Article Text

Abstract
Objective To investigate the association between recent statin exposure and risk of severe COVID-19 infection and all-cause mortality in patients with COVID-19 in Denmark.
Design and setting Observational cohort study using data from Danish nationwide registries.
Participants Patients diagnosed with COVID-19 from 22 February 2020 to 17 May 2020 were followed from date of diagnosis until outcome of interest, death or 17 May 2020.
Interventions Use of statins, defined as a redeemed drug prescription in the 6 months prior to COVID-19 diagnosis.
Primary and secondary outcome measures All-cause mortality, severe COVID-19 infection and the composite.
Results The study population comprised 4842 patients with COVID-19 (median age 54 years (25th–75th percentile, 40–72), 47.1% men), of whom 843 (17.4%) redeemed a prescription of statins. Patients with statin exposure were more often men and had a greater prevalence of comorbidities. The median follow-up was 44 days. After adjustment for age, sex, ethnicity, socioeconomic status and comorbidities, statin exposure was not associated with a significantly different risk of mortality (HR 0.96 (95% CI 0.78 to 1.18); 30-day standardised absolute risk (SAR), 9.8% (8.7% to 11.0%) vs 9.5% (8.2% to 10.8%); SAR difference, −0.4% (−1.9% to 1.2%)), severe COVID-19 infection (HR 1.16 (95% CI 0.95 to 1.41); 30-day SAR, 13.0% (11.8% to 14.2%) vs 14.9% (12.8% to 17.1%); SAR difference, 1.9% (−0.7% to 4.5%)), and the composite outcome of all-cause mortality or severe COVID-19 infection (HR 1.05 (95% CI 0.89 to 1.23); 30-day SAR, 17.6% (16.4% to 18.8%) vs 18.2% (16.4% to 20.1%); SAR difference, 0.6% (−1.6% to 2.9%)). The results were consistent across subgroups of age, sex and presumed indication for statin therapy. Among patients with statin exposure, there was no difference between statin drug or treatment intensity with respect to outcomes.
Conclusions Recent statin exposure in patients with COVID-19 infection was not associated with an increased or decreased risk of all-cause mortality or severe infection.
- COVID-19
- epidemiology
- cardiology
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Strengths and limitations of this study
The study was based on high-quality and complete data from nationwide administrative registries.
The Danish healthcare system provides equal access to healthcare services for all residents regardless of socioeconomic or insurance status.
The observational nature of this study precludes the assessment of cause–effect relationships.
Residual confounding and confounding by indication cannot be excluded.
Introduction
The COVID-19 pandemic, caused by SARS-CoV-2, is an unprecedented threat to global health in recent time.1 Governments worldwide have imposed comprehensive measures to prevent the rapid spread of SARS-CoV-2, including extensive societal lockdown and reorganisation of healthcare systems. Recently, an observational study demonstrated that in-hospital use of statins was associated with substantial improvement in survival among patients hospitalised with COVID-19.2 Specifically, the authors reported a relative risk reduction of 42% in in-hospital mortality with statin therapy. This finding may be biased by patient selection, treatment indication and residual confounding and therefore merits further investigation.2 In addition, a computer-based study suggested that rosuvastatin may be effective in the treatment of COVID-19 infection.3 However, other observational studies, including a meta-analysis, did not find any association between statins and improved outcomes in patients with COVID-19.4–6
Several mechanisms by which statins may exert their potential beneficial effects have been proposed. First, the case fatality rate with COVID-19 infection is substantially higher in patients with established cardiovascular disease and diabetes than those without, and there is evidence of cardiac involvement and myocardial injury in some patients with COVID-19.7–17 Given their potential cardioprotective effects, statins may possibly prevent myocardial injury and adverse cardiovascular events, particularly in patients with established cardiovascular disease.18 Second, beyond their lipid-lowering properties, statins exert various beneficial pleiotropic effects, including modulating the immune response at different levels, improving endothelial function, and decreasing oxidative stress and inflammation.18–21 Third, some randomised clinical trials and observational studies—but not all—have indicated that statins may be associated with less severe infection and improved outcomes in patients with viral infections.22–31 On the other hand, experimental studies have suggested that statins, among other drugs, may increase the expression of ACE2,32–34 a membrane-bound aminopeptidase expressed in the lungs, heart and other tissues that is thought to facilitate entry of SARS-CoV-2 into the cells.35–37 Also, case series have reported hypercholesterolaemia to be one of the most common comorbidities in patients with COVID-19.38 These considerations have led to the concern that statins may confer a predisposition to more severe infection and adverse outcomes during COVID-19 infection. Taken together, the effect of statins on outcomes in patients with COVID-19 infection remains unclear.
