Article Text

Abstract
Telehealth or using technology for a remote medical encounter has become an efficient solution for safe patient care during the severe acute respiratory syndrome coronavirus 2 or COVID-19 pandemic. This medium allows patient immediate healthcare access without the need for an in-person visit. We designed a time-sensitive, practical, effective and innovative scale-up of telehealth services as a response to the demand for COVID-19 evaluation and testing. As more patients made appointments through the institution’s telehealth programme, we increased the number of clinicians available. JeffConnect, the acute care telehealth programme, was expanded to increase staffing from a standing staff of 37–187 doctors within 72 hours. Telehealth care clinicians primarily trained in emergency medicine, internal medicine and family medicine followed a patient decision pathway to risk stratify patients into three groups: home quarantine no testing, home quarantine with outpatient COVID-19 testing and referral for in-person evaluation in the ED, for symptomatic and potentially unstable patients.
- emergency departments
- disaster planning and response
This article is made freely available for use in accordance with BMJ’s website terms and conditions for the duration of the covid-19 pandemic or until otherwise determined by BMJ. You may use, download and print the article for any lawful, non-commercial purpose (including text and data mining) provided that all copyright notices and trade marks are retained.
https://bmj.com/coronavirus/usageStatistics from Altmetric.com
In 2015, Thomas Jefferson University Hospital organised and founded a telehealth programme, JeffConnect. Since that time, virtually all medical and surgical specialties use the enterprise-wide telehealth programme in some way: for remote consults, postoperative follow-up appointments and routine appointments for chronic care. For unscheduled emergency medicine (EM) visits, JeffConnect has an On Demand (OD) programme. This allows patients to have a virtual acute care visit with an EM physician any day, at any hour and any day of the calendar year. Patients first download the OD app to their telephone, tablet or computer. They then interact with the software to connect with a physician and have a virtual healthcare encounter. Patients may be in their home, workplace or elsewhere with a Wi-Fi connection. This service is available to anyone in the states of Pennsylvania, New Jersey (NJ) and Delaware.
Prior to the severe acute respiratory syndrome coronavirus 2 or COVID-19 pandemic, telehealth generally had little overall engagement in the US healthcare system. Much shifted in the setting of COVID-19. Social distancing and keeping people at home became paramount to controlling the spread of the virus. Avoiding unnecessary in-person patient evaluations became valuable.1–3 Thus, telehealth became recognised as a highly effective tool for patient care.
In March 2020, the JeffConnect OD call volume census abruptly increased. COVID-19 infections rose in the Philadelphia region. Advertisements, radio announcements and publications in non-medical sources messaged the public to practise social distancing and to stay home. As a consequence, people wished to avoid in-person healthcare evaluations. Moreover, urgent care centres, where low-acuity patients typically went for less urgent and straightforward chief complaints, closed all over the region. This explained some of the increase in call volumes and growth in telehealth visits.
The historical staffing model of JeffConnect OD with EM-trained physicians was not sufficient for this surge. To aid in the response, we designed a time-sensitive and innovative scale-up: JeffConnect OD was expanded from 37 to 187 clinicians in a 72 hours’ time period. We trained non-previously trained EM faculty physicians and also added internal medicine (IM) and family medicine (FM) physicians and advanced practice providers to the pool of trained clinicians. They needed just a few tools: a reliable Wi-Fi connection, a laptop or desktop computer, with camera and microphone capabilities to see and speak with patients. For training, the clinicians accessed a centralised database with patient screening protocols (COVID-19 and non-COVID-19 specific), tip sheets, training manuals and videos (figure 1). Since JeffConnect generally, and JeffConnect OD, specifically, had a strong telehealth foundation, the institution was in a unique position to leverage the programme quickly. There was no need for new technology or electronic medical record coding billing implementation. As a number of primary care offices were closed, the FM/IM physicians were not seeing their normal volumes of in-person patients. They simply converted some of their patients to telehealth visits and staffed on demand shifts. As these physicians were still being paid their salary and benefits by their respective departments, there was no required increased cost for this staffing change. Due to emergency provisions in reimbursement by insurance companies, telehealth shifts were also reimbursed similar to in-person visits.

Jefferson Health COVID-19 decision pathway.
