Article Text

Abstract
Background Outcomes for patients with chronic obstructive pulmonary disease (COPD) with persistent hypercapnic respiratory failure are improved by long-term home non-invasive ventilation (NIV). Provision of home-NIV presents clinical and service challenges. The aim of this study was to evaluate outcomes of home-NIV in hypercapnic patients with COPD who had been set-up at our centre using remote-monitoring and iVAPS-autoEPAP NIV mode (Lumis device, ResMed).
Methods Retrospective analysis of a data set of 46 patients with COPD who commenced remote-monitored home-NIV (AirView, ResMed) between February 2017 and January 2018. Events including time to readmission or death at 12 months were compared with a retrospectively identified cohort of 27 patients with hypercapnic COPD who had not been referred for consideration of home-NIV.
Results The median time to readmission or death was significantly prolonged in patients who commenced home-NIV (median 160 days, 95% CI 69.38 to 250.63) versus the comparison cohort (66 days, 95% CI 21.9 to 110.1; p<0.01). Average time to hospital readmission was 221 days (95% CI, 47.77 to 394.23) and 70 days (95% CI, 55.31 to 84.69; p<0.05), respectively. Median decrease in bicarbonate level of 4.9 mmol/L (p<0.0151) and daytime partial pressure of carbon dioxide 2.2 kPa (p<0.032) in home-NIV patients with no required increase in nurse home visits is compatible with effectiveness of this service model. Median reduction of 14 occupied bed days per annum was observed per patient who continued home-NIV throughout the study period (N=32).
Conclusion These findings demonstrate the feasibility and provide initial utility data for a technology-assisted service model for the provision of home-NIV therapy for patients with COPD.
- COPD exacerbations
- non invasive ventilation
Data availability statement
Data are available upon reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
Remote-monitoring using an ‘auto-titrating’ mode of home non-invasive ventilation (NIV) in patients with chronic obstructive pulmonary disease (COPD) is feasible, with potential to achieve outcomes mirroring those from randomised control trials
Home-NIV supported with two-way remote monitoring and use of iVAPS-autoEPAP mode is feasible, with prolonged time to readmission or death within 12 months versus a comparator group of patients noted in this retrospective observational study.
The COVID-19 pandemic has mandated remote-management for respiratory care where feasible. This is the first study to provide an approach, demonstrate feasibility and provide encouraging early utility data for a technology-assisted service model for home NIV provision to patients with COPD.
Introduction
Chronic obstructive pulmonary disease (COPD) is the second most common cause of emergency hospital admission in the UK, accounting for over 1 million bed days at a cost to the National Health Service (NHS) of over £800 million a year.1 Around a third of those admitted to hospital following an exacerbation of COPD are readmitted within 90 days, which is also strongly associated with post-discharge mortality.2 Avoiding COPD exacerbations and hospitalisations is noted to be a key priority by patients with COPD,3 4 and targeting a reduction in these is necessary to address the substantial health and economic burden imposed by COPD.
The risk of hospital readmissions and further life-threatening events is particularly high among patients with a severe exacerbation of COPD that leads to hypercapnic respiratory failure.5 The first-line treatment for these patients in the acute setting is non-invasive ventilation (NIV), which has been shown to prevent intubation and invasive mechanical ventilation and reduce hospital mortality.6 7 However, it was previously reported that more than 75% of patients treated with NIV for acute hypercapnic respiratory failure were readmitted and nearly 50% died within the first year after discharge.5
A growing area of interest to improve outcomes for patients with severe COPD focuses on the application of long-term NIV in the home setting. In a recent landmark study, Murphy et al showed that the addition of home-NIV to long-term home oxygen therapy in patients that remained severely hypercapnic 2–4 weeks after an exacerbation delayed and reduced hospital readmissions at 12 months.8 A benefit on 12-month overall survival was noted in an earlier randomised controlled trial involving stable hypercapnic patients treated with home-NIV.9 The driver of clinical improvements across both studies can be attributed to higher inspiratory pressures targeting a reduction in carbon dioxide (CO2) in patients who were persistently hypercapnic. A task force of the European Respiratory Society has since adopted home NIV as recommended treatment for patients with COPD presenting with persistent hypercapnic respiratory failure.10
Overall, the existing body of research suggests that there are some open questions with regards to patient selection and timing of home-NIV.11 12 For example, only 5% of patients screened in home oxygen therapy-home mechanical ventilation (HOT-HMV) study were recruited to the trial, raising questions about the external validity of NIV randomised controlled trial (RCT) results. Many of the patients excluded from NIV RCTs have presentations such as coexisting obesity, recurrent episodes of acute hypercapnic respiratory failure despite optimal management or suspected or confirmed symptomatic COPD-OSA (obstructive sleep apnoea) overlap for which home NIV provision is an accepted indication. Obtaining real-world experience data to determine whether beneficial outcomes from home NIV COPD RCTs can be matched with routine clinical adoption is required.
The feasibility of delivering home-NIV to patients outside of controlled clinical trial settings also remains to be established. Provision for elective inpatient NIV initiation and titration outside of tertiary centres and clinical trial settings is limited. Patients with COPD generally wish to avoid hospitalisations, and severity of their illness limits capacity for outpatient attendances. Regular follow-up helps to monitor the effectiveness of ventilation, encourages treatment adherence and optimises patient comfort and ventilator settings, but realistic delivery of intensive follow-up is problematic.13 The COVID-19 pandemic has presented additional challenges including overall healthcare service pressures and capacity, social distancing requirements, need to minimise risk of nosocomial COVID-19 in vulnerable patient and infection control requirements for clinicians, with NIV classified as an aerosol generating procedure. There is therefore a requirement to develop and evaluate service models which can facilitate provision of home NIV for patients with COPD at scale, without variations of care.