In light of these uncertainties, it is important to assess whether statin therapy may improve the clinical course of patients with COVID-19 infection or lead to further deterioration. To address this issue, we performed a nationwide registry-based cohort study to investigate the association between recent statin exposure and the risk of severe COVID-19 infection and all-cause mortality in patients with COVID-19 infection.
Methods
Data sources
In Denmark, all citizens are assigned a unique and personal identification number, which allows accurate linkage of nationwide administrative registries at an individual level. For this study, data from the following nationwide administrative registries were obtained: the Danish National Patient Registry, which contains data on all hospital admissions and outpatient contacts according to the International Classification of Diseases (ICD)39; the Danish National Prescription Registry, which holds information on dispensing date, strength and quantity of all claimed drug prescriptions in Denmark40; the Danish Civil Registration System, which holds information on birth date, sex and vital status (ie, whether a person is alive and a resident of Denmark, disappeared, emigrated or dead, along with the date of these events)41; and Statistics Denmark, which holds data on education, household income and marital status.42 43 The Danish registries are validated, of high quality and have been described in detail previously.39–43
Study population
The study population comprised all Danish citizens who were examined at a hospital, including inpatient, outpatient and emergency department visits, and had a primary or secondary diagnosis code for COVID-19 infection (ICD-10 codes: B342, B972) from 22 February 2020 until 17 May 2020. According to the Danish Ministry of Health, these codes have a positive predictive value of 99%. Comorbidity was obtained using in-hospital and outpatient diagnosis codes any time prior to diagnosis (online supplemental etable 1 for ICD-8 and ICD-10 codes). Patients with hypertension were identified using claimed drug prescriptions as described previously.44 45 Pharmacotherapy at baseline was defined as claimed prescriptions within 180 days prior to diagnosis (online supplemental eTable 2 for Anatomical Therapeutic Chemical (ATC) Classification System codes). The highest level of completed education was classified in accordance with the International Standard Classification of Education. Average household income in 2018 was calculated and graded in quartiles. The duration of statin treatment prior to COVID-19 diagnosis was determined for each individual during follow-up using an algorithm based on claimed prescriptions, taking date of claimed prescriptions, dosage and packing size into account, as described previously.46 47
Supplemental material
Exposure
Exposure to statins was defined as at least one redeemed prescription of a statin (ATC code C10AA) in the 6 months prior to diagnosis.
Outcomes
The primary outcome was all-cause mortality. The secondary outcomes were (1) severe COVID-19 infection, defined as a hospital diagnosis of ‘COVID-19 severe acute respiratory syndrome’ (ICD-10 code: B972A) or admission to an intensive care unit; and (2) the composite of all-cause mortality or severe COVID-19 infection. Patients were followed from the date of diagnosis until occurrence of the outcome of interest, death, emigration or 17 May 2020, whichever came first.
Statistics
Baseline characteristics were reported as frequencies with percentages or medians with 25th–75th percentiles. Differences in baseline characteristics according to statin exposure were tested with χ2 test for categorical variables and Mann-Whitney test for continuous variables. Cause-specific unadjusted and adjusted Cox regression models were used to compare outcomes according to statin exposure. Adjusted models included the following variables: age (modelled as a restricted cubic spline with three knots: 10th, 50th and 90th percentile), sex, ethnicity (native Danish, immigrant, descendant from immigrant), education, income, comorbidity (ie, history of ischaemic heart disease, stroke, peripheral artery disease, diabetes mellitus, heart failure, atrial fibrillation, hypertension, malignancy, chronic kidney disease, chronic obstructive pulmonary disease, liver disease) and concomitant medical treatment (ie, aspirin, oral anticoagulants, beta-blockers, calcium channel blockers, renin-angiotensin-aldosterone system inhibitors). Reported were HRs, 30-day risks of outcomes standardised to the risk factor distribution of all patients in the sample, and differences of standardised 30-day risks. For the outcome severe COVID-19 infection, the main Cox regression model was combined with a Cox regression model for the rate of the competing risk of death without severe COVID-19 infection.48 Interactions between statin exposure and clinically relevant variables (including age categories, sex, presumed indication for statin therapy (ie, history of stroke, ischaemic heart disease, peripheral artery disease, diabetes mellitus or familial hypercholesterolaemia)) on outcomes were tested for. All statistical analyses were performed with SAS V.9.4 statistical software and R V.3.6.1 (The R Foundation).49 The level of statistical significance was set at 5%.