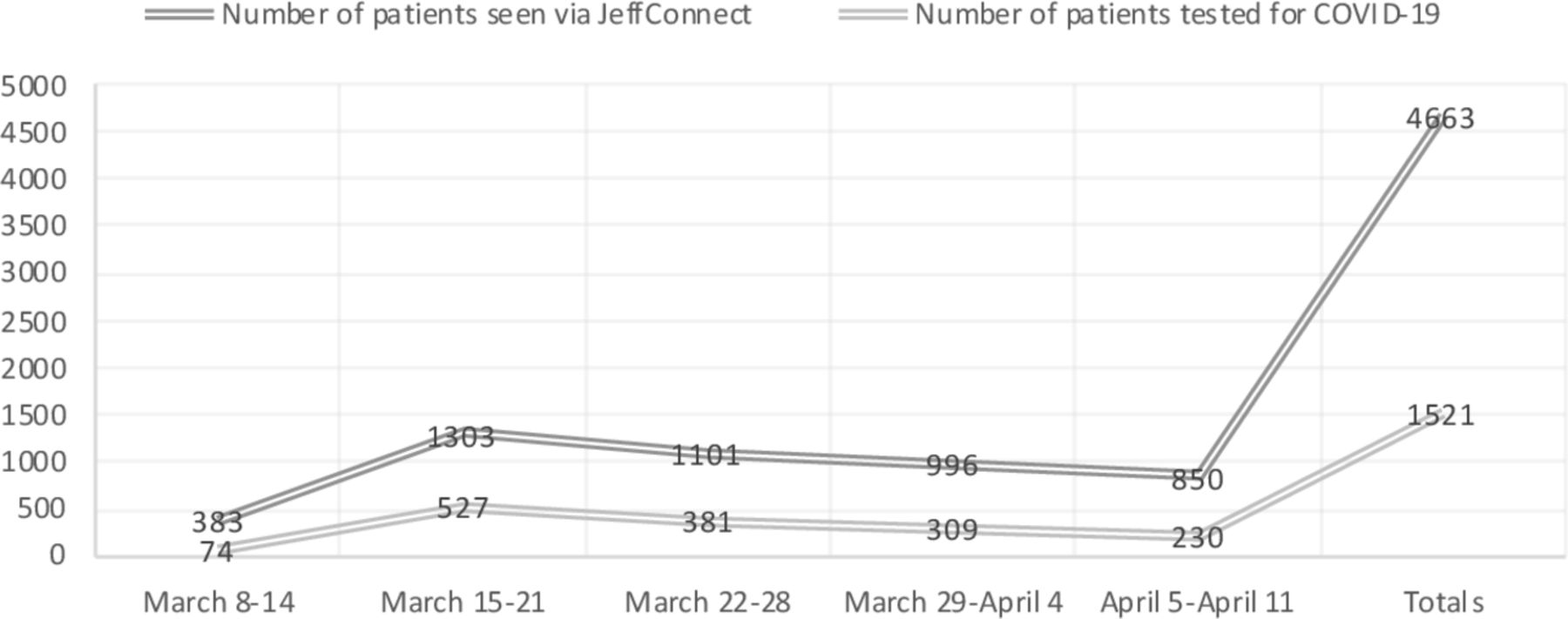
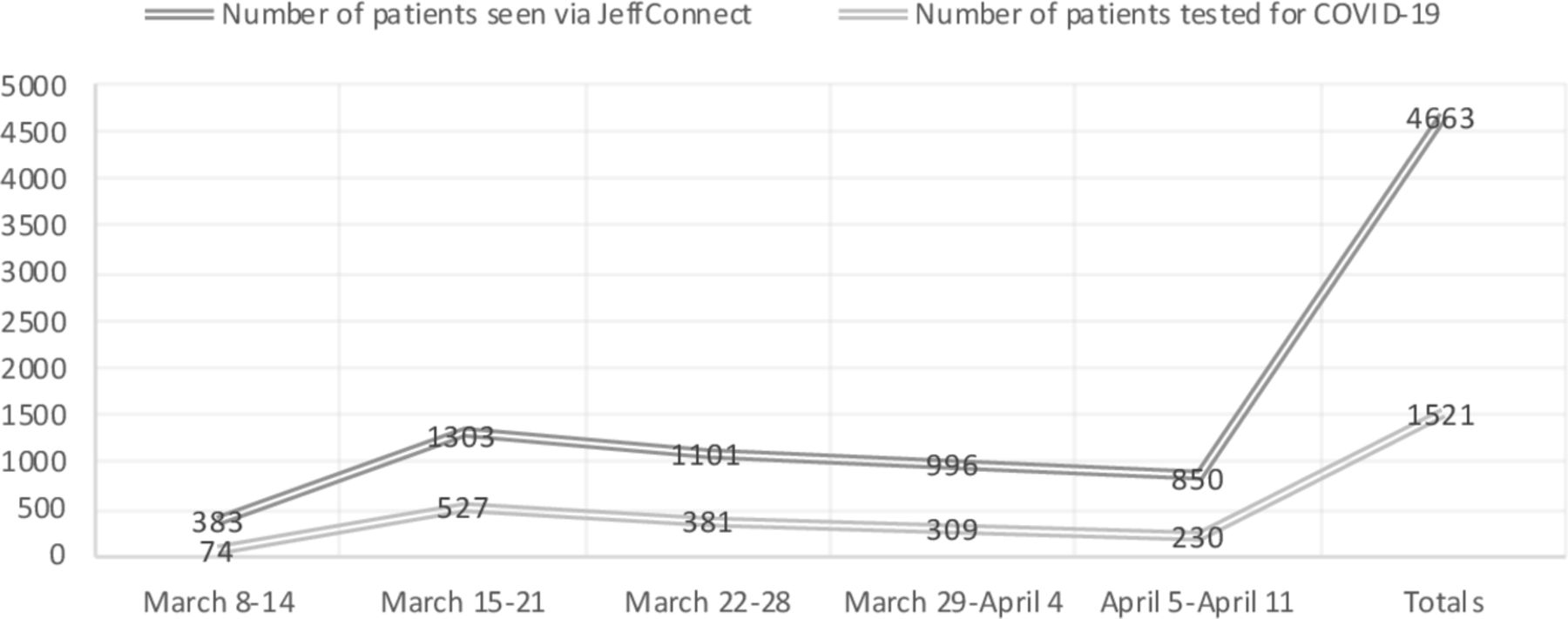
Jefferson Health organised multiple outpatient walk-up and drive-through COVID-19 testing sites. Located in and around Philadelphia and southern NJ, the sites were open to anyone with an outpatient laboratory order placed through a JeffConnect OD visit. Telehealth care clinicians followed a patient decision pathway to risk stratify patients into three groups: for home quarantine without testing, home quarantine with outpatient COVID-19 testing or referral for in-person evaluation in the ED, for patients who were symptomatic and potentially unstable (figure 1). Patients sent for outpatient testing called a central telephone number, were registered and received testing location information. Patients deemed high risk or having signs of respiratory distress on telehealth evaluations were counselled to seek an in-person evaluation. A depiction of the increase in patient call volume and outpatient testing with a peak during the week of 16 March 2020 is illustrated in figure 2.
{kind=link}
{kind=link}
JeffConnect patient visits and testing.
Currently, the JeffConnect OD telehealth programme operates at all hours and is fully staffed with streamlined data reporting. The abrupt increase in telehealth clinicians from different specialties may certainly cause variation in practice and therefore quality assurance with real-time feedback has been necessary to standardise care. The quality assurance process, which tracks metrics such as completion of patient care notes, rate of referral to the urgent care, rate of referral to the ED and patient communication, is examined. Clinicians are notified of any outstanding items in their charts, given tips to improve practice and have questions answered. Overall there has been a decreased rate of referral to a higher level of care. There are at least two reasons for this: (1) an increased number of telehealth patient visits for stable and non-critical care, and (2) clinicians, while following a pathway, are motivated to keep stable patients socially distanced and quarantined at home. Telehealth screening for patients for COVID-19 and outpatient testing referrals have successfully allowed the hospital and ED to prepare for the anticipated increase of sicker patients with COVID-19 who will need hospitalisation and critical care.
There has been an increased recognition of the benefits and ability to have medical encounters virtually. Telehealth has increased its scope and expanded rapidly due to the pandemic, and it is unlikely that healthcare will ever be practised quite the same way again.
Footnotes
Handling editor Simon Carley
Twitter @RELewiss
Contributors Both authors (AJ and REL) planned, wrote and edited the submitted manuscript.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Provenance and peer review Not commissioned; externally peer reviewed.