It has been demonstrated that patients with COPD at high risk for exacerbations can be taught to self-manage when offered ongoing support.14 Early evidence that compares remotely monitored patients with COPD with usual face-to-face care is encouraging in terms of patient quality of life and number of hospital admissions.15 With the recent advent of two-way remote-monitoring, healthcare providers can view live NIV data from patients, adjust ventilator settings remotely and prioritise workflow to facilitate personalised care.
Given preceding equipoise, prior to 2017 we had only provided home NIV to patients with COPD at our centre on a highly selected case–case basis. Following publication of the HOT-HMV study8 NHS Greater Glasgow and Clyde (GG&C) developed and implemented an assistive technology supported service for patients with COPD requiring home NIV. Service is based at Queen Elizabeth University Hospital (QEUH) which is a large tertiary centre with 1677 acute beds, serving a referral population of 1.2 million patients. Referrals for consideration of home NIV were taken from respiratory teams at QEUH and from associated general hospitals in the West of Scotland region. Patients with acute hypercapnic respiratory failure were not proactively ‘pulled’ into the service over the first year, pending acquisition of implementation-effectiveness feasibility experience.
We routinely use iVAPS-autoEPAP NIV mode (Lumis, ResMed) for home NIV at our centre. Use of iVAPS mode has been shown to reduce time required for satisfactory NIV set-up in patients with COPD.16 Additional advantages include capability of the mode to adapt to patient’s fluctuating clinical status such as improvements post exacerbation. Auto-EPAP modes can potentially address coexisting OSA (there is a high prevalence of obesity in our population) and variable expiratory flow limitation, which is emerging as important treatment target in COPD.17 Remote monitoring allows detection and management of excessive unintentional leaks and suboptimal pressure support provision which were previously a concern for the continued use of volume-assured pressure support NIV modes. It remains however essential to benchmark outcomes, to ensure that care-quality is maintained with this approach to NIV set-up.
For this evaluation, we retrospectively reviewed routinely available health record data from the patients with COPD who were commenced on remote-monitored NIV therapy over the first 12 months of this service. Our aim was to evaluate feasibility and acquire exploratory utility data from a real-world cohort of hypercapnic patients with COPD, who have a typical range of comorbidities which would have excluded many from NIV RCTs. We also had available routine health record data in a comparator cohort of patients from a 6-month period within 2017 who had received acute NIV for COPD at QEUH but had not been referred for consideration of home NIV. The primary outcome from our evaluation was median time to readmission or death over 12 months inpatients receiving home-NIV, with planned comparison of this outcome between patients who continued versus discontinued home-NIV during the follow-up period, and with patients in the comparator cohort. Data on respiratory-related hospital admissions, occupied bed days, respiratory nurse home visits and follow-up capillary blood gases was also available.
Methods
Study design and patients
This study is part of programme of work analysing outcomes in a data set of patients with COPD provided by NHS GG&C Safe Haven. Local Privacy Advisory Committee approval was obtained for release of de-identified data for this study.
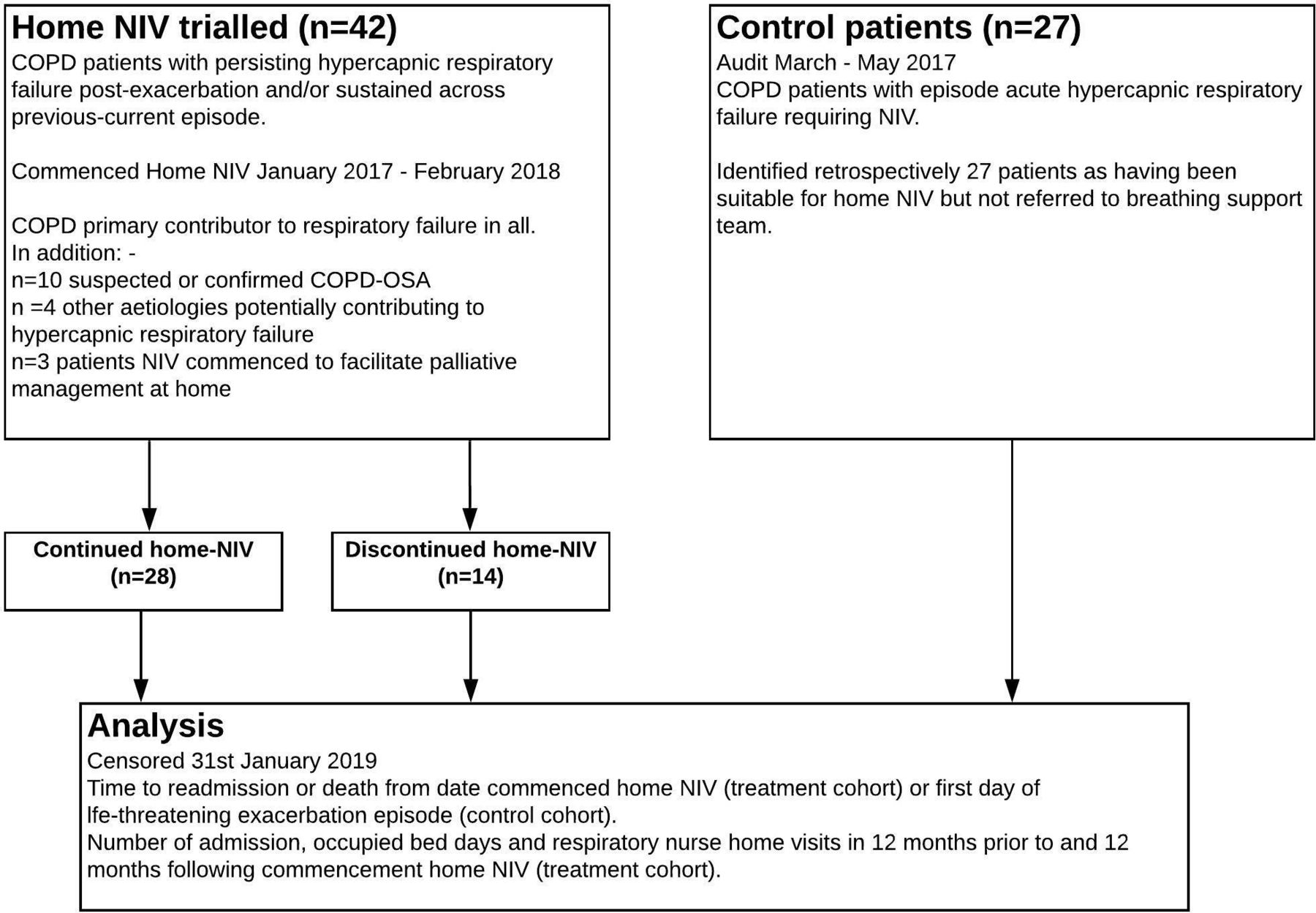
Two cohorts were sampled from the database as outlined in figure 1. The home-NIV cohort consisted of 42 consecutive patients with COPD who commenced home-NIV between 25 February 2017 and 25 January 2018 at the QEUH. COPD diagnosis was confirmed as per Global Obstructive Lung Disease (GOLD) guidelines, and was the primary diagnosis responsible for hypercapnic respiratory failure in all patients in this cohort. Hypercapnic respiratory failure was defined as partial pressure of carbon dioxide (PCO2) >7 kPa at least 2 weeks after index acute exacerbation and/or presence of persisting hypercapnia across current and previous COPD episodes, with deferred NIV assessment for attempted follow-up post episode judged inappropriate.