To test the robustness of our findings, a number of sensitivity analyses were performed: (1) The definition of statin exposure was changed from at least one redeemed prescription of a statin in the 6 months prior to diagnosis to 3 months. (2) The risk of death among patients with severe COVID-19 infection according to statin exposure was examined. (3) Among patients with statin exposure, the risks of outcomes according to statin treatment intensity (ie, high-intensity vs moderate-intensity/low-intensity) were investigated. High-intensity statin therapy was defined as either (1) atorvastatin 40–80 mg daily, (2) rosuvastatin 20–40 mg daily or (3) simvastatin 80 mg daily. (4) Among patients with statin exposure, the risk of outcomes according to statin drug (ie, simvastatin, atorvastatin, rosuvastatin) was examined. Pravastatin was excluded from this analysis due to a low number of patients prescribed this drug. (5) The statin population was restricted to those with a treatment duration of at least 3 months.
Patient and public involvement
This research was done without patient involvement. Patients were not invited to comment on the study design and were not consulted to develop patient relevant outcomes or interpret the results. Patients were not invited to contribute to the writing or editing of this document for readability or accuracy.
Results
In total, 4842 patients with COVID-19 infection were included in the study. Of these, 843 (17.4%) redeemed a prescription of statins within 6 months prior to diagnosis. The first patient was included on 22 February 2020 and the last patient on 17 May 2020. The median age of the study population was 54 years (25th–75th percentile, 40–72), and 47.1% were men. The mean duration of statin treatment prior to COVID-19 diagnosis was 3.6 years. The baseline characteristics of the patients in the groups of interest are summarised in table 1. Patients with statin exposure were older, more often men and native Danish, had a greater prevalence of cardiovascular and non-cardiovascular comorbidities, and a higher utilisation of medication compared with those admitted with no statin exposure. The median follow-up time from the date of COVID-19 diagnosis was 44 days (25th–75th percentile, 29–56).
Baseline characteristics of patients with COVID-19 with and without statin exposure
All-cause mortality, composite outcome and severe COVID-19 infection
Unadjusted, sex-adjusted and age-adjusted, and fully adjusted HRs for statin exposure and outcomes are shown in figure 1. Table 2 displays unadjusted, sex-adjusted and age-adjusted, and fully adjusted standardised 30-day absolute risks of outcomes according to statin exposure. In total, 488 (10.1%) patients died during follow-up: 177 (21.0%) in the statin group and 311 (7.8%) in the non-statin group. In the unadjusted Cox regression analysis, statin exposure was associated with a significantly higher risk of mortality compared with no statin exposure (HR 2.87 (95% CI 2.39 to 3.46)). However, when adjusting for age, sex, ethnicity, socioeconomic status and comorbidities, statin exposure was not associated with a significantly different risk of mortality (HR 0.96 (95% CI 0.78 to 1.18)). Similarly, the standardised absolute 30-day risk of all-cause mortality was not significantly different between groups (9.8% (8.7% to 11.0%) vs 9.5% (8.2% to 10.8%) in the no statin and statin exposure groups, respectively; standardised absolute risk difference, −0.4% (−1.9% to 1.2%)).

