Criteria reduced the number of athletes classified as having an abnormal ECG requiring further investigation by 74% (from 17.3% to 4.5%), while still identifying the 3/1078 (0.3%) with cardiac pathology.
Discussion
Prevalence of ECG abnormalities
In this, the first study to our knowledge to examine ECG screening findings in an athletic Australian population, and one of the first studies to assess the performance of the 2010 ESC criteria for ECG interpretation in a cohort comprised only of elite athletes, group 2 ECG abnormalities occurred with a prevalence of 17.3%, much higher than the 7% and 9.6% observed in cohorts of University level athletes of a similar age in the Netherlands and the USA, respectively.6 ,15 Although there is a paucity of data on the prevalence of ECG abnormalities in large groups of elite athletes undergoing screening using contemporary guidelines, a relationship between the degree of athletic training and ECG changes such as voltage indices for RVH has previously been documented.16 Thus, it is plausible that the high degree of athletic training in this elite cohort when compared with the University athletes in the other studies contributed, at least in part, to the higher prevalence of group 2 abnormalities. Identification of cardiac pathology on further investigation was very low (n=3/1078, 0.3%), but in absolute terms, not dissimilar to the 3/508 (0.6%) or 3/428 (0.7%) athletes identified in the aforementioned studies. However, only one of the identified pathologies (possible myocarditis) had a clear association with increased risk of SCD.
Mildly prolonged or shortened QTc intervals were seen in 6.6% and accounted for 40% of all group 2 abnormalities. This was surprising, as other screening studies to date have reported a much lower prevalence for LQTc, ranging from 0.03% to 0.3%17 ,18 and short QTc intervals usually not remarked upon, perhaps because of the rarity of SQTS (<1 : 10 000).11 While ethnic and age-related differences in QTc are possible, with no prepubescent athletes (known to have shorter QTc intervals19) included in our cohort, variations in measurement technique and threshold for reporting of borderline intervals may also have contributed to the observed differences.
Impact of the Seattle Criteria
Issues with the 2010 ESC criteria are clear, with QTc cut-offs derived from a non-athletic population set to reflect the 90–95thcentile and 2nd centile for long and short QT intervals.19 Thus, at least 5–10% would be expected to be outside the ‘normal’ range, a number which may be conservative given the difficulties in correcting for QT intervals in athletes who frequently have SA and/or profound bradycardia, which can result in over or underestimation of QTc, respectively.11
Furthermore, up to 25% of participants with genotype-positive LQTS will have QT intervals in the normal range,20 thus it is possible that screening using these cut-offs will miss some cases of LQTS. However, the goal of screening is to prevent SCD, and it has been well demonstrated that two of the more predictive features for SCD in LQTS are a QTc interval exceeding 500 ms and/or a history of syncope,21 both of which will still be identified with a schema which uses more conservative QTc cut-offs. Statistically, those few athletes with phenotype-negative or mild phenotype LQTS who will not be identified using the Seattle Criteria are at lowest risk of SCD.20
Similarly, T wave inversion in V1–2, RVH and RAD are rarely found in isolation in siubjects with diseases related to SCD, such as ARVC,22 yet occur frequently in athletes apparently free of disease.17 ,23 Adjusting QTc value cut-offs to reflect the 99th and 1st centile of the general population (figure 2), the recommendation that T wave inversion in V1–2 in isolation requires no more than a careful personal and physical examination, and the requirement of the presence of dual criteria for RVH to be considered significant (RVH on voltage and RAD >120°), reduced the number of athletes recommended to undergo further investigation by 74%.
Asymptomatic rhythm disturbances, such as junctional escape and low atrial rhythm, were seen in 2.5% of our cohort. Despite being relatively common, such findings were not discussed in the 2010 ESC criteria. In the Seattle Criteria,9 they are discussed as benign training-related changes with reference to a previous observation that such rhythms were seen in 8/1710 (0.5%) adolescent athletes.23 The classic view is that these rhythms are a manifestation of increased vagal tone and yet there is good evidence that intrinsic adaptations of the AV conduction tissue occur with exercise, with longer AV-node conduction times seen in athletes even under pharmacological double-autonomic blockade.24 While the significance of marked sinus bradycardia with atrial bigeminy, seen in an asymptomatic 21-year-old endurance athlete is unclear, it is an interesting finding given the association between long-term endurance exercise and the development of atrial fibrillation, with both increased vagal tone and atrial ectopy among the proposed mechanisms for this phenomenon.25
Markedly abnormal ECGs in asymptomatic athletes with normal imaging
ECG changes may precede the phenotypic expression of cardiomyopathy, and this has been demonstrated on long-term follow-up of asymptomatic athletes with abnormal ECGs, with a minority developing clinical evidence of disease up to 10 years after screening.26 ,27 Thus, 25 (2.3%) asymptomatic, professional athletes with very abnormal ECGs including 0.8% with deep T wave inversions in the lateral leads have been recommended to undergo thorough yearly review, inclusive of repeat imaging. It is somewhat surprising that no athlete was diagnosed with a cardiomyopathy, given that the community prevalence of HCM, for instance, is around 1 : 500.28 It could be argued that self-selection bias played a part in this elite athletic cohort; however, the presence of ‘false negatives’, a rarely discussed pitfall of screening, is possible.