Study participant flow diagram. COPD, chronic obstructive pulmonary disease; NIV, non-invasive ventilation; OSA, obstructive sleep apnoea.
Twenty-eight patients in this cohort continued optimised home-NIV throughout the 12-month study period (‘NIV users’). NIV usage, mask leak and therapy parameters were within standard acceptable range throughout this follow-up period.
Fourteen patients discontinued home-NIV due to poor acceptance despite individualised interventions to optimise therapy during the study period (‘NIV non-users’).
The comparator cohort comprised 27 patients treated with acute NIV at the QEUH between March and November 2017 following a life-threatening exacerbation of COPD that resulted in hypercapnic respiratory failure. This cohort had been created to consider patient numbers and potential care-quality gap addressable by ‘pulling’ patients with hypercapnic respiratory failure in for home NIV consideration. Retrospective review noted that patients in this group were suitable for home-NIV but they were not referred to the home-NIV service during the follow-up period of this study. None of these patients crossed over to commence home NIV during the study’s observed follow-up period.
All patients in both cohorts were noted to be receiving guideline-based COPD care, including home oxygen therapy unless contraindicated. All patients with COPD are referred for pulmonary rehabilitation post exacerbation, but data on uptake and completion is not available in the research data set.
Intervention
Since early 2017 we offer trialling home NIV to patients with COPD with persistent hypercapnia (PCO2 >7 kPa) at stable status, or during an acute episode if there has been recurrent hypercapnic respiratory failure where deferring commencing home NIV to outpatient review is judged impractical or unsafe by patient-clinician consensus. Often this decision to offer home NIV within an acute episode is supported by high serum bicarbonate levels (implying chronic hypercapnia) and/or presence of suspected or confirmed OSA overlapping with severe COPD. Inpatient sleep testing data are not routinely available at our referring general hospitals and when home NIV is clearly indicated and iVAPS-autoEPAP mode will be used for therapy, we do not undertake OSA quantification as it extends hospital stay and does not alter immediate management. This is an extrapolation of the approach recommended in American Thoracic Society guidance on management of inpatient presentations of obesity hypoventilation syndrome.18
Patients in the home-NIV cohort were commenced on remote monitored home-NIV in iVAPS-autoEPAP mode (Lumis 150 ST-A, AirView, ResMed) if persisting hypercapnia was present at day case review 2–4 weeks following hospital discharge (n=14/42) or during the index hospital admission if persisting hypercapnia had been demonstrated across previous COPD episodes as per above noted criteria (n=28/42)
Patients initiated on home-NIV consented to their data being accessed and shared on the AirView platform by the necessary healthcare professionals. AirView data review was used to inform routine clinical care and identify NIV therapy issues (usage, leak) as well as ventilation data patterns supporting optimised NIV provision. Remote-monitoring pathway is used to support day case NIV initiation, or early hospital discharge if NIV is initiated during an inpatient episode. Remote-monitoring data are reviewed at day 1–2, day 5–7 and weekly thereafter, combined with individualised telephone or video consultation based initial follow-up. Remote-adjustments to iVAPS-autoEPAP NIV settings, adjustment to NIV interface and face–face at home or day case review arrangement are made where remote-monitoring and consultation data indicates a requirement. Stability is judged based on patient comfort and symptoms, acceptable NIV usage durations, minimised unintentional leak and appropriate pressure support and other ventilator parameters. Clinic follow-up within 8–12 weeks including repeat capillary blood gases is scheduled for stable patients who can attend. Patients who are having persisting difficulties establishing home NIV despite remote-monitoring inputs are offered elective admission.