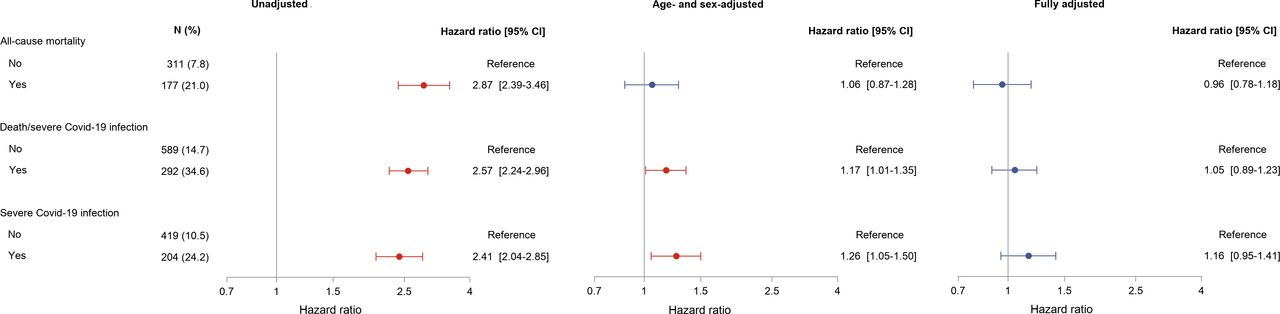{kind=link}
HR for all-cause mortality, a composite of severe COVID-19 infection or all-cause mortality, and severe COVID-19 infection according to statin exposure. Adjusted for age, sex, ethnicity, education, income, comorbidity (ie, history of ischaemic heart disease, stroke, peripheral artery disease, diabetes mellitus, heart failure, atrial fibrillation, hypertension, malignancy, chronic kidney disease, chronic obstructive pulmonary disease, liver disease) and concomitant medical treatment (ie, aspirin, oral anticoagulants, beta-blockers, calcium channel blockers, renin-angiotensin-aldosterone system inhibitors).
Standardised 30-day absolute risks and risk differences for all-cause mortality, a composite of severe COVID-19 infection or all-cause mortality, and severe COVID-19 infection according to statin exposure
During follow-up, 881 (18.2%) patients experienced the composite outcome of all-cause mortality or severe COVID-19 infection: 292 (34.6%) in the statin group and 589 (14.7%) in the non-statin group. Although statin exposure was associated with a significantly higher risk of the composite outcome compared with no statin exposure in the unadjusted Cox regression analysis (HR 2.57 (95% CI 2.34 to 2.96)), statin exposure was not associated with a significantly different risk of mortality in the fully adjusted analysis (HR 1.05 (95% CI 0.89 to 1.23)). Similarly, the standardised absolute 30-day risk of the composite outcome was not significantly different between groups (17.6% (16.4% to 18.8%) vs 18.2% (16.4% to 20.1%) in the no statin and statin exposure groups, respectively; standardised absolute risk difference, 0.6% (−1.6% to 2.9%)).
In total, 623 (12.9%) patients developed severe COVID-19 infection during follow-up: 204 (24.2%) in the statin group and 419 (10.5%) in the non-statin group. In the unadjusted Cox regression analysis, statin exposure was associated with a significantly higher risk of severe COVID-19 infection compared with no statin exposure (HR 2.41 (95% CI 2.04 to 2.85)). However, in the fully adjusted analysis, statin exposure was not associated with a significantly different risk of severe COVID-19 infection (HR 1.16 (95% CI 0.95 to 1.41)). Similarly, the standardised absolute 30-day risk of severe COVID-19 infection was not significantly different between groups (13.0% (11.8% to 14.2%) vs 14.9% (12.8% to 17.1%) in the no statin and statin exposure groups, respectively; standardised absolute risk difference, 1.9% (−0.7% to 4.5%)).
Subgroup and sensitivity analyses
The results of the prespecified subgroup analyses for the primary and secondary outcomes are displayed in table 3. In all subgroups, statin exposure was not associated with a significantly different risk of all-cause mortality, a composite of all-cause mortality or severe COVID-19 infection, and COVID-19 infection (p for interaction >0.23 for all subgroups).