Non-specific ‘abnormal’ ECG changes in the Seattle Criteria
While the Seattle Criteria are likely to represent a significant improvement over the 2010 ESC recommendations, a false-positive rate of 4.2% could perhaps be further improved on. Seven athletes (0.65%) had isolated atrial abnormalities, with TTE demonstrating only physiological remodelling, including mild left/right or biatrial enlargement as commonly seen in athlete's heart.29 Isolated (LAHB) is a common incidental ECG finding, seen in 2.7% of healthy individuals; in the absence of hypertension or coronary artery disease, it seems unlikely to have any prognostic implications or clear association with diseases related to SCD.30 ,31 In our study, isolated LAHB was seen in 4 (0.4%) normotensive, asymptomatic athletes who all subsequently had a normal TTE. There are no studies which specifically address how many participants with HCM (or other cardiomyopathies) would be identified by isolated atrial abnormalities or LAHB. We suspect that these athletes would be few and may represent those with a mild phenotype, at lower risk of SCD. While a minor reduction in sensitivity is possible with the reclassification of isolated atrial abnormalities and LAHB, the false-positive rate of screening would be further reduced to 3.2%
Implications for screening programmes
Using the most contemporary ECG criteria published to date, the number of athletes requiring further investigation on the basis of a single screening episode was reduced from 17.3% to 4.5%. Thus, our data suggest that the use of the Seattle Criteria would result in a marked cost reduction while still identifying those athletes who are likely to have a true underlying pathology. This is the first comprehensive description of the prevalence of ECG abnormalities in a large elite athletic cohort and provides a useful benchmark on which financial constraints may be weighed against potential benefit in the ongoing discussion regarding the role of ECG screening in modern society.
We have also identified factors not previously considered, such as implications for life and health insurance, with participants whose cardiac findings are within limits of normal being charged excesses on insurance premiums on the basis of a ‘diagnosis’ of athlete's heart. For the 2.3% of athletes with very abnormal ECGs, but no current evidence of disease, the ongoing financial and emotional expense may extend beyond that of repeated investigations if they face similar penalties on life and health insurance.
Study limitations
It was not feasible to perform cardiac imaging on all athletes. Thus, the true false-negative rate of ECG screening in this cohort cannot be determined. TTE was the most commonly utilised form of imaging, with CMR being reserved for those with concerning findings on TTE or history. Thus, it is possible that some more subtle cardiomyopathies, apical HCM, for example, may not have been identified. However, the recommendation that any athlete with a distinctly abnormal ECG undergo yearly ECG, imaging and review will improve the identification of subclinical cases on follow-up.
Given the relatively small absolute number of indigenous Australian/Torres Strait Islander and Pacific Islander/Maori athletes in this study, we are unable to draw conclusions about the nature of ECG adaptations in this cohort, and further research is needed.
It was not feasible for all ECGs to be collected by the same person nation-wide, thus inconsistencies in lead placement occurred. However, abnormal ECGs or groups of ECGs with unusual patterns were repeated with careful lead placement. The findings do, however, reflect ‘real world’ practice. Finally, the true effectiveness of screening in identifying those at risk of SCD and preventing SCD would require a far larger cohort with extended follow-up.
Conclusion
In this unique cohort of elite Australian athletes, potentially significant ECG changes requiring further assessment were identified in nearly one in five athletes using the 2010 ESC recommendations for ECG interpretation in athletes. Of the 186 athletes who underwent further testing as a result of their ECG, only three were diagnosed with a cardiac abnormality, reflecting a very high false-positive rate in this elite cohort. Using the Seattle Criteria, less than 1 athlete in 20 would have been required to undergo further testing, while none of the three cardiac abnormalities would have been missed. Thus, the new criteria appear to be as sensitive as the 2010 ESC criteria while markedly reducing the financial and emotional burden of false-positive findings.
What are the new findings?
-
Group 2 ECG abnormalities using the 2010 European Society of Cardiology recommendations were common, seen in 17.3% of this cohort of truly elite athletes.
-
The Seattle Criteria improved the specificity of ECG screening by 74%, reducing the number of athletes who required further investigation from almost 1 in 5 to 1 in 20.
-
The Seattle Criteria improved the specificity of screening while still identifying the three athletes (0.3%) with a cardiac abnormality.
How it might impact clinical practice in the near future?
-
The improved accuracy of ECG screening using the Seattle Criteria will increase the feasibility of broad-based screening programmes.
-
Fewer athletes will be referred for secondary and tertiary investigations as a result of ECG screening.
-
If screening is recommended, this more refined estimate of the prevalence of ECG abnormalities among elite athletes will inform financial and practical resource planning.
Acknowledgments
The authors would like to thank staff and athletes from the various sporting organisations including, but not limited to, the Australian Football League (AFL), Australian Institute of Sport (AIS), South Australian Institute of Sport (SASI), Northern Territory Institute of Sport (NTIS) and Australian Rugby Union (ARU) for their participation in this study. Special thanks to Don Mooney for assistance with the collection of echocardiographic data. MB and ALG are supported by post-graduate and post-doctoral scholarships from the National Health and Medical Research Council (NHMRC) of Australia.
References
Footnotes
-
Contributors MB was responsible for study design, data acquisition, data analysis and manuscript preparation. ALG assisted with study design, data analysis and manuscript preparation. JK assisted with data analysis and manuscript preparation. WL and KF assisted with data acquisition and manuscript preparation. DP assisted with the study design, data acquisition, data analyses and manuscript preparation.
-
Competing interests None.
-
Ethics approval Human Research and Ethics Committee, St Vincent’s Hospital Melbourne and Australian Institute of Sport, Canberra, Australia.
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement All published and unpublished data are available for peer review by correspondence with the authors.