The online supplemental material provides an additional overview of the technology-assisted COPD NIV therapy protocol as implemented in NHS GG&C, with typical follow-up schedule and representative remote monitoring data.
Supplemental material
Outcome measures
Baseline descriptive data were available including gender, age, body mass index (BMI), predicted forced expiratory volume in 1 s (FEV1)% as well as comorbidities that could potentially contribute to hypercapnia. The primary outcome was time to readmission or death, censored at date of admission, date of death or 25 January 2019. Secondary outcome measures included time to hospital admissions and overall survival in the home-NIV and comparator cohort.
Subgroup analyses of the home-NIV cohort explored differences between NIV users and NIV non-users in the primary and secondary outcome measures. Changes in number of hospital admissions, occupied bed days (OBDs) and respiratory nurse home visits were evaluated in NIV users and NIV non-users before and after home-NIV. Changes in capillary blood gas PCO2 and bicarbonate were available for review in patients in the home-NIV cohort who were able to attend for follow-up.
Statistical analyses
Baseline characteristics of the study population are presented as mean (SD), median (IQR) or count (percentage), as appropriate. Primary and secondary study outcome measures were compared between the home-NIV and control cohort using Kaplan-Meier survival analysis and the Mantel-Cox log rank test.
Additional subgroup analyses compared primary and secondary outcome measures between the NIV user group and the NIV non-user group alongside the control cohort using Kaplan-Meier and Mantel-Cox tests. Changes in healthcare usage (number of hospital admissions, OBDs and respiratory nurse home visits) and capillary blood gas PCO2 and bicarbonate between NIV users, NIV non-users and the control cohort were analysed using Wilcoxon signed-rank test. Statistical analyses were conducted using IBM SPSS Statistics V.24 (IBM, New York, USA) and GraphPad Prism V.7.0 (GraphPad Software, San Diego, USA).
Patient and public involvement
Due to the nature of a retrospective analysis, the research was undertaken without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes, interpret the results or to contribute to the writing or editing of this document for readability or accuracy.
Results
Baseline characteristics
Baseline characteristics are shown in table 1. Gender, BMI and age are similar across all study cohorts except for a higher rate of men, lower BMI and a lower rate of notable comorbidities (suspected or confirmed overlapping OSA, long-term opiate therapy) in the NIV non-user subgroup. All patients were ‘white British’ ethnicity, which is typical of the local population. The FEV1% predicted value was around 40% across all study groups, in line with a ‘severe’ classification of COPD(3) particularly as in many patients the spirometry was an historical rather than contemporary result.