Fully adjusted HR for all-cause mortality, a composite of severe COVID-19 infection or all-cause mortality, and severe COVID-19 infection according to statin exposure in subgroups
To test the robustness of the findings, we performed a number of sensitivity analyses. (1) The definition of statin exposure was changed from as at least one redeemed prescription of a statin in the 6 months prior to diagnosis to 3 months. In total, 646 (13.3%) patients redeemed a prescription of a statin within 3 months. Among those who redeemed a statin prescription within 6 months, but not within 3 months, 82.2% redeemed a prescription of 100 tablets or more. In this analysis, statin exposure was not associated with a significantly different risk of all-cause mortality (adjusted HR 0.97 (95% CI 0.78 to 120); standardised absolute 30-day risk difference, −0.2% (−1.8% to 1.3%)), a composite of all-cause mortality or severe COVID-19 infection (adjusted HR 1.06 (95% CI 0.90 to 1.26); standardised absolute 30-day risk difference, 0.9% (−1.4% to 3.3%)), or severe COVID-19 infection (adjusted HR 1.18 (95% CI 0.97 to 1.45); standardised absolute 30-day risk difference, 2.3% (−0.4% to 5.1%)). (2) The risk of death among patients with severe COVID-19 infection according to statin exposure was examined. In this analysis, statin exposure was not associated with a significantly different risk of all-cause mortality (adjusted HR 0.91 (95% CI 0.65 to 1.27)). (3) Among patients with statin exposure, the risks of outcomes according to intensity of statin therapy were investigated. In total, 305 (36.2%) patients received high-intensity statin therapy. Compared with moderate-intensity/low-intensity therapy, high-intensity statin therapy was not associated with a significantly different risk of all-cause mortality (adjusted HR 1.07 (95% CI 0.77 to 1.50)), a composite of all-cause mortality or severe COVID-19 infection (adjusted HR 0.95 (95% CI 0.73 to 1.22)), or severe COVID-19 infection (adjusted HR 0.81 (95% CI 0.60 to 1.10)). (4) Among patients with statin exposure, the risks of outcomes according to statin drug were investigated. Compared with simvastatin, atorvastatin and rosuvastatin were not associated with a significantly different risk of all-cause mortality (atorvastatin: adjusted HR 0.99 (95% CI 0.72 to 1.37); rosuvastatin: adjusted HR 0.43 (95% CI 0.15 to 1.19)), a composite of all-cause mortality or severe COVID-19 infection (atorvastatin: adjusted HR 0.91 (95% CI 0.71 to 1.17); rosuvastatin: adjusted HR 0.90 (95% CI 0.53 to 1.54)), or severe COVID-19 infection (atorvastatin: adjusted HR 0.80 (95% CI 0.60 to 1.08); rosuvastatin: adjusted HR 1.03 (95% CI 0.59 to 1.82)). (5) The statin population was restricted to those with a treatment duration of at least 3 months. Excluding patients in the statin group with a treatment duration less than 3 months, the population yielded similar findings as the main results (all-cause mortality, adjusted HR 1.00 (95% CI 0.81 to 1.24); a composite of all-cause mortality or severe infection, 1.09 (0.92 to 1.29); severe COVID-19 infection, 1.19 (0.97 to 1.47)).
Discussion
In this Danish nationwide cohort study, we investigated the association between recent statin exposure and the risk of all-cause mortality or severe infection, individually and as a composite, in patients with COVID-19 infection. The main finding of this study was that statin exposure prior to COVID-19 diagnosis was not associated with an improvement or deterioration in the clinical course of patients with COVID-19 infection, and this was consistent across clinically relevant subgroups.
In a recent observational study using data from 21 hospitals in Hubei Province, China, Zhang et al 2 demonstrated that in-hospital use of statins was associated with improved survival among patients hospitalised with COVID-19. Specifically, the authors found a 28-day mortality risk of 5.2% and 9.4% in the statin and non-statin user groups, respectively, and that in-hospital use of statins was associated with a 42% decrease in in-hospital mortality.2 Although the data may be biased by patient selection, treatment indication and residual confounding, including lack of adjustment for socioeconomic status and prehospital medication, this controversial finding merits further investigation. In addition, Farag et al3 performed a computer-based study and used a structure-based drug design to screen more than 2000 Food and Drug Administration-approved drugs against SARS-CoV-2 main protease enzyme substrate-binding pocket. Other than antiviral drugs, the authors also identified rosuvastatin as a drug that may be useful against SARS-CoV-2. On the other hand, other observational studies, including a meta-analysis, did not find an association between statin therapy and improved outcomes in patients with COVID-19.4–6 In our nationwide cohort study including all patients with COVID-19, irrespective of hospitalisation status, we did not find any association between statin use prior to diagnosis and the risk of all-cause mortality or severe COVID-19 infection, individually and as a composite. These results were consistent across clinically relevant subgroups, including age, sex and presumed indication for statin therapy. In addition, among patients using statins, type of statin drug did not significantly modify the risk of outcomes, although there was a trend towards a lower risk of all-cause mortality with rosuvastatin. Further studies are warranted to establish whether rosuvastatin may improve outcomes in patients with COVID-19 infection. Taken together, our study does not provide evidence of a beneficial effect of statin exposure prior to COVID-19 diagnosis.