Baseline characteristics
Time to readmission or death
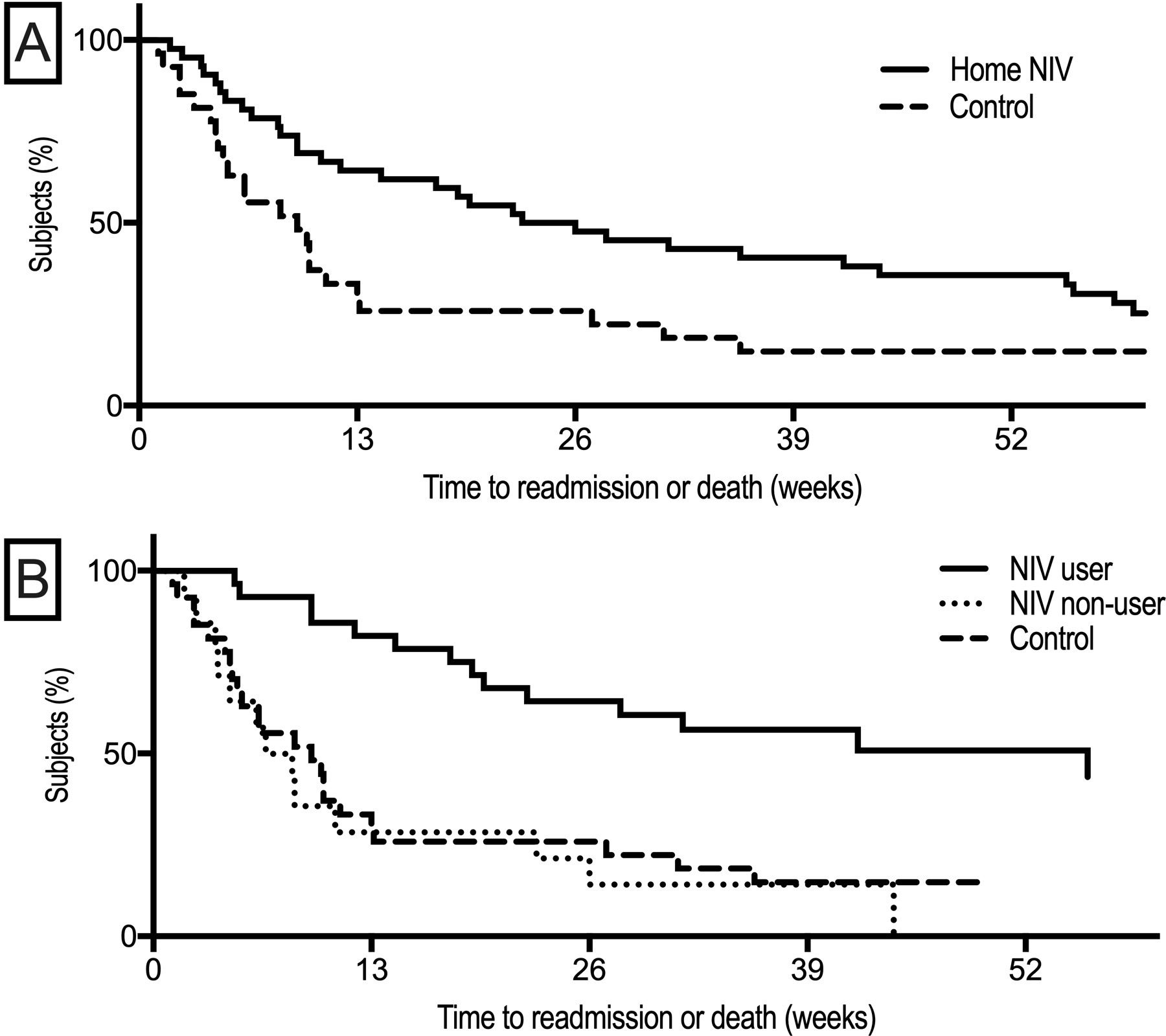
The median time to readmission or death was significantly prolonged in patients with persisting hypercapnic respiratory failure treated with home-NIV compared with the comparator cohort of hypercapnic patients with COPD (p<0.01, see figure 2A). Subgroup analyses showed significant differences between the NIV user subgroup versus both the NIV non-user group and the comparator cohort (both p<0.001). Improvement in time to readmission or death was not seen in patients who discontinued home-NIV (figure 2B). Table 2 summarises time to readmission or death for each group.

Kaplan-Meier plot of time to readmission or death from study initiation to the end of study follow-up. (A) Primary analysis shows significant differences between the home-NIV and the comparator cohort. (B) Subgroup analyses showing improved time to readmission or death in patients who continued home NIV during study follow-up period compared with patients who discontinued home NIV and patients in the comparator cohort who had acute hypercapnic respiratory failure but were not referred for consideration of home NIV. NIV, non-invasive ventilation.
Primary and secondary study endpoints per study population
Median number of days to hospital readmission
Time to hospital readmission followed the same pattern as time to readmission or death. Median time to hospital readmission was 221 days for the home-NIV cohort (95% CI, 148 to 294) and 68 days (95% CI, 18 to 118; p<0.05) for the comparator cohort. Subgroup analyses showed that time to hospital readmission was significantly improved in NIV-users when compared with NIV non-users and the control group (both p<0.01). There was no significant difference in these outcomes between the comparator patients and NIV non-users (p=0.38).
Overall survival
Twelve-month overall survival was 78.6% in the home-NIV cohort and 59.3% in the comparator cohort. Patients that continued to use home-NIV during the study period had a 12-month overall survival rate of 85.7%. Due to the low number of recorded mortality events, group differences were not statistically significant in the primary (p=0.066) or subgroup analyses (p=0.07).
Healthcare usage
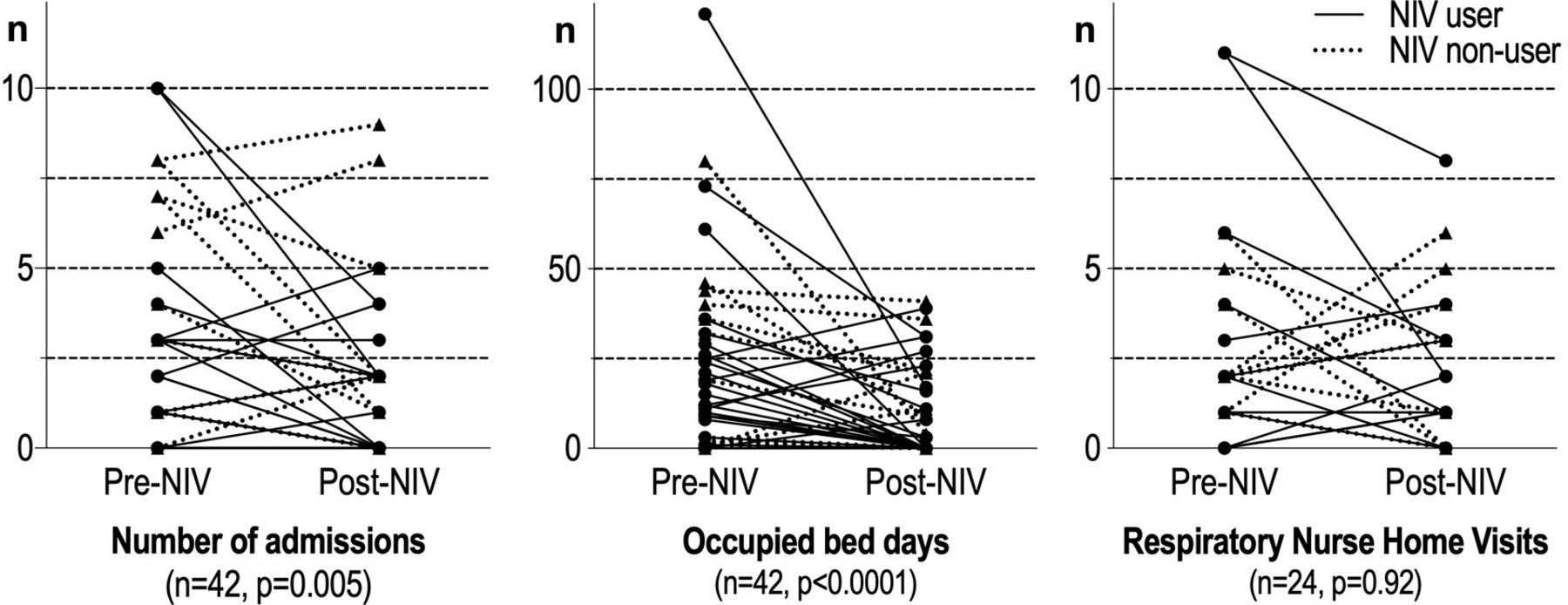
Service usage in NHS GG&C by the home-NIV cohort in the 12 months prior to commencing home-NIV (pre-NIV) and the 12 months following initiation of home-NIV (post-NIV) are outlined in table 3. A significant reduction in total number of admissions and OBDs is noted following initiation of home-NIV across all patients in the home-NIV cohort, but is particularly pronounced in NIV users (p<0.001, figure 3). The data equate to a median reduction of 14 OBDs per annum per patient who continued remote-monitored home-NIV. Requirements for respiratory nurse home visits did not change significantly following the initiation of home-NIV.
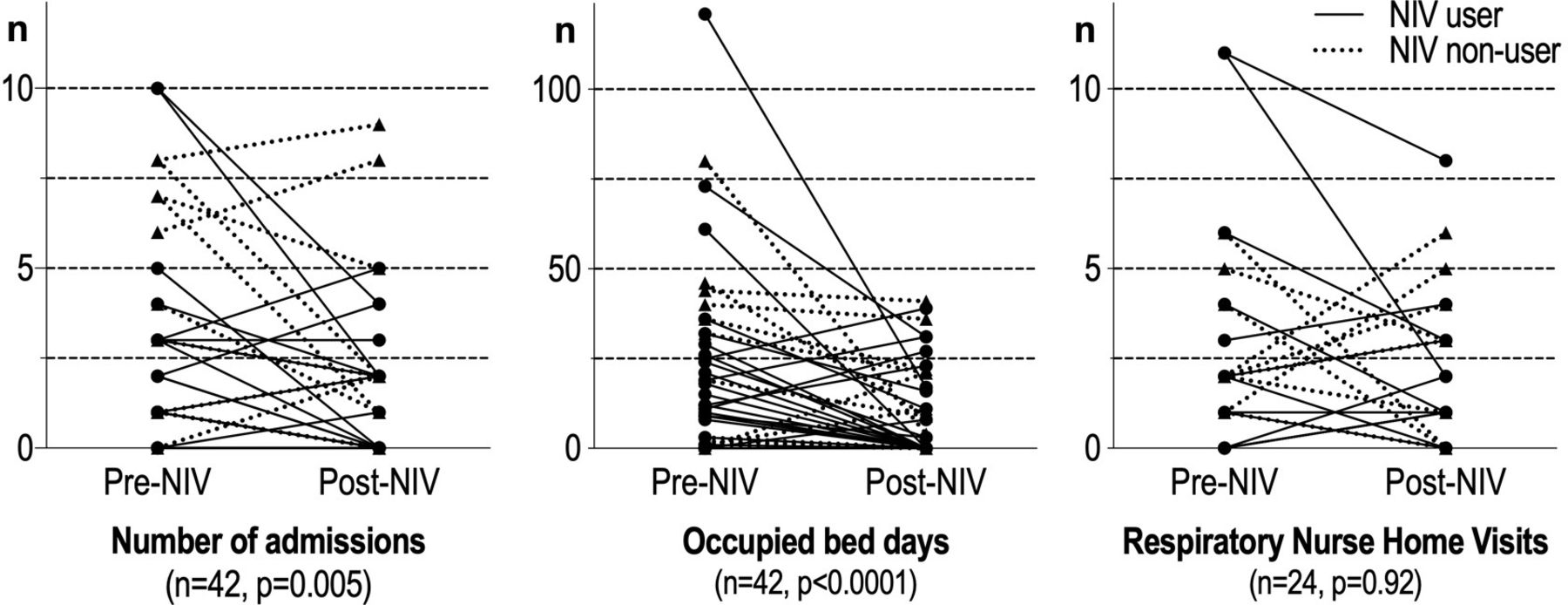
Changes in healthcare usage before and after home-NIV for NIV users (circle) and NIV non-users (triangle). Data on respiratory nurse home visits was not available in electronic health records for the 18 patients whose residence is outside our health board. NIV, non-invasive ventilation.
Changes in healthcare usage before and after home-NIV
The reduction in admissions and OBDs in the home NIV user cohort also compares favourably with patients in the comparator cohort of patients who had acute hypercapnic respiratory failure but were not referred. There was no significant change in annualised admissions in the subsequent year, but a significant rise in annualised OBDs (median increase 11 days per patient, p=0.017) following the index acute hypercapnic respiratory failure episode in this cohort (online supplemental figure 4).
Blood gases
Capillary blood gas measurements were available in 21 patients before and after home-NIV. Improvement in median PCO2 (2.2 kPa, p<0.05) and bicarbonate (4.9 mmol/L, p<0.05) from baseline was noted at follow-up after initiation of home-NIV (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in blood gas measurements at baseline and follow-up after home-NIV initiation in NIV users. Data availability limited to subset of patients who attended for face–face follow-up and had some or all components of post-NIV blood gas results inputted into electronic health record (including two patients who had PCO2 but not bicarbonate result available). Two patients had PCO2 <7 kPa at time of NIV initiation but had other standard indications to commence home NIV. NIV, non-invasive ventilation; PCO2, partial pressure of carbon dioxide.