Several hypotheses have been proposed in relation to the role of statin therapy in patients with COVID-19. It has been proposed that statins may improve the clinical course in patients with COVID-19, and several mechanisms by which statins exert their potential beneficial effects have been proposed. For example, reports of cardiac involvement during the course of the infection, particularly in severe cases, have emerged,7–17 and it has been hypothesised that statins, at least to some extent, may prevent or decrease the likelihood of myocardial injury and cardiovascular events.18 Further, statins may modulate the immune response, improve endothelial function, and decrease oxidative stress and inflammation and thereby predispose to less severe infection and better outcomes.18–21 Data on such effects of statins in humans, however, are conflicting. While some randomised trials and observational studies have demonstrated possible benefits of statins in reducing mortality and improving the clinical course of patients with severe infections, particularly viral infections, others have not found any beneficial effects of statins in this setting.22–31 On the other hand, preclinical studies have suggested that statins upregulate the expression of ACE2, an enzyme thought to facilitate entry of SARS-CoV-2 into the cells, although this hypothesis has not been proven in humans.32–34 Moreover, hypercholesterolaemia has been reported to be one of the most common comorbidities in patients with COVID-19, although the majority of these case series did not report data on medication, including statins.38 These considerations had led to the hypothesis that statins confer a greater risk of more severe infection and adverse outcomes during COVID-19 infection. In light of these concerns, it is reassuring that statins were not associated with a deterioration in the clinical course of these patients in our study. Taken together, our findings do not support discontinuation of statin therapy in patients with an indication for statins. However, it is important to emphasise the inherent limitations of observational studies, including residual confounding, confounding by indication and inadequate assessment of causal inference. There is, therefore, a need for further studies to establish the role of statins in patients with COVID-19 with and without an indication for statin therapy. Several randomised clinical trials have been initiated to assess this clinically relevant issue, and the results from these trials are anticipated.50–53
Another potential concern with statins during COVID-19 infection is liver injury. Reports of liver injury during the course of the infection, particularly in severe cases, have emerged.54–56 Although statins are generally considered to be safe and well tolerated, in rare cases, these medications may also induce liver injury.57 Consequently, the European Society of Cardiology guidelines for the diagnosis and management of cardiovascular disease during the COVID-19 pandemic recommend withholding statin therapy temporarily in patients with COVID-19 with increased liver enzymes.58 Whether statin therapy confers an increased risk of liver injury and subsequent adverse outcomes during COVID-19 infection has not been established. Our study did not allow for a direct assessment of this issue due to lack of data on in-hospital medication and laboratory findings. Nevertheless, it is reassuring that statin exposure prior to diagnosis was not associated with an increased risk of worse outcomes in patients with COVID-19. Further studies, preferably randomised controlled trials, are needed to clarify the association between statin therapy and liver injury on subsequent outcomes during COVID-19 infection.