Discussion
In this report we summarise our approach with assistive technologies for home NIV, and present retrospectively obtained outcome data in a cohort of patients with COPD with typical comorbidities who commenced treatment at our centre in the first 12 months following this service adoption. The data demonstrates the feasibility of adopting two-way remote monitoring and volume-assured auto-EPAP mode to support home NIV provision to patients with COPD. Key findings are significantly prolonged time to readmission or death in patients who commenced home NIV treatment, with fewer hospital readmissions and OBDs in the subsequent year in home-NIV users. Our experience provides early utility data for this service model, with outcomes which are in line with reported COPD-NIV RCT experience. Importantly, this data supports safety of this service model which minimises the need for elective inpatient admissions for home NIV set-up. These findings support further research and monitored adoption of technology-assisted home NIV service models using remote-monitoring and/or ‘auto-NIV’ modes.
The adverse time to readmission or death and readmission frequency noted in the comparator cohort of patients who had had acute hypercapnic respiratory failure but not been referred for home NIV consideration provides further support for the treatment benefit from home NIV. These patient cohorts are not directly comparable, which limits the inferences about home NIV treatment effect which can be made. There are also a number of potential biases. Additional comorbidity, COPD phenotype and management data are not available retrospectively. Patients were accrued over a single year which introduces seasonality and year–year variability of COPD admission confounders. In QEUH there is mandated nurse-specialist review of all admitted patients, with guideline-based care bundle provided: it is unlikely that there were major differences in approach to other components of COPD care. The observation that home NIV ‘treatment effect’ with reduction in annualised admissions and OBDs persists when the cohort is compared with non-users and the non-referred patients accrued over a similar time period mitigates the potential time-series bias. In context, this data supports—in-line with clinical trial data—the likelihood of there being a positive treatment effect from home NIV as initiated and supported with assistive technologies at our centre and demonstrates that there is a care-quality outcome gap in patients with COPD who have acute hypercapnic respiratory failure but are not considered for home NIV at presentation or early follow-up. Based on this data we now proactively ‘pull’ out patients with COPD who require acute respiratory support at our centre in for follow-up and consideration of home NIV, and we are looking to further reduce variations in care with regional and national scale-up of this approach.
We have >10 years of experience with volume-assured pressure support and auto-EPAP NIV modes rapidly achieving successful control of hypercapnic respiratory failure regardless of the complexity of the underpinning aetiology and sleep-disordered breathing. Based on this experience and with high prevalence of obesity, OSA and comorbidities in our referral population our developed service approach therefore is to commence NIV treatment for patients with COPD in iVAPS-auto-EPAP mode. We target symptom benefit, remote-monitored ventilation patterns and control of hypercapnic respiratory failure based on capillary blood gas results (see online supplemental data file), rather than targeting high pressure support in spontaneous-timed NIV mode with transcutaneous CO2 monitoring. Combining this ‘auto-NIV’ mode with two-way remote-monitoring mitigates the risk of unrecognised unintentional leak and inadequate pressure support provision confounding treatment quality. Our observed satisfactory clinical outcomes and encouraging follow-up blood gas data with a median reduction in PCO2 of 2.2 kPa in patients who could attend for follow-up demonstrates feasibility and provides encouraging support on the quality and safety of this technology assisted NIV set-up service model. Further prospective scrutiny of this approach is required, and whether matched clinical outcomes and similar efficiency would be achieved with remote-monitored NIV using other ventilation modes and/or with supporting at home transcutaneous or other modality of sleep breathing monitoring requires additional study.
The admission and survival results from our data are consistent with those in the HOT-HMV trial by Murphy et al with delayed and reduced hospital readmissions in hypercapnic patients with COPD who were referred for and continued home-NIV treatment.8 These findings are encouraging. In addition to providing preliminary support for the safety of our technology-assisted COPD-NIV service model, this data provides preliminary reassurance that benefits seen in clinical trials with home NIV in patients with COPD will be realised with real-world implementation. There are however a number of important differences comparing the HOT-HMV trial and this study, reflecting the real-world experience. Our cohort had accepted indications for starting home NIV, but our approach of pragmatically initiating home NIV during an acute episode if the patient’s presentation and shared decision-making render that appropriate are a potential confounder. Though our patients had sustained hypercapnic respiratory failure, it is possible that some of the subsequent improvement inpatient outcomes and blood gases may partly or completely reflect natural stabilisation of their condition, rather than an NIV treatment effect. It is possible that deferring NIV initiation would have achieved similar outcomes in some of our treated patients, but that other patients would have then been lost to follow-up or sustained an adverse outcome.