Strengths and limitations
The main strength of this study is the completeness of data from nationwide administrative registries. The Danish healthcare system, funded by taxes, provides equal access to healthcare services for all residents regardless of socioeconomic or insurance status. In Denmark, statins can be purchased only through prescription. Due to partial reimbursement of drug expenses by the Danish healthcare system, pharmacies are required to register all redeemed prescriptions ensuring complete and accurate registration. The findings of this study should be viewed in the context of a number of limitations. The observational nature of this study precludes the assessment of cause–effect relationships; thus, only associations are reported. Residual confounding cannot be excluded despite adjustment for potential confounders, and it is likely that these adjustments were not sufficient to even out the differences between the groups. For example, mounting evidence suggests that patients with COVID-19 may develop clinically significant coagulopathy with fatal thromboembolic complications,59–61 and more statin users were treated with aspirin and oral anticoagulants compared with non-statin users. Although we attempted to minimise the impact of these differences by adjusting for concomitant medication, including aspirin and oral anticoagulants, in the fully adjusted analyses, we cannot exclude the possibility that these differences may have had an impact on the association between statin use and outcomes. In addition, confounding by indication cannot be omitted in pharmacoepidemiological studies despite our attempt to minimise the impact of this limitation by performing several subgroup analyses (eg, patients with or without a presumed indication for statin therapy). We did not have laboratory data to confirm a positive swab test for COVID-19. However, coding of both tested individuals with tentative diagnosis codes and those with positive swabs with definite diagnosis codes have been and are systematically performed in Denmark, and the Danish Ministry of Health have indicated a positive predictive value of 99% of these codes. Compared with the official COVID-19 case numbers in Denmark, this study included fewer cases because ICD-10 codes capture only those patients who were diagnosed in the hospital system (inpatient, outpatient or emergency department visits) and not in dedicated COVID-19 diagnostic kiosks. It is therefore possible that some patients with no or few symptoms may not have been captured by our ICD-10 codes. The outcomes examined in this study were clinically relevant ‘hard’ endpoints. Although it would have been interesting to examine the association between recent statin exposure and symptom improvement in patients with COVID-19, data on symptoms were not available. In addition, due to lack of data on in-hospital medication, we were not able to investigate the impact of in-hospital statin therapy on outcomes. Likewise, data on statin treatment (dis)continuation after the COVID-19 diagnosis were not available, although it was encouraged to continue statin treatment at the Danish hospitals. Exposure to statins was defined by redeemed prescriptions in the 6 months prior to diagnosis, although similar results were yielded when restricting this definition from 6 months to 3 months. It is possible that some patients may discontinue statin treatment prior to diagnosis due to early symptoms of COVID-19 infection. However, we believe that this number is likely to be low, as the mainstream media and professional medical societies have not raised questions about statin treatment in the setting of COVID-19 to the same extent as, for example, ACE inhibitors/angiotensin receptor blocker treatment. Finally, data on whether patients were prescribed statins for primary or secondary prevention were not available. However, restricting the study population to patients with a presumed indication for statin therapy (ie, history of stroke, ischaemic heart disease, peripheral artery disease, diabetes mellitus or familial hypercholesterolaemia) yielded similar findings as the main analyses.
Conclusions
In this Danish nationwide cohort study, recent statin exposure in patients with COVID-19 infection was not associated with an increased or decreased risk of all-cause mortality or severe infection. Hence, our study does not suggest benefit or harm of statin therapy in patients with COVID-19. However, further studies are needed to establish the role of statins in patients with COVID-19 with and without an indication for statin therapy. Several randomised clinical trials have been initiated to assess this clinically relevant issue in patients with COVID-19, and the results from these trials are anticipated.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors JHB and ELF had full access to all of the data in the study and take responsibility for the integrity of the data and the accuracy of the data analysis. Study concept and design: JHB, ELF, LK. Acquisition, analysis or interpretation of data: all authors. Drafting of the manuscript: JHB. Critical revision of the manuscript for important intellectual content: all authors. Statistical analysis: JHB.
Funding The authors have not declared a specific grant for this research from any funding agency in the public, commercial or not-for-profit sectors.
Competing interests None declared.
Patient consent for publication Not required.
Ethics approval In Denmark registry-based studies that are conducted for the sole purpose of statistics and scientific research do not require ethical approval or informed consent by law. However, the study is approved by the data responsible institute (Capital Region of Denmark, approval number: P-2019-191) in accordance with the General Data Protection Regulation.
Provenance and peer review Not commissioned; externally peer reviewed.
Data availability statement No data are available. Data for this study are derived from Statistics Denmark. By law, these data are not allowed to be shared and therefore data cannot be made available to other researchers.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.