There was less severe documented airflow obstruction in our cohort compared with HOT-HMV cohort, but we only had historical rather than contemporary spirometry for many patients. There was also a higher BMI and a higher rate of comorbidities potentially contributing to hypercapnic respiratory failure in this study’s patient cohort compared with HOT-HMV, particularly in the subgroup of patients who continued home NIV in the following year. Patients who discontinued home NIV during follow-up had lower mean BMI and comorbidity rates than those in the cohort who continued therapy. Remote-monitoring data supports our informal observations that patient’s discontinue home NIV based on shared decision-making despite close attention to addressable factors and therapy optimisation during individualised follow-up, rather than suboptimal NIV provision. It is possible that an alternative service model would reduce NIV discontinuation rates, and that there are patient characteristics which predict treatment failure and need for alternative management options. It could be that greater attention to patient knowledge and readiness for home NIV, additional support for treatment provision, alternative approaches to NIV optimisation or modified level of contact is required to improve home NIV uptake and retention. Our data provides a foundation to further explore these possibilities. Continued scrutinised adoption of NIV remote-monitoring will provide data to help address these questions, and help establish service infrastructure where implementation of additional assistive innovations such as prioritised access to NIV failure clinical can be rapidly evaluated.19
In the HOT-HMV trial, home-NIV was noted to reduce exacerbation-related costs (by £1141 per case) and patient-reported costs (by £2337) relative to the control arm.20 NIV device cost and cost per physician visit had the greatest impact on cost per quality adjusted life year (QALY). The data from our study is in line with this, with a median reduction of 14 OBDs per annum and no increase in required respiratory nurse visits in home-NIV users. It is likely that a COPD home-NIV service model based on remote-monitoring and individualised follow-up which reduces hospital bed days, minimises physician visits and associated patient-carer travel costs will enhance cost-effectiveness. Further research and service adoption evaluations as this evidence-based intervention diffuses further into routine care are required to expand on the evidence for cost-effectiveness of home-NIV, explore the relative value of the assistive technology components and define whether a proactive COPD service model based on remote-monitoring is sustainable.
Among various patient groups using NIV at home, remote monitoring has been found to be non-inferior and at times more effective than usual face-to-face support, preferred by patients and associated with reduced healthcare utilisation.15 21–23 The additional channel of two-way patient engagement—that is, early intervention with an NIV therapy change to optimise settings based on remote-monitoring data—may prove particularly valuable to ensure continued treatment adherence. Our findings broadly complement those from recent study reported from the Netherlands, which demonstrated cost-effective provision of home initiation of NIV for stable hypercapnic patients with COPD using remote-monitoring of ventilator and transcutaneous CO2 data.24 As key additions, our data suggest that it is feasible to use assistive technologies to commence and follow-up patients with home NIV when commencement is indicated at an acute episode as well as at stable status. Transcutaneous monitoring is only selectively undertaken at NIV initation and not routinely undertaken at follow-up in our service model. Provision of transcutaneous monitoring at scale presents substantial challenges and the positive clinical outcomes that we noted in follow-up of home NIV users provides some provisional reassurance about the safety of omitting this monitoring. Continued supervision of this approach with an expanded prospective cohort and continued reporting of outcomes to ensure safety and quality of home-NIV therapy, with continued evaluation of other surrogate endpoints for respiratory failure monitoring is required.
This study had several strengths, including the use of clinically meaningful outcomes and the real-world nature of the patient cohorts. However, we acknowledge several limitations. Treatment allocation was not randomised. Unrecognised confounding factors including differences in COPD severity, natural disease history, unquantified patient activation measures affecting continued NIV usage and potential heterogeneity of uptake of other components of COPD care potentially bias the data. We also did not have complete data on demographics, comorbidities or provision of and adherence to other COPD treatments to ensure cohorts were otherwise matched. The statistical analyses of the subgroup analyses is exploratory due to the limited sample size and the potential issue of multiple testing. Finally, this study was not powered to find a difference in survival. While a survival benefit of home-NIV has been previously demonstrated in a similar patient population,9 clear evidence of improved survival is still lacking and should be investigated in larger prospective trials.
Conclusion
Patients with COPD with persistent hypercapnic respiratory failure have poor outcomes with limited treatment options available. In this study we confirm the feasibility of adopting a service model supported by assistive technologies—remote-monitoring and ‘auto-NIV’ mode—for the provision of home-NIV in a cohort of patients with COPD with comorbidities, as they typically present in clinical practice. Home-NIV prolonged the time to readmission or death within 12 months in treated patients, supporting the utility of this service model. In addition to being the outcomes that patients with COPD rate as most important,4 exacerbation and hospitalisation avoidance address the substantial economic burden imposed by COPD. We noted reductions in healthcare usage among home-NIV users. The COVID-19 pandemic has presented considerable challenges to home-NIV service provision. Our study provides data supporting the feasibility and utility of a service model based on outpatient or truncated inpatient NIV initiation using iVAPS-autoEPAP mode with remote monitoring based individualised follow-up. Continued prospective evaluation of safety and outcomes with use of these NIV technologies is required, but the advantages including reduced patient travel, reduced need for face–face contact and reduced nosocomial COVID-19 risk, with positive data supporting real-world positive impact of home NIV on COPD care-quality supports ongoing considered adoption of similar service models, with an approach as set out in the European Respiratory Society task force guidance on home NIV in COPD.10
Supplemental material
Data availability statement
Data are available upon reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
Part of a programme of work approved by NHS Greater Glasgow and Clyde SafeHaven Local Privacy and Advisory Committee (Ref GSH/19/RM/003).
Acknowledgments
We gratefully acknowledge the comprehensive contribution of the respiratory physiologist and nurse specialist teams in NHS Greater Glasgow and Clyde to the positive outcomes reported in this paper. They have enthusiastically adapted service models to realise benefits from assistive technologies, and their commitment to improving patient outcomes and providing realistic medicine is inspiring.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors GM, MS, HT, JH and CMC analysed the data. SK and CO provided unrestricted writing input for the manuscript. All authors drafted and revised the paper. CMC is the guarantor.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests GM, MS, HT, JH and DJL have no conflicts of interest to declare. SK and CO are employees of ResMed. CMC has received travel reimbursement and speaker’s fees to research endowment fund from ResMed, Fisher & Paykel and Phillips Respironics, and unrestricted investigator-initiated grant funding from ResMed unrelated to this study.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.